

Social Connectedness and Smoking among Adolescents in Ireland: An Analysis of the Health Behaviour in Schoolchildren Study


Abstract
1. Introduction
2. Materials and Methods
2.1. Sample
2.2. Measures
2.3. Analysis
3. Results
3.1. Profile of Respondents
3.2. Overall Patterns of Smoking
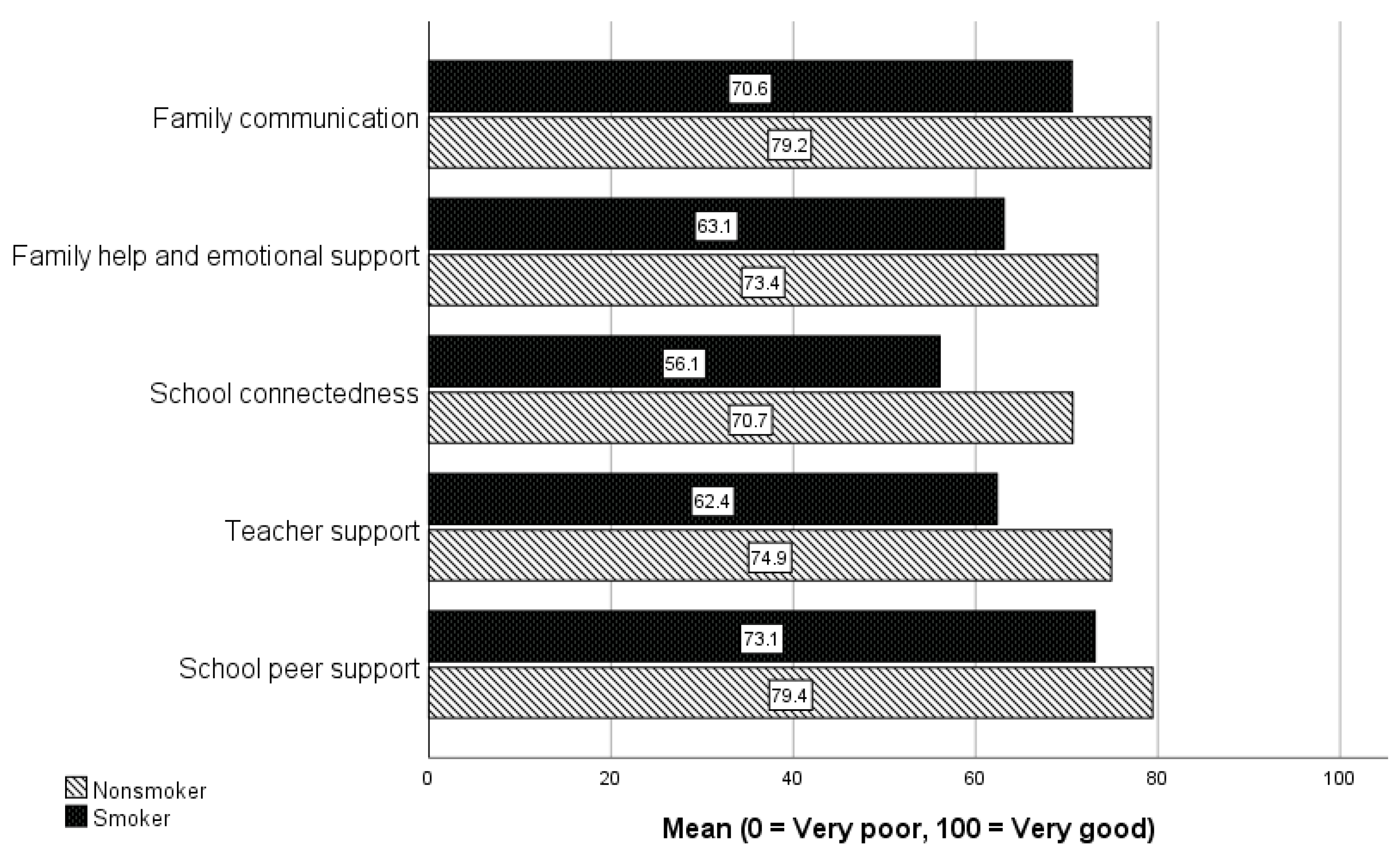
3.3. Family, School, Teacher, and Peer Scores
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mitic, M.; Woodcock, K.A.; Amering, M.; Krammer, I.; Stiehl, K.A.; Zehetmayer, S.; Schrank, B. Toward an integrated model of supportive peer relationships in early adolescence: A systematic review and exploratory meta-analysis. Front. Psychol. 2021, 12, 589403. [Google Scholar] [CrossRef]
- Polanska, K.; Znyk, M.; Kaleta, D. Susceptibility to tobacco use and associated factors among youth in five central and eastern European countries. BMC Public Health 2022, 22, 72. [Google Scholar] [CrossRef]
- Kashyap, S. Smoking Among Teenagers with Emphasis on Social Marketing as a Solution. Int. J. Res. Publ. Rev. 2021, 2, 964–968. [Google Scholar]
- Littlecott, H.; Moore, G.; Melendez-Torres, G.; McCann, M.; Reed, H.; Mann, M.; Dobbie, F.; Jennings, S.; Donaldson, C.; Hawkins, J. Perceptions of friendship, peers and influence on adolescent smoking according to tobacco control context: A systematic review and meta-ethnography of qualitative research. BMC Public Health 2022, 23, 424. [Google Scholar] [CrossRef] [PubMed]
- Phetphum, C.; Prajongjeep, A.; Youngiam, W.; Thawatchaijareonying, K. Susceptibility to smoking and determinants among never-smoking high school students in Thailand. Tob. Induc. Dis. 2023, 21, 83. [Google Scholar] [CrossRef]
- Birge, M.; Duffy, S.; Miler, J.A.; Hajek, P. What proportion of people who try one cigarette become daily smokers? A meta-analysis of representative surveys. Nicotine Tob. Res. 2018, 20, 1427–1433. [Google Scholar] [CrossRef]
- Gallus, S.; Lugo, A.; Liu, X.; Behrakis, P.; Boffi, R.; Bosetti, C.; Carreras, G.; Chatenoud, L.; Clancy, L.; Continente, X. Who smokes in Europe? Data from 12 European countries in the TackSHS survey (2017–2018). J. Epidemiol. 2021, 31, 145–151. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.H.; Stommel, M.; Broman, C.; Raheb-Rauckis, C. Age of Smoking Initiation in Relation to Multiple Health Risk Factors among US Adult Smokers: National Health Interview Survey (NHIS) Data (2006–2018). Behav. Med. 2022, 1–8, online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Hamzeh, B.; Farnia, V.; Moradinazar, M.; Pasdar, Y.; Shakiba, E.; Najafi, F.; Alikhani, M. Pattern of cigarette smoking: Intensity, cessation, and age of beginning: Evidence from a cohort study in West of Iran. Subst. Abus. Treat. Prev. Policy 2020, 15, 83. [Google Scholar] [CrossRef]
- Pesce, G.; Marcon, A.; Calciano, L.; Perret, J.L.; Abramson, M.J.; Bono, R.; Bousquet, J.; Fois, A.G.; Janson, C.; Jarvis, D. Time and age trends in smoking cessation in Europe. PLoS ONE 2019, 14, e0211976. [Google Scholar] [CrossRef]
- Puljević, C.; Morphett, K.; Hefler, M.; Edwards, R.; Walker, N.; Thomas, D.P.; Khan, M.A.; Perusco, A.; Le Grande, M.; Cullerton, K. Closing the gaps in tobacco endgame evidence: A scoping review. Tob. Control 2022, 31, 365–375. [Google Scholar] [CrossRef] [PubMed]
- Department of Health. Tobacco Free Ireland, Report of the Tobacco Policy Review Group; Department of Health: Dublin, Ireland, 2013. [Google Scholar]
- Sunday, S.; Hanafin, J.; Clancy, L. Increased smoking and e-cigarette use among Irish teenagers: A new threat to Tobacco Free Ireland 2025. ERJ Open Res. 2021, 7, 00438-2021. [Google Scholar] [CrossRef] [PubMed]
- Haslam, C.; Cruwys, T.; Haslam, S.A.; Jetten, J. Social connectedness and health. In Encyclopedia of Geropsychology; Springer: Berlin/Heidelberg, Germany, 2015. [Google Scholar]
- Wickramaratne, P.J.; Yangchen, T.; Lepow, L.; Patra, B.G.; Glicksburg, B.; Talati, A.; Adekkanattu, P.; Ryu, E.; Biernacka, J.M.; Charney, A. Social connectedness as a determinant of mental health: A scoping review. PLoS ONE 2022, 17, e0275004. [Google Scholar] [CrossRef] [PubMed]
- Butler, N.; Quigg, Z.; Bates, R.; Jones, L.; Ashworth, E.; Gowland, S.; Jones, M. The contributing role of family, school, and peer supportive relationships in protecting the mental wellbeing of children and adolescents. Sch. Ment. Health 2022, 14, 776–788. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Health for the World’s Adolescents: A Second Chance in the Second Decade: Summary; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- World Health Organization. Helping Adolescents Thrive Toolkit: Strategies to Promote and Protect Adolescent Mental Health and Reduce Self-Harm and Other Risk Behaviours; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Holubčíková, J.; Kudláček, M.; Širůček, J.; Madarasová Gecková, A. Test-retest reliability of selected HBSC items measuring problem behaviour among Slovak and Czech adolescents. Cent. Eur. J. Public Health 2018, 26, 204–208. [Google Scholar] [CrossRef]
- Kohoutek, J.; Maráček, M.; Ng, K.; Hamrik, Z. Test–retest reliability of selected HBSC items in Vietnam: Well-being, physical and sedentary activities, and eating behaviours. BMC Med. Res. Methodol. 2022, 22, 135. [Google Scholar] [CrossRef]
- Currie, C.; Nic Gabhainn, S.; Godeau, E.; Committee, I.H.N.C. The Health Behaviour in School-aged Children: WHO Collaborative Cross-National (HBSC) study: Origins, concept, history and development 1982–2008. Int. J. Public Health 2009, 54, 131–139. [Google Scholar] [CrossRef]
- Kelly, C.; Gavin, A.; Molcho, M.; Nic Gabhainn, S. The Irish Health Behaviour in School-Aged Children (HBSC) Study 2010; National University of Ireland, Galway and Department of Health, Government of Ireland: Dublin, Ireland, 2012. [Google Scholar]
- Gavin, A.; Keane, E.; Callaghan, M.; Molcho, M.; Kelly, C.; Nic Gabhainn, S. The Irish Health Behaviour in School-Aged Children (HBSC) Study 2014; National University of Ireland, Galway and Department of Health, Government of Ireland: Dublin, Ireland, 2015. [Google Scholar]
- Central Statistics Office. Population Classified by Area; Government of Ireland: Dublin, Ireland, 2012. [Google Scholar]
- Mondschein, C.F.; Monda, C. The EU’s General Data Protection Regulation (GDPR) in a research context. In Fundamentals of Clinical Data Science; Springer: Berlin/Heidelberg, Germany, 2019; pp. 55–71. [Google Scholar]
- Central Statistics Office. Census of Population 1986: Classification of Occupations; Central Statistics Office: Cork, Ireland, 1986. [Google Scholar]
- Tabak, I.; Mazur, J. Social support and family communication as factors protecting adolescents against multiple recurrent health complaints related to school stress. Dev. Period Med. 2016, 20, 27–39. [Google Scholar]
- Lasky, P.; Buckwalter, K.C.; Whall, A.; Lederman, R.; Speer, J.; McLane, A.; King, J.M.; White, M.A.; Woods, N.F.; Rees, B.L. Developing an Instrument for the Assessment of Family Dynamics. West. J. Nurs. Res. 1985, 7, 40–57. [Google Scholar] [CrossRef]
- White, M.A.; Grzankowski, J.; Paavilainen, E.; Ãstedt-Kurki, P.i.; Paunonen-Ilmonen, M. Family Dynamics and Child Abuse and Neglect in Three Finnish Communities. Issues Ment. Health Nurs. 2003, 24, 707–722. [Google Scholar] [CrossRef]
- Zimet, G.D.; Dahlem, N.W.; Zimet, S.G.; Farley, G.K. The Multidimensional Scale of Perceived Social Support. J. Personal. Assess. 1988, 52, 30–41. [Google Scholar] [CrossRef]
- Michaelson, V.; Pickett, W.; King, N.; Davison, C. Testing the theory of holism: A study of family systems and adolescent health. Prev. Med. Rep. 2016, 4, 313–319. [Google Scholar] [CrossRef]
- Rasmussen, M.; Damsgaard, M.T.; Holstein, B.r.E.; Poulsen, L.H.; Due, P. School connectedness and daily smoking among boys and girls: The influence of parental smoking norms. Eur. J. Public Health 2005, 15, 607–612. [Google Scholar] [CrossRef] [PubMed]
- McNeely, C.; Falci, C. School Connectedness and the Transition Into and Out of Health-Risk Behavior Among Adolescents: A Comparison of Social Belonging and Teacher Support. J. Sch. Health 2004, 74, 284–292. [Google Scholar] [CrossRef] [PubMed]
- Brown, R.; Evans, W.P. Extracurricular Activity and Ethnicity:Creating Greater School Connection among Diverse Student Populations. Urban Educ. 2002, 37, 41–58. [Google Scholar] [CrossRef]
- Thompson, D.R.; Iachan, R.; Overpeck, M.; Ross, J.G.; Gross, L.A. School Connectedness in the Health Behavior in School-Aged Children Study: The Role of Student, School, and School Neighborhood Characteristics. J. Sch. Health 2006, 76, 379–386. [Google Scholar] [CrossRef]
- Walsh, S.D.; Harel-Fisch, Y.; Fogel-Grinvald, H. Parents, teachers and peer relations as predictors of risk behaviors and mental well-being among immigrant and Israeli born adolescents. Soc. Sci. Med. 2010, 70, 976–984. [Google Scholar] [CrossRef] [PubMed]
- McLellan, L.; Rissel, C.E.; Donnelly, N.; Bauman, A.E. Health behaviour and the school environment in New South Wales, Australia. Soc. Sci. Med. 1999, 49, 611–619. [Google Scholar] [CrossRef]
- Moore, G.F.; Cox, R.; Evans, R.E.; Hallingberg, B.; Hawkins, J.; Littlecott, H.J.; Long, S.J.; Murphy, S. School, Peer and Family Relationships and Adolescent Substance Use, Subjective Wellbeing and Mental Health Symptoms in Wales: A Cross Sectional Study. Child Indic. Res. 2018, 11, 1951–1965. [Google Scholar] [CrossRef]
- Erginoz, E.; Alikasifoglu, M.; Ercan, O.; Uysal, O.; Alp, Z.; Ocak, S.; Oktay Tanyildiz, G.; Ekici, B.; Yucel, I.K.; Albayrak Kaymak, D. The Role of Parental, School, and Peer Factors in Adolescent Bullying Involvement:Results From the Turkish HBSC 2005/2006 Study. Asia Pac. J. Public Health 2015, 27, NP1591–NP1603. [Google Scholar] [CrossRef]
- The HBSC Ireland Team. Smoking Behaviour among Schoolchildren in Ireland, HBSC Ireland 2014, Research Factsheet 1; The HBSC Ireland Team: Galway, Ireland, 2016. [Google Scholar]
- Ipsos MRBI. Healthy Ireland Survey 2021, Summary of Findings; The Stationary Office: Dublin, Ireland, 2021. [Google Scholar]
- O’Brien, D.; Long, J.; Quigley, J.; Lee, C.; McCarthy, A.; Kavanagh, P. Association between electronic cigarette use and tobacco cigarette smoking initiation in adolescents: A systematic review and meta-analysis. BMC Public Health 2021, 21, 954. [Google Scholar] [CrossRef]
- Inchley, J.; Currie, D.; Young, T. Growing up Unequal: Gender and Socioeconomic Differences in Young People’s Health and Well-Being. Health Behaviour in School-Aged Children (HBSC) Study: International Report from the 2013/2014 Survey; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Oliver, J.A.; Foulds, J. Association between cigarette smoking frequency and tobacco use disorder in US adults. Am. J. Prev. Med. 2021, 60, 726–728. [Google Scholar] [CrossRef]
- Chaarani, B.; Kan, K.-J.; Mackey, S.; Spechler, P.A.; Potter, A.; Orr, C.; D’Alberto, N.; Hudson, K.E.; Banaschewski, T.; Bokde, A.L. Low smoking exposure, the adolescent brain, and the modulating role of CHRNA5 polymorphisms. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 2019, 4, 672–679. [Google Scholar] [CrossRef] [PubMed]
- Roditis, M.; Lee, J.; Halpern-Felsher, B.L. Adolescent (mis) perceptions about nicotine addiction: Results from a mixed-methods study. Health Educ. Behav. 2016, 43, 156–164. [Google Scholar] [CrossRef]
- Pförtner, T.-K.; De Clercq, B.; Lenzi, M.; Vieno, A.; Rathmann, K.; Moor, I.; Hublet, A.; Molcho, M.; Kunst, A.E.; Richter, M. Does the association between different dimension of social capital and adolescent smoking vary by socioeconomic status? A pooled cross-national analysis. Int. J. Public Health 2015, 60, 901–910. [Google Scholar] [CrossRef] [PubMed]
- Zaborskis, A.; Sirvyte, D. Familial determinants of current smoking among adolescents of Lithuania: A cross-sectional survey 2014. BMC Public Health 2015, 15, 889. [Google Scholar] [CrossRef]
- Zaborskis, A.; Kavaliauskienė, A.; Eriksson, C.; Klemera, E.; Dimitrova, E.; Melkumova, M.; Husarova, D. Family support as smoking prevention during transition from early to late adolescence: A study in 42 countries. Int. J. Environ. Res. Public Health 2021, 18, 12739. [Google Scholar] [CrossRef]
- Arunachalam, D.; Nguyen, D.Q.V. Family connectedness, school attachment, peer influence and health-compromising behaviours among young Vietnamese males. J. Youth Stud. 2016, 19, 287–304. [Google Scholar] [CrossRef]
- Gervais, C.; Jose, P.E. How does family connectedness contribute to youths’ health? The mediating role of coping strategies. Fam. Process 2020, 59, 1627–1647. [Google Scholar] [CrossRef]
- Oztekin, C.; Batra, M.; Abdelsalam, S.; Sengezer, T.; Ozkara, A.; Erbas, B. Impact of individual, familial and parental factors on adolescent smoking in Turkey. Int. J. Environ. Res. Public Health 2021, 18, 3740. [Google Scholar] [CrossRef]
- Sanders, M.R. Developing the Triple P System as a Population Approach to Parenting Support. In Designing Evidence-Based Public Health and Prevention Programs; Routledge: London, UK, 2020; pp. 92–112. [Google Scholar]
- Sanders, M.R.; Kirby, J.N.; Tellegen, C.L.; Day, J.J. The Triple P-Positive Parenting Program: A systematic review and meta-analysis of a multi-level system of parenting support. Clin. Psychol. Rev. 2014, 34, 337–357. [Google Scholar] [CrossRef]
- Allen, M.L.; Garcia-Huidobro, D.; Porta, C.; Curran, D.; Patel, R.; Miller, J.; Borowsky, I. Effective parenting interventions to reduce youth substance use: A systematic review. Pediatrics 2016, 138, e20154425. [Google Scholar] [CrossRef] [PubMed]
- Ladis, B.A.; Macgowan, M.; Thomlison, B.; Fava, N.M.; Huang, H.; Trucco, E.M.; Martinez, M.J. Parent-focused preventive interventions for youth substance use and problem behaviors: A systematic review. Res. Soc. Work Pract. 2019, 29, 420–442. [Google Scholar] [CrossRef]
- Hutchings, J.; Owen, D.; Williams, M. Web-based parenting support: Development of the COPING confident parenting programme. Educ. Sci. 2018, 8, 59. [Google Scholar] [CrossRef]
- Aho, H.; Konu, A.; Koivisto, A.-M.; Joronen, K. Relationship among School Connectedness, Smoking Policy, and Smoking Behavior in Finnish Vocational Schools. Health Behav. Policy Rev. 2019, 6, 56–70. [Google Scholar] [CrossRef]
- Gaete, J.; Ortúzar, C.; Zitko, P.; Montgomery, A.; Araya, R. Influence of school-related factors on smoking among Chilean adolescents: A cross-sectional multilevel study. BMC Pediatr. 2016, 16, 79. [Google Scholar] [CrossRef]
- Rose, I.D.; Lesesne, C.A.; Sun, J.; Johns, M.M.; Zhang, X.; Hertz, M. The Relationship of School Connectedness to Adolescents’ Engagement in Co-Occurring Health Risks: A Meta-Analytic Review. J. Sch. Nurs. 2022. [Google Scholar] [CrossRef]
- Shackleton, N.; Jamal, F.; Viner, R.M.; Dickson, K.; Patton, G.; Bonell, C. School-based interventions going beyond health education to promote adolescent health: Systematic review of reviews. J. Adolesc. Health 2016, 58, 382–396. [Google Scholar] [CrossRef]
- Rowe, F.; Stewart, D. Promoting connectedness through whole-school approaches: A qualitative study. Health Educ. 2009, 109, 396–413. [Google Scholar] [CrossRef]
- World Health Organization. Making Every School a Health-Promoting School: Implementation Guidance; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Carrington, S.B.; Saggers, B.R.; Shochet, I.M.; Orr, J.A.; Wurfl, A.M.; Vanelli, J.; Nickerson, J. Researching a whole school approach to school connectedness. Int. J. Incl. Educ. 2021, 1–18. [Google Scholar] [CrossRef]
- Bower, J.; van Kraayenoord, C.; Carroll, A. Building social connectedness in schools: Australian teachers’ perspectives. Int. J. Educ. Res. 2015, 70, 101–109. [Google Scholar] [CrossRef]
- O’Donnell, M.; Gavin, A.; Nic Gabhainn, S. HBSC Ireland 2018 Research Factsheet 1 Smoking Behaviour among Schoolchildren in Ireland; Health Promotion Research Centre, NUI Galway: Galway, Ireland, 2021. [Google Scholar]
- Freeman, J.; King, M.; Kuntsche, E.; Pickett, W. Protective roles of home and school environments for the health of young Canadians. J. Epidemiol. Community Health 2011, 65, 438–444. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Wang, M.; Tynjälä, J.; Lv, Y.; Villberg, J.; Zhang, Z.; Kannas, L. Test-retest reliability of selected items of Health Behaviour in School-aged Children (HBSC) survey questionnaire in Beijing, China. BMC Med. Res. Methodol. 2010, 10, 73. [Google Scholar] [CrossRef] [PubMed]
- Bowe, A.K.; Doyle, F.; Stanistreet, D.; O’Connell, E.; Durcan, M.; Major, E.; O’Donovan, D.; Kavanagh, P. E-cigarette-only and dual use among adolescents in Ireland: Emerging behaviours with different risk profiles. Int. J. Environ. Res. Public Health 2021, 18, 332. [Google Scholar] [CrossRef]


{kind=link}
| Smoker | Non-Smoker | Effect Size | Statistical Significance (Independent t Test) | |||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | (Cohen’s d) | ||
| Family communication (lower score = better communication) | 9.9 | 4.05 | 8.2 | 3.0 | 3.125, CI = −0.630–−0.478 | t = −11.541, df = 807.7, p < 0.001 |
| Family help and emotional support (higher score = better help and emotional support) | 17.7 | 7.9 | 20.6 | 7.8 | 7.845, CI = 0.289–0.443 | t = 9.365 df = 8996, p < 0.001 |
| Connectedness with school (lower score = better connectedness) | 13.0 | 3.4 | 10.1 | 3.1 | 3.107, CI = −1.014–−0.863 | t = −22.861, df = 872, p < 0.001 |
| Teacher support (lower score = better support) | 11.5 | 3.9 | 9.0 | 3.3 | 3.339, CI = −0.825–−0.675 | t = −17.258, df = 852.5, p < 0.001 |
| Supportiveness of school peers (lower score = better support) | 7.0 | 2.5 | 6.1 | 2.1 | 2.127, CI = −0.519–0.371 | t = −10.309, df = 871.1, p < 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Evans, D.S.; O’Farrell, A.; Sheridan, A.; Kavanagh, P. Social Connectedness and Smoking among Adolescents in Ireland: An Analysis of the Health Behaviour in Schoolchildren Study. Int. J. Environ. Res. Public Health 2023, 20, 5667. https://doi.org/10.3390/ijerph20095667
Evans DS, O’Farrell A, Sheridan A, Kavanagh P. Social Connectedness and Smoking among Adolescents in Ireland: An Analysis of the Health Behaviour in Schoolchildren Study. International Journal of Environmental Research and Public Health. 2023; 20(9):5667. https://doi.org/10.3390/ijerph20095667
Chicago/Turabian StyleEvans, David S., Anne O’Farrell, Aishling Sheridan, and Paul Kavanagh. 2023. "Social Connectedness and Smoking among Adolescents in Ireland: An Analysis of the Health Behaviour in Schoolchildren Study" International Journal of Environmental Research and Public Health 20, no. 9: 5667. https://doi.org/10.3390/ijerph20095667
APA StyleEvans, D. S., O’Farrell, A., Sheridan, A., & Kavanagh, P. (2023). Social Connectedness and Smoking among Adolescents in Ireland: An Analysis of the Health Behaviour in Schoolchildren Study. International Journal of Environmental Research and Public Health, 20(9), 5667. https://doi.org/10.3390/ijerph20095667