
Research and Evaluation in a Child-Focused Place-Based Initiative: West Philly Promise Neighborhood

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Setting
2.2. Target Population
2.3. Outcomes
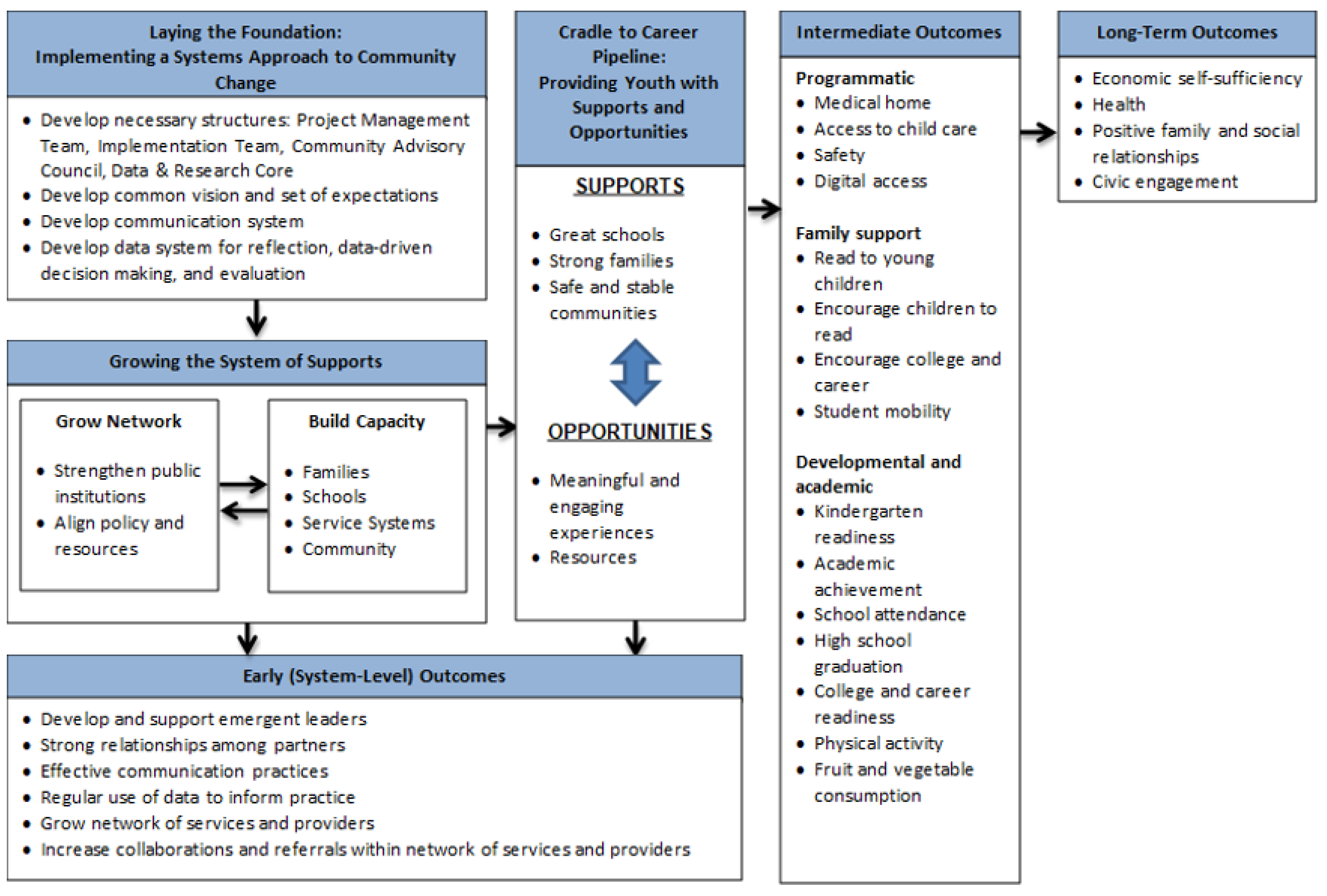
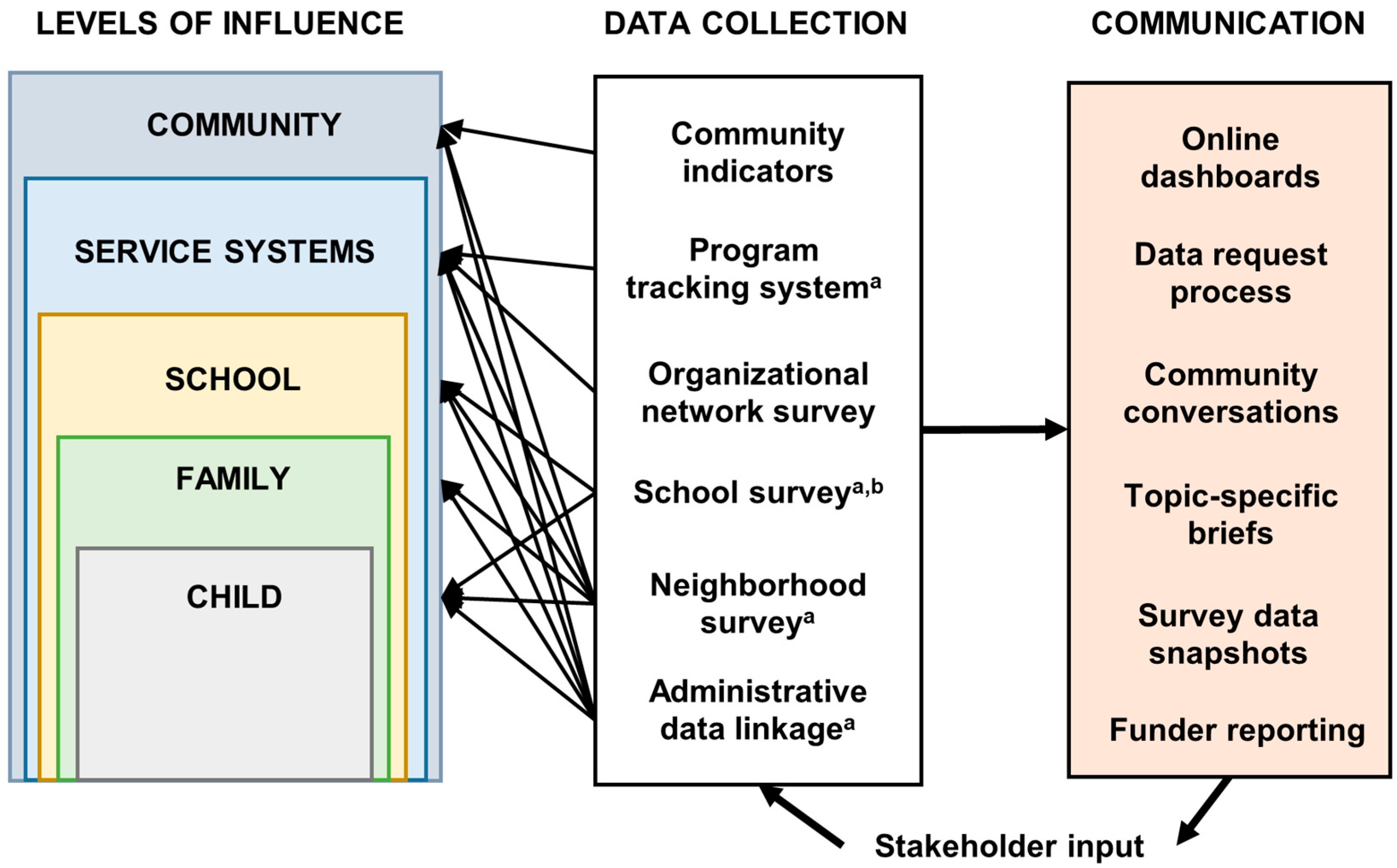
2.4. Evaluation Framework and Design
- Ensure all data and research activities adhere to guiding principles of transparency, accountability, and data democratization.
- Establish systems to collect, monitor, and communicate data at multiple levels with focus on multiple uses of the data and future sustainability.
- Adhere to grant requirements on data collection and reporting.
3. Results
3.1. Population
3.2. WPPN Programming (Supports and Opportunities)
3.3. Outcomes
3.4. Communication
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Burke, L.M.; Schwalbach, J. Housing Redlining and Its Lingering Effects on Education Opportunity; The Heritage Foundation: Washington, DC, USA, 2021. [Google Scholar]
- Mujahid, M.S.; Gao, X.; Tabb, L.P.; Morris, C.; Lewis, T.T. Historical redlining and cardiovascular health: The Multi-Ethnic Study of Atherosclerosis. Proc. Natl. Acad. Sci. USA 2021, 118, e2110986118. [Google Scholar] [CrossRef]
- Dankwa-Mullan, I.; Perez-Stable, E.J. Addressing health disparities is a place-based issue. Am. J. Public Health 2016, 106, 637–639. [Google Scholar] [CrossRef] [PubMed]
- Kelly, T., Jr. Five simple rules for evaluating complex community initiatives. Community Invest. 2010, 22, 19–36. [Google Scholar]
- Smith, R.E. How to Evaluate Choice and Promise Neighborhoods; Urban Institute: Washington, DC, USA, 2011. [Google Scholar]
- Bellefontaine, T.; Wisener, R. The Evaluation of Place-Based Approaches: Questions for Further Research; Policy Horizons Canada: Ottawa, ON, Canada, 2011.
- Theodos, B.; Firschein, J. Evaluating Community Change Programs; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2015; pp. 259–280. [Google Scholar] [CrossRef]
- Burgemeister, F.C.; Crawford, S.B.; Hackworth, N.J.; Hokke, S.; Nicholson, J.M. Place-based approaches to improve health and development outcomes in young children: A scoping review. PLoS ONE 2021, 16, e0261643. [Google Scholar] [CrossRef] [PubMed]
- Moore, T.G.; McHugh-Dillon, H.; Bull, K.; Fry, L.; Laidlaw, B.; West, S. The Evidence: What We Know about Place-Based Approaches to Support Children’s Wellbeing; Murdoch Childrens Research Institute and The Royal Children’s Hospital Centre for Community Child Health: Parkville, VI, Australia, 2014. [Google Scholar]
- Wilks, S.; Lahausse, J.; Edwards, B. Commonwealth Place-Based Service Delivery Initiatives: Key Learnings Project (Research Report No. 32); Australian Institute of Family Studies: Melbourne, VIC, Australia, 2015.
- Heery, L.; Naccarella, L.; McKenzie, R. “Improvement focused” evaluation of place-based initiatives: An approach to examining three methodologies. Eval. J. Australas. 2018, 18, 99–108. [Google Scholar] [CrossRef]
- Heery, L.; Naccarella, L.; McKenzie, R. ‘Improvement focused’ evaluation of place-based initiatives: An examination of three methodologies. Eval. J. Australas. 2018, 18, 165–182. [Google Scholar] [CrossRef]
- Crew, M. The Effectiveness of Place-Based Programmes and Campaigns in Improving Outcomes for Children; The National Literacy Trust: London, UK, 2020. [Google Scholar]
- US Department of Education. Initiatives: Promise Neighborhoods. Available online: https://www2.ed.gov/programs/promiseneighborhoods/resources.html (accessed on 28 February 2023).
- Horsford, S.D.; Sampson, C. Promise Neighborhoods: The Promise and Politics of Community Capacity Building as Urban School Reform. Urban Educ. 2014, 49, 955–991. [Google Scholar] [CrossRef]
- Comey, J.; Tatian, P.A.; Freiman, L.; Winkler, M.K.; Hayes, C.; Franks, K.; Jordan, R. Measuring Performance: A Guidance Document for Promise Neighborhoods on Collecting Data and Reporting Results; The Urban Institute: Washington, DC, USA, 2013. [Google Scholar]
- Philadelphia Office of Community Empowerment and Opportunity. Promise Zone. Available online: http://www.sharedprosperityphila.org/our-initiatives/promise-zone/ (accessed on 10 March 2023).
- Kania, J.; Kramer, M. Collective impact. Stanf. Soc. Innov. Rev. 2011, 9, 36–41. [Google Scholar] [CrossRef]
- Urban Health Collaborative. Drexel University Urban Health Collaborative. Available online: https://drexel.edu/uhc/ (accessed on 2 June 2020).
- US Census Bureau. American Community Survey 5-Year Estimates. Available online: https://data.census.gov/all?q=american+community+survey+5-year (accessed on 1 December 2022).
- School District of Philadelphia. School Selection. Available online: https://www.philasd.org/studentplacement/services/school-selection/ (accessed on 19 August 2022).
- Bronfenbrenner, U. Toward an experimental ecology of human development. Am. Psychol. 1977, 32, 513–531. [Google Scholar] [CrossRef]
- Kaplan, G.A. What is the role of the social environment in understanding inequalities in health? Ann. N. Y. Acad. Sci. 1999, 896, 116–119. [Google Scholar] [CrossRef]
- US Department of Education. Promise Neighborhoods Program—Implementation Grant Competition; US Department of Education: Washington, DC, USA, 2016; Volume 81.
- Carroll-Scott, A. Importance of a place-based and community-moderated system of research oversight to maximize benefits for social change. Soc. Innov. J. 2020, 2. Available online: https://socialinnovationsjournal.com/index.php/sij/article/view/435 (accessed on 4 January 2023).
- Corbie-Smith, G.; Thomas, S.B.; Williams, M.V.; Moody-Ayers, S. Attitudes and beliefs of African Americans toward participation in medical research. J. Gen. Intern. Med. 1999, 14, 537–546. [Google Scholar] [CrossRef] [PubMed]
- Scharff, D.P.; Mathews, K.J.; Jackson, P.; Hoffsuemmer, J.; Martin, E.; Edwards, D. More than Tuskegee: Understanding mistrust about research participation. J. Health Care Poor Underserved 2010, 21, 879–897. [Google Scholar] [CrossRef] [PubMed]
- Ashley, F. Accounting for research fatigue in research ethics. Bioethics 2021, 35, 270–276. [Google Scholar] [CrossRef]
- Clark, T. We’re over-researched here!: Exploring accounts of research fatigue within qualitative research engagements. Sociology 2008, 42, 953–970. [Google Scholar] [CrossRef]
- Dart, J. Place-Based Evaluation Framework A Guide for Evaluation of Place-Based Approaches in Australia; Commissioned by the Queensland Government Department of Communities; Disability Services and Seniors (DCDSS) and the Australian Government Department of Social Services (DSS): Cremorne, VIC, Australia, 2018.
- OpenDataPhilly. Available online: https://www.opendataphilly.org/ (accessed on 1 June 2022).
- West Philly Promise Neighborhood Data & Research Core. West Philly Promise Neighborhood: Neighborhood Indicators. Available online: https://westphillypn.org/how-we-measure-success/neighborhood-indicators (accessed on 6 June 2022).
- The School District of Philadelphia Office of Research and Evaluation. District-Wide Surveys. Available online: https://www.philasd.org/research/programsservices/district-wide-surveys/ (accessed on 6 June 2022).
- Jannetti, M.; Carroll-Scott, A.; Gilliam, E.; Headen, I.; Beverly, M.; Le-Scherban, F. Improving sampling probability definitions with predictive algorithms. Field Methods 2022, 35, 1525822X2211131. [Google Scholar] [CrossRef]
- Actionable Intelligence for Social Policy. Integrated Data Systems (IDS). Available online: https://www.aisp.upenn.edu/integrated-data-systems/ (accessed on 3 March 2020).
- Culhane, D.; Fantuzzo, J.; Hill, M.; Burnett, T. Maximizing the use of integrated data systems: Understanding the challenges and advancing solutions. Ann. Am. Acad. Political Soc. Sci. 2018, 675, 221–239. [Google Scholar] [CrossRef]
- The Annie E. Casey Foundation. An Introduction to Integrated Data Systems. Available online: https://www.aecf.org/blog/watch-it-now-an-introduction-to-integrated-data-systems/ (accessed on 3 March 2020).
- Fantuzzo, J.; Henderson, C.; Coe, K.; Culhane, D. The Integrated Data System Approach: A Vehicle to More Effective and Efficient Data-Driven Solutions in Government; Actionable Intelligence for Social Policy, University of Pennsylvania: Philadelphia, PA, USA, 2017. [Google Scholar]
- City of Philadelphia. Community Schools. Available online: https://www.phila.gov/programs/community-schools/ (accessed on 9 March 2023).
- Lebrun-Harris, L.A.; Ghandour, R.M.; Kogan, M.D.; Warren, M.D. Five-year trends in US children’s health and well-being, 2016–2020. JAMA Pediatr. 2022, 176, e220056. [Google Scholar] [CrossRef]
- Treviño, E.; Miranda, C.; Hernández, M.; Villalobos, C. Socioeconomic status, parental involvement and implications for subjective well-being during the global pandemic of COVID-19. Front. Educ. 2021, 6, 762780. [Google Scholar] [CrossRef]
- Lee, E.K.; Parolin, Z. The care burden during COVID-19: A national database of child care closures in the United States. Socius 2021, 7, 23780231211032028. [Google Scholar] [CrossRef]
- West Philly Promise Neighborhood. What We’re Learning. Available online: https://westphillypn.org/what-we-re-learning (accessed on 22 June 2022).
- Muir, K.; Katz, I.; Edwards, B.; Gray, M.; Wise, S.; Hayes, A.; Stronger Families and Communities Strategy Evaluation Team. The national evaluation of the Communities for Children initiative. Fam. Matters 2010, 84, 35–42. [Google Scholar]
- Urban Health Collaborative. COVID-19 Vulnerability Indicators. Available online: https://drexel.edu/uhc/resources/coronavirus/vulnerability-indicators/ (accessed on 28 June 2022).
- Centers for Disease Control and Prevention/Agency for Toxic Substances and Disease Registry. CDC/ATSDR Social Vulnerability Index. Available online: https://www.atsdr.cdc.gov/placeandhealth/svi/index.html (accessed on 28 June 2022).



{kind=link}
{kind=link}
| Indicator Number | Description | Specific Measure(s) | Source |
|---|---|---|---|
| 1 | Medical home | % children aged 0–5 who have a place where they usually go, other than an emergency room, when they are sick or in need of advice about their health | Neighborhood survey |
| 2 | Kindergarten readiness | % 3-year-old children scoring above threshold on kindergarten readiness assessment | Early childhood education provider records |
| % kindergarteners scoring above threshold on kindergarten readiness assessment | School district records | ||
| % kindergarteners receiving intensive reading support | School district records | ||
| 3 | Child care | % children aged <5 cared for outside of the home in a child care center or home care center | Neighborhood survey |
| 4 | Academic achievement | % students scoring above threshold on statewide Math assessment | School district records |
| % students scoring above threshold on statewide English Language Arts assessment | School district records | ||
| 5 | School attendance | Average daily attendance | School district records |
| % students absent at least 5% of school year | School district records | ||
| % students absent at least 10% of school year | School district records | ||
| 6 | High school graduation | High school graduation rate | School district records |
| 7 | Career readiness | % high school graduates enrolled in college within 18 months of graduation | School district records |
| % college enrollees completing college within 6 years | School district records | ||
| % students scoring above threshold on technical education exam | School district records | ||
| 8 | Physical activity | % students in grades 3–12 who report engaging in 60 min of physical activity daily | School survey |
| 9 | Fruit and vegetable consumption | % students in grades 3–12 who report eating 5+ servings of fruits and vegetables daily | School survey |
| 10 | Safety | % students in grades 3–12 who report feeling safe in and traveling to school | School survey |
| 11 | Student mobility | Student mobility rate | School district records |
| 12 | Parents read to young children | % caregivers who report reading to their 0–5-year-old children 3+ times per week | Neighborhood survey |
| 13 | Parents encourage older children to read | % caregivers who report encouraging their K-8th-grade children to read outside of school | Neighborhood survey |
| 14 | Parents talk about college and career with children | % caregivers who report talking to their 9–12th-grade children about college and career | Neighborhood survey |
| 15 | Digital access | % students in grades 3–12 who report having school and home access to internet and a computer | School survey |
| Academic Year | |||||
|---|---|---|---|---|---|
| Program Focus Area | 2017–2018 | 2018–2019 | 2019–2020 | 2020–2021 | 2021–2022 |
| School Climate | 4 | 4 | 8 | 4 | 4 |
| Educational Supports (Kindergarten-12) | 8 | 9 | 4 | 7 | 5 |
| College and Career | 1 | 2 | 5 | 5 | 3 |
| Out of School Time (OST) Education | 4 | 5 | 15 | 11 | 6 |
| Community Safety/Mobility | 1 | 1 | 3 | 2 | 0 |
| Family Supports | 3 | 3 | 6 | 5 | 3 |
| Healthy Food/Nutrition | 1 | 1 | 5 | 5 | 4 |
| Early Childhood Education | 2 | 2 | 2 | 2 | 2 |
| TOTAL | 24 | 27 | 48 | 41 | 27 |
| Indicator Number | Description | Specific Measure | 2018% | 2019/2020% | 2021% |
|---|---|---|---|---|---|
| 1 | Medical home | % children aged 0–5 who have a place where they usually go, other than an emergency room, when they are sick or in need of advice about their health | 92.2 | 91.7 | 91.9 |
| 3 | Child care | % children aged <5 cared for outside of the home in a child care center or home care center | 74.0 | 68.6 | 56.9 |
| 12 | Parents read to young children | % caregivers who report reading to their 0–5-year-old children 3+ times per week | 86.9 | 79.1 | 66.6 |
| 13 | Parents encourage older children to read | % caregivers who report encouraging their kingertarten-8th-grade children to read outside of school | 94.4 | 90.6 | 93.1 |
| 14 | Parents talk about college and career with children | % caregivers who report talking to their 9–12th-grade children about college and career | 70.2 | 66.4 | 63.9 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lê-Scherban, F.; Headen, I.; Klem, A.M.; Traister, K.; Gilliam, E.; Beverly, M.; Jannetti, M.; Ferroni, J.; Carroll-Scott, A. Research and Evaluation in a Child-Focused Place-Based Initiative: West Philly Promise Neighborhood. Int. J. Environ. Res. Public Health 2023, 20, 5716. https://doi.org/10.3390/ijerph20095716
Lê-Scherban F, Headen I, Klem AM, Traister K, Gilliam E, Beverly M, Jannetti M, Ferroni J, Carroll-Scott A. Research and Evaluation in a Child-Focused Place-Based Initiative: West Philly Promise Neighborhood. International Journal of Environmental Research and Public Health. 2023; 20(9):5716. https://doi.org/10.3390/ijerph20095716
Chicago/Turabian StyleLê-Scherban, Félice, Irene Headen, Adena M. Klem, Kelley Traister, Erikka Gilliam, Maggie Beverly, Matthew Jannetti, Joanne Ferroni, and Amy Carroll-Scott. 2023. "Research and Evaluation in a Child-Focused Place-Based Initiative: West Philly Promise Neighborhood" International Journal of Environmental Research and Public Health 20, no. 9: 5716. https://doi.org/10.3390/ijerph20095716
APA StyleLê-Scherban, F., Headen, I., Klem, A. M., Traister, K., Gilliam, E., Beverly, M., Jannetti, M., Ferroni, J., & Carroll-Scott, A. (2023). Research and Evaluation in a Child-Focused Place-Based Initiative: West Philly Promise Neighborhood. International Journal of Environmental Research and Public Health, 20(9), 5716. https://doi.org/10.3390/ijerph20095716