
Self-Reported Chronic Back Pain and Current Depression in Brazil: A National Level Study


Abstract
1. Introduction
2. Materials and Methods
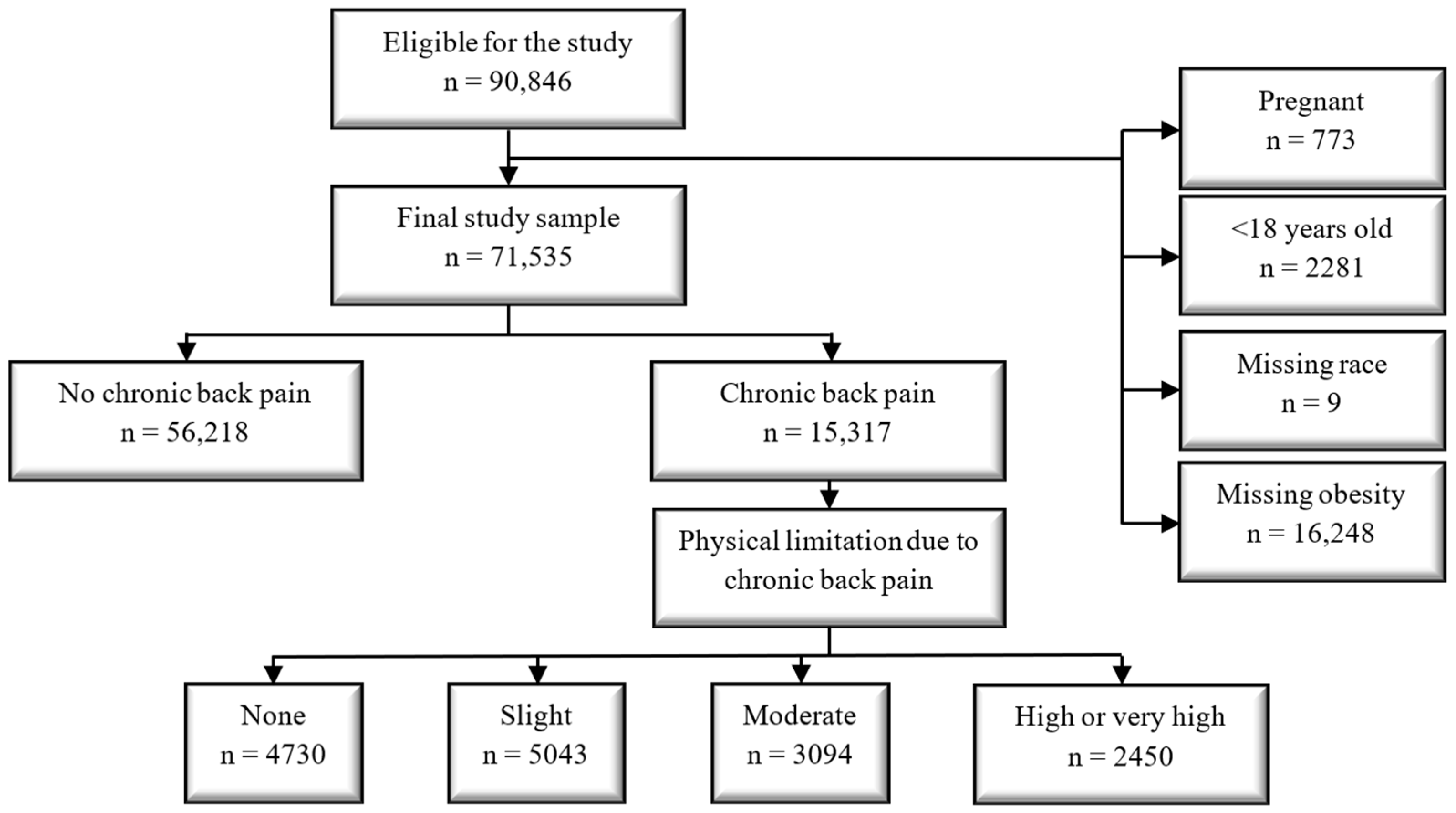
2.1. Study Sample
2.2. Outcome of Interest: Self-Reported Current Depression (SRCD)
2.3. First Exposure of Interest: Self-Reported Chronic Back Pain (CBP)
2.4. Second Exposure of Interest: Physical Limitation due to CBP (Slight, Moderate, and High Limitation)
2.5. Covariates of Interest
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Depression. Available online: https://www.who.int/news-room/fact-sheets/detail/depression (accessed on 21 February 2023).
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013; ISBN 978-0-89042-555-8. [Google Scholar]
- Nezu, A.M.; Ronan, G.F.; Meadows, E.A.; McClure, K.S. (Eds.) . Practitioner’s Guide to Empirically Based Measures of Depression; AABT Clinical Assessment Series; Kluwer Academic Publishers: Boston, MA, USA, 2002; ISBN 0-306-46246-X. [Google Scholar]
- Hedden, S.L.; Kennet, J.; Lipari, R.; Medley, G.; Tice, P. Behavioral Health Trends in the United States: Results from the 2014 National Survey on Drug Use and Health. US Dep. Heal. Hum. Serv. 2015. Available online: https://www.samhsa.gov/data/sites/default/files/NSDUH-FRR1-2014/NSDUH-FRR1-2014.pdf (accessed on 21 February 2023).
- Weissman, M.M. Cross-National Epidemiology of Major Depression and Bipolar Disorder. JAMA J. Am. Med. Assoc. 1996, 276, 293. [Google Scholar] [CrossRef]
- Eisendrath, S.J.; Cole, S.A.; Christensen, J.F.; Gutnick, D.; Cole, M.R.; Feldman, M.D. Depression. In Behavioral Medicine: A Guide for Clinical Practice, 4e; Feldman, M.D., Christensen, J.F., Satterfield, J.M., Eds.; McGraw-Hill Education: New York, NY, USA, 2014. [Google Scholar]
- Koyanagi, A.; Oh, H.; Stubbs, B.; Haro, J.M.; DeVylder, J.E. Epidemiology of Depression with Psychotic Experiences and Its Association with Chronic Physical Conditions in 47 Low- and Middle-Income Countries. Psychol. Med. 2017, 47, 531–542. [Google Scholar] [CrossRef]
- Fernandez, M.; Colodro-Conde, L.; Hartvigsen, J.; Ferreira, M.L.; Refshauge, K.M.; Pinheiro, M.B.; Ordoñana, J.R.; Ferreira, P.H. Chronic Low Back Pain and the Risk of Depression or Anxiety Symptoms: Insights from a Longitudinal Twin Study. Spine J. 2017, 17, 905–912. [Google Scholar] [CrossRef]
- Sagheer, M.A.; Khan, M.F.; Sharif, S. Association between Chronic Low Back Pain, Anxiety and Depression in Patients at a Tertiary Care Centre. J. Pak. Med. Assoc. 2013, 63, 688–690. [Google Scholar]
- Banks, S.M.; Kerns, R.D. Explaining High Rates of Depression in Chronic Pain: A Diathesis-Stress Framework. Psychol. Bull. 1996, 119, 95–110. [Google Scholar] [CrossRef]
- Rush, A.J.; Polatin, P.; Gatchel, R.J. Depression and Chronic Low Back Pain. Spine 2000, 25, 2566–2571. [Google Scholar] [CrossRef]
- Dworkin, R.H.; Gitlin, M.J. Clinical Aspects of Depression in Chronic Pain Patients. Clin. J. Pain 1991, 7, 79–94. [Google Scholar] [CrossRef]
- van’t Land, H.; Verdurmen, J.; Ten, M.; Van, S.; De, R. The Association between Chronic Back Pain and Psychiatric Disorders: Results from a Longitudinal Population-Based Study. In Anxiety and Related Disorders; InTech: Jakarta Selatan, Indonesia, 2011; pp. 247–256. [Google Scholar]
- Gerrits, M.M.J.G.; van Oppen, P.; van Marwijk, H.W.J.; Penninx, B.W.J.H.; van der Horst, H.E. Pain and the Onset of Depressive and Anxiety Disorders. Pain 2014, 155, 53–59. [Google Scholar] [CrossRef]
- Vos, T.; Barber, R.M.; Bell, B.; Bertozzi-Villa, A.; Biryukov, S.; Bolliger, I.; Charlson, F.; Davis, A.; Degenhardt, L.; Dicker, D.; et al. Global, Regional, and National Incidence, Prevalence, and Years Lived with Disability for 301 Acute and Chronic Diseases and Injuries in 188 Countries, 1990–2013: A Systematic Analysis for the Global Burden of Disease Study 2013. Lancet 2015, 386, 743–800. [Google Scholar] [CrossRef]
- Treede, R.-D.; Rief, W.; Barke, A.; Aziz, Q.; Bennett, M.I.; Benoliel, R.; Cohen, M.; Evers, S.; Finnerup, N.B.; First, M.B.; et al. A Classification of Chronic Pain for ICD-11. Pain 2015, 156, 1003–1007. [Google Scholar] [CrossRef]
- Patrick, N.; Emanski, E.; Knaub, M.A. Acute and Chronic Low Back Pain. Med. Clin. N. Am. 2014, 98, 777–789. [Google Scholar] [CrossRef]
- Hoy, D.; Bain, C.; Williams, G.; March, L.; Brooks, P.; Blyth, F.; Woolf, A.; Vos, T.; Buchbinder, R. A Systematic Review of the Global Prevalence of Low Back Pain. Arthritis Rheum. 2012, 64, 2028–2037. [Google Scholar] [CrossRef]
- Malta, D.C.; Stopa, S.R.; Szwarcwald, C.L.; Gomes, N.L.; Silva Júnior, J.B.; Reis, A.A.C. dos A Vigilância e o Monitoramento Das Principais Doenças Crônicas Não Transmissíveis No Brasil—Pesquisa Nacional de Saúde, 2013. Rev. Bras. Epidemiol. 2015, 18, 3–16. [Google Scholar] [CrossRef]
- Vancampfort, D.; Stubbs, B.; Koyanagi, A. Physical Chronic Conditions, Multimorbidity and Sedentary Behavior amongst Middle-Aged and Older Adults in Six Low- and Middle-Income Countries. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 147. [Google Scholar] [CrossRef]
- Adilay, U.; Guclu, B.; Goksel, M.; Keskil, S. The Correlation of SCL-90-R Anxiety, Depression, Somatization Subscale Scores with Chronic Low Back Pain. Turk. Neurosurg. 2018, 28, 434–438. [Google Scholar] [CrossRef]
- Marshall, P.W.M.; Schabrun, S.; Knox, M.F. Physical Activity and the Mediating Effect of Fear, Depression, Anxiety, and Catastrophizing on Pain Related Disability in People with Chronic Low Back Pain. PLoS ONE 2017, 12, e0180788. [Google Scholar] [CrossRef]
- Tsuji, T.; Matsudaira, K.; Sato, H.; Vietri, J. The Impact of Depression among Chronic Low Back Pain Patients in Japan. BMC Musculoskelet. Disord. 2016, 17, 447. [Google Scholar] [CrossRef]
- Trocoli, T.O.; Botelho, R.V. Prevalência de Ansiedade, Depressão e Cinesiofobia Em Pacientes Com Lombalgia e Sua Associação Com Os Sintomas Da Lombalgia. Rev. Bras. Reumatol. 2016, 56, 330–336. [Google Scholar] [CrossRef]
- Rodrigues-De-Souza, D.P.; Fernández-De-Las-Peñas, C.; Martín-Vallejo, F.J.; Blanco-Blanco, J.F.; Moro-Gutiérrez, L.; Alburquerque-Sendín, F. Differences in Pain Perception, Health-Related Quality of Life, Disability, Mood, and Sleep between Brazilian and Spanish People with Chronic Non-Specific Low Back Pain. Braz. J. Phys. Ther. 2016, 20, 412–421. [Google Scholar] [CrossRef]
- Stopa, S.R.; Szwarcwald, C.L.; de sOliveira, M.M.; Gouvea, E.d.C.D.P.; Vieira, M.L.F.P.; de Freitas, M.P.S.; Sardinha, L.M.V.; Macário, E.M. Pesquisa Nacional de Saúde 2019: Histórico, Métodos e Perspectivas. Epidemiol. E Serviços Saúde 2020, 29, e2020315. [Google Scholar] [CrossRef]
- Szwarcwald, C.L.; Malta, D.C.; Pereira, C.A.; Vieira, M.L.F.P.; Conde, W.L.; de Souza Júnior, P.R.B.; Damacena, G.N.; Azevedo, L.O.; Azevedo e Silva, G.; Theme Filha, M.M.; et al. Pesquisa Nacional de Saúde No Brasil: Concepção e Metodologia de Aplicação. Cien. Saude Colet. 2014, 19, 333–342. [Google Scholar] [CrossRef] [PubMed]
- Amiel Castro, R.T.; Pinard Anderman, C.; Glover, V.; O’Connor, T.G.; Ehlert, U.; Kammerer, M. Associated Symptoms of Depression: Patterns of Change during Pregnancy. Arch. Womens. Ment. Health 2017, 20, 123–128. [Google Scholar] [CrossRef] [PubMed]
- Silva, M.M.d.J.; Leite, E.P.R.C.; Nogueira, D.A.; Clapis, M.J. Depression in Pregnancy: Prevalence and Associated Factors. Investig. Educ. Enfermería 2016, 34, 342–350. [Google Scholar] [CrossRef] [PubMed]
- Pearlstein, T. Depression during Pregnancy. Best Pract. Res. Clin. Obstet. Gynaecol. 2015, 29, 754–764. [Google Scholar] [CrossRef]
- Anderson, J.E.; Michalak, E.E.; Lam, R.W. Depression in Primary Care: Tools for Screening, Diagnosis, and Measuring Response to Treatment. B. C. Med. J. 2022, 44, 415–419. [Google Scholar]
- Santos, I.S.; Tavares, B.F.; Munhoz, T.N.; de Almeida, L.S.P.; da Silva, N.T.B.; Tams, B.D.; Patella, A.M.; Matijasevich, A. Sensibilidade e Especificidade Do Patient Health Questionnaire-9 (PHQ-9) Entre Adultos Da População Geral. Cad. Saude Publica 2013, 29, 1533–1543. [Google Scholar] [CrossRef]
- Razykov, I.; Ziegelstein, R.C.; Whooley, M.A.; Thombs, B.D. The PHQ-9 versus the PHQ-8—Is Item 9 Useful for Assessing Suicide Risk in Coronary Artery Disease Patients? Data from the Heart and Soul Study. J. Psychosom. Res. 2012, 73, 163–168. [Google Scholar] [CrossRef]
- Shin, C.; Lee, S.-H.; Han, K.-M.; Yoon, H.-K.; Han, C. Comparison of the Usefulness of the PHQ-8 and PHQ-9 for Screening for Major Depressive Disorder: Analysis of Psychiatric Outpatient Data. Psychiatry Investig. 2019, 16, 300–305. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W.; Löwe, B. The Patient Health Questionnaire Somatic, Anxiety, and Depressive Symptom Scales: A Systematic Review. Gen. Hosp. Psychiatry 2010, 32, 345–359. [Google Scholar] [CrossRef]
- Kroenke, K.; Strine, T.W.; Spitzer, R.L.; Williams, J.B.W.; Berry, J.T.; Mokdad, A.H. The PHQ-8 as a Measure of Current Depression in the General Population. J. Affect. Disord. 2009, 114, 163–173. [Google Scholar] [CrossRef]
- Instituto Brasileiro de Geografia e Estatística (IBGE). Diretoria de Pesquisas Coordenação de Trabalho e Rendimento Questionário Dos Moradores Do Domicílio. Available online: https://www.pns.icict.fiocruz.br/wp-content/uploads/2021/02/Questionario-PNS-2013.pdf (accessed on 21 February 2023).
- Gullich, I.; Duro, S.M.S.; Cesar, J.A. Depressão Entre Idosos: Um Estudo de Base Populacional No Sul Do Brasil. Rev. Bras. Epidemiol. 2016, 19, 691–701. [Google Scholar] [CrossRef] [PubMed]
- Engin, S.; Ozturk, M.; Engin, N.; Baral Kulaksizoglu, I. Dark Side of the Town: Depressive Symptoms in Disadvantaged Senior Citizens. J. Nutr. Health Aging 2010, 14, 483–487. [Google Scholar] [CrossRef]
- Silva, M.T.; Galvao, T.F.; Martins, S.S.; Pereira, M.G. Prevalence of Depression Morbidity among Brazilian Adults: A Systematic Review and Meta-Analysis. Rev. Bras. Psiquiatr. 2014, 36, 262–270. [Google Scholar] [CrossRef] [PubMed]
- Stopa, S.R.; Malta, D.C.; de Oliveira, M.M.; Lopes, C.d.S.; Menezes, P.R.; Kinoshita, R.T. Prevalência Do Autorrelato de Depressão No Brasil: Resultados Da Pesquisa Nacional de Saúde, 2013. Rev. Bras. Epidemiol. 2015, 18, 170–180. [Google Scholar] [CrossRef] [PubMed]
- Moreira, V. Critical Phenomenology of Depression in Brazil, Chile and the United States. Lat. Am. J. Fundam. Psychopathol. Line 2007, 4, 193–218. [Google Scholar]
- de Oliveira, G.D.; Oancea, S.C.; Nucci, L.B.; Vogeltanz-Holm, N. The Association between Physical Activity and Depression among Individuals Residing in Brazil. Soc. Psychiatry Psychiatr. Epidemiol. 2018, 53, 373–383. [Google Scholar] [CrossRef]
- Schuch, F.B.; Vancampfort, D.; Richards, J.; Rosenbaum, S.; Ward, P.B.; Stubbs, B. Exercise as a Treatment for Depression: A Meta-Analysis Adjusting for Publication Bias. J. Psychiatr. Res. 2016, 77, 42–51. [Google Scholar] [CrossRef]
- Schuch, F.B.; Vancampfort, D.; Rosenbaum, S.; Richards, J.; Ward, P.B.; Veronese, N.; Solmi, M.; Cadore, E.L.; Stubbs, B. Exercise for Depression in Older Adults: A Meta-Analysis of Randomized Controlled Trials Adjusting for Publication Bias. Rev. Bras. Psiquiatr. 2016, 38, 247–254. [Google Scholar] [CrossRef]
- Fleck, M.P.d.A.; Lima, A.F.B.d.S.; Louzada, S.; Schestasky, G.; Henriques, A.; Borges, V.R.; Camey, S. Associação Entre Sintomas Depressivos e Funcionamento Social Em Cuidados Primários à Saúde. Rev. Saude Publica 2002, 36, 431–438. [Google Scholar] [CrossRef]
- Furtado, R.N.V.; Ribeiro, L.H.; de Arruda Abdo, B.; Descio, F.J.; Martucci Junior, C.E.; Serruya, D.C. Dor Lombar Inespecífica Em Adultos Jovens: Fatores de Risco Associados. Rev. Bras. Reumatol. 2014, 54, 371–377. [Google Scholar] [CrossRef]
- Jacobs, J.M.; Hammerman-Rozenberg, R.; Cohen, A.; Stessman, J. Chronic Back Pain among the Elderly: Prevalence, Associations, and Predictors. Spine 2006, 31, E203–E207. [Google Scholar] [CrossRef] [PubMed]
- Carey, T.S.; Freburger, J.K.; Holmes, G.M.; Jackman, A.; Knauer, S.; Wallace, A.; Darter, J. Race, Care Seeking, and Utilization for Chronic Back and Neck Pain: Population Perspectives. J. Pain 2010, 11, 343–350. [Google Scholar] [CrossRef] [PubMed]
- Angst, F.; Angst, J.; Ajdacic-Gross, V.; Aeschlimann, A.; Rössler, W. Epidemiology of Back Pain in Young and Middle-Aged Adults: A Longitudinal Population Cohort Survey from Age 27–50 Years. Psychosomatics 2017, 58, 604–613. [Google Scholar] [CrossRef] [PubMed]
- Zanuto, E.A.C.; Codogno, J.S.; Christófaro, D.G.D.; Vanderlei, L.C.M.; Cardoso, J.R.; Fernandes, R.A. Prevalence of Low Back Pain and Associated Factors in Adults from a Middle-Size Brazilian City. Cien. Saude Colet. 2015, 20, 1575–1582. [Google Scholar] [CrossRef] [PubMed]
- Rinaldo, L.; McCutcheon, B.A.; Gilder, H.; Kerezoudis, P.; Murphy, M.; Maloney, P.; Hassoon, A.; Bydon, M. Diabetes and Back Pain: Markers of Diabetes Disease Progression Are Associated with Chronic Back Pain. Clin. Diabetes 2017, 35, 126–131. [Google Scholar] [CrossRef]
- Dionne, C.E. Formal Education and Back Pain: A Review. J. Epidemiol. Community Health 2001, 55, 455–468. [Google Scholar] [CrossRef]
- Trask, C.; Bath, B.; McCrosky, J.; Lawson, J. A Profile of Farmers and Other Employed Canadians with Chronic Back Pain: A Population-Based Analysis of the 2009-2010 Canadian Community Health Surveys. J. Rural Health 2014, 30, 300–310. [Google Scholar] [CrossRef]
- Rundell, S.D.; Sherman, K.J.; Heagerty, P.J.; Mock, C.N.; Dettori, N.J.; Comstock, B.A.; Avins, A.L.; Nedeljkovic, S.S.; Nerenz, D.R.; Jarvik, J.G. Predictors of Persistent Disability and Back Pain in Older Adults with a New Episode of Care for Back Pain. Pain Med. 2016, 18, 1049–1062. [Google Scholar] [CrossRef]
- Hardt, J.; Jacobsen, C.; Goldberg, J.; Nickel, R.; Buchwald, D. Prevalence of Chronic Pain in a Representative Sample in the United States. Pain Med. 2008, 9, 803–812. [Google Scholar] [CrossRef]
- Latza, U.; Kohlmann, T.; Deck, R.; Raspe, H. Influence of Occupational Factors on the Relation between Socioeconomic Status and Self-Reported Back Pain in a Population-Based Sample of German Adults with Back Pain. Spine 2000, 25, 1390–1397. [Google Scholar] [CrossRef]
- Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults—The Evidence Report. National Institutes of Health. Obes. Res. 1998, 6 (Suppl. 2), 51S–209S.
- Sullivan, M.J.L.; Reesor, K.; Mikail, S.; Fisher, R. The Treatment of Depression in Chronic Low Back Pain: Review and Recommendations. Pain 1992, 50, 5–13. [Google Scholar] [CrossRef] [PubMed]
- Bair, M.J.; Wu, J.; Damush, T.M.; Sutherland, J.M.; Kroenke, K. Association of Depression and Anxiety Alone and in Combination with Chronic Musculoskeletal Pain in Primary Care Patients. Psychosom. Med. 2008, 70, 890–897. [Google Scholar] [CrossRef] [PubMed]
- Moultry, A.M.; Poon, I.O. The Use of Antidepressants for Chronic Pain. US Pharmacyst 2009, 34, 26–34. [Google Scholar]
- Blier, P.; Abbott, F.V. Putative Mechanisms of Action of Antidepressant Drugs in Affective and Anxiety Disorders and Pain. J. Psychiatry Neurosci. 2001, 26, 37–43. [Google Scholar]
- Jann, M.W.; Slade, J.H. Antidepressant Agents for the Treatment of Chronic Pain and Depression. Pharmacotherapy 2007, 27, 1571–1587. [Google Scholar] [CrossRef]
- Thase, M.E. Managing Medical Comorbidities in Patients with Depression to Improve Prognosis. J. Clin. Psychiatry 2016, 77, 22–27. [Google Scholar] [CrossRef]
- Maes, M. An Intriguing and Hitherto Unexplained Co-Occurrence: Depression and Chronic Fatigue Syndrome Are Manifestations of Shared Inflammatory, Oxidative and Nitrosative (IO&NS) Pathways. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2011, 35, 784–794. [Google Scholar] [CrossRef]
- Gilkey, D.P.; Keefe, T.J.; Peel, J.L.; Kassab, O.M.; Kennedy, C.A. Risk Factors Associated with Back Pain: A Cross-Sectional Study of 963 College Students. J. Manip. Physiol. Ther. 2010, 33, 88–95. [Google Scholar] [CrossRef]
- Teychenne, M.; Ball, K.; Salmon, J. Sedentary Behavior and Depression Among Adults: A Review. Int. J. Behav. Med. 2010, 17, 246–254. [Google Scholar] [CrossRef]
- Magni, G.; Caldieron, C.; Rigatti-Luchini, S.; Merskey, H. Chronic Musculoskeletal Pain and Depressive Symptoms in the General Population. An Analysis of the 1st National Health and Nutrition Examination Survey Data. Pain 1990, 43, 299–307. [Google Scholar] [CrossRef] [PubMed]
- Rudy, T.E.; Kerns, R.D.; Turk, D.C. Chronic Pain and Depression: Toward a Cognitive-Behavioral Mediation Model. Pain 1988, 35, 129–140. [Google Scholar] [CrossRef] [PubMed]
- Von Korff, M.; Simon, G. The Relationship between Pain and Depression. Br. J. Psychiatry 1996, 168, 101–108. [Google Scholar] [CrossRef]
- Waxman, R.; Tennant, A.; Helliwell, P. Community Survey of Factors Associated with Consultation for Low Back Pain. BMJ 1998, 317, 1564–1567. [Google Scholar] [CrossRef] [PubMed]
- Elfving, B.; Lund, I.; Boström, C. Ratings of Pain and Activity Limitation on the Visual Analogue Scale and Global Impression of Change in Multimodal Rehabilitation of Back Pain—Analyses at Group and Individual Level. Disabil. Rehabil. 2016, 38, 2206–2216. [Google Scholar] [CrossRef] [PubMed]
- Razzouk, D. Por Que o Brasil Deveria Priorizar o Tratamento Da Depressão Na Alocação Dos Recursos Da Saúde? Epidemiol. e Serviços Saúde 2016, 25, 845–848. [Google Scholar] [CrossRef]
- Barrientos, A.; Møller, V.; Saboia, J.; Lloyd-Sherlock, P.; Mase, J. ‘Growing’ Social Protection in Developing Countries: Lessons from Brazil and South Africa. Dev. South. Afr. 2013, 30, 54–68. [Google Scholar] [CrossRef]
- Chisholm, D.; Sweeny, K.; Sheehan, P.; Rasmussen, B.; Smit, F.; Cuijpers, P.; Saxena, S. Scaling-up Treatment of Depression and Anxiety: A Global Return on Investment Analysis. Lancet Psychiatry 2016, 3, 415–424. [Google Scholar] [CrossRef]
- World Health Organization. Mental Health Atlas 2014; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Dunlop, D.D.; Song, J.; Lyons, J.S.; Manheim, L.M.; Chang, R.W. Racial/Ethnic Differences in Rates of Depression among Preretirement Adults. Am. J. Public Health 2003, 93, 1945–1952. [Google Scholar] [CrossRef]
- Kessler, R.C.; Birnbaum, H.G.; Shahly, V.; Bromet, E.; Hwang, I.; McLaughlin, K.A.; Sampson, N.; Andrade, L.H.; de Girolamo, G.; Demyttenaere, K.; et al. Age Differences in the Prevalence and Co-Morbidity of DSM-IV Major Depressive Episodes: Results from the WHO World Mental Health Survey Initiative. Depress. Anxiety 2010, 27, 351–364. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Overall (n = 71,535) | Current Depression | p-Value * | |||||
|---|---|---|---|---|---|---|---|---|
| Yes (n = 7100) | No (n = 64,435) | |||||||
| Unweighted Counts | Weighted | Weighted | Weighted | |||||
| Median | Interquartile Range | Median | Interquartile Range | Median | Interquartile Range | |||
| Age at survey | 71,535 | 42.34 | 30.55–55.91 | 43.28 | 31.16–55.73 | 42.23 | 30.47–55.93 | 0.411 |
| Characteristics | Percent | 95% CI for Percent | Percent | 95% CI for Percent | Percent | 95% CI for Percent | p-value ** | |
| Gender | ||||||||
| Female | 36,262 | 51.19 | 50.54–51.84 | 72.02 | 70.12–73.92 | 48.79 | 48.09–49.49 | <0.001 |
| Male | 35,273 | 48.81 | 48.16–49.46 | 27.98 | 26.08–29.88 | 51.21 | 50.51–51.91 | |
| Race | ||||||||
| Brown | 34,724 | 41.79 | 41.04–42.54 | 42.35 | 40.33–44.36 | 41.73 | 40.95–42.51 | 0.255 |
| White | 27,962 | 46.01 | 45.21–46.81 | 44.60 | 42.48–46.73 | 46.17 | 45.34–47.00 | |
| Other | 8849 | 12.20 | 11.74–12.65 | 13.05 | 11.62–14.48 | 12.10 | 11.62–12.58 | |
| Education | ||||||||
| Less than high school | 34,313 | 44.48 | 43.67–45.29 | 49.26 | 47.23–51.30 | 43.93 | 43.11–44.75 | <0.001 |
| Completed high school | 20,675 | 31.77 | 31.11–32.42 | 28.08 | 26.22–29.94 | 32.19 | 31.48–32.90 | |
| More than high school | 16,547 | 23.75 | 22.95–24.56 | 22.66 | 20.66–24.66 | 23.88 | 23.03–24.73 | |
| Health Insurance | ||||||||
| Yes | 18,733 | 30.19 | 29.32–31.70 | 26.34 | 24.31–28.36 | 30.64 | 29.74–31.53 | <0.001 |
| No | 52,802 | 69.81 | 68.93–70.68 | 73.66 | 71.64–75.69 | 69.36 | 68.47–70.26 | |
| Diabetes | ||||||||
| Yes | 3018 | 4.12 | 3.88–4.37 | 8.70 | 7.53–9.87 | 3.60 | 3.35–3.84 | <0.001 |
| No | 68,517 | 95.88 | 95.63–96.12 | 91.30 | 90.13–92.47 | 96.41 | 96.16–96.65 | |
| Hypertension | ||||||||
| Yes | 9558 | 12.90 | 12.48–13.32 | 22.90 | 21.21–24.58 | 11.75 | 11.34–12.15 | <0.001 |
| No | 61,977 | 87.10 | 86.69–87.52 | 77.10 | 75.42–78.79 | 88.25 | 87.85–88.66 | |
| Physical activity for leisure | ||||||||
| Yes | 22,120 | 31.90 | 31.22–32.58 | 21.96 | 20.09–23.83 | 33.05 | 32.34–33.76 | <0.001 |
| No | 49,415 | 68.10 | 67.42–68.78 | 78.04 | 76.17–79.91 | 66.95 | 66.24–67.66 | |
| Obesity | ||||||||
| Yes | 15,248 | 21.81 | 21.00–22.63 | 27.97 | 25.89–30.05 | 21.10 | 20.32–21.89 | <0.001 |
| No | 56,287 | 78.19 | 77.37–79.00 | 72.03 | 69.65–74.11 | 78.90 | 78.11–79.68 | |
| Characteristics | Overall (n = 71,535) | Current Depression | p-Value * | |||||
|---|---|---|---|---|---|---|---|---|
| Yes (n = 7100) | No (n = 64,435) | |||||||
| Unweighted Counts | Weighted | Weighted | Weighted | |||||
| Percent | 95% CI for Percent | Percent | 95% CI for Percent | Percent | 95% CI for Percent | |||
| Chronic Back Pain | ||||||||
| Yes | 15,317 | 21.64 | 21.05–22.23 | 40.64 | 38.64–42.64 | 19.45 | 18.85–20.05 | <0.001 |
| No | 56,218 | 78.36 | 77.77–78.95 | 59.36 | 57.36–61.36 | 80.55 | 79.95–81.15 | |
| Physical limitation due to chronic back pain | ||||||||
| Characteristics | Overall (n = 15,437) | Current Depression | p-value ** | |||||
| Yes (n = 2855) | No (n = 12,582) | |||||||
| Unweighted counts | Weighted | Weighted | Weighted | |||||
| Percent | 95% CI for Percent | Percent | 95% CI for Percent | Percent | 95% CI for Percent | |||
| Physical Limitation (n = 15,437) | ||||||||
| None | 4730 | 32.88 | 31.41–34.36 | 17.47 | 14.90–20.03 | 36.60 | 34.92–38.27 | <0.001 |
| Slight | 5043 | 32.42 | 30.06–33.78 | 29.32 | 26.38–32.26 | 33.17 | 31.69–34.64 | |
| Moderate | 3094 | 19.20 | 18.03–20.38 | 22.32 | 19.78–24.86 | 18.45 | 17.12–19.79 | |
| High or very high | 2450 | 15.49 | 14.34–16.64 | 30.89 | 27.84–33.94 | 11.78 | 10.74–12.83 | |
| Exposure of Interest | Self-Reported Current Depression | |
|---|---|---|
| WUOR (95% CI) | WAOR (95% CI) | |
| Chronic back pain (n = 71,535) | ||
| No | REF | REF |
| Yes | 2.84 (2.59, 3.10) | 2.68 (2.44, 2.94) |
| Physical limitation due to back pain (n = 15,317) | ||
| None | REF | REF |
| Slight | 1.85 (1.49, 2.31) | 1.86 (1.49, 2.33) |
| Moderate | 2.53 (2.02, 3.18) | 2.49 (1.98, 3.14) |
| High or Very High | 5.49 (4.43, 6.81) | 5.47 (4.38, 6.83) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Norris, R.J.; Oancea, S.C.; Nucci, L.B. Self-Reported Chronic Back Pain and Current Depression in Brazil: A National Level Study. Int. J. Environ. Res. Public Health 2023, 20, 5501. https://doi.org/10.3390/ijerph20085501
Norris RJ, Oancea SC, Nucci LB. Self-Reported Chronic Back Pain and Current Depression in Brazil: A National Level Study. International Journal of Environmental Research and Public Health. 2023; 20(8):5501. https://doi.org/10.3390/ijerph20085501
Chicago/Turabian StyleNorris, Ryan J., S. Cristina Oancea, and Luciana B. Nucci. 2023. "Self-Reported Chronic Back Pain and Current Depression in Brazil: A National Level Study" International Journal of Environmental Research and Public Health 20, no. 8: 5501. https://doi.org/10.3390/ijerph20085501
APA StyleNorris, R. J., Oancea, S. C., & Nucci, L. B. (2023). Self-Reported Chronic Back Pain and Current Depression in Brazil: A National Level Study. International Journal of Environmental Research and Public Health, 20(8), 5501. https://doi.org/10.3390/ijerph20085501