
The Moderating Role of Self-Care Behaviors in Personal Care Aides of Older Adults during the COVID-19 Pandemic


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design, Participants and Procedure
2.2. Measures
2.2.1. Sociodemographic Questionnaire [44]
2.2.2. Short-Form Health Survey-12 (SF-12) [45,46]
2.2.3. Depression, Anxiety and Stress Scale (DASS-21) [47,48]
2.2.4. Self-Care Assessment for Psychologists Scale (SCAP) [35,50]
2.2.5. Preventive COVID-19 Infection Behaviors Scale (PCOVID-19IBS) [51,52]
2.2.6. COVID-19 Traumatic Stress Scale (COVID-19TSC) [52,54]
2.3. Data Analysis
3. Results
3.1. Sample Description
3.2. Differences in QoL According to Caregiving Contextual Variables
3.3. Contributors to QoL
3.4. Moderating Role of Self-Care between COVID-19 Traumatic Stress and QoL
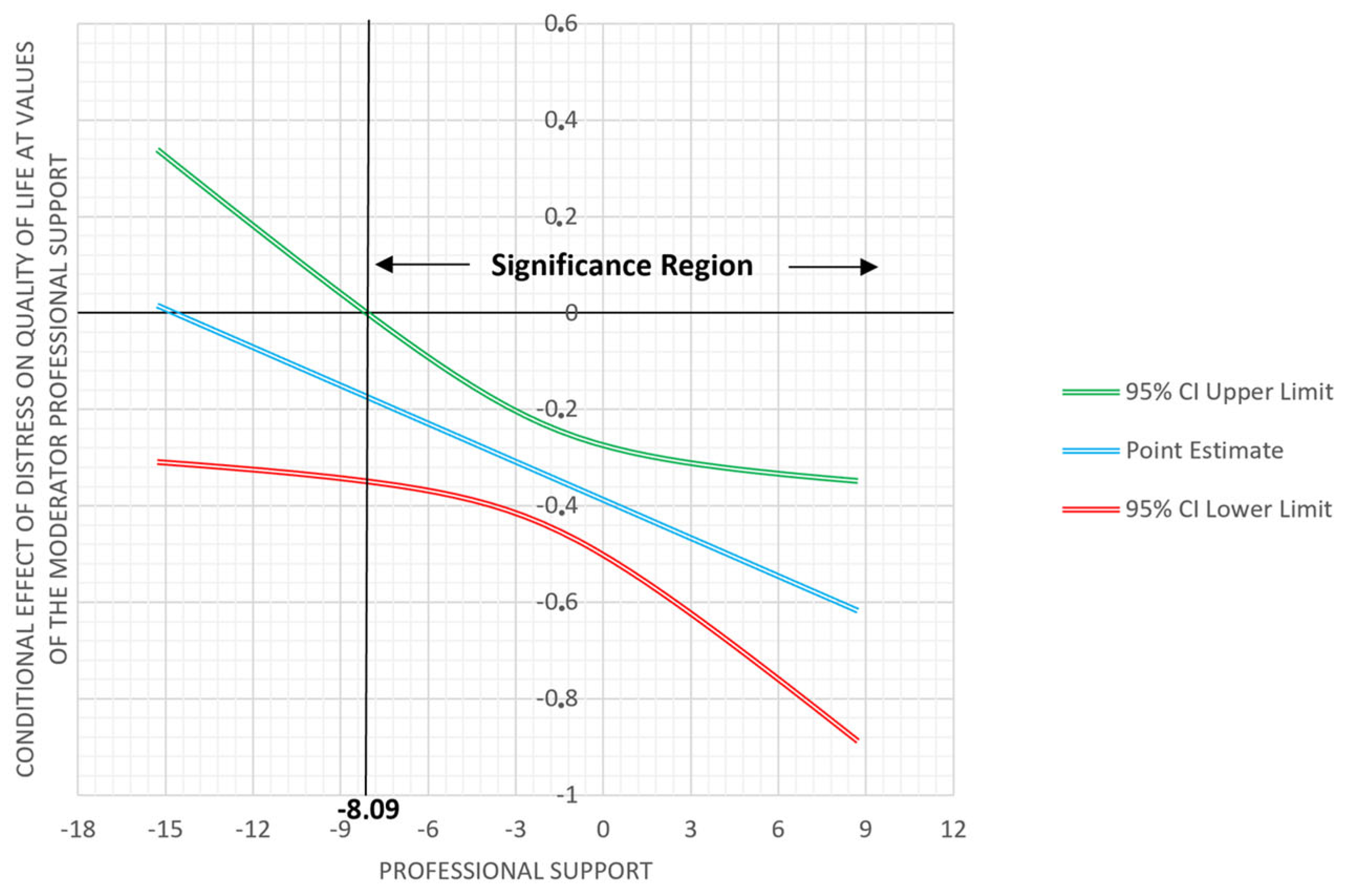
3.5. Moderating Role of Self-Care between Distress and QoL
4. Discussion
Limitations and Future Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dias, E.F. O Envelhecimento populacional e o direito à saúde da pessoa idosa. Rev. Jurídica Direito Soc. Justiça 2015, 1, 1–14. Available online: https://periodicosonline.uems.br/index.php/RJDSJ/article/view/659 (accessed on 29 December 2022).
- United Nations. Department of Economic and Social Affairs: Population Division; World population ageing 2019; United Nations: New York, NY, USA, 2019; Available online: https://www.un.org/development/desa/pd/news/world-population-ageing-2019-0 (accessed on 25 September 2022).
- Wiles, J. Informal caregivers’ experiences of formal support in a changing context. Health Soc. Care Community 2003, 11, 189–207. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, A.S.S. “Cuidar Para Apessoar”: Proposta de UM Programa de Prevenção Do Burnout E de Promoção Do Engagement Para Ajudantes de ação Direta Que Trabalham Em Respostas Sociais Para a População Idosa. Ph.D. Thesis, Instituto Universitário de Lisboa, Repositório do Iscte, Lisbon, Portugal, 2015. [Google Scholar]
- Li, J.; Song, Y. Formal and Informal Care. In Encyclopedia of Gerontology and Population Aging; Gu, D., Dupre, M.E., Eds.; Springer: New York, NY, USA, 2019; pp. 1–8. [Google Scholar] [CrossRef]
- Stone, R.; Harahan, M.F. Improving the long-term care workforce serving older adults. Health Aff. 2010, 29, 109–115. [Google Scholar] [CrossRef]
- Guerra, M.; Martins, I.; Santos, D.; Veiga, J.; Moitas, R.; Silva, R. Cuidadores formais de idosos institucionalizados: Perceções e satisfação profissional. Gestão Desenvolv. 2019, 27, 291–313. [Google Scholar] [CrossRef]
- Wilks, S.E.; Croom, B. Perceived stress and resilience in Alzheimer’s disease caregivers: Testing moderation and mediation models of social support. Aging Ment. Health 2008, 12, 357–365. [Google Scholar] [CrossRef]
- Etters, L.; Goodall, D.; Harrison, B.E. Caregiver burden among dementia patient caregivers: A review of the literature. J. Am. Assoc. Nurse Pract. 2008, 20, 423–428. [Google Scholar] [CrossRef]
- Sołtys, A.; Tyburski, E. Predictors of mental health problems in formal and informal caregivers of patients with Alzheimer’s disease. BMC Psychiatry 2020, 20, 435. [Google Scholar] [CrossRef]
- Aguilar, L.V.; Peña, M.Z.; Ponce, G.C. Sobrecarga y dolor percibido en cuidadoras de ancianos dependientes. Enferm. Glob. 2012, 11, 166–171. [Google Scholar] [CrossRef]
- Jeong, Y.G.; Jeong, Y.J.; Kim, W.C.; Kim, J.S. The mediating effect of caregiver burden on the caregivers’ quality of life. J. Phys. There. Sci. 2015, 27, 1543–1547. [Google Scholar] [CrossRef]
- World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing on COVID. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 11 March 2020).
- World Health Organization. Portugal: WHO Coronavirus Disease (COVID-19) Dashboard|Portugal Situation. Available online: https://covid19.who.int/region/euro/country/pt (accessed on 25 November 2022).
- Anderson, R.M.; Heesterbeek, H.; Klinkenberg, D.; Hollingsworth, T.D. How will Country-Based Mitigation Measures Influence the Course of the COVID-19 Epidemic? Lancet: London, UK, 2020; Volume 395, pp. 931–934. [Google Scholar] [CrossRef]
- Brown, E.E.; Kumar, S.; Rajji, T.K.; Pollock, B.G.; Mulsant, B.H. Anticipating and mitigating the impact of the COVID-19 pandemic on Alzheimer’s disease and related dementias. Am. J. Geriatr. Psychiatry 2020, 28, 712–721. [Google Scholar] [CrossRef]
- Cheng, W.; Zhang, F.; Liu, Z.; Zhang, H.; Lyu, Y.; Xu, H.; Hua, Y.; Gu, J.; Yang, Z.; Liu, J. A psychological health support scheme for medical teams in COVID-19 outbreak and its effectiveness. Arch. Gen. Psychiatry 2020, 33, e100288. [Google Scholar] [CrossRef] [PubMed]
- Galehdar, N.; Toulabi, T.; Kamran, A.; Heydari, H. Exploring nurses’ perception about the care needs of patients with COVID-19: A qualitative study. BMC Nurs. 2020, 19, 119. [Google Scholar] [CrossRef] [PubMed]
- Cagnin, A.; Di Lorenzo, R.; Marra, C.; Bonanni, L.; Cupidi, C.; Laganà, V.; Rubino, E.; Vacca, A.; Provero, P.; Isella, V.; et al. Behavioral and psychological effects of coronavirus disease-19 quarantine in patients with dementia. Front. Psychiatry 2020, 11, 578015. [Google Scholar] [CrossRef] [PubMed]
- Dourado, M.; Belfort, T.; Monteiro, A.; Lucena, A.; Barbeito Lacerda, I.; Gaigher, J.; Baptista, M.; Brandt, M.; Kimura, N.; Souza, N.; et al. COVID-19: Challenges for dementia care and research. Dement. Neuropsychol. 2020, 14, 340–344. [Google Scholar] [CrossRef] [PubMed]
- Forte, G.; Favieri, F.; Tambelli, R.; Casagrande, M. COVID-19 Pandemic in the Italian population: Validation of a post-traumatic stress disorder questionnaire and prevalence of PTSD symptomatology. Int. J. Environ. Res. Public Health 2020, 17, 4151. [Google Scholar] [CrossRef]
- Caillet, A.; Allaouchiche, B. COVID Impact: Psychological disorders and COVID-19 among ICU caregivers in April and October 2020. Minerva Anestesiol. 2021, 87, 950–951. [Google Scholar] [CrossRef]
- d’Ettorre, G.; Ceccarelli, G.; Santinelli, L.; Vassalini, P.; Innocenti, G.P.; Alessandri, F.; Koukopoulos, A.E.; Russo, A.; d’Ettorre, G.; Tarsitani, L. Post-Traumatic stress symptoms in healthcare workers dealing with the COVID-19 pandemic: A systematic review. Int. J. Environ. Res. Public Health 2021, 18, 601. [Google Scholar] [CrossRef]
- Luceño-Moreno, L.; Talavera-Velasco, B.; García-Albuerne, Y.; Martín-García, J. Symptoms of posttraumatic stress, anxiety, depression, levels of resilience and burnout in Spanish health personnel during the COVID-19 pandemic. Int. J. Environ. Res. Public Health 2020, 17, 5514. [Google Scholar] [CrossRef]
- Giusti, E.M.; Pedroli, E.; D’Aniello, G.E.; Stramba Badiale, C.; Pietrabissa, G.; Manna, C.; Stramba Badiale, M.; Riva, G.; Castelnuovo, G.; Molinari, E. The psychological impact of the COVID-19 outbreak on health professionals: A cross-sectional study. Front. Psychol. 2020, 11, 1684. [Google Scholar] [CrossRef]
- Zhang, Y.; Ma, Z.F. Impact of the COVID-19 Pandemic on mental health and quality of life among local residents in Liaoning province, China: A cross-sectional study. Int. J. Environ. Res. Public Health 2020, 17, 2381. [Google Scholar] [CrossRef]
- Ayandele, O.; Ramos-Vera, C.A.; Iorfa, S.K.; Chovwen, C.O.; Olapegba, P.O. Exploring the complex pathways between the fear of COVID-19 and preventive health behavior among Nigerians: Mediation and moderation analyses. Am. J. Trop. Med. Hyg. 2021, 105, 701–707. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.G.; Kamruzzaman, M.; Rahman, M.N.; Mahmood, M.; Uddin, M.A. Quality of life in the COVID-19 outbreak: Influence of psychological distress, government strategies, social distancing, and emotional recovery. Heliyon 2021, 7, e06407. [Google Scholar] [CrossRef]
- Geirdal, A.Ø.; Ruffolo, M.; Leung, J.; Thygesen, H.; Price, D.; Bonsaksen, T.; Schoultz, M. Mental health, quality of life, wellbeing, loneliness and use of social media in a time of social distancing during the COVID-19 outbreak. A cross-country comparative study. J. Ment. Health 2021, 30, 148–155. [Google Scholar] [CrossRef]
- Sandesh, R.; Shahid, W.; Dev, K.; Mandhan, N.; Shankar, P.; Shaikh, A.; Rizwan, A. Impact of COVID-19 on the mental health of healthcare professionals in Pakistan. Queries 2020, 12, e8974. [Google Scholar] [CrossRef] [PubMed]
- Shechter, A.; Diaz, F.; Moise, N.; Anstey, D.E.; Ye, S.; Agarwal, S.; Birk, J.L.; Brodie, D.; Cannon, D.E.; Chang, B.; et al. Psychological distress, coping behaviors, and preferences for support among New York healthcare workers during the COVID-19 pandemic. Gen. Hosp. Psychiatry 2020, 66, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Lai, J.; Ma, S.; Wang, Y.; Cai, Z.; Hu, J.; Wei, N.; Wu, J.; Du, H.; Chen, T.; Li, R.; et al. Factors associated with mental health outcomes among health care workers exposed to coronavirus disease 2019. JAMA Netw. Open 2020, 3, e203976. [Google Scholar] [CrossRef]
- Porcari, D.E.; Palmer, K.; Spalletta, G.; Ciullo, V.; Banaj, N. A survey for examining the effects of COVID-19 and infection control measures in older persons with mild cognitive impairment and dementia and their caregivers. Front. Psychiatry 2020, 11, 599851. [Google Scholar] [CrossRef] [PubMed]
- Godfrey, C.M.; Harrison, M.B.; Lysaght, R.; Lamb, M.; Graham, I.D.; Oakley, P. Care of self-care of other-care of another: The meaning of self-care from research, practice, policy and industry perspectives. Int. J. Evid.-Based Healthc. 2011, 9, 3–24. [Google Scholar] [CrossRef]
- Dorociak, K.E.; Rupert, P.A.; Bryant, F.B.; Zahniser, E. Development of a self-care assessment for psychologists. J. Cons. Psychol. 2017, 64, 325–334. [Google Scholar] [CrossRef]
- Ayala, E.E.; Winseman, J.S.; Johnsen, R.D.; Mason, H.R.C.U.S. medical students who engage in self-care report less stress and higher quality of life. BMC Med. Educ. 2018, 18, 189. [Google Scholar] [CrossRef]
- Pender, N.J.; Murdaugh, C.; Parsons, M. Health Promotion in Nursing Practice, 6th ed.; Prentice Hall: Upper Saddle River, NJ, USA, 2010. [Google Scholar]
- Acton, G.J. Health-promoting self-care in family caregivers. West. J. Nurse. Res. 2002, 24, 73–86. [Google Scholar] [CrossRef] [PubMed]
- Ayala, E.E.; Ellis, M.V.; Grudev, N.; Cole, J. Women in health service psychology programs: Stress, self-care, and quality of life. Train. Educ. Prof. Psychol. 2017, 11, 18–25. [Google Scholar] [CrossRef]
- Sansó, N.; Galiana, L.; Oliver, A.; Pascual, A.; Sinclair, S.; Benito, E. Palliative care professionals’ inner life: Exploring the relationships among awareness, self-care, and compassion satisfaction and fatigue, burnout, and coping with death. J. Pain Symptom Manag. 2015, 50, 200–207. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Q.; Zhang, X. Influence of workload, mental health and professional quality of life on healthcare workers’ hand hygiene behavior in medical aid during COVID-19 pandemic. Res. Sq. 2020. preprint. [Google Scholar] [CrossRef]
- Dreher, M.M.; Hughes, R.G.; Handley, P.A.; Tavakoli, A.S. Improving retention among certified nursing assistants through compassion fatigue awareness and self-care skills education. Holiest. Nurse. Pract. 2019, 37, 296–308. [Google Scholar] [CrossRef] [PubMed]
- Pearlin, L.I.; Mullan, J.T.; Semple, S.J.; Skaff, M.M. Caregiving and the stress process: An overview of concepts and their measures. Gerontologist 1990, 30, 583–594. [Google Scholar] [CrossRef] [PubMed]
- Pereira, M.G.; Brito, L.; Alves, O. Projeto Investigação-Ação nas Demências, Grupo de Investigação em Saúde & Família; Escola de Psicologia, Universidade do Minho: Braga, Portugal, 2020. [Google Scholar]
- Ware, J.E.; Kosinski, M.; Keller, J.E. A 12-item short-form health survey: Construction of scales and preliminary tests of reliability and validity. Med. Care 1996, 34, 220–233. [Google Scholar] [CrossRef]
- Ferreira, P.L.; Ferreira, L.N.; Pereira, L.N. Medidas sumário física e mental de estado de saúde para a população portuguesa. Rec. Port. Saúde Pública 2012, 30, 163–171. [Google Scholar] [CrossRef]
- Lovibond, P.F.; Lovibond, S.H. The structure of negative emotional states: Comparison of the Depression Anxiety Stress scales (DASS) with the beck depression and anxiety inventories. Behav. Res. There. 1995, 33, 335–343. [Google Scholar] [CrossRef]
- Pais-Ribeiro, J.; Honrado, A.; Leal, I. Contribuição para o estudo da adaptação portuguesa das escalas de depressão ansiedade stress de Lovibond e Lovibond. Psychologica 2004, 36, 235–246. [Google Scholar]
- Antunes, S.M.; Mónico, L.S.M. Depressão, ansiedade e stress em doentes deprimidos: Estudo com a EADS-21. Int. J. Sch. Educ. Psychol. 2015, 2, 419–428. [Google Scholar] [CrossRef]
- Reis, M.T.S.C.D.C. O Autocuidado DOS Psicólogos: Adaptação DA Self-care Assessment for Psychologists Scale (SCAP) Para Portugal. Ph.D. Thesis, Repositório da Universidade de Lisboa, Lisbon, Portugal, 2020. [Google Scholar]
- Chang, K.; Hou, W.; Pakpour, A.H.; Lin, C. Psychometric testing of three COVID-19-related scales among people with mental illness. Int. J. Ment. Health Addict. 2020, 20, 324–336. [Google Scholar] [CrossRef] [PubMed]
- Leite, Â.; Almeida, A.C.; Pereira, M.G. COVID-19 traumatic stress and preventive COVID infection behaviors scale: Psychometric properties in Portuguese male adults. J. Men’s Health 2022, 18, 110. (In Portuguese) [Google Scholar] [CrossRef]
- Taber, K.S. The Use of cronbach’s alpha when developing and reporting research instruments in science education. Res. SCI. Educ. 2018, 48, 1273–1296. [Google Scholar] [CrossRef]
- Kira, I.A.; Shuwiekh, H.A.; Rice, K.G.; Ashby, J.S.; Elwakeel, S.A.; Sous, M.S.F.; Jamil, H.J. Measuring COVID-19 as traumatic stress: Initial psychometric and validation. J. Loss Trauma 2020, 26, 220–237. [Google Scholar] [CrossRef]
- Kheiraoui, F.; Gualano, M.R.; Mannocci, A.; Boccia, A.; La Torre, G. Quality of life among healthcare workers: A multicenter cross-sectional study in Italy. Public Health 2012, 126, 624–629. [Google Scholar] [CrossRef]
- Muthuri, R.N.D.K.; Senkubuge, F.; Hongoro, C. Predictors of health-related quality of life among healthcare workers in the context of health system strengthening in Kenya. Healthcare 2021, 9, 18. [Google Scholar] [CrossRef] [PubMed]
- Decadt, I.; Laenen, A.; Celus, J.; Geyskens, S.; Vansteenlandt, H.; Coolbrandt, A. Caregiver distress and quality of life in primary caregivers of oncology patients in active treatment and follow-up. Eur. J. Cancer Care 2021, 30, e13399. [Google Scholar] [CrossRef]
- Manh Than, H.; Minh Nong, V.; Trung Nguyen, C.; Phu Dong, K.; Ngo, H.T.; Thu Doan, T.; Thu Do, N.; Huyen Thi Nguyen, T.; Van Do, T.; Xuan Dao, C.; et al. Mental health and health-related quality-of-life outcomes among frontline health workers during the peak of COVID-19 outbreak in Vietnam: A cross-sectional study. Risk Manag. Healthc. Policy 2020, 13, 2927–2936. [Google Scholar] [CrossRef]
- Hudson, P.; Trauer, T.; Kelly, B.; O’Connor, M.; Thomas, K.; Summers, M.; Zordan, R.; White, V. Reducing the psychological distress of family caregivers of home-based palliative care patients: Short-term effects from a randomised controlled trial. Psycho. Oncol. 2013, 22, 1987–1993. [Google Scholar] [CrossRef]
- Sambasivam, R.; Liu, J.; Vaingankar, J.A.; Ong, H.L.; Tan, M.-E.; Fauziana, R.; Picco, L.; Chong, S.A.; Subramaniam, M. The hidden patient: Chronic physical morbidity, psychological distress, and quality of life in caregivers of older adults: Physical and mental health of caregivers. Psychogeriatrics 2019, 19, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Li, W.Q.; Yuan, P.; Sun, J.; Xu, M.L.; Wang, Q.X.; Ge, D.D.; Jiang, M.M.; Xing, L.Q.; Du, W.J.; Li, Q. Resilience, coping style, and COVID-19 stress: Effects on the quality of life in frontline health care workers. Psychol. Health Med. 2022, 27, 312–324. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Ji, R.; Ji, Y.; Liu, M.; Wang, R.; Xu, C. Relationship between acute stress responses and quality of life in Chinese health care workers during the COVID-19 outbreak. Front. Psychol. 2021, 12, 614964. [Google Scholar] [CrossRef] [PubMed]
- Bang, Y.R.; Park, S.C.; Jang, O.J.; Kim, J.H.; Kim, E.O.; Kim, S.H.; Park, J.H. Lifestyle changes that impact personal quality of life in the COVID-19 pandemic in South Korea. Psychiatry Investig. 2021, 18, 701–707. [Google Scholar] [CrossRef]
- Pasayan, E. Exploring the vulnerability of frontline nurses to COVID-19 and its impact on perceived stress. J. Taibah Univ. Med. Sci. 2020, 15, 404–409. [Google Scholar] [CrossRef]
- Shanafelt, T.D.; Gorringe, G.; Menaker, R.; Storz, K.A.; Reeves, D.; Buskirk, S.J.; Sloan, J.A.; Swensen, S.J. Impact of organizational leadership on physician burnout and satisfaction. Mayo Clin. Proc. 2015, 90, 432–440. [Google Scholar] [CrossRef]
- Pereira, M.G.; Abreu, A.R.; Rego, D.; Ferreira, G.; Lima, S. Contributors and moderators of quality of life in caregivers of Alzheimer’s disease patients. Exp. Aging Res. 2021, 47, 357–372. [Google Scholar] [CrossRef]
- Lucchetti, G.; Lucchetti, A.L.G.; Oliveira, G.R.; Crispim, D.; Pires, S.L.; Gorzoni, M.L.; Panicio, C.R.G.; Koenig, H.G. Nursing home care: Exploring the role of religion in the mental health, quality of life and stress of formal caregivers: Religiousness and formal caregivers. J. Psychiatr. Nurs. 2014, 21, 403–413. [Google Scholar] [CrossRef]
- Huang, C.-Y.; Musil, C.M.; Zauszniewski, J.A.; Wykle, M.L. Effects of social support and coping of family caregivers of older adults with dementia in Taiwan. Int. J. Aging Hum. Dev. 2006, 63, 1–25. [Google Scholar] [CrossRef]
- Bloomquist, K.R.; Wood, L.; Friedmeyer-Trainor, K.; Kim, H.W. Self-care and professional quality of life: Predictive factors among MSW practitioners. Adv. Soc. Work 2015, 16, 292–311. [Google Scholar] [CrossRef]


{kind=link}
| Continuous Variable | Min | Max | Mean | SD |
|---|---|---|---|---|
| Age | 21 | 66 | 42.2 | 10.1 |
| Education (years) | 4 | 20 | 11.4 | 3.4 |
| Duration of care (in years) | 1 | 32 | 7.8 | 6.8 |
| Categorical Variables | Frequency | % | ||
| Material Status | ||||
| Single/Divorced/Separated | 42 | 33.1 | ||
| Married | 85 | 66.9 | ||
| Caregiver Typology | ||||
| Formal caregiver—Nursing home | 100 | 78.7 | ||
| Formal caregiver—Home Support | 27 | 21.3 | ||
| Working hours per day | ||||
| 0–8 h | 113 | 89.2 | ||
| 8–18 h | 14 | 10.8 | ||
| Weekly days off | ||||
| None | 2 | 1.6 | ||
| 1 day off | 12 | 9.4 | ||
| 2 days off | 107 | 84.3 | ||
| More than two | 6 | 4.7 | ||
| Measures | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Quality of Life | — | ||||||||||||
| 2. General Physical Health Dimension | 0.87 *** | — | |||||||||||
| 3. General Mental Health Dimension | 0.85 *** | 0.54 *** | — | ||||||||||
| 4. Age | −0.12 | −0.28 ** | 0.07 | — | |||||||||
| 5. Duration of care | −0.20 * | −0.21 * | −0.16 | 0.25 ** | — | ||||||||
| 6. Years of education | 0.06 | 0.19 * | −0.09 | −0.39 *** | −0.17 | — | |||||||
| 7. Distress | −0.54 *** | −0.42 *** | −0.45 *** | 0.01 | 0.12 | −0.11 | — | ||||||
| 8. COVID-19 traumatic stress | −0.43 *** | −0.30 *** | −0.37 *** | −0.01 | 0.09 | 0.02 | 0.30 *** | — | |||||
| 9. Preventive behaviors | −0.04 | 0.06 | −0.10 | −0.09 | 0.04 | 0.05 | 0.03 | 0.47 *** | — | ||||
| Self-Care | |||||||||||||
| 10. Professional Support | 0.37 *** | 0.29 *** | 0.36 *** | −0.02 | 0.16 | 0.23 * | −0.30 *** | −0.14 | 0.04 | — | |||
| 11. Professional Development | 0.25 ** | 0.20 * | 0.31 *** | −0.10 | 0.17 | 0.12 | −0.12 | −0.03 | 0.03 | 0.55 *** | — | ||
| 12. Life Balance | 0.38 *** | 0.24 ** | 0.43 *** | −0.15 | 0.10 | 0.29 ** | −0.23 * | −0.10 | 0.09 | 0.57 *** | 0.64 *** | — | |
| 13. Cognitive Strategies | 0.47 *** | 0.35 *** | 0.47 *** | −0.15 | −0.05 | 0.23 ** | −0.34 *** | −0.12 | 0.10 | 0.57 *** | 0.47 *** | 0.65 *** | — |
| Variables | Model 1 | Model 2 | ||
|---|---|---|---|---|
| B | t | B | t | |
| -Duration of care | −0.22 * | −2.29 * | −0.17 * | −2.20 * |
| -Distress | −0.24 *** | −4.49 *** | ||
| -COVID-19 Traumatic Stress | −0.31 *** | −3.95 *** | ||
| -Professional Support | 0.10 | 0.84 | ||
| -Life Balance | 0.20 | 1.36 | ||
| -Cognitive Strategies | 0.35 * | 2.06 * | ||
| R2 | 0.04 | 0.49 | ||
| F | 5.25 * | 19.03 *** | ||
| ∆R2 | 0.03 | 0.45 | ||
| ∆F | 5.25 * | 20.95 *** | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pereira, M.G.; Gonçalves, A.F.; Brito, L. The Moderating Role of Self-Care Behaviors in Personal Care Aides of Older Adults during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2023, 20, 5177. https://doi.org/10.3390/ijerph20065177
Pereira MG, Gonçalves AF, Brito L. The Moderating Role of Self-Care Behaviors in Personal Care Aides of Older Adults during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2023; 20(6):5177. https://doi.org/10.3390/ijerph20065177
Chicago/Turabian StylePereira, M. Graça, Ana Filipa Gonçalves, and Laura Brito. 2023. "The Moderating Role of Self-Care Behaviors in Personal Care Aides of Older Adults during the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 20, no. 6: 5177. https://doi.org/10.3390/ijerph20065177
APA StylePereira, M. G., Gonçalves, A. F., & Brito, L. (2023). The Moderating Role of Self-Care Behaviors in Personal Care Aides of Older Adults during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health, 20(6), 5177. https://doi.org/10.3390/ijerph20065177