
Salus Platform: A Digital Health Solution Tool for Managing Syphilis Cases in Brazil—A Comparative Analysis

 ,
, 
 ,
,  , ,
, ,  ,
,  ,
, 
Abstract
:1. Introduction
1.1. Syphilis
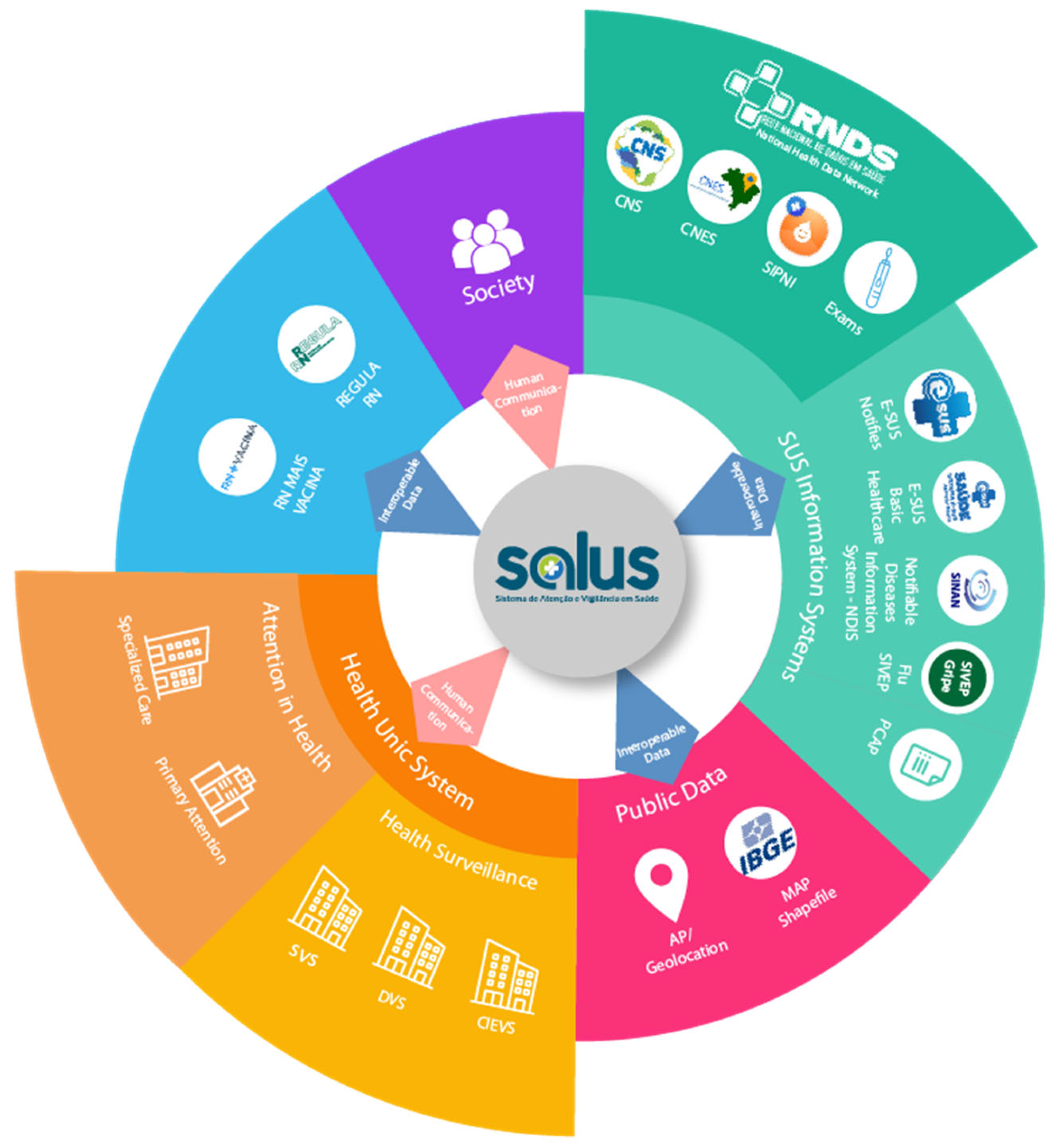
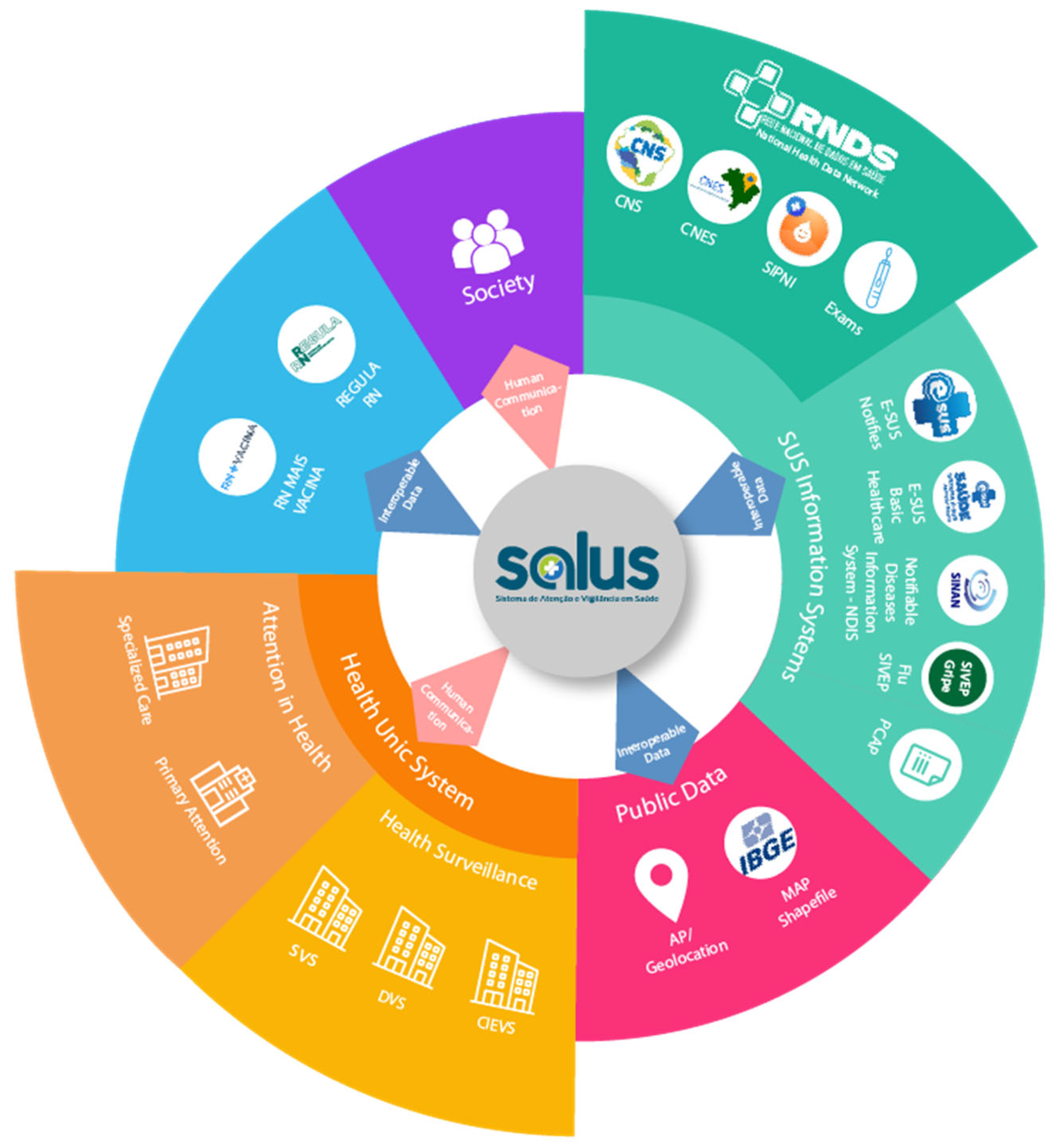
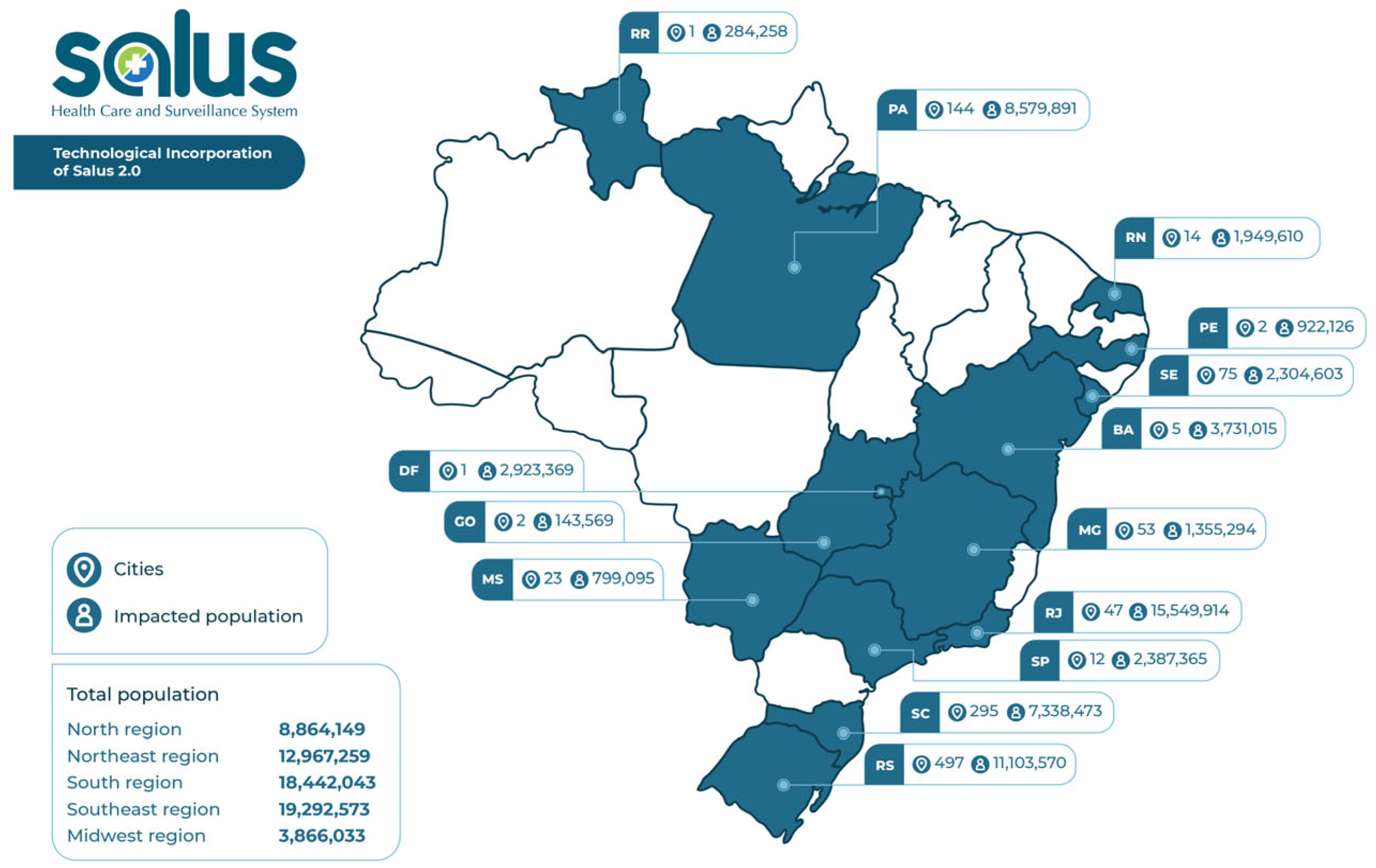
1.2. Salus (Intelligent Disease Monitoring System in Primary Care and Epidemiological Surveillance)
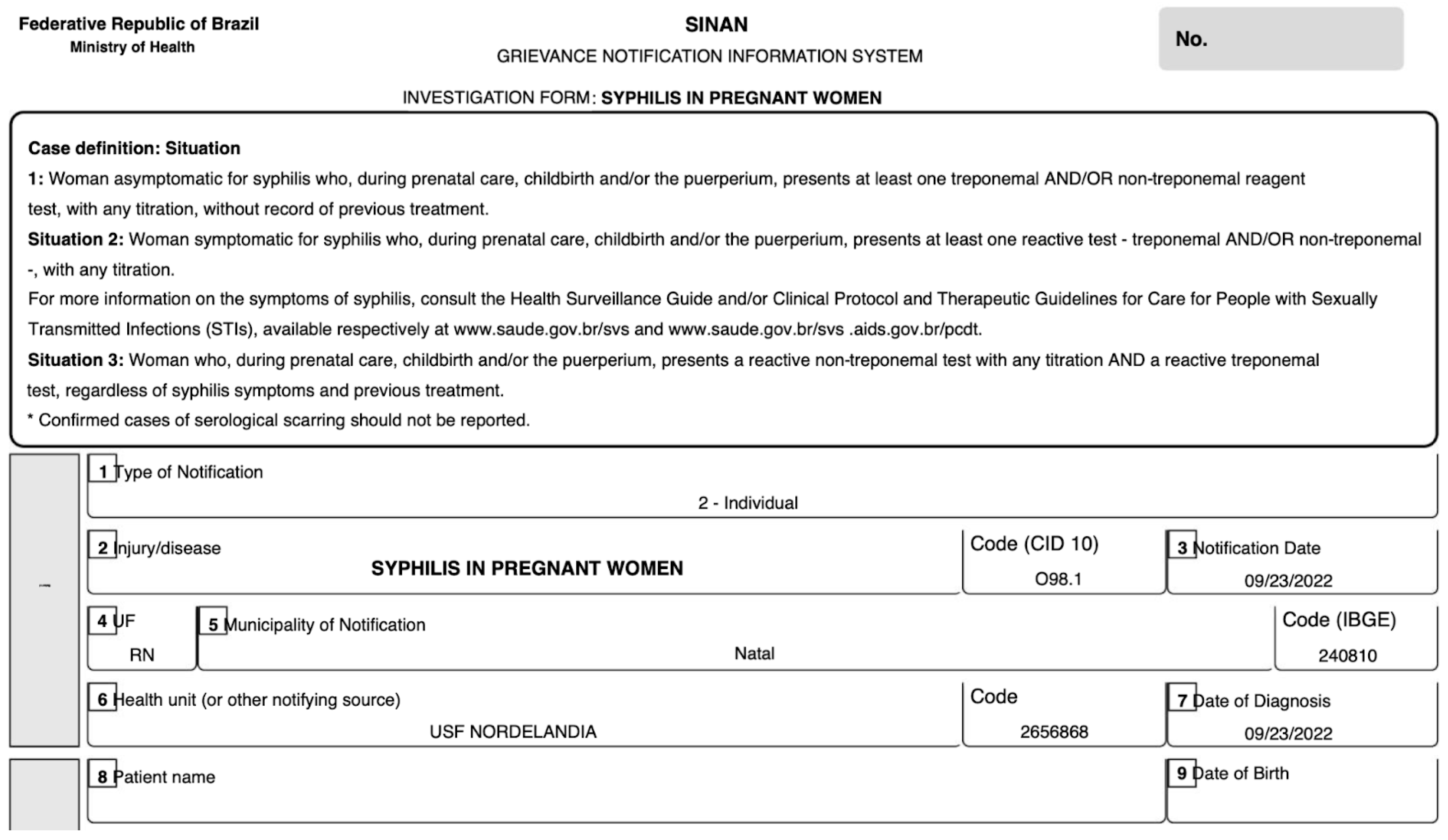
1.3. Data Entry Tools in Health Care in Brazil
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
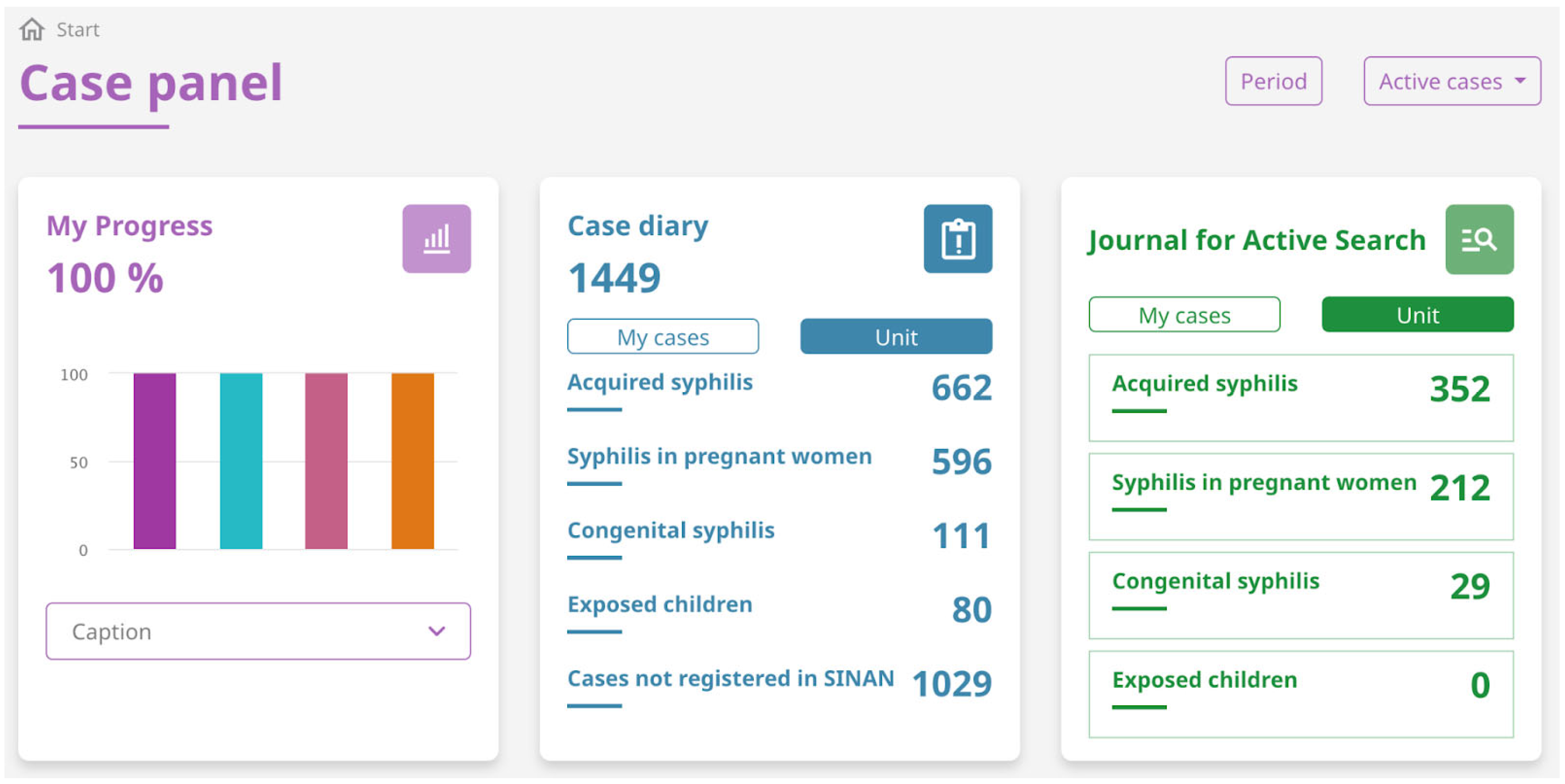
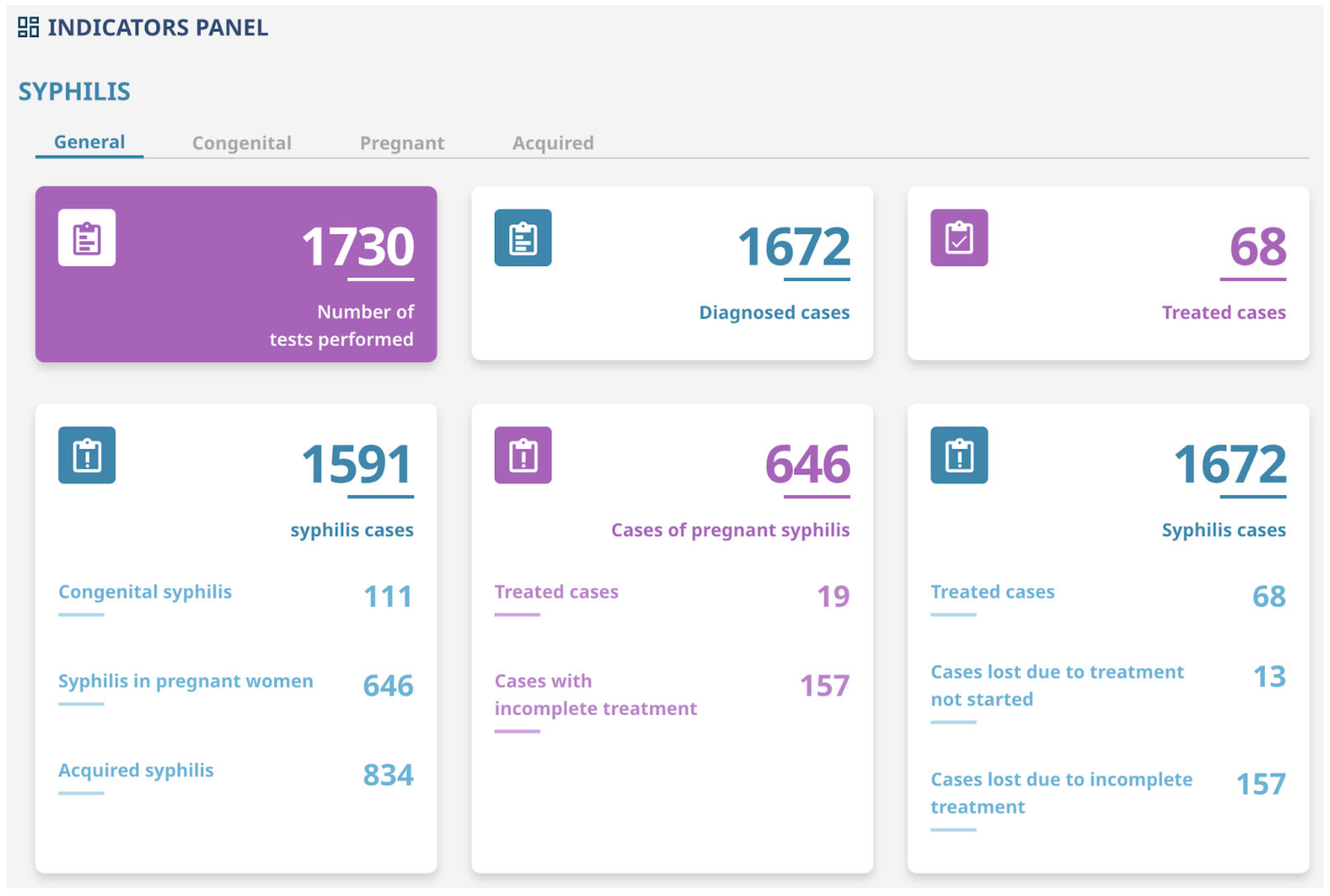
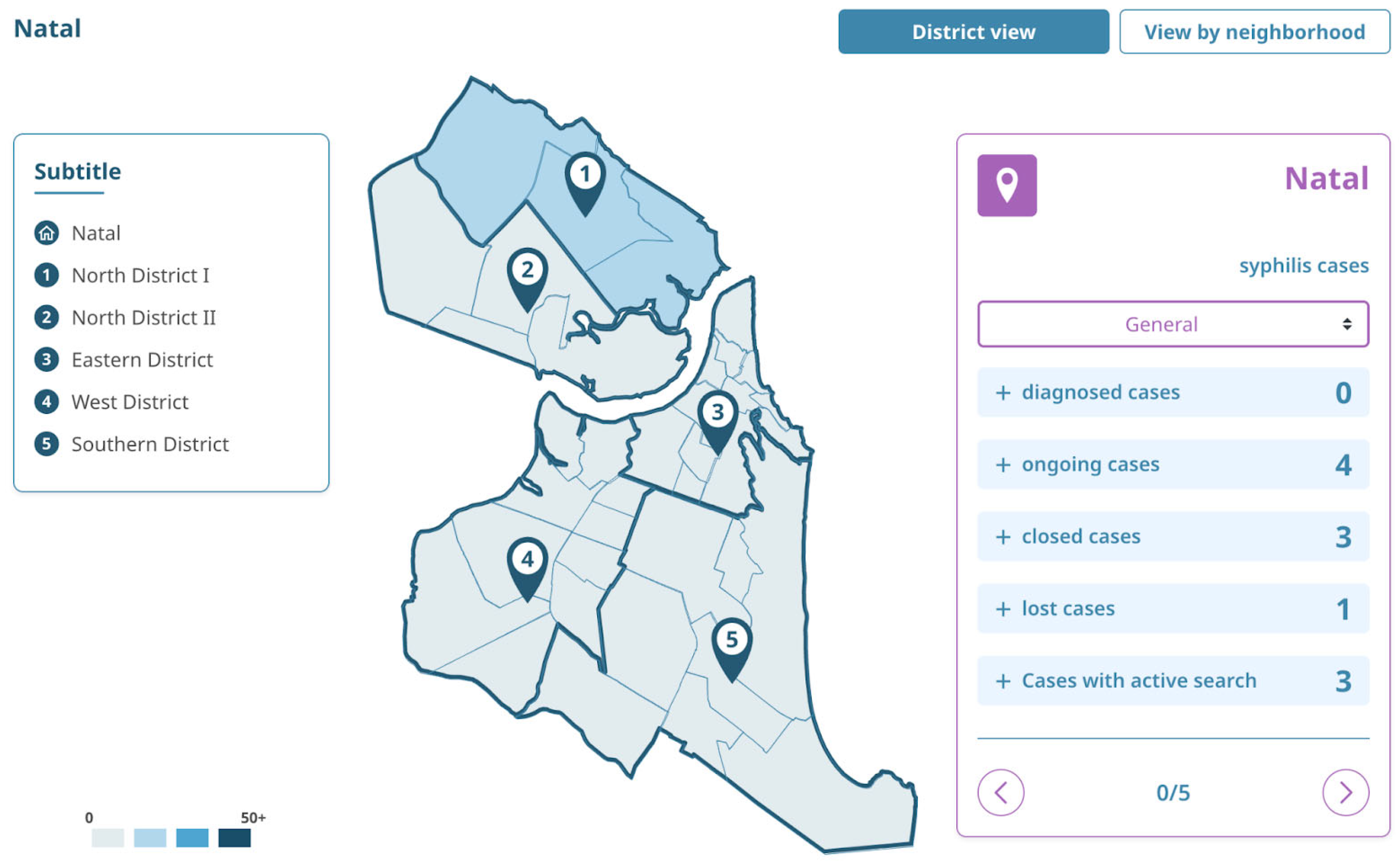
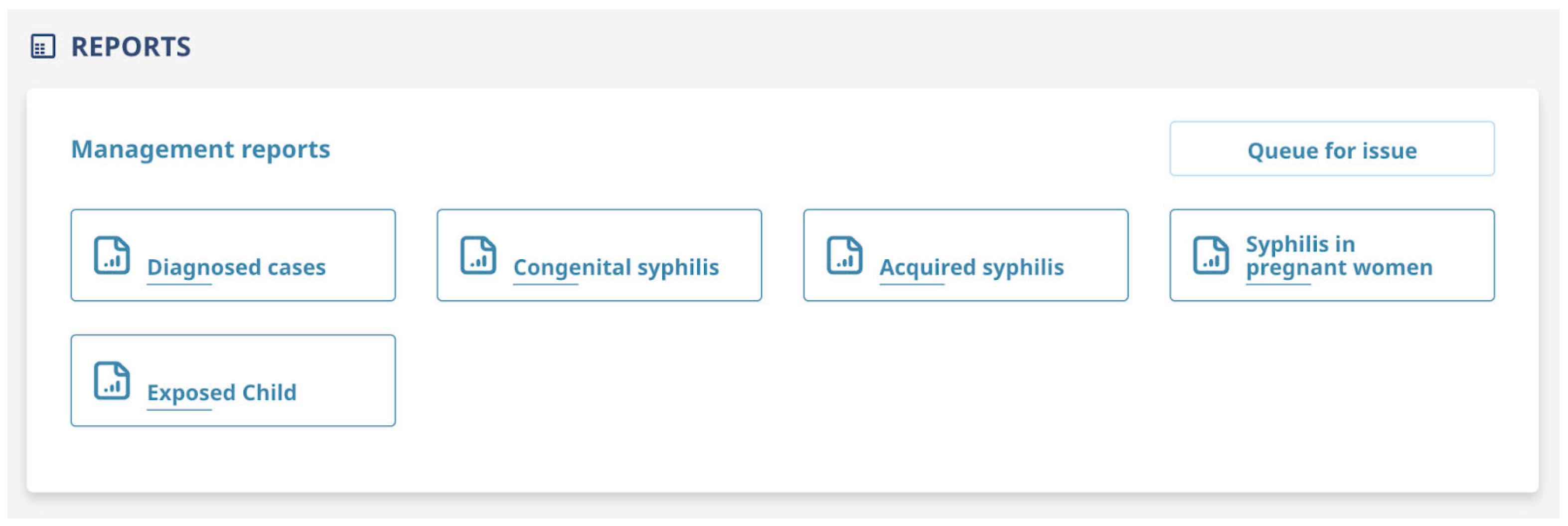
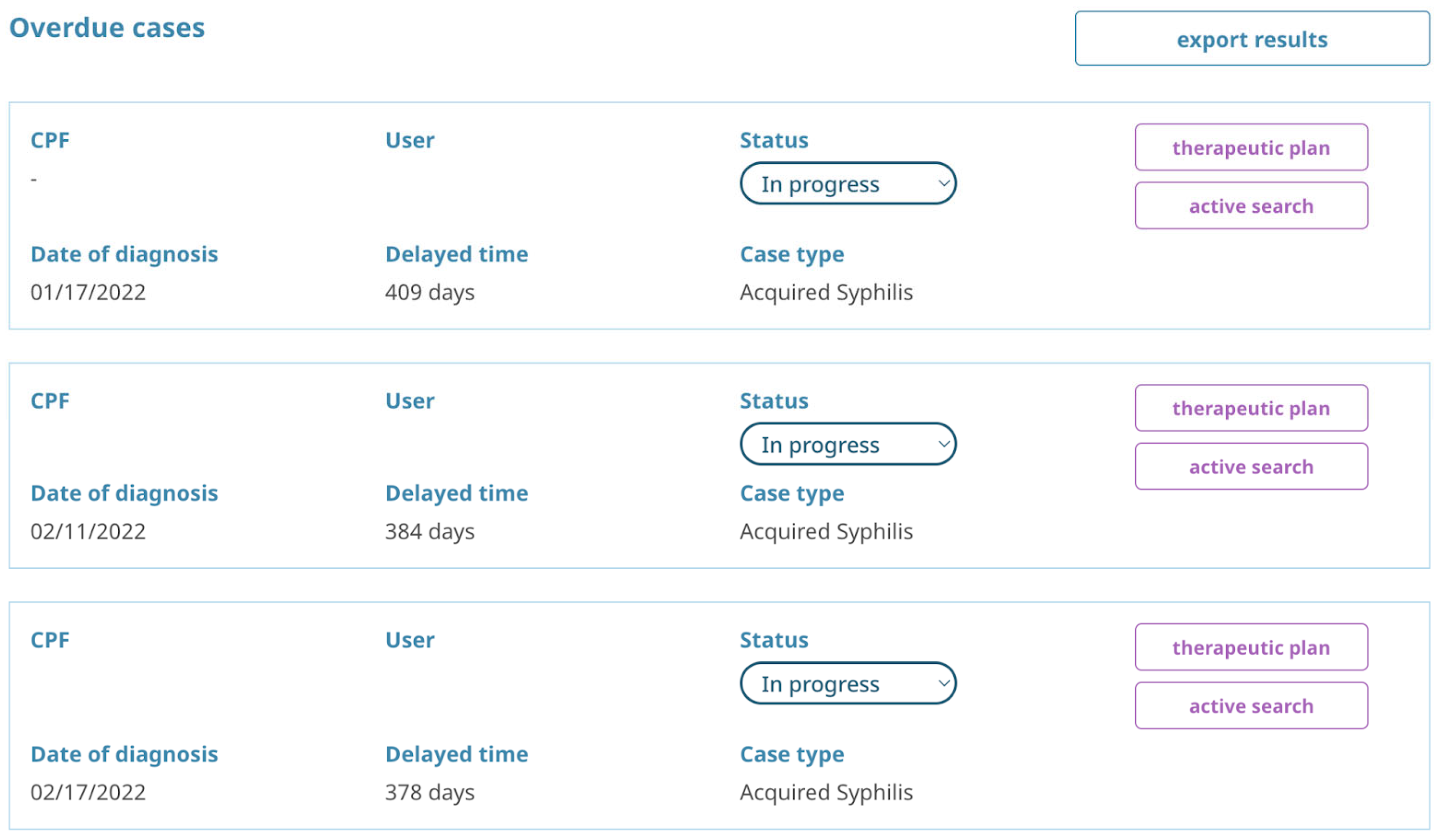
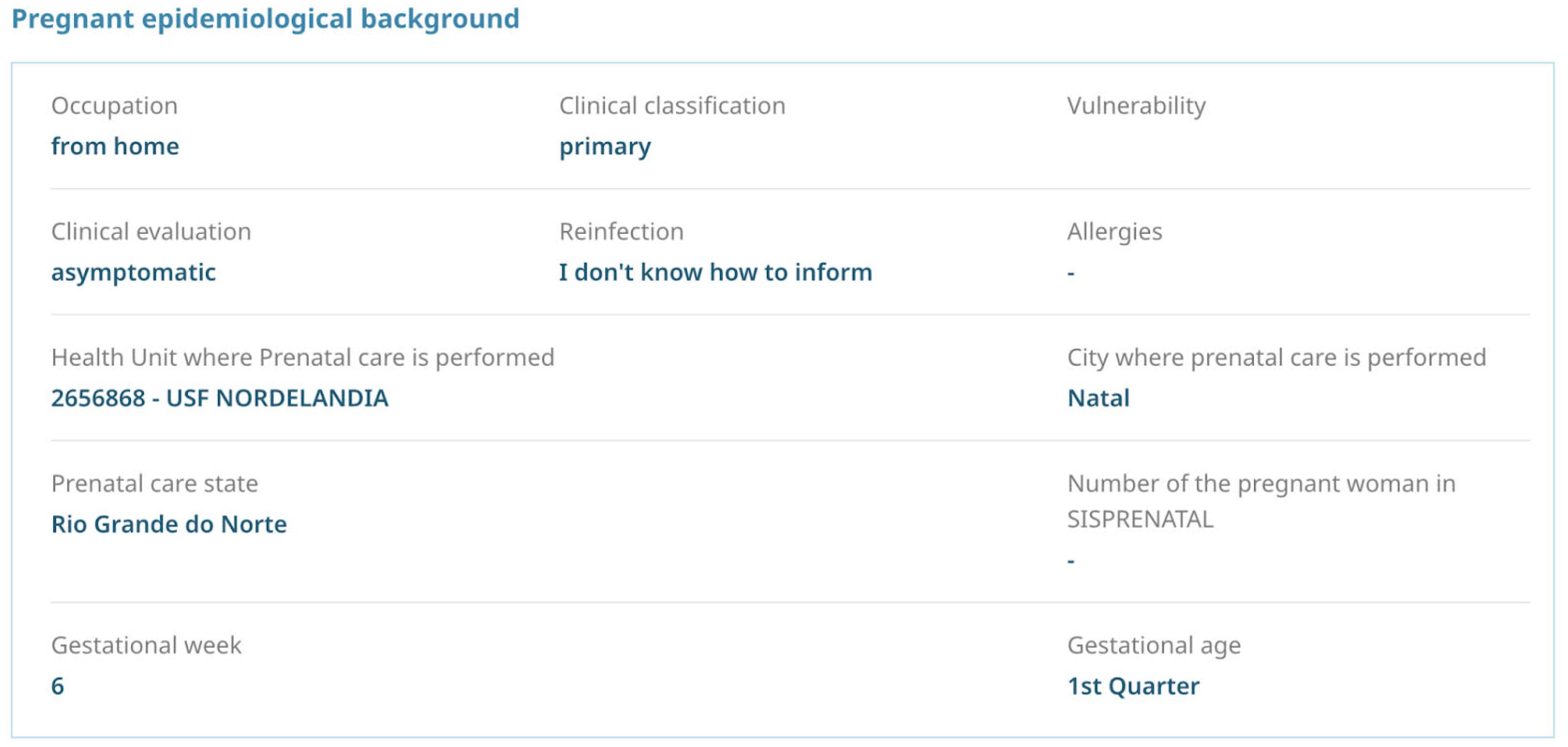
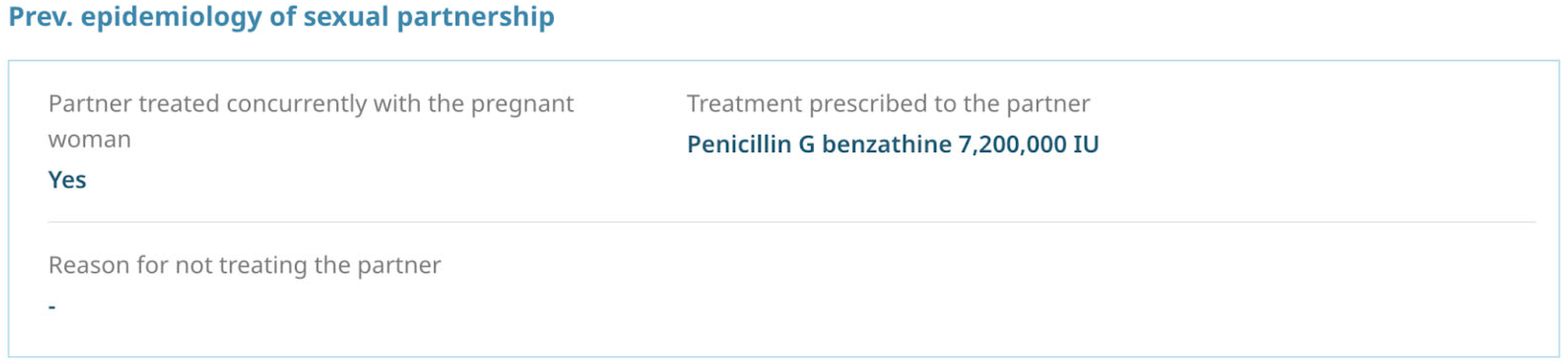
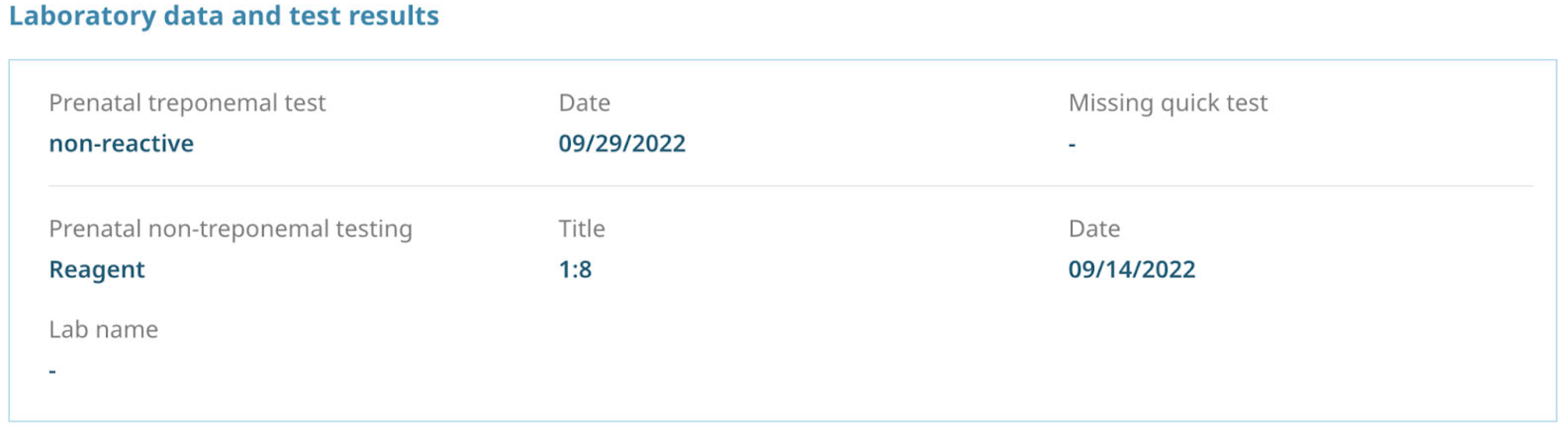
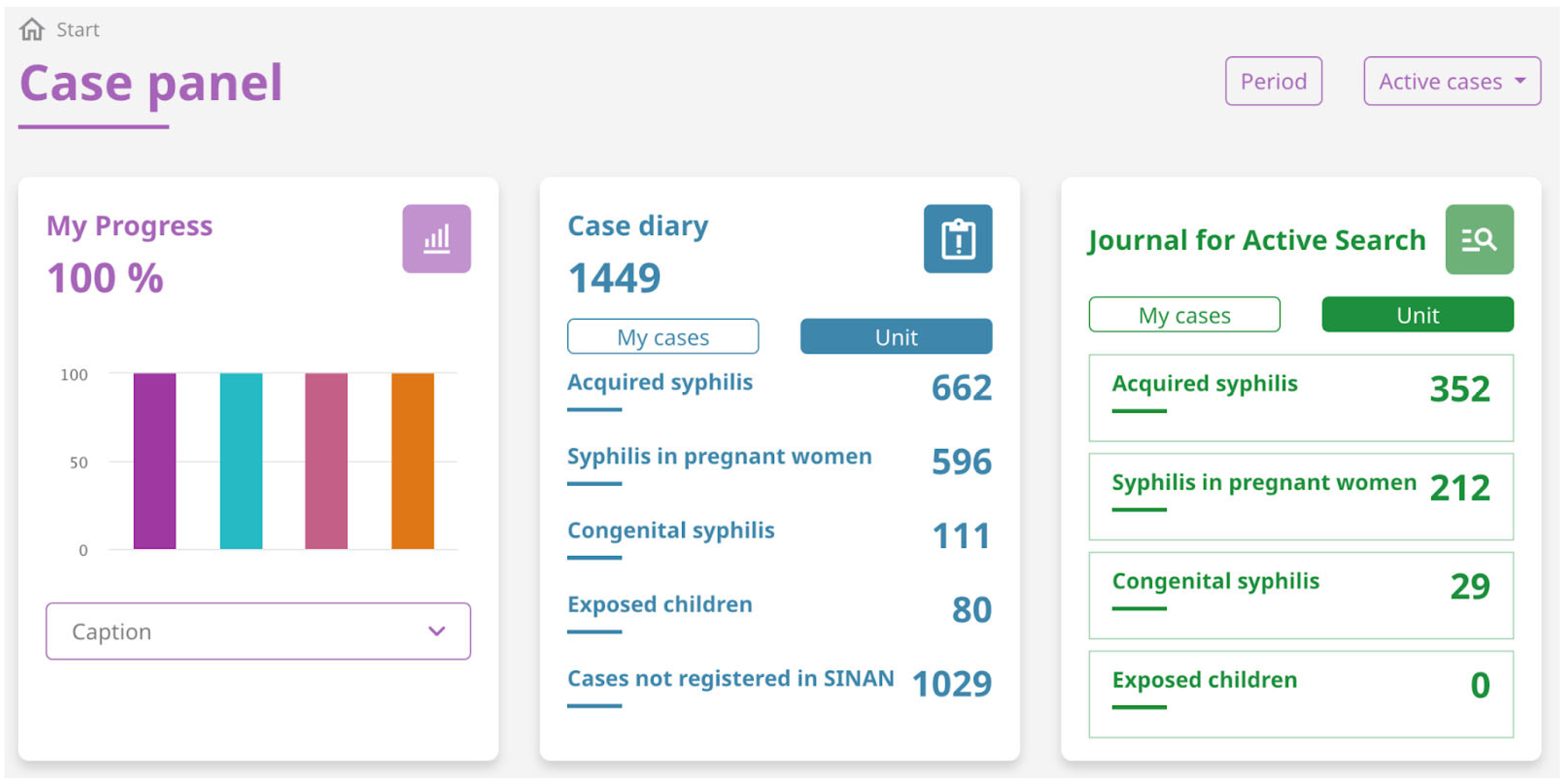
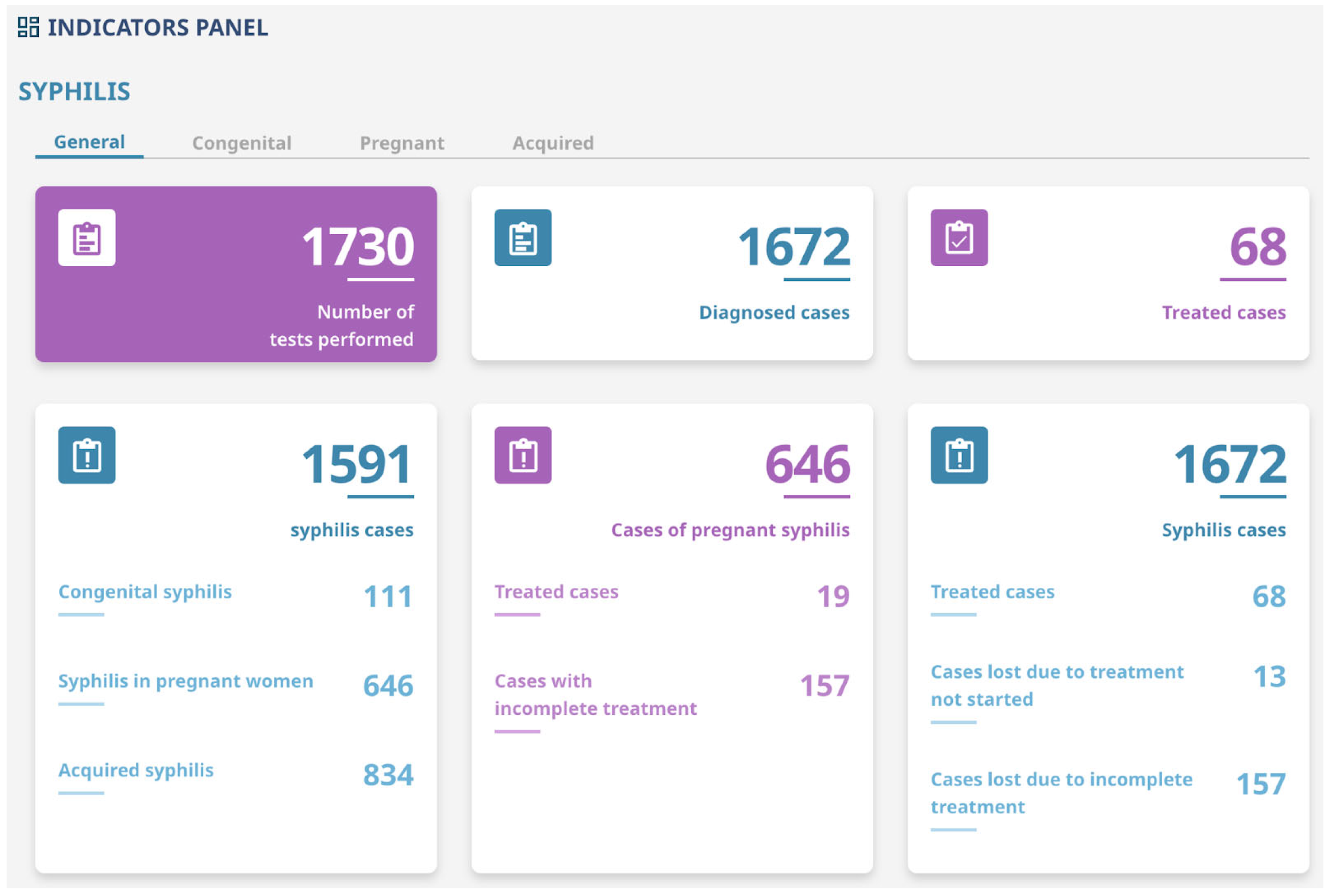
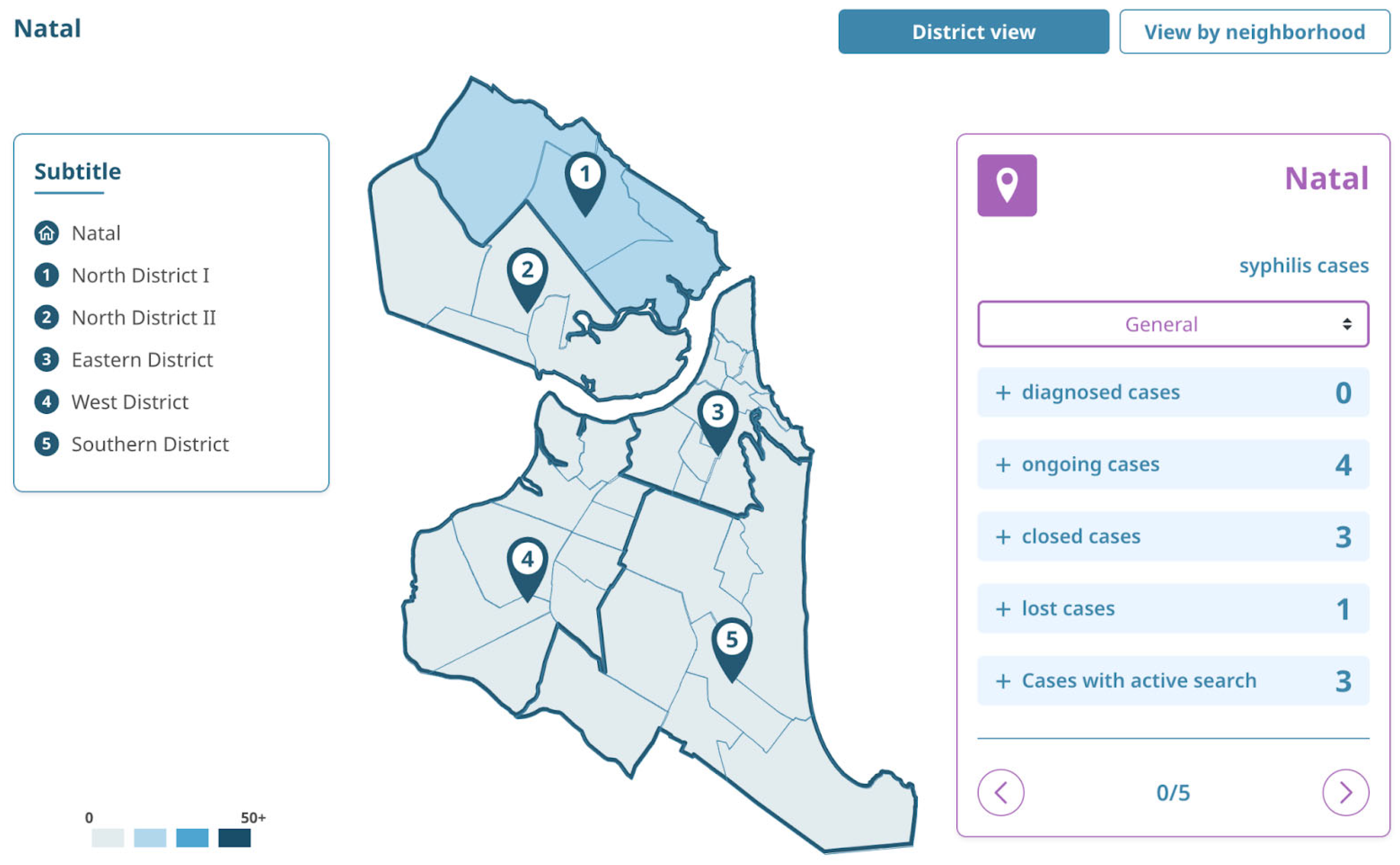
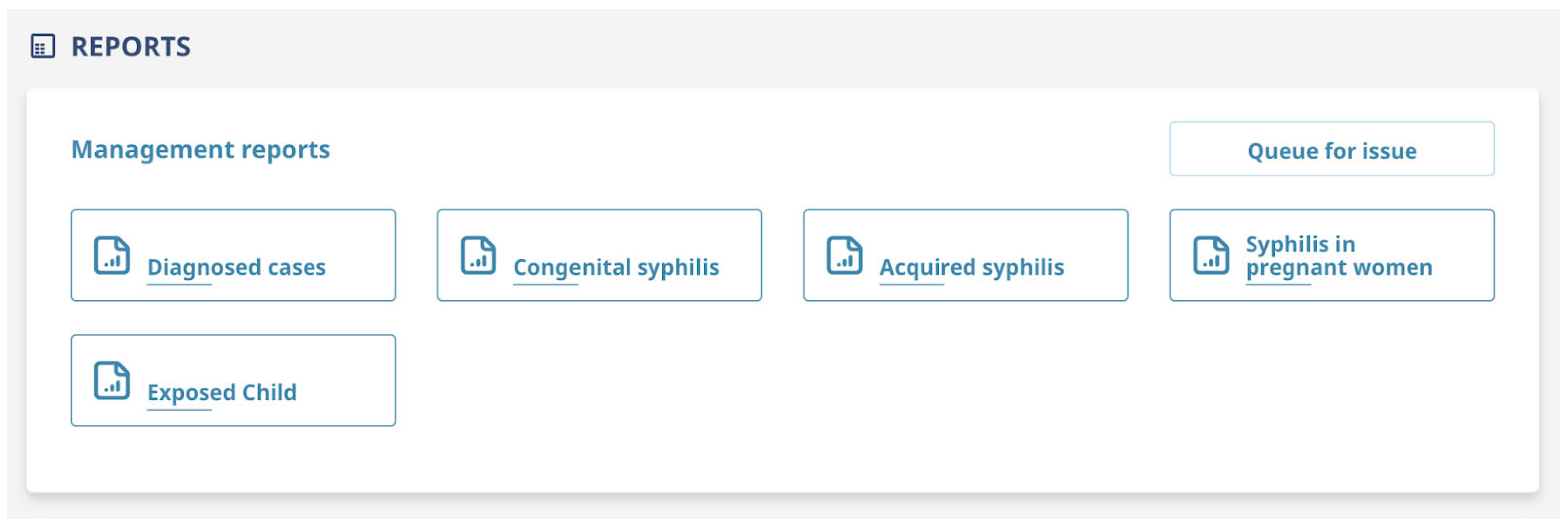
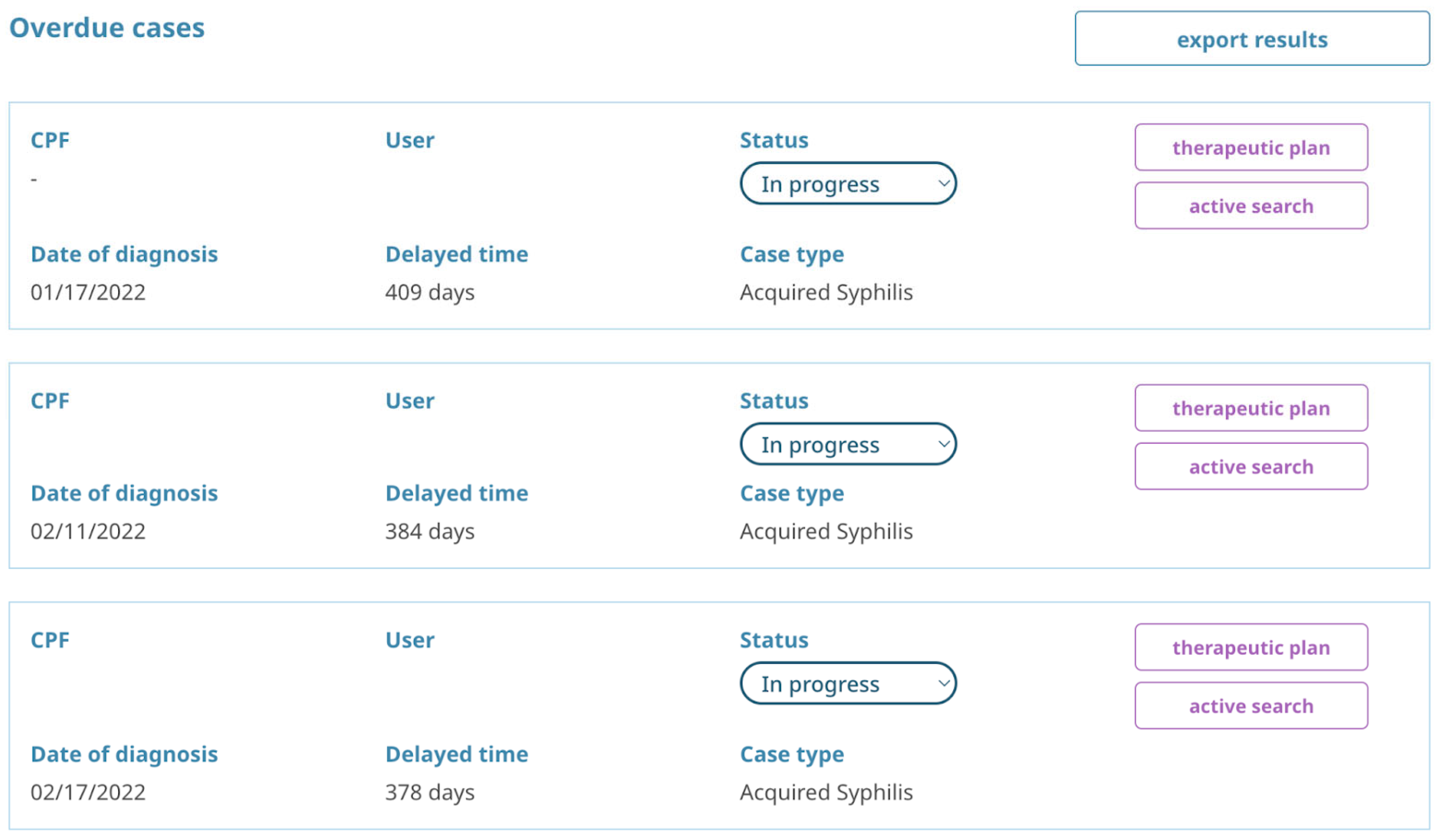
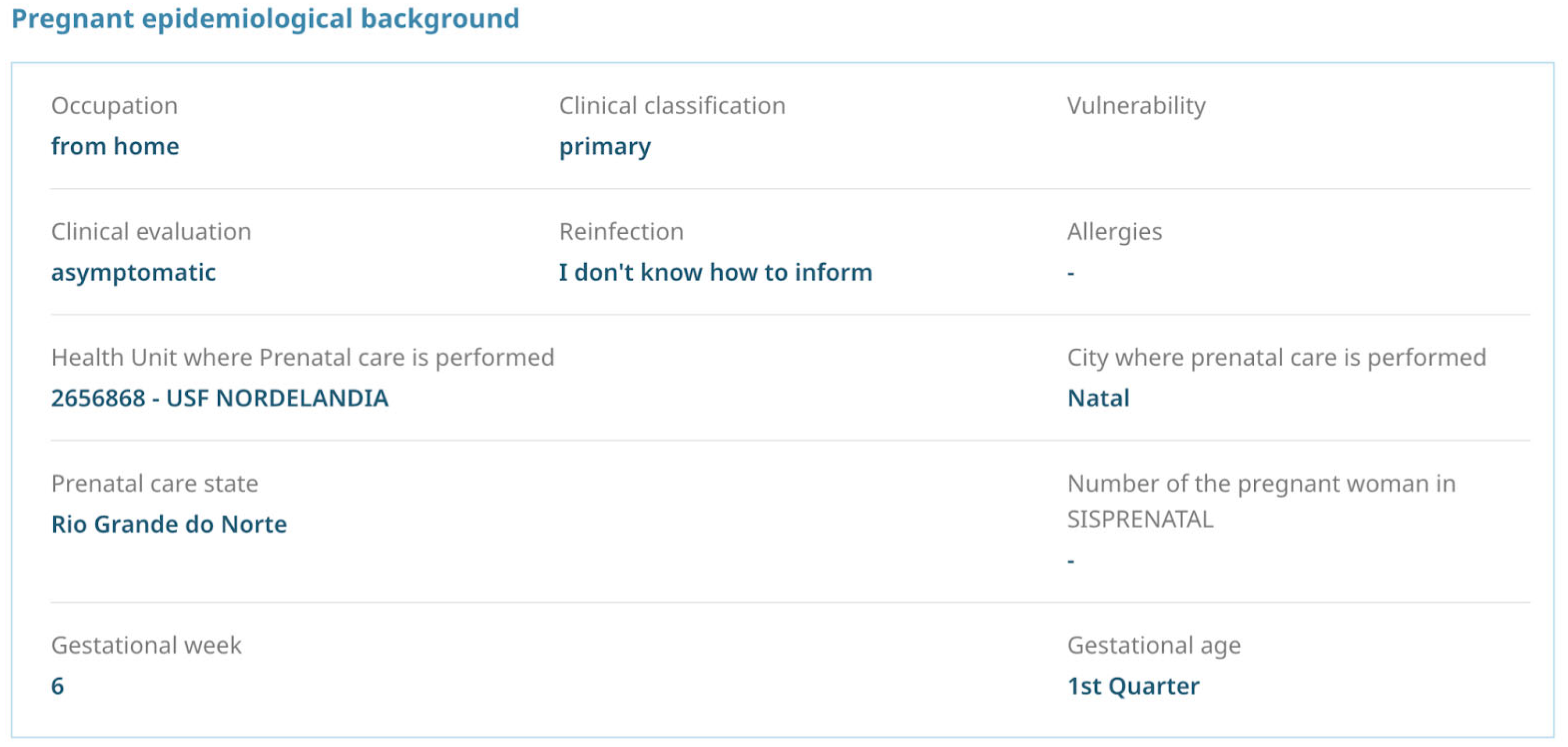
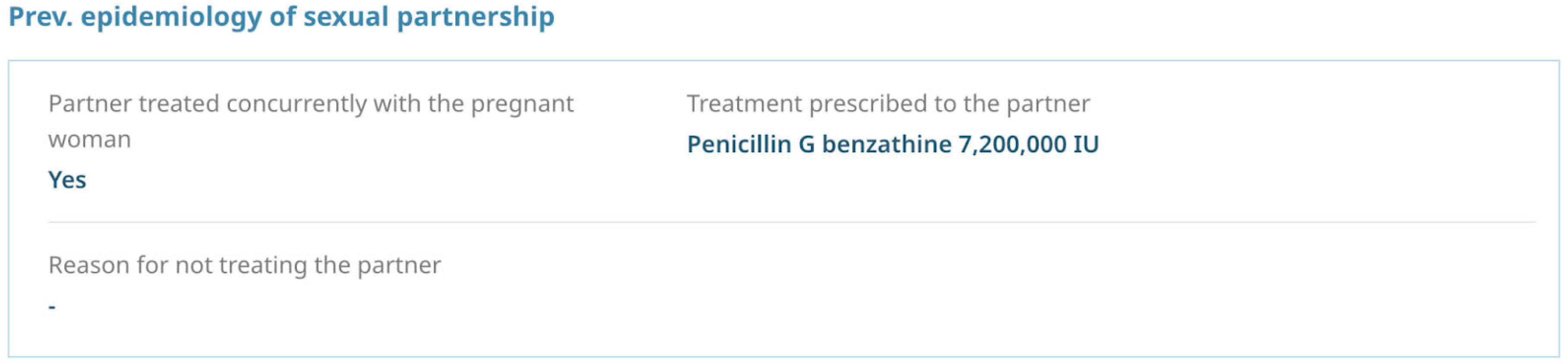
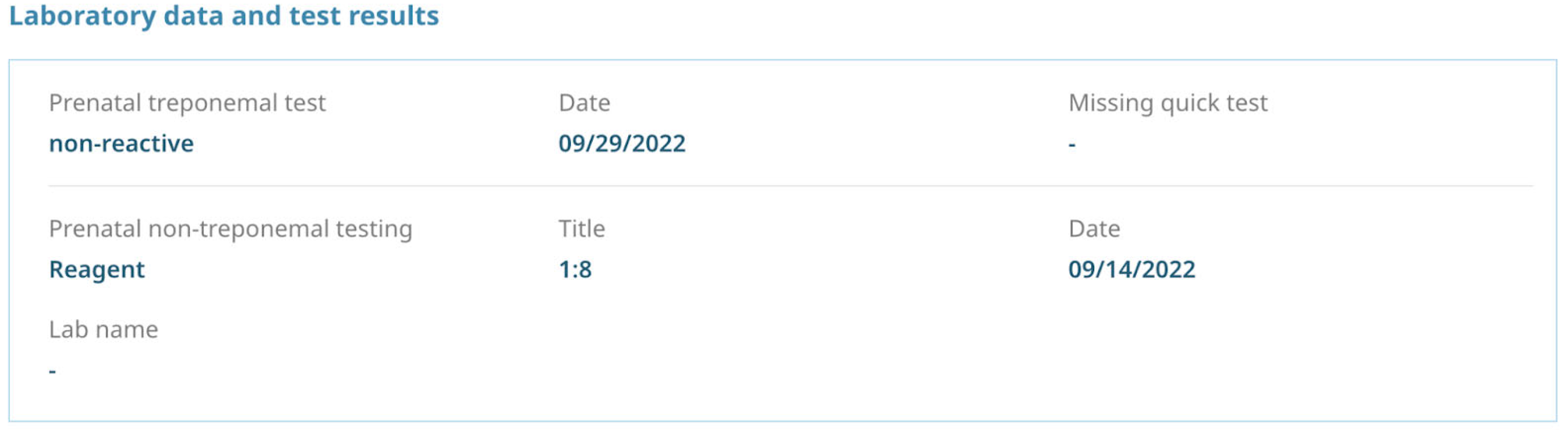
Appendix A. Important Screens of the Salus Platform
Appendix B. Salus Functionalities
References
- Amorim, E.K.R.; Matozinhos, F.P.; Araújo, L.A.; Silva, T.P.R.D. Trend in cases of gestational and congenital syphilis in Minas Gerais, Brazil, 2009–2019: An ecological study. Epidemiol. E Serviços Saúde 2021, 30. [Google Scholar] [CrossRef]
- Secretariat of Health Surveillance, Ministry of Health. Syphilis 2020. Special Epidemiological Bulletin 2020; Department of Diseases of Chronic Conditions and Sexually Transmitted Infections. Available online: https://www.gov.br/aids/pt-br/centrais-de-conteudo/boletins-epidemiologicos/2020/sifilis/boletim_sifilis_2020.pdf/view (accessed on 3 June 2022).
- De Brito Pinto, T.K.; da Cunha-Oliveira, A.C.G.D.P.; Sales-Moioli, A.I.L.; Dantas, J.F.; da Costa, R.M.M.; Silva Moura, J.P.; Gómez-Cantarino, S.; Valentim, R.A.M. Clinical Protocols and Treatment Guidelines for the Management of Maternal and Congenital Syphilis in Brazil and Portugal: Analysis and Comparisons: A Narrative Review. Int. J. Environ. Res. Public Health 2022, 19, 10513. [Google Scholar] [CrossRef] [PubMed]
- Kleber, G.; Alves, D.; de Paiva, J.; Diógenes, D.; Valentim, R.; Medeiros, A. SOS Syphilis: Smartphone application for the mapping of syphilis attention networks. Procedia Comput. Sci. 2021, 181, 434–441. [Google Scholar] [CrossRef]
- Clement, M.E.; Okeke, N.L.; Hicks, C.B. Treatment of syphilis: A systematic review. Jama 2014, 312, 1905–1917. [Google Scholar] [CrossRef]
- Liang, Z.; Chen, Y.P.; Yang, C.S.; Guo, W.; Jiang, X.X.; Xu, X.F.; Jiang, G. Meta-analysis of ceftriaxone compared with penicillin for the treatment of syphilis. Int. J. Antimicrob. Agents 2016, 47, 6–11. [Google Scholar] [CrossRef]
- World Health Organization. WHO Guidelines for the Treatment of Treponema pallidum (Syphilis)—2016. Available online: https://apps.who.int/iris/bitstream/handle/10665/249572/9789241549806-eng.pdf (accessed on 3 June 2022).
- Brazil. Ministry of Health. Secretary of Health Surveillance. General Coordination for the Development of Epidemiology in Services. Health Surveillance Guide: Volume 2/Ministry of Health, Health Surveillance Secretariat, General Coordination for the Development of Epidemiology in Services—1st ed. 2017. Available online: https://bvsms.saude.gov.br/bvs/publicacoes/guia_vigilancia_saude_volume_2.pdf (accessed on 6 May 2022).
- Saes, M.D.O.; Duro, S.M.S.; Gonçalves, C.D.S.; Tomasi, E.; Facchini, L.A. Assessment of the appropriate management of syphilis patients in primary health care in different regions of Brazil from 2012 to 2018. Cad. De Saúde Pública 2022, 38, EN231921. [Google Scholar] [CrossRef]
- Ghanem, K.G.; Ram, S.; Rice, P.A. The modern epidemic of syphilis. N. Engl. J. Med. 2020, 382, 845–854. [Google Scholar] [CrossRef]
- World Health Organization. WHO Model List of Essential Medicines: 20th List; World Health Organization: Geneva, Switzerland, 2017; Available online: http://www.who.int/medicines/publications/essentialmedicines/20th_EML2017_FINAL_amendedAug2017.pdf?ua=1 (accessed on 4 July 2022).
- World Health Organization. Global Progress Report on HIV, Viral Hepatitis and Sexually Transmitted Infections, 2021. Accountability for the Global Health Sector Strategies 2016–2021: Actions for Impact. Available online: https://www.who.int/publications/i/item/9789240027077 (accessed on 4 July 2022).
- De Andrade, I.G.M.; de Medeiros Valentim, R.A.; de Oliveira, C.A.P. The influence of the no syphilis project on congenital syphilis admissions between 2018 and 2019. Braz. J. Sex. Transm. Dis. 2020, 32, e3205. [Google Scholar]
- Valentim, R.A.; Caldeira-Silva, G.J.; da Silva, R.D.; Albuquerque, G.A.; de Andrade, I.G.; Sales-Moioli, A.I.L.; Rodrigues, A.G.C. Stochastic Petri net model describing the relationship between reported maternal and congenital syphilis cases in Brazil. BMC Med. Inform. Decis. Mak. 2022, 22, 40. [Google Scholar]
- Daniel, V.M. Health Information Systems and Their Support for SUS Management and Planning: An Analysis of Brazilian States. Master’s Thesis, Pontifical Catholic University of Rio Grande do Sul, Porto Alegre, Brazil, 2013. [Google Scholar]
- Laguardia, J.; Domingues, C.M.A.; Carvalho, C.; Lauerman, C.R.; Macário, E.; Glatt, R. Information system for notifiable health problems (SINAN): Challenges in developing a health information system. Epidemiol. Health Serv. 2004, 13, 135–146. [Google Scholar]
- De Araújo, Y.B.; Rezende, L.C.M.; de Queiroga, M.M.D.; dos Santos, S.R. Health Information Systems: Information inconsistencies in the context of Primary Care. J. Health Inform. 2016, 8, 164–170. [Google Scholar]
- Coelho Neto, G.C.; Chioro, A. After all, how many nationally based Health Information Systems exist in Brazil? Public Health Noteb. 2021, 37, e00182119. [Google Scholar]
- Brazil. Ministry of Health. Secretary of Health Care. Regulation, Evaluation and Control Department. Health Care Information Systems: Historical Contexts, Advances and Perspectives in the SUS/Pan American Health Organization—Brasília. Health Care Information Systems: From Fragmentation to Interoperability. 2015. Available online: http://www.escoladesaude.pr.gov.br/arquivos/File/sistemas_informacao_atencao_saude_contextos_historicos.pdf (accessed on 4 July 2022).
- World Health Organization. Monitoring the Building Blocks of Health Systems: A Handbook of Indicators and Their Measurement Strategies; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Moraes, I.H.S.D.; Gómez, M.N.G.D. Information and informatics in health: Contemporary kaleidoscope of health. Sci. Collect. Health 2007, 12, 553–565. [Google Scholar]
- Morais, A.H.F.; Barros, D.M.S.; Valentim, R.A.M.; Balen, S.A.; Oliveira, C.A.P.; Andrade, I.G.M.; Lacerda, J.S.; Lima, L.J.G.; Silva, G.J.P.C.; Moioli, A.I.L.S.; et al. Inconsistencies in Reports of Congenital Syphilis: An Analysis Based on SINAN, Confirmed by Clinical, Laboratory and Epidemiological Findings—Version 2. Technical Report: 2022. Available online: https://repositorio.lais.huol.ufrn.br/media/documents/Relat%C3%B3rio-S%C3%ADfilis_-Inconsist%C3%AAncias-do-SINAN-e-do-Diagn%C3%B3stico-de-S%C3%ADfilis-Cong%C3%AAnita-V2.pdf (accessed on 6 May 2022).
- Fernandes, Y.Y.M.P.; Araújo, G.T.D.; Araújo, B.G.D.; Dantas, M.D.C.R.; Carvalho, D.R.D.; Valentim, R.A.D.M. ILITIA: Telehealth architecture for high-risk gestation classification. Res. Biomed. Eng. 2017, 33, 237–246. [Google Scholar] [CrossRef] [Green Version]
- Saraceni, V.; Vellozo, V.; Leal, M.D.C.; Hartz, Z.M.D.A. SINAN reliability study based on the Campaigns for the Elimination of Congenital Syphilis in the Municipality of Rio de Janeiro. Braz. J. Epidemiol. 2005, 8, 419–424. [Google Scholar]
- Brazil. Ministry of Health, Secretary of Health Care. Syphilis Epidemiological Bulletin—2016. Available online: https://www.gov.br/aids/pt-br/pub/2016/boletim-epidemiologico-de-sifilis-2016 (accessed on 10 August 2022).
- De Morais, C.M.; Teixeira, I.V.; Sadok, S.; Endo, P.T.; Kelner, J. Syphilis Trigram: A domain-specific visualization to combat syphilis epidemic and improve the quality of maternal and child health in Brazil. BMC Pregnancy Childbirth 2022, 22, 379. [Google Scholar] [CrossRef]
- Ministry of Health. Ordinance 204, of 17 February 2016. Defines the National List of Compulsory Notification of Diseases, Injuries and Public Health Events in Public and Private Health Services throughout the National Territory, according to the Annex, and Makes other Provisions. SINAN Reliability Study Based on the Campaigns for the Elimination of Congenital Syphilis in the Municipality of Rio de Janeiro. 2016. Available online: http://bvsms.saude.gov.br/bvs/saudelegis/gm/2016/prt0204_17_02_2016.html (accessed on 10 August 2022).
- Garbin, A.J.Í.; Martins, R.J.; Belila, N.D.M.; Exaltação, S.M.; Garbin, C.A.S. Reemerging diseases in Brazil: Sociodemographic and epidemiological characteristics of syphilis and its under-reporting. J. Braz. Soc. Trop. Med. 2019, 52. [Google Scholar] [CrossRef]
- Valentim, R.A.D.M.; Lima, T.S.; Cortez, L.R.; Barros, D.M.D.S.; Silva, R.D.D.; Paiva, J.C.D.; André, F.R.D. The relevance of a technological ecosystem in the face of COVID-19 in the Unified Health System: The case of Rio Grande Do Norte, Brazil. Sci. Collect. Health 2021, 26, 2035–2052. [Google Scholar]
- Brazil. Ministry of Health. Secretary of Health Surveillance. National IST/AIDS Program. Guidelines for Controlling Congenital Syphilis: Pocket Manual/Ministry of Health, Health Surveillance Secretariat, National IST/AIDS Program—2nd ed. 2006. Available online: https://bvsms.saude.gov.br/bvs/publicacoes/manual_sifilis_bolso.pdf (accessed on 9 November 2022).
- Department of Diseases, Chronic Conditions and Sexually Transmitted Infections, Secretariat of Health Surveillance, Ministry of Health. Strategic Agenda for Reducing Syphilis in Brazil, 2020–2021. Available online: http://bvsms.saude.gov.br/bvs/publicacoes/agenda_reducao_sifilis_2020_2021.pdf (accessed on 4 April 2022).
- Ramos, A.N., Jr. Persistence of syphilis as a challenge for the Brazilian public health: The solution is to strengthen SUS in defense of democracy and life. Cad. De Saúde Pública 2022, 38. [Google Scholar] [CrossRef]
- Barros, G.M.C.; Carvalho, D.D.A.; Cruz, A.S.; Morais, E.K.L.; Sales-Moioli, A.I.L.; Pinto, T.K.B.; Almeida, M.C.D.; Sanchez-Gendriz, I.; Fernandes, F.; Barbalho, I.M.P.; et al. Development of a method based on cyclic voltammetry for detecting antigens and antibodies as a new strategy for diagnosing syphilis. Int. J. Environ. Res. Public Health 2022, 19, 16206. [Google Scholar] [CrossRef]
- De Morais Pinto, R.; de Medeiros Valentim, R.A.; Fernandes da Silva, L.; Lima, G.F.D.M.S.; Kumar, V.; Pereira de Oliveira, C.A.; de Andrade, I. Analyzing the reach of public health campaigns based on multidimensional aspects: The case of the syphilis epidemic in Brazil. BMC Public Health 2021, 21, 1632. [Google Scholar] [CrossRef]
- Morais, P.S.G.D. Salus: A digital health architecture applied to syphilis case management. Front. Public Health 2022, 10, 1002245. [Google Scholar]
- Secretariat of Health Surveillance Ministry of Health, 2022. Ministry of Health. National List of Compulsory Notification of Diseases, Injuries and Public Health Events. Available online: https://www.gov.br/saude/pt-br/composicao/svsa/notificacao-compulsoria/lista-nacional-de-notificacao-compulsoria-de-doencas-agravos-e-eventos-de-saude-publica (accessed on 12 August 2022).
- Daniel, V.M.; Pereira, G.V.; Macadar, M.A. An institutional perspective of health information systems in two Brazilian states/Perspectiva institucional dos sistemas de informacao em saude em dois estados brasileiros. RAC-Rev. De Adm. Contemp. 2014, 18, 650–670. [Google Scholar] [CrossRef]
- Marques dos Santos, M.; Lopes, A.K.B.; Roncalli, A.G.; Lima, K.C.D. Trends of syphilis in Brazil: A growth portrait of the treponemic epidemic. PLoS ONE 2020, 15, e0231029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lima, A.C.; Januário, M.C.; Lima, P.T.; de Moura, W. DATASUS: The use of Information Systems in Public Health. Refas- Fatec Zona Sul Mag. 2015, 1, 16–31. [Google Scholar]
- Benedetti, K.C.S.V.; da Costa Ribeiro, A.D.; de Sá Queiroz, J.H.F.; Melo, A.B.D.; Batista, R.B.; Delgado, F.M.; Simionatto, S. High prevalence of syphilis and inadequate prenatal care in Brazilian pregnant women: A cross-sectional study. Am. J. Trop. Med. Hyg. 2019, 101, 761. [Google Scholar] [CrossRef]
- Coelho Neto, G.C.; Andreazza, R.; Chioro, A. Integration among national health information systems in Brazil: The case of e-SUS Primary Care. Rev. De Saúde Pública 2021, 55. [Google Scholar] [CrossRef]
- Brazil. Ministry of Health. Secretary of Health Surveillance. National STD and AIDS Program. Protocol for Preventing mother-to-Child Transmission of HIV and Syphilis: Pocket Manual/Ministry of Health, Health Surveillance Secretariat, National STD and AIDS Program—Brasilia: Ministry of Health, 2007. Available online: https://bvsms.saude.gov.br/bvs/publicacoes/.pdf (accessed on 11 March 2022).
- Donisi, A.; Colpani, A.; Zauli, B.; De Vito, A.; Fiore, V.; Babudieri, S.; Madeddu, G. Sexually Transmitted Infections Prevalence and Cascade of Care among Undocumented Sex Workers: A Twenty-Year-Long Experience. Life 2023, 13, 606. [Google Scholar] [CrossRef]
- Santos, E.J.L. Evaluation of Sinan for Cases of Syphilis in Pregnant Women in Amambaí—MS from 2007 to 2010. Available online: https://www.arca.fiocruz.br/handle/icict/23393 (accessed on 7 June 2022).
- Hammann, E.M.; Laguardia, J. Reflections on epidemiological surveillance: Beyond compulsory notification. Inf. Epidemiológico Do Sus 2000, 9, 211–219. [Google Scholar]
- Valentim, J.L.; Dias-Trindade, S.; Oliveira, E.S.; Moreira, J.A.; Fernandes, F.; Romão, M.H.; Valentim, R.A. The relevancy of massive health education in the Brazilian prison system: The course” health care for people deprived of freedom” and its impacts. Front. Public Health 2022, 10, 2731. [Google Scholar] [CrossRef]
- Domingues, R.M.S.M.; Leal, M.D.C.; Pereira, A.P.E.; Ayres, B.; Sánchez, A.R.; Larouzé, B. Prevalence of syphilis and HIV infection during pregnancy in incarcerated women and the incidence of congenital syphilis in births in prison in Brazil. Cad. De Saúde Pública 2017, 33, e00183616. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Other Systems | Functionalities | System Salus Syphilis | Comparative Analysis |
|---|---|---|---|
| AMAQ—Self-Assessment to Improve Access and Quality of Primary Care—Evaluation of the primary health care work process | Evaluation of the primary health care work process | Indicators panel; Case Panel; Management Reports; Management of notifications launched on SINAN; Alerts and Notifications Center. | Fully meets |
| CADSUS—SUS User Registration System | Register of SUS users | Case Management; Active Search; Indicators panel; Case Panel; Management Reports. | Fully meets |
| CNES—National Register of Health Establishments—Register of health establishments | Register of health establishments | Link Management | Fully meets |
| e-SUS AB/SISAB—Health Information System for Primary Care—Support for care management and control and monitoring of activities and procedures performed in primary health care | Support for care management and control and monitoring of activities and procedures performed in primary health care | Indicators panel; Case Panel; Management Reports; Management of notifications launched on SINAN; Alerts and Notifications Center; Case Management; Active Search. | Fully meets |
| GAL—Laboratory Environment Management System—Control and monitoring of laboratory results of diseases and conditions of public health interest; supports the management of state public health laboratories. | Control and monitor laboratory results of diseases and conditions of public health interest; supports the management of state public health laboratories. | Alerts and Notifications Center; Case Management. | Fully meets |
| PMAQ-AB—National Program for Improving Access and Quality of Primary Care—Control, monitoring, and evaluation of APS programmatic actions and work processes | Control, monitor, and evaluation of APS programmatic actions and work processes | Indicators panel; Case Panel; Management Reports; Management of notifications launched on SINAN; Alerts and Notifications Center; Case Management; Active Search; Register User; Link Management; Interactive Map with Georeferencing of Cases (GEOSalus); Citizen Transparency. | Fully meets |
| SARGSUS—Support System for the Preparation of the Management Report—Support to municipal management for the preparation and submission of the Annual Management Report (RAG) to the Health Council | Support to municipal management for the preparation and submission of the Annual Management Report (RAG) to the Health Council | Indicators panel; Case Panel; Management Reports; Management of notifications launched on SINAN; Alerts and Notifications Center; Interactive Map with Georeferencing of Cases (GEOSalus); Citizen Transparency. | Fully meets |
| SIA—Outpatient Information System—Control and monitoring of the performance of outpatient procedures | Control and monitoring of the performance of outpatient procedures | Case Management; Active Search; Indicators panel; Case Panel; Management Reports; Interactive Map with Georeferencing of Cases (GEOSalus). | Fully meets |
| SIAB—Primary Care Information System—Control and monitoring of activities and procedures performed in Primary Health Care | Control and monitoring of activities and procedures performed in Primary Health Care | Case Management; Active Search; Indicators panel; Case Panel; Management Reports; Interactive Map with Georeferencing of Cases (GEOSalus). | Fully meets |
| SIASI—Indigenous Health Information System—Control and monitoring of demographic information and health care for indigenous peoples | Control and monitoring of demographic information and health care for indigenous peoples | Case Management; Active Search; Indicators panel; Case Panel; Management Reports; Interactive Map with Georeferencing of Cases (GEOSalus). | Fully meets |
| SIS PRÉ-NATAL—Information System for Monitoring and Evaluation of Prenatal, Childbirth, Puerperium and Children—Control and monitoring of health care for pregnant women, postpartum women, and newborns | Control and monitoring of health care for pregnant women, postpartum women, and newborns | Case Management; Active Search; Indicators panel; Case Panel; Management Reports; Interactive Map with Georeferencing of Cases (GEOSalus). | Fully meets |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brito, T.; Lima, T.; Cunha-Oliveira, A.; Noronha, A.; Brito, C.; Farias, F.; Morais, S.; Paiva, J.; Honorato, C.; Queirós, P.; et al. Salus Platform: A Digital Health Solution Tool for Managing Syphilis Cases in Brazil—A Comparative Analysis. Int. J. Environ. Res. Public Health 2023, 20, 5258. https://doi.org/10.3390/ijerph20075258
Brito T, Lima T, Cunha-Oliveira A, Noronha A, Brito C, Farias F, Morais S, Paiva J, Honorato C, Queirós P, et al. Salus Platform: A Digital Health Solution Tool for Managing Syphilis Cases in Brazil—A Comparative Analysis. International Journal of Environmental Research and Public Health. 2023; 20(7):5258. https://doi.org/10.3390/ijerph20075258
Chicago/Turabian StyleBrito, Talita, Thaísa Lima, Aliete Cunha-Oliveira, André Noronha, Cintia Brito, Fernando Farias, Sedir Morais, Jailton Paiva, Cintia Honorato, Paulo Queirós, and et al. 2023. "Salus Platform: A Digital Health Solution Tool for Managing Syphilis Cases in Brazil—A Comparative Analysis" International Journal of Environmental Research and Public Health 20, no. 7: 5258. https://doi.org/10.3390/ijerph20075258
APA StyleBrito, T., Lima, T., Cunha-Oliveira, A., Noronha, A., Brito, C., Farias, F., Morais, S., Paiva, J., Honorato, C., Queirós, P., Gómez-Cantarino, S., Lucena, M., & Valentim, R. (2023). Salus Platform: A Digital Health Solution Tool for Managing Syphilis Cases in Brazil—A Comparative Analysis. International Journal of Environmental Research and Public Health, 20(7), 5258. https://doi.org/10.3390/ijerph20075258