
Knowledge of Obstetric Danger Signs among Pregnant Women in the Eastern Democratic Republic of the Congo

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Setting
2.3. Study Population and Sampling
2.4. Sampling
2.4.1. Sample Size
2.4.2. Sampling Technique
2.5. Data Collection Techniques
2.6. Study Variables
2.6.1. Definition of Variables
2.6.2. Operational Definitions of the Variables
2.7. Data Collection Tool
2.8. Data Analysis
2.9. Ethical Considerations
3. Results
3.1. Description of the Population
3.2. Sociodemographic and Clinical Characteristics of the Respondents
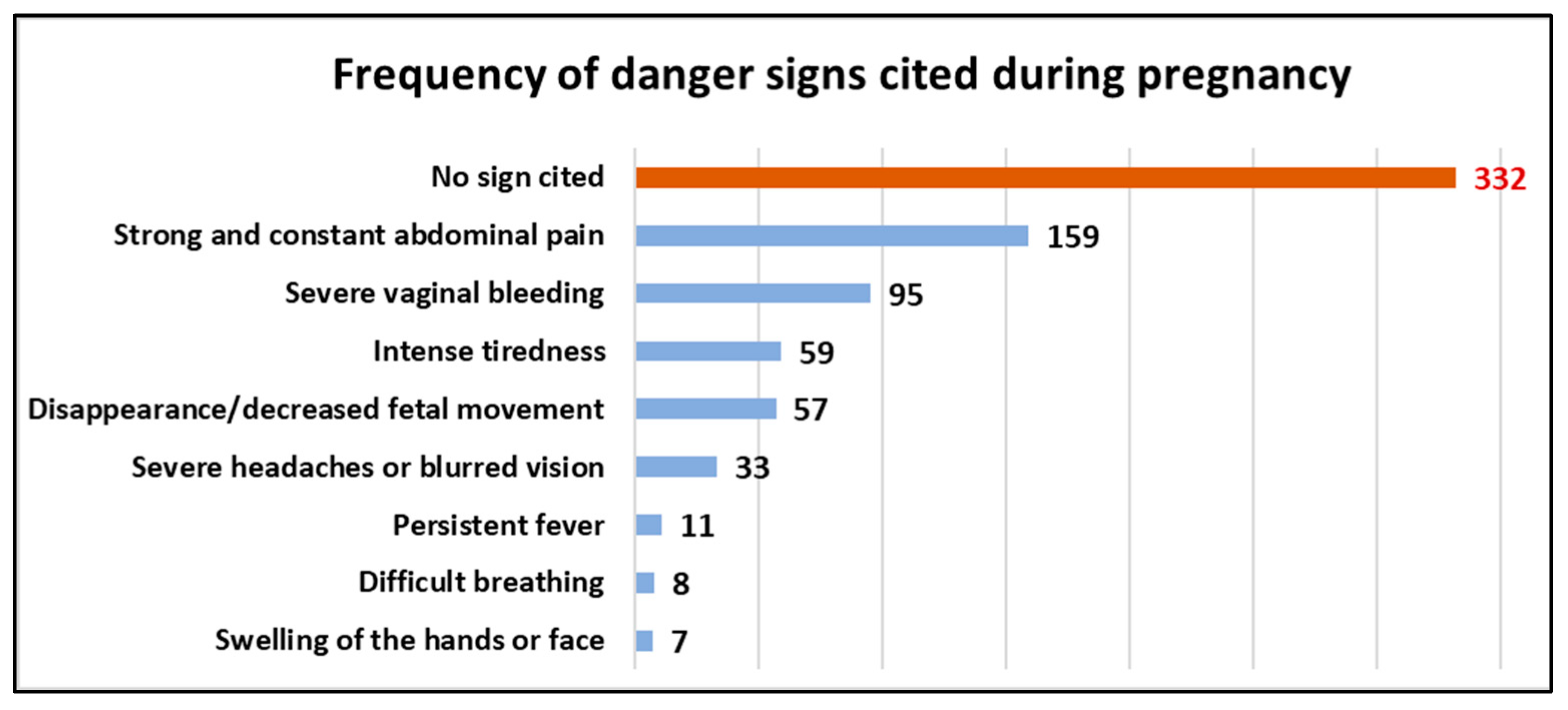
3.3. Frequency of ODS Cited during Pregnancy (Antepartum)
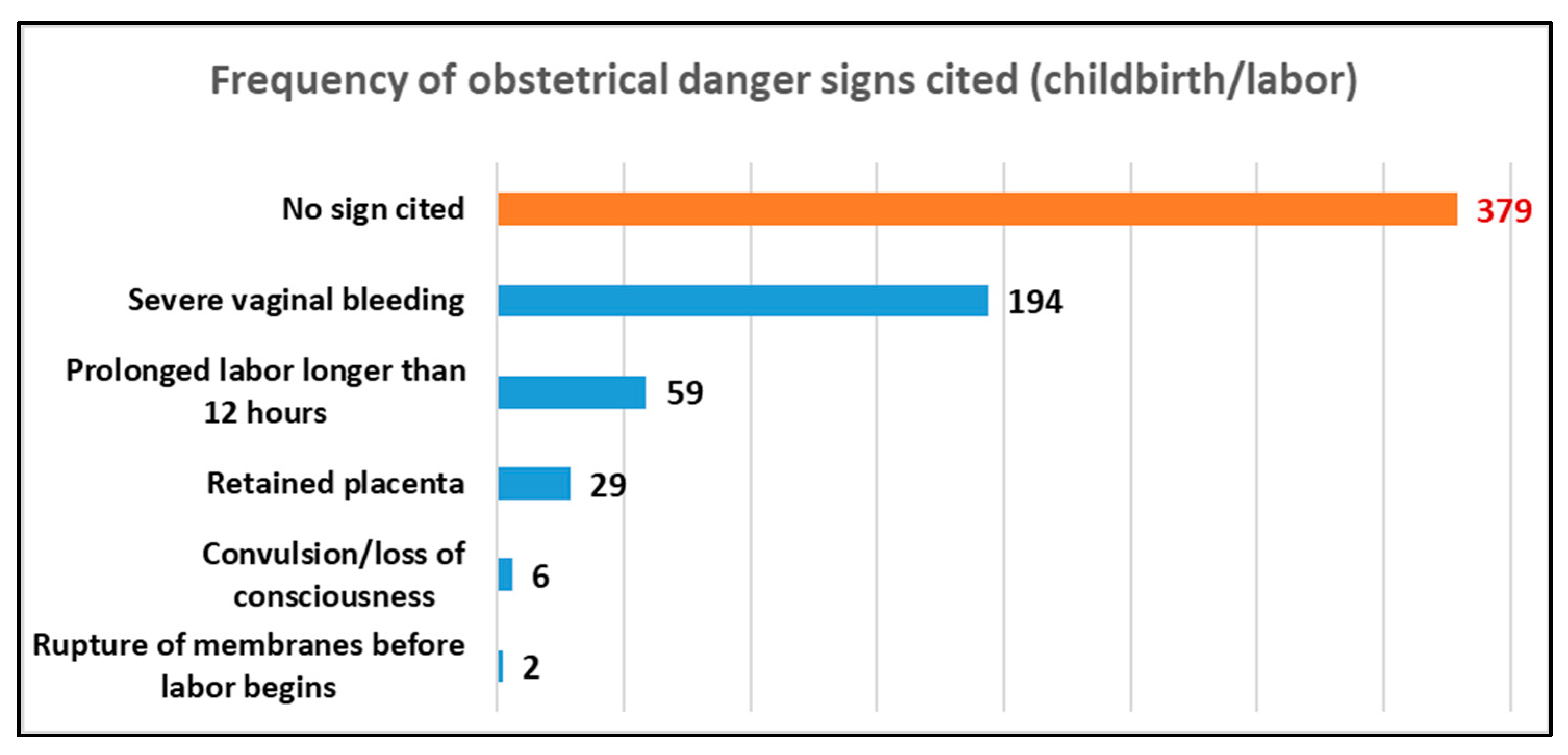
3.4. Frequent ODS Cited during Labor or Delivery (Peripartum)
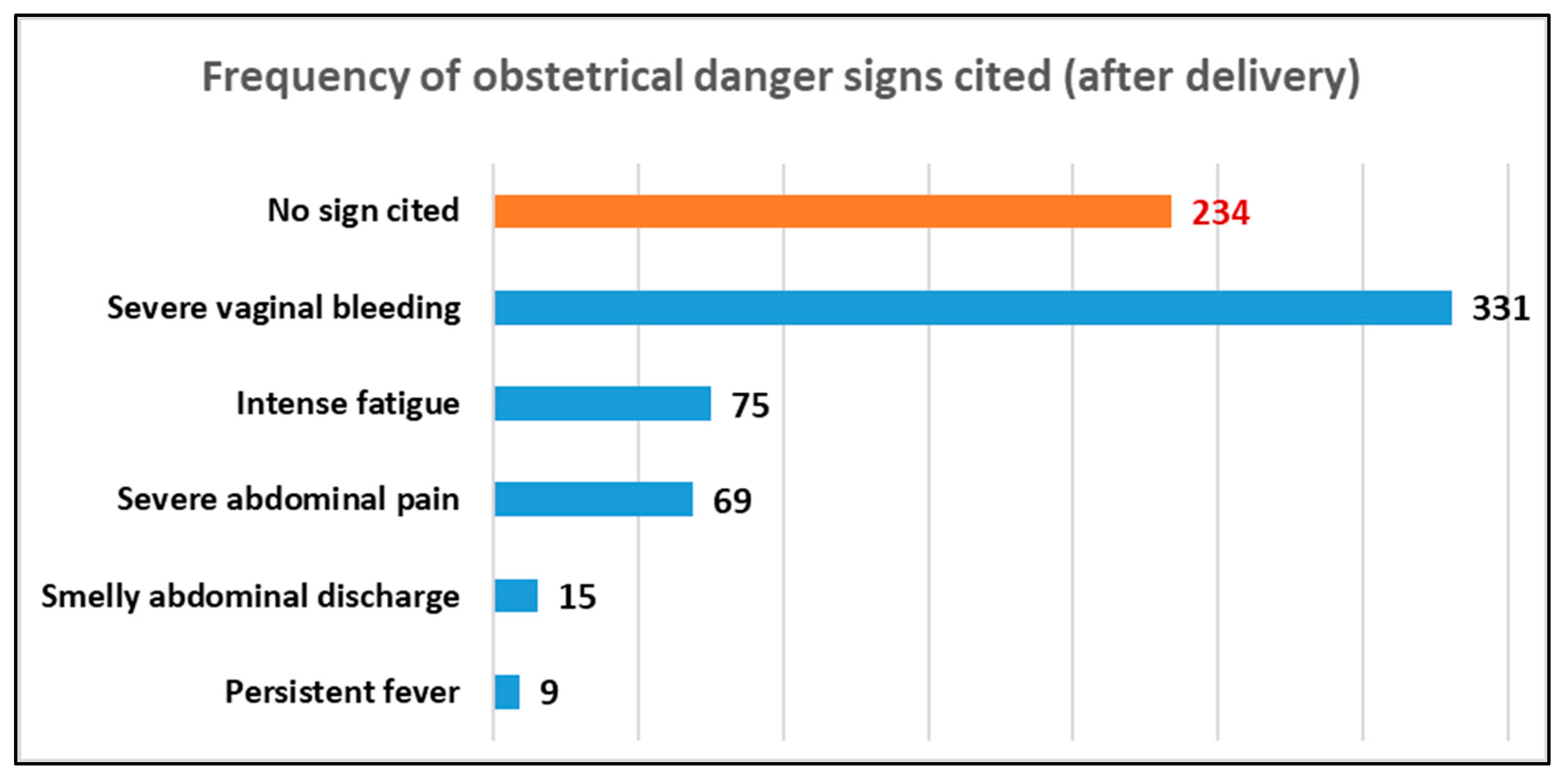
3.5. Frequency of ODS Cited after Delivery (Postpartum)
4. Discussion
4.1. Knowledge of ODS among Women
4.2. ODS Most Cited by Respondents
4.3. ODS Least Cited by Respondents
4.4. Factors Associated with the Knowledge of ODS among Pregnant Women
4.5. Knowledge of ODS and Respondents’ Education Levels
4.6. Knowledge of ODS and ANC Follow-Up
4.7. Knowledge of ODS and Parity of Respondents
4.8. Strengths and Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ANC | antenatal consultation |
| ODS | obstetric danger signs |
| DRC | Democratic Republic of the Congo |
| HZ | health zone |
| WHO | World Health Organization |
References
- Bintabara, D.; Mpembeni, R.N.M.; Mohamed, A.A. Knowledge of obstetric danger signs among recently delivered women in Chamwino district, Tanzania: A cross-sectional study. BMC Pregnancy Childbirth 2017, 17, 276. [Google Scholar] [CrossRef] [PubMed]
- Nkamba, D.M.; Wembodinga, G.; Bernard, P.; Ditekemena, J.; Robert, A. Awareness of obstetric danger signs among pregnant women in the Democratic Republic of Congo: Evidence from a nationwide cross-sectional study. BMC Women’s Health 2021, 21, 82. [Google Scholar] [CrossRef] [PubMed]
- Ngom, N.F. Medical Assistance-Delivery in Senegal. Ph.D. Thesis, Montesquieu University, Bordeaux, France, 2016. Available online: http://www.theses.fr/2016BORD0432 (accessed on 31 March 2020).
- World Health Organization; United Nations Children’s Fund; United Nations Population Fund World Bank Group and the United Nations Population Division. Trends in Maternal Mortality: 1990 to 2015; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Vijay, N.R.; Kumare, B.; Yerlekar, D.S. Awareness of obstetric danger signs among pregnant women in tertiary care teaching hospital. J. South Asian Fed. Obstet. Gynaecol. 2015, 7, 171. [Google Scholar]
- Woldeamanuel, G.G.; Lemma, G.; Zegeye, B. Knowledge of obstetric danger signs and its associated factors among pregnant women in Angolela Tera District, Northern Ethiopia. BMC Res. Notes 2019, 12, 606. [Google Scholar] [CrossRef]
- Bolanko, A.; Namo, H.; Minsamo, K.; Addisu, N.; Gebre, M. Knowledge of obstetric danger signs and associated factors among pregnant women in Wolaita Sodo town, South Ethiopia: A community-based cross-sectional study. SAGE Open Med. 2021, 9, 20503121211001160. [Google Scholar] [CrossRef]
- Wassihun, B.; Negese, B.; Bedada, H.; Bekele, S.; Bante, A.; Yeheyis, T.; Abebe, A.; Uli, D.; Mohammed, M.; Gashawbez, S.; et al. Knowledge of obstetric danger signs and associated factors: A study among mothers in Shashamane town, Oromia region, Ethiopia. Reprod. Health 2020, 17, 4. [Google Scholar] [CrossRef]
- Bazant, E.; Rakotovao, J.P.; Rasolofomanana, J.R.; Tripathi, V.; Gomez, P.; Favero, R.; Moffson, S. Quality of care to prevent and treat postpartum hemorrhage and preeclampsia/eclampsia: An observational assessment in hospitals in Madagascar. Trop. Med. Health 2013, 23, 168–175. [Google Scholar]
- Imaralu, J.O.; Ani, I.F.; Olaleye, A.O.; Jaiyesimi, E.; Afolabi-Imaralu, A.; Odugbemi, O.O. Maternal and perinatal outcomes of birth preparedness and complication readiness in recently delivered women of a Southwestern Nigerian town. Ann. Afr. Med. 2020, 19, 60. [Google Scholar] [CrossRef]
- Tarekegn, S.M.; Lieberman, L.S.; Giedraitis, V. Determinants of maternal health service utilization in Ethiopia: Analysis of the 2011 Ethiopian demographic and health survey. BMC Pregnancy Childbirth 2014, 14, 161. [Google Scholar] [CrossRef]
- Workineh, Y.; Hailu, D.; Gultie, T.; Degefu, N.; Mihrete, M.; Shimeles, M. Knowledge of obstetric danger signs and its associated factors in Arba Minch town, Ethiopia. Am. J. Health Res. 2014, 2, 255. [Google Scholar] [CrossRef]
- Yosef, T.; Tesfaye, M. Pregnancy danger signs: Knowledge and health-seeking behavior among reproductive age women in southwest Ethiopia. Womens Health 2021, 17, 17455065211063296. [Google Scholar] [CrossRef] [PubMed]
- Hibstu, D.T.; Siyoum, Y.D. Knowledge of obstetric danger signs and associated factors among pregnant women attending antenatal care at health facilities of Yirgacheffe town, Gedeo zone, Southern Ethiopia. Arch. Public Health 2017, 75, 35. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Recommendations on Intrapartum Care for a Positive Childbirth Experience; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Mwilike, B.; Nalwadda, G.; Kagawa, M.; Malima, K.; Mselle, L.; Horiuchi, S. Knowledge of danger signs during pregnancy and subsequent healthcare seeking actions among women in urban Tanzania: A cross-sectional study. BMC Pregnancy Childbirth 2018, 18, 4. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Public Health. Democratic Republic of Congo. Ministry of Health. Bulletin N°2 of the Maternal Death Surveillance and Response (SDMR). 2018. Available online: https://www.afro.who.int/sites/default/files/2022-01/RAPPORT%20REVUE%20SRMNIA%202021%20DEF.pdf (accessed on 27 July 2021).
- Ramazani, I.B.E.; Ntela, S.M.; Ahouah, M.; Ishoso, D.K.; Monique, R.T. Maternal mortality study in the Eastern Democratic Republic of the Congo. BMC Pregnancy Childbirth 2022, 22, 452. [Google Scholar] [CrossRef]
- DRC/MINISANTE. Compendium of Norms for the Organization and Operation of Health Structures in the Health Zone in the DRC; DRC/MINISANTE: Kinshasa, Democratic Republic of the Congo, 2006. [Google Scholar]
- Maniema Provincial Health Division. Populations of the Health Areas of the Province of Maniema; Maniema Provincial Health Division: Kindu, Democratic Republic of the Congo, 2020. [Google Scholar]
- Bililign, N.; Mulatu, T. Knowledge of obstetric danger signs and associated factors among reproductive age women in raya Kobo district of Ethiopia: A community based cross-sectional study. BMC Pregnancy Childbirth 2017, 17, 70. [Google Scholar] [CrossRef]
- Actis Danna, V.; Bedwell, C.; Wakasiaka, S.; Lavender, T. Utility of the three-delays model and its potential for supporting a solution-based approach to accessing intrapartum care in low- and middle-income countries. A qualitative evidence synthesis. Glob. Health Action 2020, 13, 1819052. [Google Scholar] [CrossRef]
- Cox, N.J. History of Stata. In Thirty Years with Stata: A Retrospective, 1st ed.; Pinzon, E., Ed.; A Stata Press Publication: College Station, TX, USA, 2015. [Google Scholar]
- Ossai, E.N.; Uzochukwu, B.S. Knowledge of danger signs of pregnancy among clients of maternal health service in urban and rural primary health centres of Southeast Nigeria. J. Community Med. Health Educ. 2015, 5, 337. [Google Scholar] [CrossRef]
- Okour, A.; Alkhateeb, M.; Amarin, Z. Awareness of danger signs and symptoms of pregnancy complication among women in Jordan. Int. J. Gynaecol. Obstet. 2012, 118, 11–14. [Google Scholar] [CrossRef]
- Hoque, M.; Hoque, M.E. Knowledge of danger signs for major obstetric complications among pregnant KwaZulu-Natal women: Implications for health education. Asia-Pac. J. Public Health 2011, 23, 946. [Google Scholar] [CrossRef]
- Dangura, A.D. Knowledge about child birth and postpartum obstetric danger signs and associated factors among mothers in Dale district, Southern Ethiopia. BMC Pregnancy Childbirth 2020, 20, 340. [Google Scholar] [CrossRef]
- Congo, D.R. Determinants of late attendance at antenatal care services in the health zones of Equateur and Katanga in the Democratic Republic of the Congo. Ann. Afr. Med. 2011, 4, 845. [Google Scholar]
- Nigatu, S.G.; Worku, A.G.; Dadi, A.F. Level of mother’s knowledge about neonatal danger signs and associated factors in North West of Ethiopia: A community based study. BMC Res. Notes 2015, 8, 309. [Google Scholar] [CrossRef] [PubMed]
- Migliani, R.; Amat-Roze, J.M. Health situation in the Democratic Republic of the Congo in 2020. Herodotus 2020, 4, 146. [Google Scholar]
- Mbalinda, S.N.; Nakimuli, A.; Kakaire, O.; Osinde, M.O.; Kakande, N.; Kaye, D.K. Does knowledge of danger signs of pregnancy predict birth preparedness? A critique of the evidence from women admitted with pregnancy complications. Health Res. Policy Syst. 2014, 12, 60. [Google Scholar] [CrossRef] [PubMed]
- Hamad, K.K. The Association between Antenatal Attendance and Knowledge on Obstetric Danger Signs among Postnatal Mothers in Zanzibar: A Community Based Cross-Sectional Study. 2019. Available online: http://repository.udom.ac.tz/handle/20.500.12661/2054 (accessed on 9 December 2021).
- Kare, A.P.; Gujo, A.B.; Yote, N.Y. Quality of antenatal care and associated factors among pregnant women attending government hospitals in Sidama region, Southern Ethiopia. SAGE Open Med. 2021, 9, 20503121211058055. Available online: https://pubmed.ncbi.nlm.nih.gov/34868590/ (accessed on 17 April 2023). [CrossRef]
- Ministry of Public Health. National Health Development Plan/PNDS 2016–2020; General Secretariat of Health, Kinshasa, Democratic Republic of the Congo: Kinshasa, Democratic Republic of the Congo, 2016.




{kind=link}
{kind=link}
{kind=link}
| Variables | Definitions | Types | Modalities | Justifications |
|---|---|---|---|---|
| Sociodemographic characteristics | ||||
| Age | Age range of pregnant women aged 19–35 years | Continuous and categorical | ≤19 20–24 25–29 30–34 ≥35 | Can explain knowledge of ODS |
| Education level | Training courses attended by pregnant women: primary, secondary, or higher education or nothing at all | Categorical | Not in school Primary Secondary Higher | Can explain knowledge of ODS |
| Religion | Religious affiliation of the woman | Categorical | Muslim Catholic Protestant Kimbanguist Revival church Others, to be specified | Can explain knowledge of ODS |
| Marital status | Marital status of pregnant women who live in a union or alone | Categorical | Married Single Divorced Widowed | Can explain knowledge of ODS |
| Clinical characteristics | ||||
| Parity | Number of deliveries that the woman has experienced | Categorical | Primiparous (1 birth) Pauciparous (2–4 births) Multiparous (5–7 births) Grand multiparous (>7 births) | Can explain knowledge of ODS |
| Gestity | Number of pregnancies the pregnant woman had | Categorical | Too early (<19 years) Too reproductive (reproductive interval of <2 years) Too many (>5 births) Too late (>35 years) | Can explain knowledge of ODS |
| Antenatal consultation (ANC) | Number of times the pregnant women have attended prenatal consultation | Categorical | ANC 1 ANC 2 ANC 3 ANC 4 | Can explain knowledge of ODS |
| Obstetric characteristics | ||||
| Antepartum (during pregnancy) | Obstetric complications that can occur in pregnant women during pregnancy | Categorical | Constant severe abdominal pain, severe vaginal bleeding, persistent fever, severe headaches or blurred vision, intense fatigue, swelling of the hands or face, difficulty in breathing, and absent or decreased fetal movement | Important variable |
| Peripartum (during labor and delivery) | Obstetric complications that can occur in a pregnant woman during labor or delivery | Categorical | Rupture of the membrane before the onset of labor, prolonged labor over 12 h, severe vaginal bleeding, convulsions/loss of consciousness, and retention of the placenta | Important variable |
| Postpartum (after childbirth) | Obstetric complications that occur in a pregnant woman after delivery | Categorical | Severe vaginal bleeding, foul-smelling vaginal discharge, severe abdominal pain, persistent fever, and intense fatigue | Important variable |
| Category | ODS | Has Knowledge of Danger Signs | Number of ODS Cited |
|---|---|---|---|
| Antepartum (during pregnancy) | Constant severe abdominal pain, severe vaginal bleeding, fever and weakness (cannot get out of bed), rapid or difficult breathing, severe headaches with blurred vision, rapid or difficult breathing, swelling of fingers, face and legs, severe fatigue, lack of or decreased fetal movement [2,4,5] | Yes | ≥3 signs |
| No | <3 signs | ||
| Peripartum (during labor/delivery) | Rupture of the membrane before the onset of labor, prolonged labor of >12 h, severe vaginal bleeding, convulsions/loss of consciousness, retention of the placenta... [5,7,20] | Yes | ≥3 signs |
| No | <3 signs | ||
| Postpartum | Severe vaginal bleeding, foul-smelling vaginal discharge, severe abdominal pain, fever, intense fatigue... [5,7,20] | Yes | ≥3 signs |
| No | <3 signs |
| Variables | N | % | Mean | Min–Max |
|---|---|---|---|---|
| Age (years) | 623 | 25 (±7) | 12–49 | |
| ≤19 years | 143 | 22.9 | ||
| 20–29 years | 303 | 48.9 | ||
| 30–39 years | 158 | 25.4 | ||
| 40–49 years | 19 | 3.1 | ||
| Level of education | 626 | |||
| Not in school | 39 | 6.2 | ||
| Primary | 208 | 32.4 | ||
| Secondary | 379 | 60.6 | ||
| Higher | 5 | 0.8 | ||
| Marital status | 626 | |||
| Single | 4 | 0.6 | ||
| Married/common-law | 622 | 99.4 | ||
| Occupation | 626 | |||
| Unemployed | 91 | 14.5 | ||
| Pupil/student | 13 | 2.1 | ||
| Farmer/trader | 504 | 80.5 | ||
| Civil servant | 18 | 2.9 | ||
| Religion | 624 | |||
| Muslim | 424 | 67.9 | ||
| Revival church | 94 | 15.1 | ||
| Catholic | 61 | 9.8 | ||
| Protestant | 41 | 6.6 | ||
| Kimbanguist | 4 | 0.6 | ||
| Parity | 626 | |||
| First pregnancy | 74 | 11.8 | ||
| Given birth 1 time | 131 | 20.9 | ||
| Given birth 2 times | 105 | 16.8 | ||
| Given birth 3–5 times | 130 | 20.8 | ||
| Given birth >5 times | 186 | 29.7 | ||
| Prenatal consultations ANC 1 | 626 | |||
| Yes | 355 | 56.7 | ||
| No | 271 | 43.3 | ||
| Completion ofall 4 ANCs (completionof ANC4) | 626 | |||
| Yes | 63 | 10.1 | ||
| No | 563 | 89.9 |
| Women Surveyed | n | % (95% CI) |
|---|---|---|
| Knowledge of signs | ||
| Yes | 137 | 21.9 (18.7–25.3) |
| No | 489 | 78.1 (74.7–81.3) |
| Total | 626 |
| Variables | N | % KODS | Adjusted OR (95% CI) | p Value |
|---|---|---|---|---|
| Age groups | 623 | 0.015 | ||
| ≤19 years | 143 | 14.7 | 1 | |
| 20–29 years | 303 | 20.8 | 1.5 (0.9–2.6) | |
| 30–39 years | 158 | 22.1 | 2.4 (1.3–4.2) | |
| 40–49 years | 19 | 31.6 | 2.7 (0.9–7.8) | |
| Level of education | 626 | 0.217 f | ||
| No schooling | 39 | 23.1 | 1 | |
| Primary | 203 | 25.6 | 1.2 (0.5–2.6) | |
| Secondary | 379 | 19.5 | 0.8 (0.4–1.8) | |
| Higher | 5 | 40.0 | 2.2 (0.3–15.4) | |
| Marital status | 626 | 0.629 f | ||
| Single/divorced/widowed | 4 | 25.0 | 1 | |
| Married/common-law | 622 | 21.9 | 0.8 (0.1–36.8) | |
| Occupation | 626 | 0.122 f | ||
| Unemployed | 91 | 13.2 | 1 | |
| Pupil/student | 13 | 14.4 | 1.2 (0.2–6.1) | |
| Farmer/trader | 504 | 23.8 | 2.1 (1.0–3.9) | |
| Civil servant | 18 | 16.7 | 1.3 (0.3–5.2) | |
| Religion | 624 | 0.099 f | ||
| Muslim | 424 | 22.4 | 1 | |
| Revival church | 94 | 12.7 | 0.5 (0.3–0.9) | |
| Catholic | 61 | 27.9 | 1.3 (0.7–2.5) | |
| Protestant | 41 | 26.8 | 1.3 (0.6–2.6) | |
| Kimbanguist | 4 | 0.0 | -- | |
| Parity | 626 | 0.001 | ||
| First pregnancy | 74 | 6.8 | 1 | |
| Given birth 1 time | 131 | 16.0 | 2.6 (0.9–7.3) | |
| Given birth 2 times | 105 | 24.8 | 4.5 (1.7–12.5) | |
| Given birth 3–5 times | 130 | 25.9 | 4.7 (1.8–12.6) | |
| Given birth >5 times | 186 | 28.0 | 5.4 (2.1–14.0) | |
| Prenatal consultations ANC 1 | 626 | 0.952 | ||
| No | 271 | 21.7 | 1 | |
| Yes | 355 | 21.9 | 1.0 (0.7–1.5) | |
| Completion of all 4 ANCs (completionof ANC 4) | 626 | 0.946 | ||
| No | 563 | 21.9 | 1 | |
| Yes | 63 | 22.2 | 1.0 (0.2–1.9) |
| Variables | Adjusted OR (95% CI) | p Value |
|---|---|---|
| Age groups | 0.739 | |
| ≤19 years | 1 | |
| 20–29 years | 0.8 (0.4–1.5) | 0.438 |
| 30–39 years | 1.1 (0.5–2.6) | 0.862 |
| 40–49 years | 1.2 (0.3–4.5) | 0.755 |
| Parity | 0.021 | |
| First pregnancy | 1 | |
| Given birth 1 time | 2.9 (1.0–8.1) | 0.049 |
| Given birth 2 times | 5.4 (1.8–16.6) | 0.003 |
| Given birth 3–5 times | 5.3 (1.7–16.9) | 0.004 |
| Given birth >5 times | 4.9 (1.5–16.4) | 0.009 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Imani Ramazani, B.-E.; Mabakutuvangilanga Ntala, S.-D.; Katuashi Ishoso, D.; Rothan-Tondeur, M. Knowledge of Obstetric Danger Signs among Pregnant Women in the Eastern Democratic Republic of the Congo. Int. J. Environ. Res. Public Health 2023, 20, 5593. https://doi.org/10.3390/ijerph20085593
Imani Ramazani B-E, Mabakutuvangilanga Ntala S-D, Katuashi Ishoso D, Rothan-Tondeur M. Knowledge of Obstetric Danger Signs among Pregnant Women in the Eastern Democratic Republic of the Congo. International Journal of Environmental Research and Public Health. 2023; 20(8):5593. https://doi.org/10.3390/ijerph20085593
Chicago/Turabian StyleImani Ramazani, Bin-Eradi, Simon-Decap Mabakutuvangilanga Ntala, Daniel Katuashi Ishoso, and Monique Rothan-Tondeur. 2023. "Knowledge of Obstetric Danger Signs among Pregnant Women in the Eastern Democratic Republic of the Congo" International Journal of Environmental Research and Public Health 20, no. 8: 5593. https://doi.org/10.3390/ijerph20085593
APA StyleImani Ramazani, B.-E., Mabakutuvangilanga Ntala, S.-D., Katuashi Ishoso, D., & Rothan-Tondeur, M. (2023). Knowledge of Obstetric Danger Signs among Pregnant Women in the Eastern Democratic Republic of the Congo. International Journal of Environmental Research and Public Health, 20(8), 5593. https://doi.org/10.3390/ijerph20085593