
Noncompliance with Hypertension Treatment and Related Factors among Kumamoto Earthquake Victims Who Experienced the COVID-19 Pandemic during Postearthquake Recovery Period



Abstract
1. Introduction
2. Materials and Methods
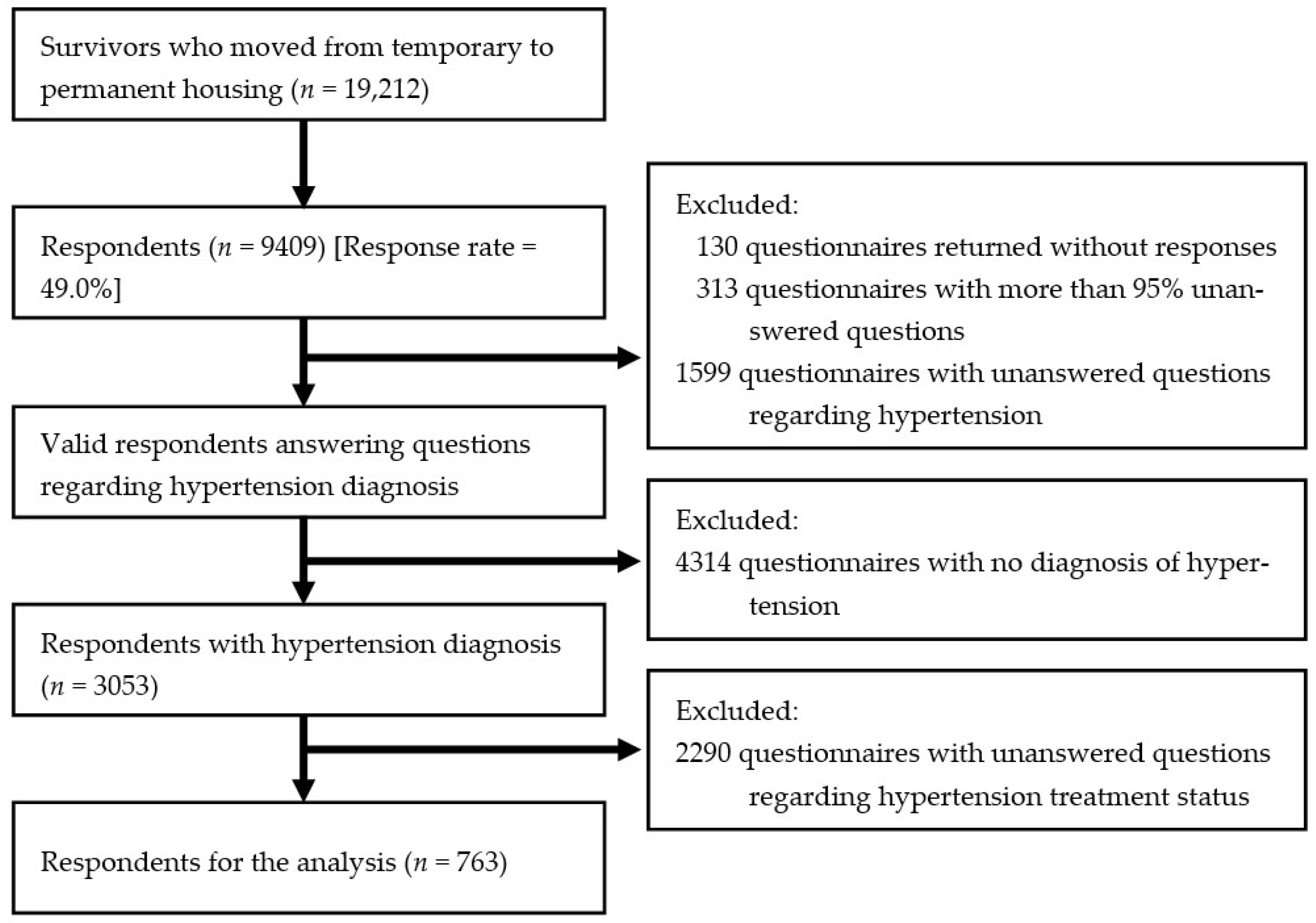
2.1. Participants
2.2. Hypertension Treatment Noncompliance
2.3. Other Variables
2.3.1. Attributes
2.3.2. Housing Conditions
2.3.3. Relations with Society
2.3.4. Health Conditions Other than Hypertension
2.3.5. Changes Due to COVID-19
2.4. Data Analysis
3. Results
4. Discussion
4.1. Factors Related to HTTx Noncompliance
4.1.1. Types of Permanent Dwellings
4.1.2. Self-Rated Health
4.1.3. Change Due to the COVID-19 Pandemic
4.2. Limitations and Significance of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Japan Meteorological Agency. The 2016 Kumamoto Earthquake—Portal. Available online: https://www.jma.go.jp/jma/en/2016_Kumamoto_Earthquake/2016_Kumamoto_Earthquake.html (accessed on 15 January 2023). (In Japanese)
- Hashimoto, M.; Savage, M.; Nishimura, T.; Horikawa, H.; Tsutsumi, H. 2016 Kumamoto earthquake sequence and its impact on earthquake science and hazard assessment. Earth Planets Space 2017, 69, 98. [Google Scholar] [CrossRef]
- Cabinet Office, Government of Japan. 2016 Kumamoto Earthquake. Available online: https://www.bousai.go.jp/kaigirep/houkokusho/hukkousesaku/saigaitaiou/output_html_1/pdf/201601.pdf (accessed on 15 January 2023).
- Mainichi Shimbun. Strongest Aftershock since April Jolts Kumamoto. Available online: https://mainichi.jp/english/articles/20160613/p2a/00m/0na/001000c (accessed on 15 January 2023).
- Chapter Overview of the Kumamoto Earthquake—Kumamoto City Website. Available online: https://www.city.kumamoto.jp/common/UploadFileDsp.aspx?c_id=5&id=19060&sub_id=1&flid=134903 (accessed on 31 January 2022). (In Japanese).
- Fire and Disaster Management Agency, Japan Ministry of Internal Affairs and Communications. Earthquake with Seismic Origin in the Kumamoto District, Kumamoto Prefecture; Report No. 120; Fire and Disaster Management Agency: Tokyo, Japan, 2016. Available online: https://www.fdma.go.jp/bn/2016/detail/960.html (accessed on 15 January 2023). (In Japanese)
- Ide-Okochi, A.; Samiso, T.; Kanamori, Y.; He, M.; Sakaguchi, M.; Fujimura, K. Depression, Insomnia, and Probable Post-Traumatic Stress Disorder among Survivors of the 2016 Kumamoto Earthquake and Related Factors during the Recovery Period Amidst the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 4403. [Google Scholar] [CrossRef] [PubMed]
- Babaie, J.; Naghipour, B.; Faridaalaee, G. Cardiovascular diseases in natural disasters; a systematic review. Arch. Acad. Emerg. Med. 2021, 9, e36. [Google Scholar] [PubMed]
- Satoh, M.; Kikuya, M.; Ohkubo, T.; Imai, Y. Acute and subacute effects of the Great East Japan Earthquake on home blood pressure values. Hypertension 2011, 58, e193–e194. [Google Scholar] [CrossRef]
- Narita, K.; Hoshide, S.; Tsoi, K.; Siddique, S.; Shin, J.; Chia, Y.; Tay, J.C.; Teo, B.W.; Turana, Y.; Chen, C.; et al. Disaster hypertension and cardiovascular events in the disaster and COVID-19 pandemic. J. Clin. Hypertens. 2021, 23, 575–583. [Google Scholar] [CrossRef]
- Suzuki, S.; Sakamoto, S.; Koide, M.; Fujita, H.; Sakuramoto, H.; Kuroda, T.; Kintaka, T.; Matsuo, T. Hanshin-Awaji earthquake as a trigger for acute myocardial infarction. Am. Heart J. 1997, 134, 974–977. [Google Scholar] [CrossRef]
- Kario, K. Disaster Hypertension—Its characteristics, mechanism, and management. Circ. J. 2012, 76, 553–562. [Google Scholar] [CrossRef]
- Nakaya, N.; Nakamura, T.; Tsuchiya, N.; Narita, A.; Tsuji, I.; Hozawa, A.; Tomita, H. Psychological distress and risk of withdrawing from hypertension treatment after an earthquake. Disaster Med. Public Health Prep. 2017, 11, 179–182. [Google Scholar] [CrossRef]
- Ministry of Health, Labor and Welfare. Visualizing the Data: Information on COVID-19 Infections. Available online: https://covid19.mhlw.go.jp/extensions/public/en/index.html (accessed on 15 January 2023).
- Pfefferbaum, B.; North, C.S. Mental health and the COVID-19 pandemic. N. Engl. J. Med. 2020, 383, 510–512. [Google Scholar] [CrossRef]
- Yamaguchi, S.; Okada, A.; Sunaga, S.; Ikeda Kurakawa, K.; Yamauchi, T.; Nangaku, M.; Kadowaki, T. Impact of COVID-19 pandemic on healthcare service use for non-COVID-19 patients in Japan: A retrospective cohort study. BMJ Open 2022, 12, e060390. [Google Scholar] [CrossRef]
- The Nishinippon Shimbun. Six Months after the End of Medical Fee Waiver, Some Point Out That It Will “Create New Victims”. Available online: https://www.nishinippon.co.jp/item/n/405659/ (accessed on 15 January 2023). (In Japanese).
- The Mainichi Newspaper. Questionnaire to Doctors and Dentists in the Affected Areas: 46% Refrain from Seeing a Doctor after the End of Medical Fee Waiver. Kumamoto. Available online: https://mainichi.jp/articles/20180123/ddl/k43/040/283000c (accessed on 15 January 2023). (In Japanese).
- Burnier, M.; Egan, B.M. Adherence in Hypertension. Circ. Res. 2019, 124, 1124–1140. [Google Scholar] [CrossRef]
- Statistical Survey Division, Kumamoto Prefecture. Kumamoto Prefecture Population Estimation Report (Annual Report). Available online: https://www.pref.kumamoto.jp/soshiki/20/78661.html (accessed on 15 January 2023). (In Japanese).
- Yoshida, S.; The Asahi Shimbun. 614 Evacuees Die Alone in Public Housing over Decade Since. Available online: https://www.asahi.com/ajw/articles/14250592 (accessed on 15 January 2023). (In Japanese).
- Hogg, D.; Kingham, S.; Wilson, T.M.; Ardagh, M. The effects of relocation and level of affectedness on mood and anxiety symptom treatments after the 2011 Christchurch earthquake. Soc. Sci. Med. 2016, 152, 18–26. [Google Scholar] [CrossRef]
- Holt-Lunstad, J.; Smith, B.; Layton, B. Social relationships and mortality risk: A meta-analytic review. PLoS Med. 2010, 7, e1000316. [Google Scholar] [CrossRef]
- Kinoshita, Y.; Nakayama, C.; Ito, N.; Moriyama, N.; Iwasa, H.; Yasumura, S. Subjective Well-being and Related Factors of Older Adults Nine and a Half Years after the Great East Japan Earthquake: A Cross-Sectional Study in the Coastal Area of Soma City. Int. J. Environ. Res. Public Health 2022, 19, 2639. [Google Scholar] [CrossRef]
- Wada, K.; Higuchi, Y.; Smith, D.R. Socioeconomic status and self-reported health among middle-aged Japanese men: Results from a nationwide longitudinal study. BMJ Open 2015, 5, e008178. [Google Scholar] [CrossRef]
- Tanaka, H.; Nusselder, W.J.; Kobayashi, Y.; Mackenbach, J.P. Socioeconomic inequalities in self-rated health in Japan, 32 European countries and the United States: An international comparative study. Scand. J. Public Health 2022. [Google Scholar] [CrossRef]
- Ministry of Health, Labour and Welfare. Report of the National Health and Nutrition Survey in 2019. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/kenkou_iryou/kenkou/eiyou/r1-houkoku_00002.html (accessed on 15 January 2023). (In Japanese)
- Hisamatsu, T.; Segawa, H.; Kadota, A.; Ohkubo, T.; Arima, H.; Miura, K. Epidemiology of hypertension in Japan: Beyond the new 2019 Japanese guidelines. Hypertens. Res. 2020, 43, 1344–1351. [Google Scholar] [CrossRef]
- Sasaki, Y.; Aida, J.; Tsuji, T.; Miyaguni, Y.; Tani, Y.; Koyama, S.; Matsuyama, Y.; Sato, Y.; Tsuboya, T.; Nagamine, Y.; et al. Does type of residential housing matter for depressive symptoms in the aftermath of a disaster? Insights from the Great East Japan Earthquake and Tsunami. Am. J. Epidemiol. 2018, 187, 455–464. [Google Scholar] [CrossRef]
- Moriyama, N.; Iwasa, H.; Tsubokura, M.; Kuroda, Y.; Yasumura, S. Living in the Restoration Public Housing after the Great East Japan Earthquake Correlates with Lower Subjective Well-Being of Older Adults. Int. J. Environ. Res. Public Health 2019, 16, 2696. [Google Scholar] [CrossRef]
- Alsabbagh, M.H.D.W.; Lemstra, M.; Eurich, D.; Lix, L.M.; Wilson, T.W.; Watson, E.; Blackburn, D.F. Socioeconomic Status and Nonadherence to Antihypertensive Drugs: A Systematic Review and Meta-Analysis. Value Health 2014, 17, 288–296. [Google Scholar] [CrossRef]
- Ma, C.; Zhou, W.; Huang, C.; Huang, S. A cross-sectional survey of self-rated health and its determinants in patients with hypertension. Appl. Nurs. Res. 2015, 28, 347–351. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.S.; Bohn, R.L.; Knight, E.; Glynn, R.J.; Mogun, H.; Avorn, J. Noncompliance with antihypertensive medications: The impact of depressive symptoms and psychosocial factors. J. Gen. Intern. Med. 2002, 17, 504–511. [Google Scholar] [CrossRef] [PubMed]
- Engström, G.; Hedblad, B.; Janzon, L. Subjective well-being associated with improved survival in smoking and hypertensive men. J. Cardiovasc. Risk 1999, 6, 257–261. [Google Scholar] [CrossRef] [PubMed]
- Lau, D.; McAlister, F.A. Implications of the COVID-19 pandemic for cardiovascular disease and risk-factor management. Can. J. Cardiol. 2021, 37, 722–732. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| n = 763 | |||
|---|---|---|---|
| n | % | ||
| Sex | Male | 328 | 43.0 |
| Female | 435 | 57.0 | |
| Age | 18–64 years old | 374 | 49.0 |
| 65+ years old | 389 | 51.0 | |
| Interruption of treatment | None | 525 | 68.8 |
| Yes | 238 | 31.2 | |
| Current residence | Owned house | 373 | 48.9 |
| Houses for rent | 240 | 31.5 | |
| Public housing | 114 | 14.9 | |
| RPH | 12 | 1.6 | |
| Other | 24 | 3.1 | |
| Cohabitant | None | 199 | 26.1 |
| Yes | 564 | 73.9 | |
| Self-rated health | Not healthy | 274 | 35.9 |
| Healthy | 489 | 64.1 | |
| Loneliness | None ** | 492 | 64.5 |
| Yes | 271 | 35.5 | |
| Community participation | No information of such events | 108 | 14.2 |
| None | 514 | 67.4 | |
| Yes | 141 | 18.5 | |
| Change of residential school district | None | 437 | 57.3 |
| Yes | 326 | 42.7 | |
| Decrease in income due to COVID-19 | None *** | 426 | 55.8 |
| Yes | 337 | 44.2 |
| n = 763 | |||||||
|---|---|---|---|---|---|---|---|
| HTTx Noncompliance | |||||||
| Applicable (Untreated or Interrupted Treatment) | Not Applicable (under Treatment) | ||||||
| n = 238 | n = 525 | p-Value | Cramér’s V | ||||
| n | % | n | % | ||||
| Sex | 0.914 | 0.040 | |||||
| Male | 103 | 43.3 | 225 | 42.9 | |||
| Female | 135 | 56.7 | 300 | 57.1 | |||
| Age | 143 | 60.1 | 231 | 44.0 | <0.001 | 0.149 | |
| 18–64 years old | 95 | 39.9 | 294 | 56.0 | |||
| 65+ years old | |||||||
| Cohabitant | 0.052 | 0.070 | |||||
| None | 73 | 30.7 | 126 | 24.0 | |||
| Yes | 165 | 69.3 | 399 | 76.0 | |||
| Self-rated health | <0.001 | 0.221 | |||||
| Not healthy | 123 | 51.7 | 151 | 28.8 | |||
| Healthy | 115 | 48.3 | 374 | 71.2 | |||
| Current residence | <0.001 | 0.216 | |||||
| Owned house | 79 | 33.2 | 294 | 56.0 | |||
| Houses for rent | 94 | 39.5 | 146 | 27.8 | |||
| Public housing | 50 | 21.0 | 64 | 12.2 | |||
| RPH | 6 | 2.5 | 6 | 1.1 | |||
| Other | 9 | 3.8 | 15 | 2.9 | |||
| Change of residential school district | 0.002 | 0.110 | |||||
| None | 117 | 49.2 | 320 | 61.0 | |||
| Yes | 121 | 50.8 | 205 | 39.0 | |||
| Loneliness | <0.001 | 0.156 | |||||
| None | 127 | 53.4 | 365 | 69.5 | |||
| Yes | 111 | 46.6 | 160 | 30.5 | |||
| Community participation | 0.734 | 0.028 | |||||
| No information of such events | 37 | 15.5 | 71 | 13.5 | |||
| None | 159 | 66.8 | 355 | 67.6 | |||
| Yes | 42 | 17.6 | 99 | 18.9 | |||
| Decrease in income due to COVID-19 | <0.001 | 0.290 | |||||
| None | 82 | 34.5 | 344 | 65.5 | |||
| Yes | 156 | 65.5 | 181 | 34.5 | |||
| n = 763 | |||
|---|---|---|---|
| HTTx Noncompliance | |||
| AOR | 95% CI | ||
| Sex (ref: male) | |||
| Female | 1.09 | 0.76–1.55 | |
| Age (ref: 18–64 years old) | |||
| 65 years and older | 0.97 | 0.96–0.99 | |
| Cohabitant (ref: yes) | |||
| No | 1.08 | 0.72–1.63 | |
| Current residence (ref: owned house) | |||
| Houses for rent | 1.92 | 1.20–3.07 | |
| Public housing | 2.47 | 1.38–4.42 | |
| RPH | 4.12 | 1.14–14.90 | |
| Other | 2.33 | 0.89–6.10 | |
| Change of residential school district (ref: none) | |||
| Yes | 0.87 | 0.57–1.33 | |
| Loneliness (ref: none) | |||
| Yes | 1.43 | 0.99–2.06 | |
| Community participation (ref: yes) | |||
| No information of such events | 0.60 | 0.32–1.12 | |
| None | 0.70 | 0.44–1.11 | |
| Self-rated health (ref: healthy) | |||
| Not healthy | 2.49 | 1.72–3.61 | |
| Decrease in income due to COVID-19 (ref: none) | |||
| Yes | 3.23 | 2.27–4.58 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ide-Okochi, A.; He, M.; Murayama, H.; Samiso, T.; Yoshinaga, N. Noncompliance with Hypertension Treatment and Related Factors among Kumamoto Earthquake Victims Who Experienced the COVID-19 Pandemic during Postearthquake Recovery Period. Int. J. Environ. Res. Public Health 2023, 20, 5203. https://doi.org/10.3390/ijerph20065203
Ide-Okochi A, He M, Murayama H, Samiso T, Yoshinaga N. Noncompliance with Hypertension Treatment and Related Factors among Kumamoto Earthquake Victims Who Experienced the COVID-19 Pandemic during Postearthquake Recovery Period. International Journal of Environmental Research and Public Health. 2023; 20(6):5203. https://doi.org/10.3390/ijerph20065203
Chicago/Turabian StyleIde-Okochi, Ayako, Mu He, Hiroshi Murayama, Tomonori Samiso, and Naoki Yoshinaga. 2023. "Noncompliance with Hypertension Treatment and Related Factors among Kumamoto Earthquake Victims Who Experienced the COVID-19 Pandemic during Postearthquake Recovery Period" International Journal of Environmental Research and Public Health 20, no. 6: 5203. https://doi.org/10.3390/ijerph20065203
APA StyleIde-Okochi, A., He, M., Murayama, H., Samiso, T., & Yoshinaga, N. (2023). Noncompliance with Hypertension Treatment and Related Factors among Kumamoto Earthquake Victims Who Experienced the COVID-19 Pandemic during Postearthquake Recovery Period. International Journal of Environmental Research and Public Health, 20(6), 5203. https://doi.org/10.3390/ijerph20065203