
A Pilot Study of the Effects of Individualized Home Dual Task Training by Mobile Health Technology in People with Dementia

 and
and
Abstract
1. Introduction
2. Materials and Methods
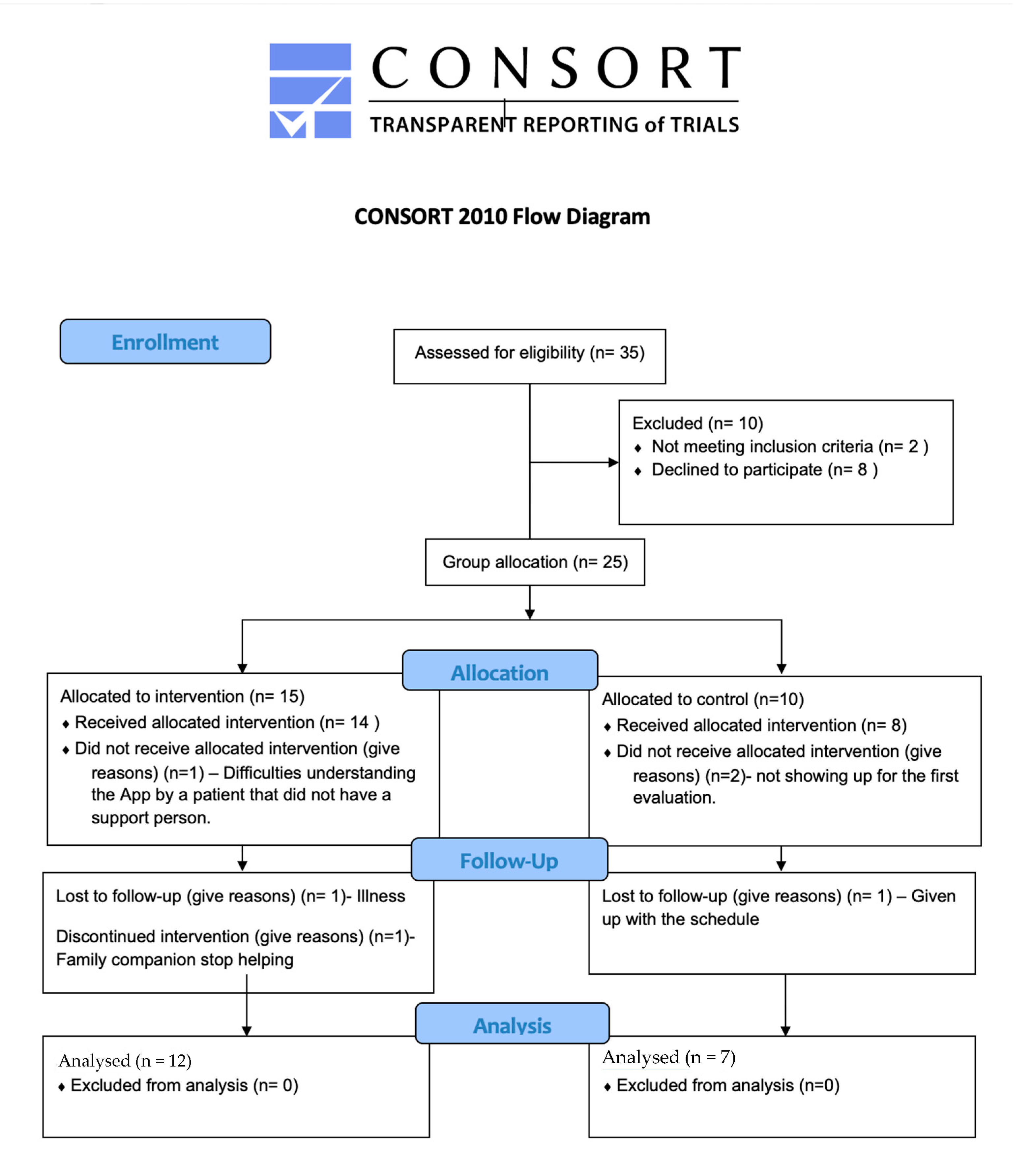
2.1. Study Participants
2.2. Procedure
2.3. Motor and Dual-Task Assessments
2.3.1. Gait at Preferred Speed
2.3.2. Gait Dual Task
2.3.3. Gait at Maximal Speed
2.3.4. Timed Up and Go (TUG)
2.3.5. Handgrip Strength Measurement
2.4. Intervention
3. Statistical Analysis
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brodaty, H.; Donkin, M. Family caregivers of people with dementia. Dialogues Clin. Neurosci. 2009, 11, 217–228. [Google Scholar] [CrossRef] [PubMed]
- Forbes, D.; Forbes, S.C.; Blake, C.M.; Thiessen, E.J.; Forbes, S. Exercise programs for people with dementia. Cochrane Database Syst. Rev. 2015, 4, CD006489. [Google Scholar] [CrossRef] [PubMed]
- Jia, R.-X.; Liang, J.-H.; Xu, Y.; Wang, Y.-Q. Effects of physical activity and exercise on the cognitive function of patients with Alzheimer disease: A meta-analysis. BMC Geriatr. 2019, 19, 181. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.-T.; Xu, W.; Tan, C.-C.; Andrieu, S.; Suckling, J.; Evangelou, E.; Pan, A.; Zhang, C.; Jia, J.; Feng, L.; et al. Evidence-based prevention of Alzheimer’s disease: Systematic review and meta-analysis of 243 observational prospective studies and 153 randomised controlled trials. J. Neurol. Neurosurg. Psychiatry 2020, 91, 1201–1209. [Google Scholar] [CrossRef]
- Karssemeijer, E.G.A.; Aaronson, J.A.; Bossers, W.J.; Smits, T.; Olde Rikkert, M.G.M.; Kessels, R.P.C. Positive effects of combined cognitive and physical exercise training on cognitive function in older adults with mild cognitive impairment or dementia: A meta-analysis. Ageing Res. Rev. 2017, 40, 75–83. [Google Scholar] [CrossRef]
- Yang, H.; Luo, Y.; Hu, Q.; Tian, X.; Wen, H. Benefits in Alzheimer’s Disease of Sensory and Multisensory Stimulation. J. Alzheimer’s Dis. 2021, 82, 463–484. [Google Scholar] [CrossRef]
- Dietrich, M.O.; Andrews, Z.B.; Horvath, T.L. Exercise-Induced Synaptogenesis in the Hippocampus Is Dependent on UCP2-Regulated Mitochondrial Adaptation. J. Neurosci. 2008, 28, 10766–10771. [Google Scholar] [CrossRef]
- Colcombe, S.J.; Erickson, K.I.; Scalf, P.E.; Kim, J.S.; Prakash, R.; McAuley, E.; Elavsky, S.; Marquez, D.X.; Hu, L.; Kramer, A.F. Aerobic Exercise Training Increases Brain Volume in Aging Humans. J. Gerontol. Ser. A 2006, 61, 1166–1170. [Google Scholar] [CrossRef]
- Nokia, M.S.; Lensu, S.; Ahtiainen, J.; Johansson, P.P.; Koch, L.G.; Britton, S.L.; Kainulainen, H. Physical exercise increases adult hippocampal neurogenesis in male rats provided it is aerobic and sustained. J. Physiol. 2016, 594, 1855–1873. [Google Scholar] [CrossRef]
- Martorell, A.J.; Paulson, A.L.; Suk, H.-J.; Abdurrob, F.; Drummond, G.T.; Guan, W.; Young, J.Z.; Kim, D.N.-W.; Kritskiy, O.; Barker, S.J.; et al. Multi-sensory Gamma Stimulation Ameliorates Alzheimer’s-Associated Pathology and Improves Cognition. Cell 2019, 177, 256–271.e22. [Google Scholar] [CrossRef]
- King, J.B.; Jones, K.; Goldberg, E.; Rollins, M.; MacNamee, K.; Moffit, C.; Naidu, S.R.; Ferguson, M.A.; Garcia-Leavitt, E.; Amaro, J.; et al. Increased functional connectivity after listening to favored music in adults with Alzheimer dementia. J. Prev. Alzheimer’s Dis. 2019, 6, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Morris, M.E.; Martin, C.L.; Schenkman, M.L. Striding Out With Parkinson Disease: Evidence-Based Physical Therapy for Gait Disorders. Phys. Ther. Rehabil. J. 2010, 90, 2. [Google Scholar] [CrossRef] [PubMed]
- Eplummer, P.; Eskes, G.A. Measuring treatment effects on dual-task performance: A framework for research and clinical practice. Front. Hum. Neurosci. 2015, 9, 225. [Google Scholar] [CrossRef]
- Roos, M.A.; Rudolph, K.S.; Reisman, D.S. The Structure of Walking Activity in People After Stroke Compared With Older Adults Without Disability: A Cross-Sectional Study. Phys. Ther. Rehabil. J. 2012, 92, 1141–1147. [Google Scholar] [CrossRef] [PubMed]
- Fritz, N.E.; Cheek, F.M.; Nichols-Larsen, D.S. Motor-Cognitive Dual-Task Training in Persons With Neurologic Disorders. J. Neurol. Phys. Ther. 2015, 39, 142–153. [Google Scholar] [CrossRef]
- Friedman, N.P.; Robbins, T.W. The role of prefrontal cortex in cognitive control and executive function. Neuropsychopharmacology 2021, 47, 72–89. [Google Scholar] [CrossRef] [PubMed]
- McMaughan, D.J.; Oloruntoba, O.; Smith, M.L. Socioeconomic Status and Access to Healthcare: Interrelated Drivers for Healthy Aging. Front. Public Health 2020, 8, 231. [Google Scholar] [CrossRef]
- Kivimäki, M.; Batty, G.D.; Pentti, J.; Shipley, M.J.; Sipilä, P.; Nyberg, S.T.; Suominen, S.B.; Oksanen, T.; Stenholm, S.; Virtanen, M.; et al. Association between socioeconomic status and the development of mental and physical health conditions in adulthood: A multi-cohort study. Lancet Public Health 2020, 5, e140–e149. [Google Scholar] [CrossRef]
- Appel, A.M.; Brønnum-Hansen, H.; Garde, A.H.; Hansen, M.; Ishtiak-Ahmed, K.; Islamoska, S.; Mortensen, E.L.; Osler, M.; Nabe-Nielsen, K. Socioeconomic Position and Late-Onset Dementia: A Nationwide Register-Based Study. J. Aging Health 2021, 34, 184–195. [Google Scholar] [CrossRef]
- Ministerio de Inclusión, Seguridad Social y Migraciones; Instituto de Mayores y Servicios Sociales (IMSERSO). Convenio Especial de Cuidadores no Profesionales de Personas en Situación de Dependencia. 2014. Available online: https://www.seg-social.es/wps/portal/wss/internet/Trabajadores/Afiliacion/10547/10555/51635 (accessed on 3 February 2023).
- Censo de Personas con Alzheimer y Otras Demencias en España. Available online: https://www.ceafa.es/alzheimer-blog/noticias/censo-las-personas-con-alzheimer-otras-demencias-espana (accessed on 3 February 2023).
- Hill, K.D.; Hunter, S.W.; Batchelor, F.A.; Cavalheri, V.; Burton, E. Individualized home-based exercise programs for older people to reduce falls and improve physical performance: A systematic review and meta-analysis. Maturitas 2015, 82, 72–84. [Google Scholar] [CrossRef]
- Kaufman, B.G.; Thomas, S.R.; Randolph, R.K.; Perry, J.R.; Thompson, K.W.; Holmes, G.M.; Pink, G.H. The Rising Rate of Rural Hospital Closures. J. Rural Health 2015, 32, 35–43. [Google Scholar] [CrossRef]
- Glauber, R. Rural depopulation and the rural-urban gap in cognitive functioning among older adults. J. Rural Health 2022, 38, 696–704. [Google Scholar] [CrossRef]
- Ramey, L.; Osborne, C.; Kasitinon, D.; Juengst, S. Apps and Mobile Health Technology in Rehabilitation. Phys. Med. Rehabil. Clin. N. Am. 2019, 30, 485–497. [Google Scholar] [CrossRef]
- Arevalo-Rodriguez, I.; Smailagic, N.; Roqué-Figuls, M.; Ciapponi, A.; Sanchez-Perez, E.; Giannakou, A.; Pedraza, O.L.; Cosp, X.B.; Cullum, S. Mini-Mental State Examination (MMSE) for the early detection of dementia in people with mild cognitive impairment (MCI). Cochrane Database Syst. Rev. 2021, 2021, CD010783. [Google Scholar] [CrossRef]
- Pangman, V.C.; Sloan, J.; Guse, L. An examination of psychometric properties of the Mini-Mental State Examination and the Standardized Mini-Mental State Examination: Implications for clinical practice. Appl. Nurs. Res. 2000, 13, 209–213. [Google Scholar] [CrossRef]
- Crum, R.M. Population-Based Norms for the Mini-Mental State Examination by Age and Educational Level. JAMA 1993, 269, 2386. [Google Scholar] [CrossRef] [PubMed]
- Lawton, M.P.; Brody, E.M. Assessment of older people: Self-maintaining and instrumental activities of daily living. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Mahoney, F.I.; Barthel, D.W. Functional evaluation: The Barthel Index. Md. State Med. J. 1965, 14, 61–65. [Google Scholar]
- Lee, M.M.; Song, C.H.; Lee, K.J.; Jung, S.W.; Shin, D.C.; Shin, S.H. Concurrent Validity and Test-retest Reliability of the OPTOGait Photoelectric Cell System for the Assessment of Spatio-temporal Parameters of the Gait of Young Adults. J. Phys. Ther. Sci. 2014, 26, 81–85. [Google Scholar] [CrossRef]
- Montero-Odasso, M.; Muir, S.W.; Speechley, M. Dual-Task Complexity Affects Gait in People With Mild Cognitive Impairment: The Interplay Between Gait Variability, Dual Tasking, and Risk of Falls. Arch. Phys. Med. Rehabil. 2012, 93, 293–299. [Google Scholar] [CrossRef]
- Muhaidat, J.; Kerr, A.; Evans, J.J.; Pilling, M.; Skelton, D.A. Validity of Simple Gait-Related Dual-Task Tests in Predicting Falls in Community-Dwelling Older Adults. Arch. Phys. Med. Rehabil. 2013, 95, 58–64. [Google Scholar] [CrossRef]
- Yogev-Seligmann, G.; Hausdorff, J.M.; Giladi, N. Do we always prioritize balance when walking? Towards an integrated model of task prioritization. Mov. Disord. 2012, 27, 765–770. [Google Scholar] [CrossRef]
- Podsiadlo, D.; Richardson, S. The Timed “Up & Go”: A Test of Basic Functional Mobility for Frail Elderly Persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Luque-Casado, A.; Novo-Ponte, S.; Sánchez-Molina, J.A.; Sevilla-Sánchez, M.; Santos-García, D.; Fernández-Del-Olmo, M. Test-Retest Reliability of the Timed Up and Go Test in Subjects with Parkinson’s Disease: Implications for Longitudinal Assessments. J. Park. Dis. 2021, 11, 2047–2055. [Google Scholar] [CrossRef] [PubMed]
- Morris, S.; Morris, M.; Iansek, R. Reliability of Measurements Obtained With the Timed “Up & Go” Test in People With Parkinson Disease. Phys. Ther. 2001, 81, 810–818. [Google Scholar] [CrossRef]
- Villafañe, J.H.; Valdes, K.; Buraschi, R.; Martinelli, M.; Bissolotti, L.; Negrini, S. Reliability of the Handgrip Strength Test in Elderly Subjects With Parkinson Disease. Hand 2016, 11, 54–58. [Google Scholar] [CrossRef] [PubMed]
- Montero-Odasso, M.; Speechley, M. Falls in Cognitively Impaired Older Adults: Implications for Risk Assessment And Prevention. J. Am. Geriatr. Soc. 2018, 66, 367–375. [Google Scholar] [CrossRef]
- Cottone, C.; Porcaro, C.; Cancelli, A.; Olejarczyk, E.; Salustri, C.; Tecchio, F. Neuronal electrical ongoing activity as a signature of cortical areas. Anat. Embryol. 2016, 222, 2115–2126. [Google Scholar] [CrossRef]
- Dettmers, C.; Fink, G.R.; Lemon, R.N.; Stephan, K.M.; Passingham, R.E.; Silbersweig, D.; Holmes, A.; Ridding, M.C.; Brooks, D.; Frackowiak, R. Relation between cerebral activity and force in the motor areas of the human brain. J. Neurophysiol. 1995, 74, 802–815. [Google Scholar] [CrossRef]
- Baker, L.D.; Frank, L.L.; Foster-Schubert, K.; Green, P.S.; Wilkinson, C.; McTiernan, A.; Plymate, S.R.; Fishel, M.A.; Watson, G.S.; Cholerton, B.A.; et al. Effects of Aerobic Exercise on Mild Cognitive Impairment. Arch. Neurol. 2010, 67, 71–79. [Google Scholar] [CrossRef]
- Bloem, B.R.; Grimbergen, Y.A.; van Dijk, J.G.; Munneke, M. The “posture second” strategy: A review of wrong priorities in Parkinson’s disease. J. Neurol. Sci. 2006, 248, 196–204. [Google Scholar] [CrossRef] [PubMed]
- Schwenk, M.; Zieschang, T.; Oster, P.; Hauer, K. Dual-task performances can be improved in patients with dementia: A randomized controlled trial. Neurology 2010, 74, 1961–1968. [Google Scholar] [CrossRef] [PubMed]
- Bucci, S.; Schwannauer, M.; Berry, N. The digital revolution and its impact on mental health care. Psychol. Psychother. Theory, Res. Pract. 2019, 92, 277–297. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Diagnostic | Age | Sex | MMSE | IADL | BI |
|---|---|---|---|---|---|
| Vascular dementia | 66 | M | 30 | 4 | 100 |
| Parkinson’s disease | 74 | M | 24 | 3 | 95 |
| Alzheimer’s disease | 69 | F | 18 | 3 | 100 |
| Parkinson’s disease | 74 | M | 28 | 4 | 95 |
| Alzheimer’s disease | 77 | M | 30 | 5 | 100 |
| Alzheimer’s disease | 74 | M | 25 | 8 | 100 |
| Mild cognitive impairment | 68 | F | 19 | 8 | 100 |
| Parkinson’s disease | 69 | M | 22 | 7 | 90 |
| Lewy body dementia | 72 | M | 23 | 5 | 90 |
| Alzheimer’s disease | 79 | M | 16 | 2 | 85 |
| Alzheimer’s disease | 77 | M | 20 | 3 | 100 |
| Alzheimer’s disease | 76 | M | 21 | 2 | 85 |
| Alzheimer’s disease | 79 | M | 26 | 8 | 100 |
| Alzheimer’s disease | 65 | M | 9 | 0 | 55 |
| Parkinson’s disease | 79 | M | 24 | 3 | 100 |
| Mild cognitive impairment | 79 | M | 17 | 5 | 100 |
| Alzheimer’s disease | 65 | F | 13 | 4 | 100 |
| Parkinson’s disease | 69 | F | 23 | 7 | 100 |
| Alzheimer’s disease | 70 | F | 22 | 5 | 95 |
| Age | Sex | MMSE | IADL | BI | |
|---|---|---|---|---|---|
| Overall sample (n = 19) | 72 ± 4 (65–79) | 14 males 5 females | 21 ± 5.6 (9–30) | 4 ± 2.25 (0–8) | 93 ± 11 (55–100) |
| Experimental Group (EG) (n = 12) | 72 ± 4 (66–79) | 10 males 2 females | 23 ± 5.36 (16–30) | 4 ± 2.26 (2–8) | 96 ± 5.39 (85–100) |
| Control Group (CG) (n = 7) | 72 ± 7 (65–79) | 4 males 2 females | 18 ± 6.66 (9–24) | 4 ± 2.64 (0–8) | 91 ± 7.30 (55–100) |
| Task | Experimental Group | Control Group | ||
|---|---|---|---|---|
| Pre | Post | Pre | Post | |
| Walking at preferred speed (m/s) | 1.14 ± 0.14 | 1.07 ± 0.14 | 1.06 ± 0.25 | 1.05 ± 0.19 |
| Walking at maximal speed (m/s) | 1.66 ± 0.33 | 1.60 ± 0.36 | 1.56 ± 0.39 | 1.62 ± 0.27 |
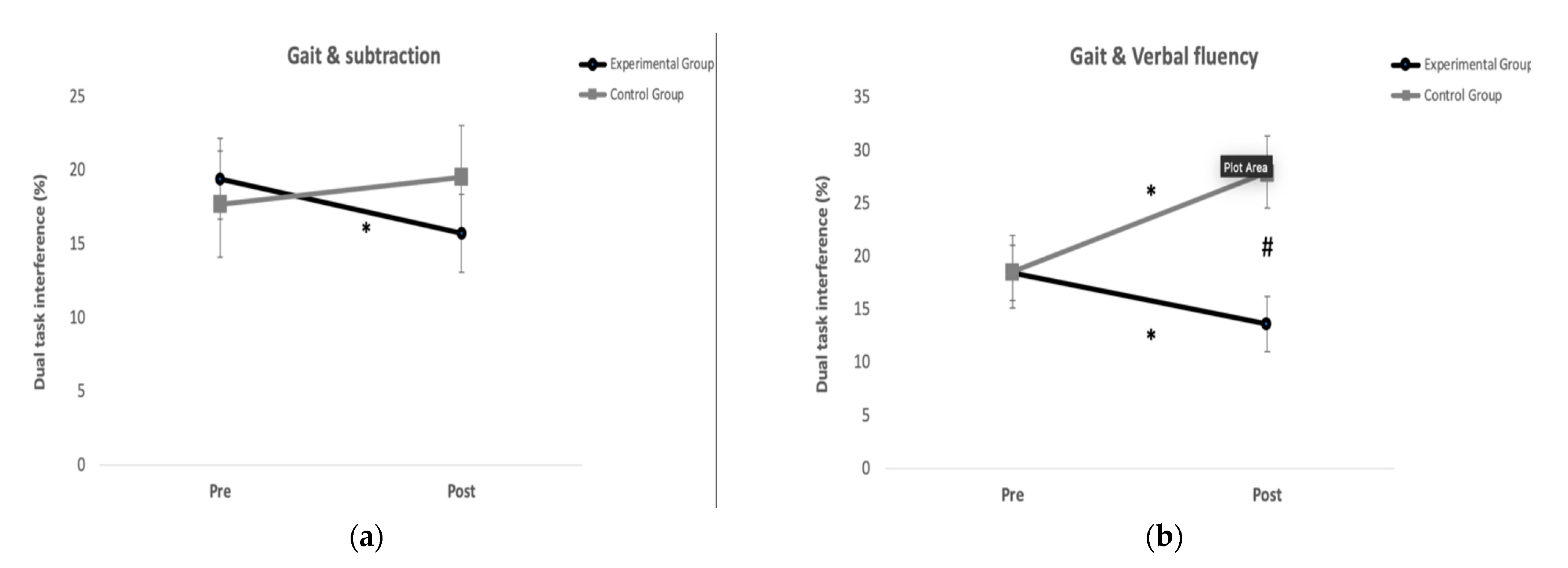
| Dual task interference (%) (Gait and subtraction) | 19.41 ± 10.20 | 15.71 ± 9.36 * | 17.68 ± 8.16 | 19.53 ± 8.88 |
| Dual task interference (%) (Gait and Verbal fluency) | 18.44 ± 9.29 | 13.61 ± 7.17 * | 18.54 ± 8.51 | 27.01± 11.60 *,# |
| Time up and go test (s) | 9.27 ± 1.59 | 9.51 ± 1.93 | 10.21 ± 2.07 | 9.62 ± 2.08 |
| Grip strength dominant hand (N) | 197.17 ± 61.74 | 200.34 ± 54.92 | 231.3 ± 97.65 | 226.78 ± 92.46 |
| Grip strength non-dominant hand (N) | 185.65 ± 55.85 | 193.67 ± 39.53 | 207.49 ± 127 | 208.53 ± 105.13 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Villamil-Cabello, E.; Meneses-Domínguez, M.; Fernández-Rodríguez, Á.; Ontoria-Álvarez, P.; Jiménez-Gutiérrez, A.; Fernández-del-Olmo, M. A Pilot Study of the Effects of Individualized Home Dual Task Training by Mobile Health Technology in People with Dementia. Int. J. Environ. Res. Public Health 2023, 20, 5464. https://doi.org/10.3390/ijerph20085464
Villamil-Cabello E, Meneses-Domínguez M, Fernández-Rodríguez Á, Ontoria-Álvarez P, Jiménez-Gutiérrez A, Fernández-del-Olmo M. A Pilot Study of the Effects of Individualized Home Dual Task Training by Mobile Health Technology in People with Dementia. International Journal of Environmental Research and Public Health. 2023; 20(8):5464. https://doi.org/10.3390/ijerph20085464
Chicago/Turabian StyleVillamil-Cabello, Eduardo, Mercedes Meneses-Domínguez, Ángela Fernández-Rodríguez, Patricia Ontoria-Álvarez, Alfonso Jiménez-Gutiérrez, and Miguel Fernández-del-Olmo. 2023. "A Pilot Study of the Effects of Individualized Home Dual Task Training by Mobile Health Technology in People with Dementia" International Journal of Environmental Research and Public Health 20, no. 8: 5464. https://doi.org/10.3390/ijerph20085464
APA StyleVillamil-Cabello, E., Meneses-Domínguez, M., Fernández-Rodríguez, Á., Ontoria-Álvarez, P., Jiménez-Gutiérrez, A., & Fernández-del-Olmo, M. (2023). A Pilot Study of the Effects of Individualized Home Dual Task Training by Mobile Health Technology in People with Dementia. International Journal of Environmental Research and Public Health, 20(8), 5464. https://doi.org/10.3390/ijerph20085464