
Pain and Motor Function in Myotonic Dystrophy Type 1: A Cross-Sectional Study


 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Outcomes
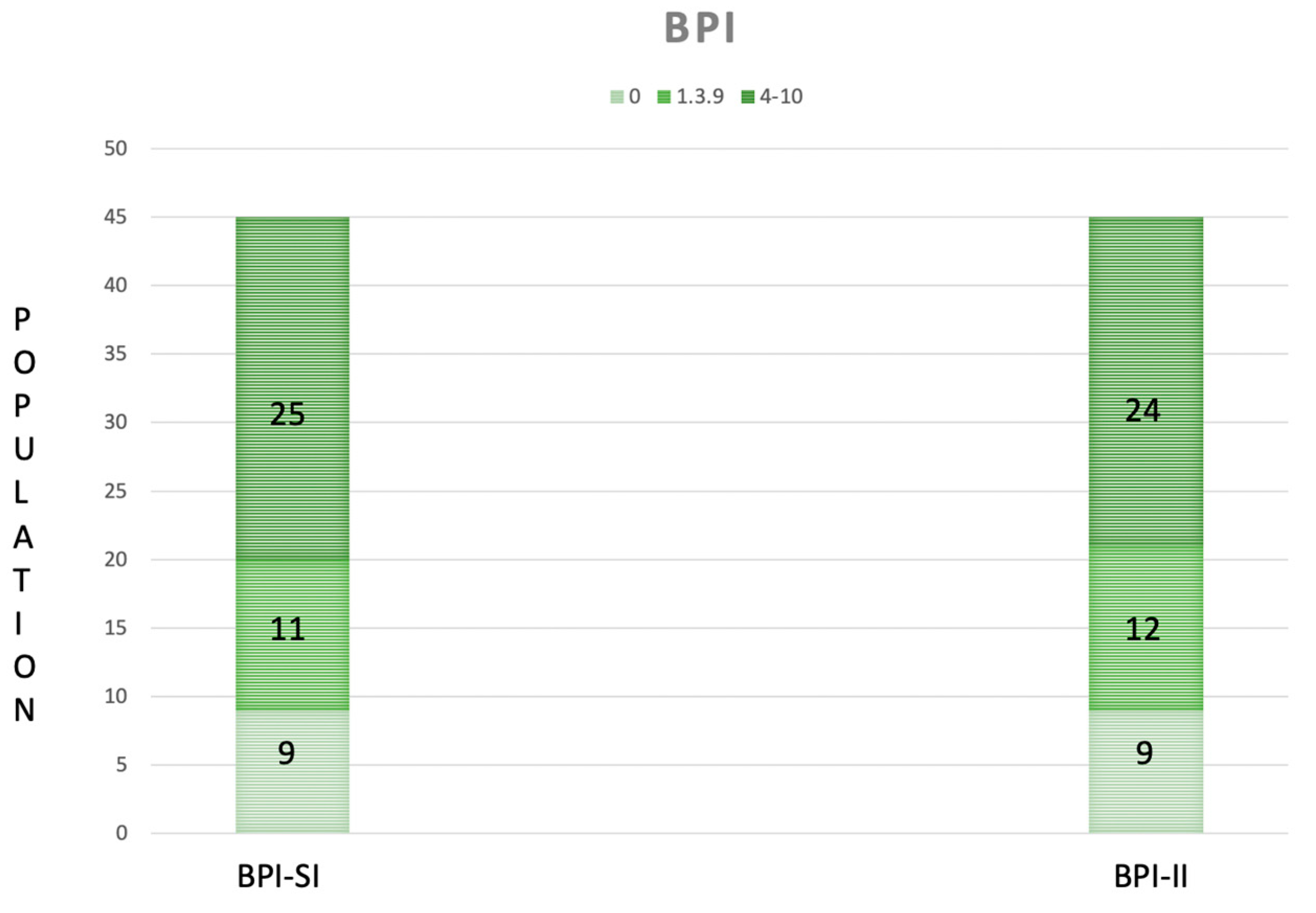
2.2.1. The Brief Pain Inventory (BPI)
2.2.2. The Tinetti Performance-Oriented Mobility Assessment (POMA)
2.2.3. The Functional Independence Measure (FIM)
2.2.4. The Fatigue Severity Scale (FSS)
2.3. Statistical Analysis
3. Results
- -
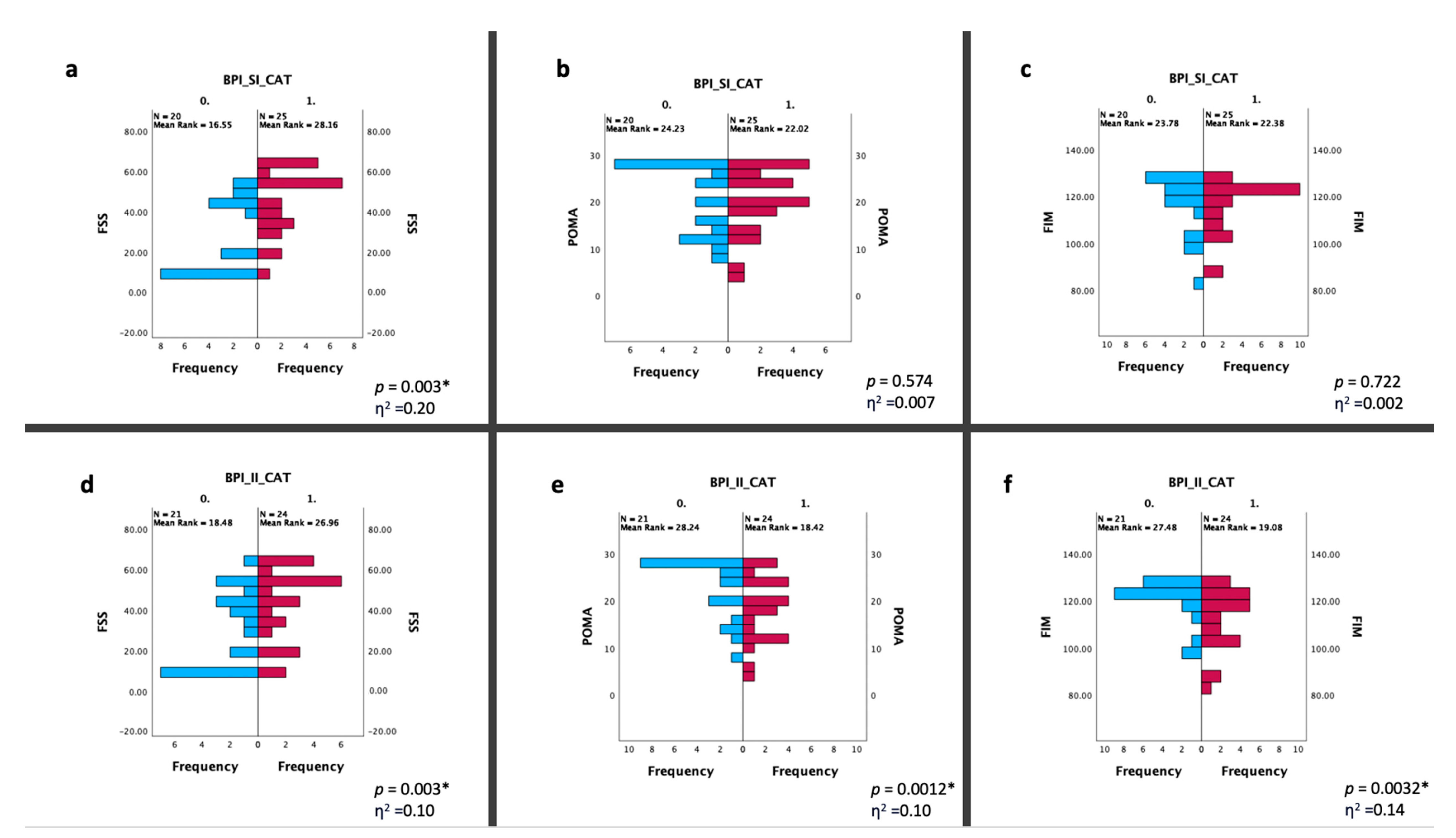
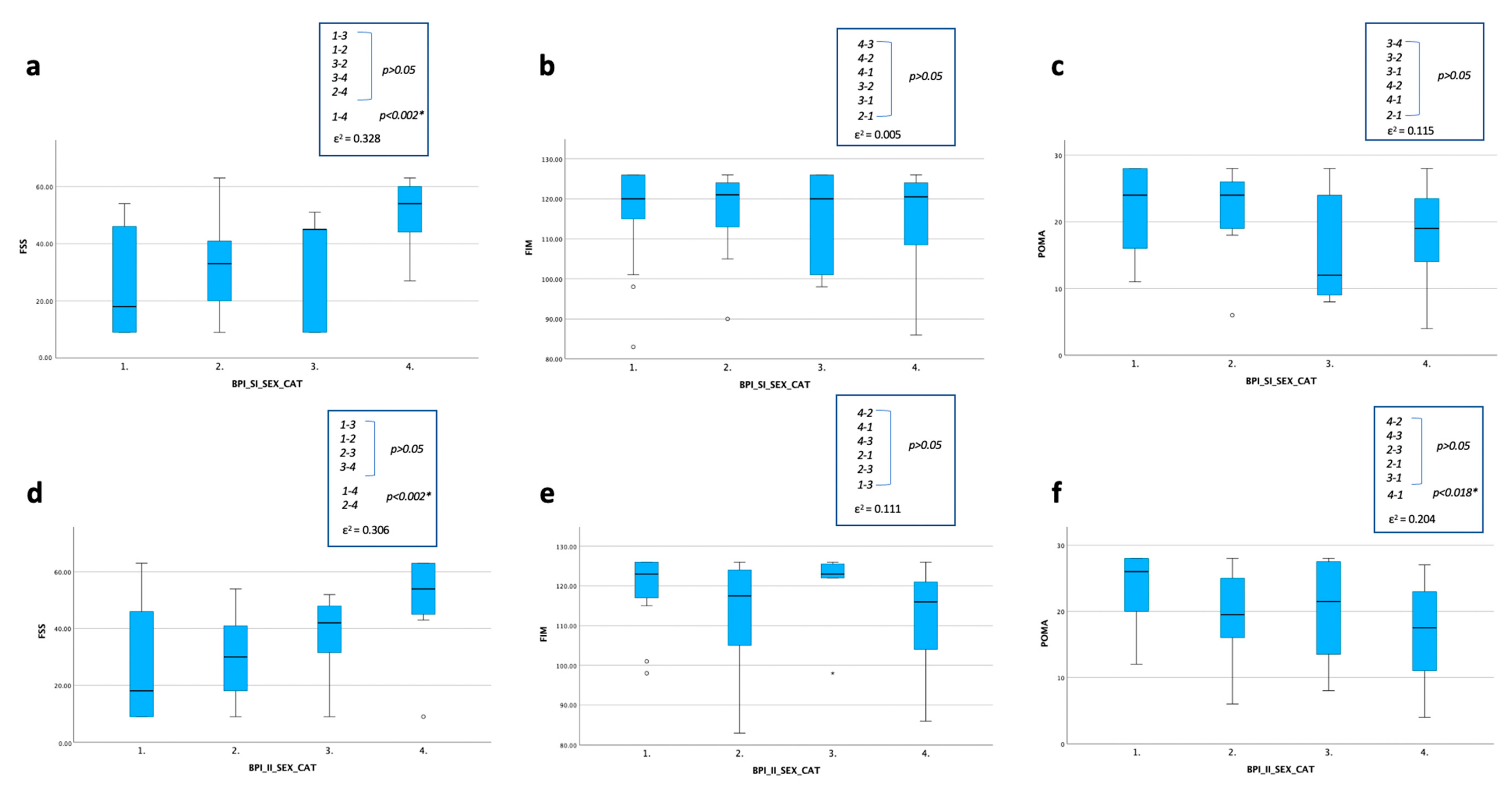
- For the BPI-SI (Figure 5a–c), a statistically significant difference was found for the FSS with a lower score in male group with less severe pain compared to the female group with more severe pain (p < 0.002);
- -
- For the BPI-II (Figure 5d–f), a statistically significant difference was found for the FSS between the two groups with BPI-II ≥ 4 (with worsen score in the female one) (p < 0.002) and for the FSS and the POMA, with a lower score in the male group with the BPI-II ≤ 4 compared to the female group with BPI-II ≥ 4 (p < 0.002).
4. Discussion
4.1. A Multidimensional Assessment of Pain for People with DM1
4.2. Pain and Fatigue in People with DM1
4.3. Pain and Gait/Balance in People with DM1
4.4. Pain and Functional Abilities in People with DM1
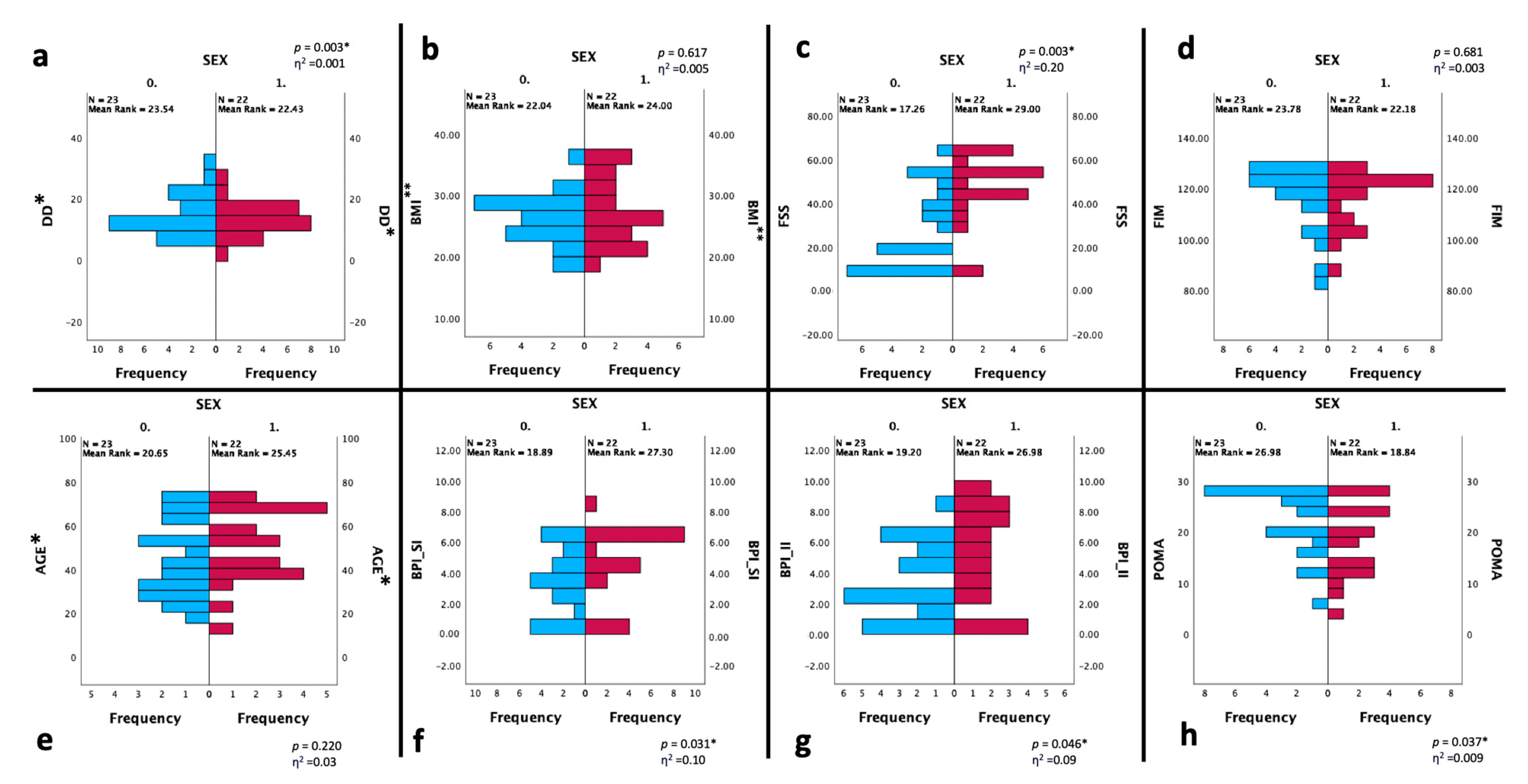
4.5. Pain, Functional Outcomes and Gender in People with DM1
4.6. Limitations of Our Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hahn, C.; Salajegheh, M.K. Myotonic disorders: A review article. Iran. J. Neurol. 2016, 5, 46–53. [Google Scholar]
- Suominen, T.; Bachinski, L.L.; Auvinen, S.; Hackman, P.; Baggerly, K.A.; Angelini, C.; Peltonen, L.; Krahe, R.; Udd, B. Population frequency of myotonic dystrophy: Higher than expected frequency of myotonic dystrophy type 2 (DM2) mutation in Finland. Eur. J. Hum. Genet. 2011, 19, 776–782. [Google Scholar] [CrossRef] [PubMed]
- Pratte, A.; Prévost, C.; Puymirat, J.; Mathieu, J. Anticipation in myotonic dystrophy type 1 parents with small CTG expansions. Am. J. Med. Genet. A 2015, 167, 708–714. [Google Scholar] [CrossRef]
- Thornton, C.A. Myotonic dystrophy. Neurol. Clin. 2014, 32, 705–719. [Google Scholar] [CrossRef]
- Zaki, M.; Boyd, P.A.; Impey, L.; Roberts, A.; Chamberlain, P. Congenital myotonic dystrophy: Prenatal ultrasound findings and pregnancy outcome. Ultrasound Obstet. Gynecol. 2007, 29, 284–288. [Google Scholar] [CrossRef] [PubMed]
- Turner, C.; Hilton-Jones, D. The myotonic dystrophies: Diagnosis and management. J. Neurol. Neurosurg. Psychiatry 2010, 81, 358–367. [Google Scholar] [CrossRef] [PubMed]
- Angeard, N.; Jacquette, A.; Gargiulo, M.; Radvanyi, H.; Moutier, S.; Eymard, B.; Héron, D. A new window on neurocognitive dysfunction in the childhood form of myotonic dystrophy type 1 (DM1). Neuromuscul. Disord. 2011, 21, 468–476. [Google Scholar] [CrossRef]
- Wenninger, S.; Montagnese, F.; Schoser, B. Core Clinical Phenotypes in Myotonic Dystrophies. Front. Neurol. 2018, 9, 303. [Google Scholar] [CrossRef]
- Miró, J.; Gertz, K.J.; Carter, G.T.; Jensen, M.P. Pain location and intensity impacts function in persons with myotonic dystrophy type 1 and facioscapulohumeral dystrophy with chronic pain. Muscle Nerve 2014, 49, 900–905. [Google Scholar] [CrossRef]
- Peric, M.; Peric, S.; Rapajic, N.; Dobricic, V.; Savic-Pavicevic, D.; Nesic, I.; Radojicic, S.; Novakovic, I.; Lavrnic, D.; Rakocevic-Stojanovic, V. Multidimensional aspects of pain in myotonic dystrophies. Acta Myol. 2015, 34, 126–132. [Google Scholar]
- Jensen, M.P.; Hoffman, A.J.; Stoelb, B.L.; Abresch, R.T.; Carter, G.T.; McDonald, C.M. Chronic pain in persons with myotonic dystrophy and facioscapulohumeral dystrophy. Arch. Phys. Med. Rehabil. 2008, 89, 320–328. [Google Scholar] [CrossRef] [PubMed]
- Solbakken, G.; Løseth, S.; Froholdt, A.; Eikeland, T.D.; Nærland, T.; Frich, J.C.; Dietrichs, E.; Ørstavik, K. Pain in adult myotonic dystrophy type 1: Relation to function and gender. BMC Neurol. 2021, 4, 101–110. [Google Scholar] [CrossRef] [PubMed]
- Krivickas, L.S. Electrodiagnosis in neuromuscular disease. Phys. Med. Rehabil. Clin. N. Am. 1998, 9, 83–114. [Google Scholar] [CrossRef] [PubMed]
- Solbakken, G.; Bjørnarå, B.; Kirkhus, E.; Nguyen, B.; Hansen, G.; Frich, J.C.; Ørstavik, K. MRI of trunk muscles and motor and respiratory function in patients with myotonic dystrophy type 1. BMC Neurol. 2019, 19, 135. [Google Scholar] [CrossRef]
- Park, D.; Park, J.S. Quantitative Assessment of Trunk Muscles Involvement in Patients with Myotonic Dystrophy Type 1 Using a Whole Body Muscle Magnetic Resonance Imaging. Eur. Neurol. 2017, 77, 238–245. [Google Scholar] [CrossRef]
- Peric, S.; Stojanovic, V.R.; Nikolic, A.; Kacar, A.; Basta, I.; Pavlovic, S.; Lavrnic, D. Peripheral neuropathy in patients with myotonic dystrophy type 1. Neurol. Res. 2013, 35, 331–335. [Google Scholar] [CrossRef]
- Katz, N. The impact of pain management on quality of life. J. Pain Symptom Manag. 2002, 1, 38–47. [Google Scholar] [CrossRef]
- Harper, P.S.; van Engelen, B.G.; Eymard, B.; Rogers, M.; Wilcox, D. 99th ENMC international workshop: Myotonic dystrophy: Present management, future therapy. 9–11 November 2001, Naarden, The Netherlands. Neuromuscul. Disord. 2002, 12, 596–599. [Google Scholar] [CrossRef]
- Caraceni, A.; Mendoza, T.R.; Mencaglia, E.; Baratella, C.; Edwards, K.; Forjaz, M.J.; Martini, C.; Serlin, R.C.; de Conno, F.; Cleeland, C.S. A validation study of an Italian version of the Brief Pain Inventory (Breve Questionario per la Valutazione del Dolore). Pain 1996, 65, 87–92. [Google Scholar] [CrossRef]
- Deandrea, S.; Montanari, M.; Moja, L.; Apolone, G. Prevalence of undertreatment in cancer pain. A review of published literature. Ann. Oncol. 2008, 19, 1985–1991. [Google Scholar] [CrossRef]
- Cleeland, C.S.; Ryan, K.M. Pain assessment: Global use of the Brief Pain Inventory. Ann. Acad. Med. 1994, 23, 129–138. [Google Scholar]
- Ventafridda, V.; Saita, L.; Ripamonti, C.; De Conno, F. WHO guidelines for the use of analgesics in cancer pain. Int. J. Tissue React. 1985, 7, 93–96. [Google Scholar] [PubMed]
- Tinetti, M.E.; Williams, T.F.; Mayewski, R. Fall risk index for elderly patients based on number of chronic disabilities. Am. J. Med. 1986, 80, 429–434. [Google Scholar] [CrossRef] [PubMed]
- Huang, M.E.; Wartella, J.E.; Kreutzer, J.S. Functional outcomes and quality of life in patients with brain tumors: A preliminary report. Arch. Phys. Med. Rehabil. 2001, 82, 1540–1546. [Google Scholar] [CrossRef] [PubMed]
- Goodwin, E.; Hawton, A.; Green, C. Using the Fatigue Severity Scale to inform healthcare decision-making in multiple sclerosis: Mapping to three quality-adjusted life-year measures (EQ-5D-3L, SF-6D, MSIS-8D). Health Qual. Life Outcomes 2019, 5, 136. [Google Scholar] [CrossRef]
- Miles, J.; Shevlin, M. Applying Regression and Correlation: A Guide for Students and Researchers; Sage: London, UK, 2001. [Google Scholar]
- Rea, L.M.; Parker, R.A. Designing and Conducting Survey Research: A Comprehensive Guide; Jossey-Bass Publishers: San Francisco, CA, USA, 1992. [Google Scholar]
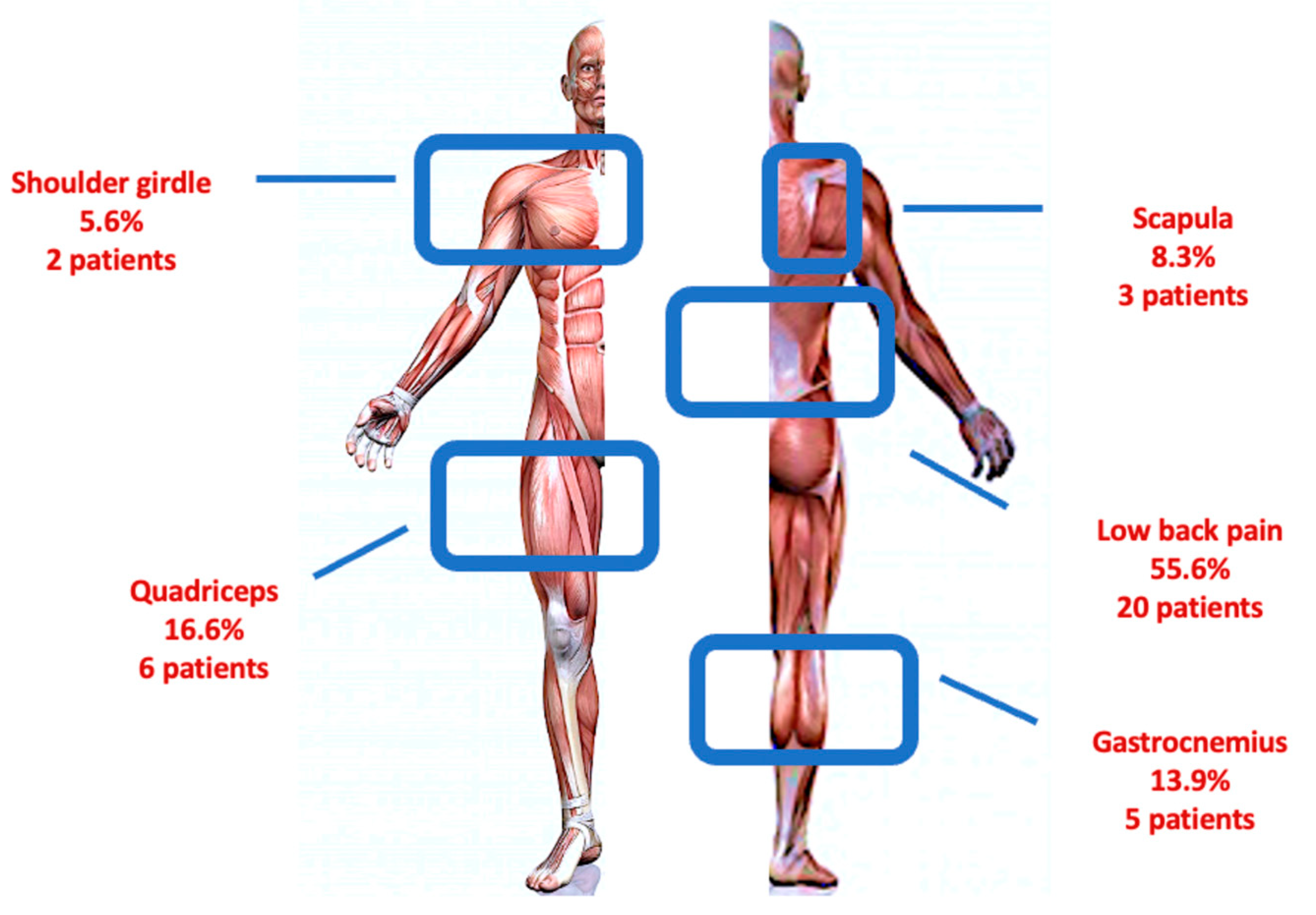
- Hoy, D.; Bain, C.; Williams, G.; March, L.; Brooks, P.; Blyth, F.; Woolf, A.; Vos, T.; Buchbinder, R. A systematic review of the global prevalence of low back pain. Arthritis Rheum. 2012, 64, 2028–2037. [Google Scholar] [CrossRef]
- Landfeldt, E.; Nikolenko, N.; Jimenez-Moreno, C.; Cumming, S.; Monckton, D.G.; Faber, C.G.; Merkies, I.S.J.; Gorman, G.; Turner, C.; Lochmüller, H. Activities of daily living in myotonic dystrophy type 1. Acta Neurol. Scand. 2020, 141, 380–387. [Google Scholar] [CrossRef]
- Tabry, V.; Vogel, T.A.; Lussier, M.; Brouillard, P.; Buhle, J.; Rainville, P.; Bherer, L.; Roy, M. Inter-individual predictors of pain inhibition during performance of a competing cognitive task. Sci. Rep. 2020, 11, 21785. [Google Scholar] [CrossRef]
- Dulai, J.S.; Smith, E.S.J.; Rahman, T. Acid-sensing ion channel 3: An analgesic target. Channels 2021, 15, 94–127. [Google Scholar] [CrossRef]
- Migliore, A.; Gigliucci, G.; Moretti, A.; Pietrella, A.; Peresson, M.; Atzeni, F.; Sarzi-Puttini, P.; Bazzichi, L.; Liguori, S.; Iolascon, G. Cross Cultural Adaptation and Validation of Italian Version of the Leeds Assessment of Neuropathic Symptoms and Signs Scale and Pain DETECT Questionnaire for the Distinction between Nociceptive and. Neuropathic Pain. Pain Res. Manag. 2021, 28, 6623651. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | DM1 Patients (N = 45) |
|---|---|
| Age (years) | 47.33 ± 17.15 |
| BMI (kg/m2) | 26.84 ± 4.84 |
| Gender Male (%) Female (%) | 23 (51.11%) 22 (49.89%) |
| DD (years) | 14.00 ± 5.85 |
| BPI-SI | 4.40 (0–8) |
| BPI-II | 4.20 (0–9) |
| POMA | 20 (4–28) |
| FIM | 121 (83–126) |
| FSS | 43 (9–63) |
| HYPOTHESIS (Regression Weights) | Beta Coefficient | t-Value | p-Value |
| DD- > BPI-SI | −0.093 | −1.533 | 0.134 |
| AGE- > BPI-SI | 0.040 | 2.018 | 0.051 |
| SEX- > BPI-SI | −0.515 | −0.638 | 0.527 |
| BMI- > BPI-SI | 0.157 | 2.295 | 0.028 * |
| FSS- > BPI-SI | 0.064 | 2.954 | 0.005 * |
| FIM- > BPI-SI | 0.051 | 1.229 | 0.227 |
| POMA- > BPI-SI | −0.032 | −0.492 | 0.626 |
| HYPOTHESIS (Regression Weights) | Beta Coefficient | t-Value | p-Value |
| DD- > BPI-II | −0.041 | −0.553 | 0.583 |
| AGE-> BPI-II | 0.044 | 1.815 | 0.078 |
| SEX-> BPI-II | −0.099 | −0.100 | 0.921 |
| BMI-> BPI-II | 0.135 | 1.622 | 0.113 |
| FSS-> BPI-II | 0.060 | 2.285 | 0.028 * |
| FIM-> BPI-II | 0.020 | 0.386 | 0.702 |
| POMA-> BPI-II | −0.062 | −0.779 | 0.441 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liguori, S.; Moretti, A.; Toro, G.; Paoletta, M.; Palomba, A.; Barra, G.; Gimigliano, F.; Iolascon, G. Pain and Motor Function in Myotonic Dystrophy Type 1: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2023, 20, 5244. https://doi.org/10.3390/ijerph20075244
Liguori S, Moretti A, Toro G, Paoletta M, Palomba A, Barra G, Gimigliano F, Iolascon G. Pain and Motor Function in Myotonic Dystrophy Type 1: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2023; 20(7):5244. https://doi.org/10.3390/ijerph20075244
Chicago/Turabian StyleLiguori, Sara, Antimo Moretti, Giuseppe Toro, Marco Paoletta, Angela Palomba, Giuseppe Barra, Francesca Gimigliano, and Giovanni Iolascon. 2023. "Pain and Motor Function in Myotonic Dystrophy Type 1: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 20, no. 7: 5244. https://doi.org/10.3390/ijerph20075244
APA StyleLiguori, S., Moretti, A., Toro, G., Paoletta, M., Palomba, A., Barra, G., Gimigliano, F., & Iolascon, G. (2023). Pain and Motor Function in Myotonic Dystrophy Type 1: A Cross-Sectional Study. International Journal of Environmental Research and Public Health, 20(7), 5244. https://doi.org/10.3390/ijerph20075244