

An Assessment of Austrian School Students’ Mental Health and Their Wish for Support: A Mixed Methods Approach

 , , , , , , and
, , , , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Variables
2.3.1. Wish for Support
2.3.2. Type of Support (Open Question)
2.3.3. Depressive Symptoms (PHQ-9)
2.3.4. Anxiety (GAD-7)
2.3.5. Insomnia (ISI)
2.3.6. Perceived Stress (PSS-10)
2.3.7. Eating Disorders (SCOFF)
2.3.8. Alcohol Abuse (CAGE)
2.3.9. Sociodemographic Characteristics
2.4. Data Analysis
2.4.1. Qualitative Data Analysis
2.4.2. Quantitative and Mixed Methods Analysis
- differences in the amount of clinically relevant mental health problems (depression, anxiety, stress, insomnia, eating problems, alcohol abuse) between female, male, and diverse participants, as well as between the age groups of 14 to 17 and 18 to 20 years.
- differences between the students with a wish for support and students without a wish for support in gender, age group, and clinically relevant mental health problems (depression, anxiety, stress, insomnia, eating problems, alcohol abuse).
- differences between the students with a wish for professional help and students without a wish for professional help in gender, age group, and clinically relevant mental health problems (depression, anxiety, stress, insomnia, eating problems, alcohol abuse).
- differences between the students with a wish to talk to someone and students without a wish to talk to someone in gender, age group, and clinically relevant mental health problems (depression, anxiety, stress, insomnia, eating problems, alcohol abuse).
3. Results
3.1. Sample
3.2. Qualitative Results
3.3. Quantitative and Mixed Methods Results
3.3.1. Mental Health Indicators
3.3.2. Wish for Support
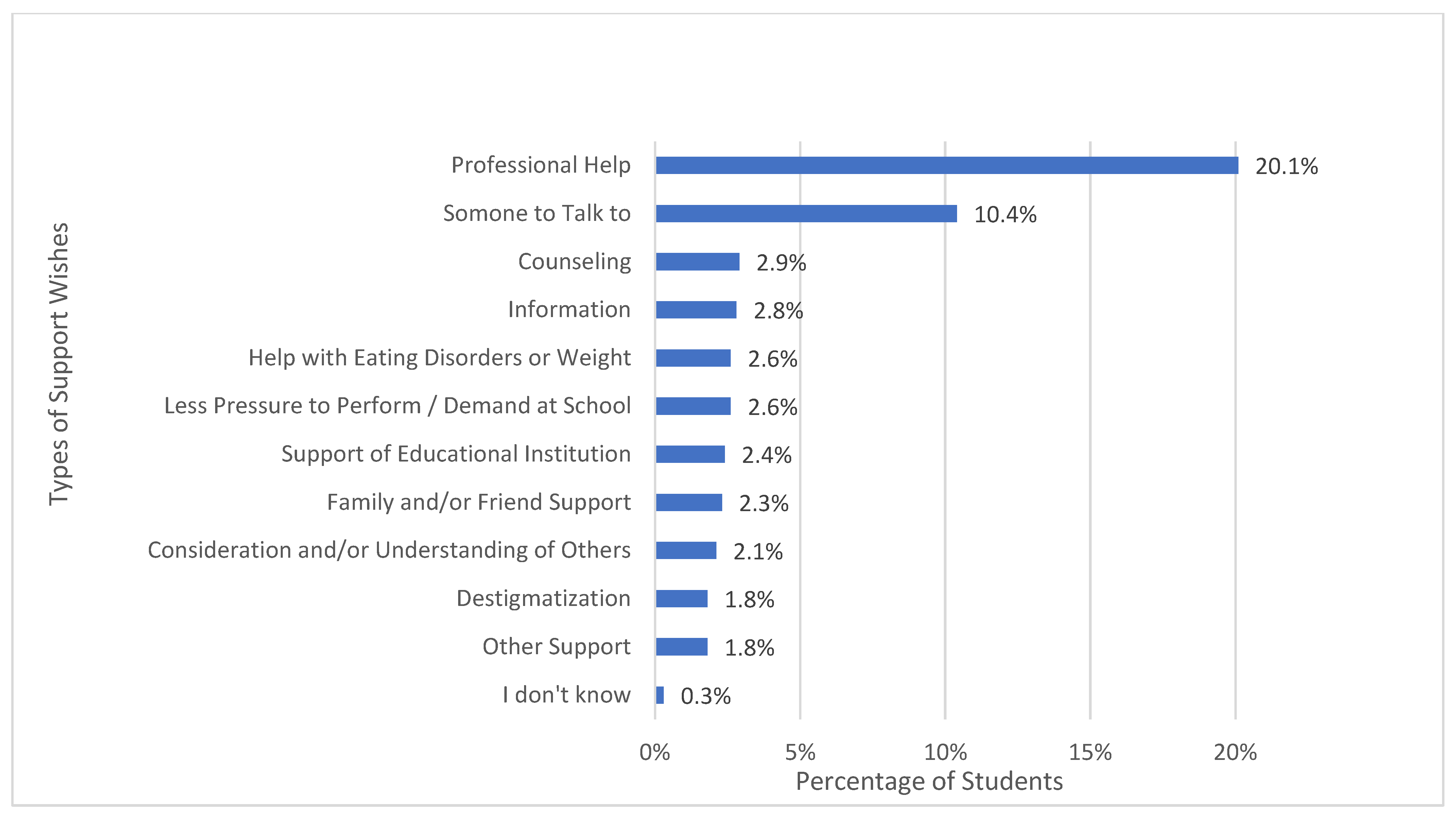
3.3.3. Types of Support Wishes
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ravens-Sieberer, U.; Kaman, A.; Erhart, M.; Devine, J.; Schlack, R.; Otto, C. Impact of the COVID-19 pandemic on quality of life and mental health in children and adolescents in Germany. Eur. Child Adolesc. Psychiatry 2021, 37, 879–889. [Google Scholar] [CrossRef] [PubMed]
- Octavius, G.S.; Silviani, F.R.; Lesmandjaja, A.; Juliansen, A. Impact of COVID-19 on adolescents’ mental health: A systematic review. Middle East Curr. Psychiatry 2020, 27, 72. [Google Scholar] [CrossRef]
- Hossain, M.M.; Tasnim, S.; Sultana, A.; Faizah, F.; Mazumder, H.; Zou, L.; McKyer, E.L.J.; Ahmed, H.U.; Ma, P. Epidemiology of mental health problems in COVID-19: A review. F1000Research 2020, 9, 636. [Google Scholar] [CrossRef]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [PubMed]
- Galea, S.; Merchant, R.M.; Lurie, N. The Mental Health Consequences of COVID-19 and Physical Distancing: The Need for Prevention and Early Intervention. JAMA Intern. Med. 2020, 180, 817–818. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Zhao, N. Generalized anxiety disorder, depressive symptoms and sleep quality during COVID-19 outbreak in China: A web-based cross-sectional survey. Psychiatry Res. 2020, 288, 112954. [Google Scholar] [CrossRef] [PubMed]
- Salari, N.; Hosseinian-Far, A.; Jalali, R.; Vaisi-Raygani, A.; Rasoulpoor, S.; Mohammadi, M.; Rasoulpoor, S.; Khaledi-Paveh, B. Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: A systematic review and meta-analysis. Glob. Health 2020, 16, 57. [Google Scholar] [CrossRef]
- Gualano, M.R.; Lo Moro, G.; Voglino, G.; Bert, F.; Siliquini, R. Effects of Covid-19 Lockdown on Mental Health and Sleep Disturbances in Italy. Int. J. Environ. Res. Public Health 2020, 17, 4779. [Google Scholar] [CrossRef]
- Wu, T.; Jia, X.; Shi, H.; Niu, J.; Yin, X.; Xie, J.; Wang, X. Prevalence of mental health problems during the COVID-19 pandemic: A systematic review and meta-analysis. J. Affect. Disord. 2021, 281, 91–98. [Google Scholar] [CrossRef]
- Pieh, C.; Budimir, S.; Humer, E.; Probst, T. Comparing Mental Health During the COVID-19 Lockdown and 6 Months After the Lockdown in Austria: A Longitudinal Study. Front. Psychiatry 2021, 12, 625973. [Google Scholar] [CrossRef]
- Dale, R.; Budimir, S.; Probst, T.; Stippl, P.; Pieh, C. Mental health during the COVID-19 lockdown over the christmas period in Austria and the effects of sociodemographic and lifestyle factors. Int. J. Environ. Res. Public Health 2021, 18, 3679. [Google Scholar] [CrossRef] [PubMed]
- Pieh, C.; Probst, T.; Budimir, S.; Humer, E. Diminished well-being persists beyond the end of the COVID-19 lockdown. Gen. Hosp. Psychiatry 2021, 70, 137–138. [Google Scholar] [CrossRef] [PubMed]
- Pieh, C.; Budimir, S.; Probst, T. The effect of age, gender, income, work, and physical activity on mental health during coronavirus disease (COVID-19) lockdown in Austria. J. Psychosom. Res. 2020, 136, 110186. [Google Scholar] [CrossRef]
- Humer, E.; Schaffler, Y.; Jesser, A.; Probst, T.; Pieh, C. Mental health in the Austrian general population during COVID-19: Cross-sectional study on the association with sociodemographic factors. Front. Psychiatry 2022, 13, 943303. [Google Scholar] [CrossRef]
- Racine, N.; McArthur, B.A.; Cooke, J.E.; Eirich, R.; Zhu, J.; Madigan, S. Global prevalence of depressive and anxiety symptoms in children and adolescents during COVID-19: A meta-analysis. JAMA Pediatr. 2021, 175, 1142–1150. [Google Scholar] [CrossRef] [PubMed]
- Viner, R.; Russell, S.; Saulle, R.; Croker, H.; Stansfield, C.; Packer, J.; Nicholls, D.; Goddings, A.-L.; Bonell, C.; Hudson, L.; et al. School closures during social lockdown and mental health, health behaviors, and well-being among children and adolescents during the first COVID-19 wave: A systematic review. JAMA Pediatr. 2022, 176, 400–409. [Google Scholar] [CrossRef]
- Jesser, A.; Schaffler, Y.; Gachter, A.; Dale, R.; Humer, E.; Pieh, C. School students’ concerns and support after one year of COVID-19 in Austria: A qualitative study using content analysis. Healthcare 2022, 10, 1334. [Google Scholar] [CrossRef]
- Haider, K.; Humer, E.; Pieh, C.; Plener, P.L.; Jesser, A. Burdens of apprentices caused by the COVID-19 pandemic and how they deal with them: A qualitative study using content analysis one-year post-breakout. Healthcare 2022, 10, 2206. [Google Scholar] [CrossRef]
- ORF.at. Schulschließungen im OECD-Vergleich. Available online: https://orf.at/stories/3228781/ (accessed on 1 March 2023).
- Bock-Schappelwein, J.; Famira-Mühlberger, U. COVID-19-Bedingte Schulschliessungen: Ökonomische Herausforderungen für Kinder, Eltern, Unternehmen und Gesellschaft; ÖGB-Verlag: Vienna, Austria, 2021; pp. 77–86. [Google Scholar]
- Walcherberger, C.; Holl, F.; Pollak, M.; Kowarz, N.; Partheymüller, J. Chronologie zur Corona-Krise in Österreich—Teil 7: Der Delta-Lockdown, die Omikron-Welle und das “Frühlingserwachen”. Available online: https://viecer.univie.ac.at/corona-blog/corona-blog-beitraege/blog-150-chronologie-zur-corona-krise-in-oesterreich-teil-7-der-delta-lockdown-die-omikron-welle-und-das-fruehlingserwachen/ (accessed on 28 February 2023).
- Kaltschik, S.; Pieh, C.; Dale, R.; Probst, T.; Pammer, B.; Humer, E. Assessment of the long-term mental health effects on Austrian students after COVID-19 restrictions. Int. J. Environ. Res. Public Health 2022, 19, 13110. [Google Scholar] [CrossRef]
- Dale, R.; O’Rourke, T.; Humer, E.; Jesser, A.; Plener, P.L.; Pieh, C. Mental health of apprentices during the COVID-19 pandemic in Austria and the effect of gender, migration background, and work situation. Int. J. Environ. Res. Public Health 2021, 18, 8933. [Google Scholar] [CrossRef]
- Pieh, C.; Plener, P.L.; Probst, T.; Dale, R.; Humer, E. Assessment of Mental Health of High School Students During Social Distancing and Remote Schooling During the COVID-19 Pandemic in Austria. JAMA Netw. Open 2021, 4, e2114866. [Google Scholar] [CrossRef] [PubMed]
- Sheffield, J.K.; Fiorenza, E.; Sofronoff, K. Adolescents’ willingness to seek psychological help: Promoting and preventing factors. J. Youth Adolesc. 2004, 33, 495–507. [Google Scholar] [CrossRef]
- Schaffler, Y.; Probst, T.; Jesser, A.; Humer, E.; Pieh, C.; Stippl, P.; Haid, B.; Schigl, B. Perceived barriers and facilitators to psychotherapy utilisation and how they relate to patient’s psychotherapeutic goals. Healthcare 2022, 10, 2228. [Google Scholar] [CrossRef] [PubMed]
- Galdas, P.M.; Cheater, F.; Marshall, P. Men and health help-seeking behaviour: Literature review. J. Adv. Nurs. 2005, 49, 616–623. [Google Scholar] [CrossRef] [PubMed]
- Creswell, J.W.; Plano Clark, V.L. Designing and Conducting Mixed Methods Research; Sage: Thousand Oaks, CA, USA, 2007; pp. 1–275. [Google Scholar]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap). A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Richardson, L.P.; McCauley, E.; Grossman, D.C.; McCarty, C.A.; Richards, J.; Russo, J.E.; Rockhill, C.; Katon, W. Evaluation of the Patient Health Questionnaire-9 Item for detecting major depression among adolescents. Pediatrics 2010, 126, 1117–1123. [Google Scholar] [CrossRef]
- Löwe, B.; Spitzer, R.L.; Gräfe, K.; Kroenke, K.; Quenter, A.; Zipfel, S.; Buchholz, C.; Witte, S.; Herzog, W. Comparative validity of three screening questionnaires for DSM-IV depressive disorders and physicians’ diagnoses. J. Affect. Disord. 2004, 78, 131–140. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef]
- Löwe, B.; Decker, O.; Müller, S.; Brähler, E.; Schellberg, D.; Herzog, W.; Herzberg, P.Y. Validation and standardization of the Generalized Anxiety Disorder Screener (GAD-7) in the general population. Med. Care 2008, 46, 266–274. [Google Scholar] [CrossRef] [PubMed]
- Mossman, S.A.; Luft, M.J.; Schroeder, H.K.; Varney, S.T.; Fleck, D.E.; Barzman, D.H.; Gilman, R.; DelBello, M.P.; Strawn, J.R. The Generalized Anxiety Disorder 7-item scale in adolescents with generalized anxiety disorder: Signal detection and validation. Ann. Clin. Psychiatry 2017, 29, 227–234a. [Google Scholar] [PubMed]
- Gerber, M.; Lang, C.; Lemola, S.; Colledge, F.; Kalak, N.; Holsboer-Trachsler, E.; Pühse, U.; Brand, S. Validation of the German version of the Insomnia Severity Index in adolescents, young adults and adult workers: Results from three cross-sectional studies. BMC Psychiatry 2016, 16, 174. [Google Scholar] [CrossRef] [PubMed]
- Morin, C.M.; Belleville, G.; Bélanger, L.; Ivers, H. The Insomnia Severity Index: Psychometric indicators to detect insomnia cases and evaluate treatment response. Sleep 2011, 34, 601–608. [Google Scholar] [CrossRef]
- Klein, E.M.; Brähler, E.; Dreier, M.; Reinecke, L.; Müller, K.W.; Schmutzer, G.; Wölfling, K.; Beutel, M.E. The German version of the Perceived Stress Scale—Psychometric characteristics in a representative German community sample. BMC Psychiatry 2016, 16, 159. [Google Scholar] [CrossRef]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of Perceived Stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Morgan, J.F.; Reid, F.; Lacey, J.H. The SCOFF questionnaire: Assessment of a new screening tool for eating disorders. BMJ 1999, 319, 1467–1468. [Google Scholar] [CrossRef]
- Richter, F.; Strauss, B.; Braehler, E.; Adametz, L.; Berger, U. Screening disordered eating in a representative sample of the German population: Usefulness and psychometric properties of the German SCOFF questionnaire. Eat. Behav. 2017, 25, 81–88. [Google Scholar] [CrossRef]
- Ewing, J.A. Detecting alcoholism: The CAGE Questionnaire. JAMA 1984, 252, 1905–1907. [Google Scholar] [CrossRef]
- Williams, N. The CAGE questionnaire. Occup. Med. 2014, 64, 473–474. [Google Scholar] [CrossRef]
- ATLAS.ti Scientific Software Development GmbH. ATLAS.ti 22 Windows; ATLAS.ti Scientific Software Development GmbH: Berlin, Germany, 2022. [Google Scholar]
- Dale, R.; Jesser, A.; Pieh, C.; O’Rourke, T.; Probst, T.; Humer, E. Mental health burden of high school students, and suggestions for psychosocial support, 1.5 years into the COVID-19 pandemic in Austria. Eur. Child Adolesc. Psychiatry 2022. [Google Scholar] [CrossRef] [PubMed]
- Felder-Puig, R.; Teufl, L. Die Psychische Gesundheit Österreichischer Schülerinnen und Schüler: HBSC-Factsheet 01: Ergebnisse der HBSC-Studie 2018.; Bundesministerium für Arbeit, Soziales, Gesundheit und Konsumentschutz: Vienna, Austria, 2019. [Google Scholar]
- Jesser, A.; Schmalwieser, S.; Mädge, A.-L.; Culen, C.; Schrank, B.; Böckle, M. Chancen niederschwelliger online Peer-to-Peer Begleitung für Jugendliche am Beispiel der Online-Plattform OPEN. Psychother. Forum 2021, 25, 154–160. [Google Scholar] [CrossRef]
- Kurier. Psychotherapeuten Wollen Regelmäßig an Die Schulen; Kurier: Vienna, Austria, 2021. [Google Scholar]
- Kinder- und Jugendanwaltschaft Österreichs. Recht auf Psychische Gesundheit: Verbesserung der Psychosozialen und Psychotherapeutischen Versorgung für Kinder und Jugendliche; Kinder- und Jugendanwaltschaft Österreichs: Vienna, Austria, 2022. [Google Scholar]
- Österreichische Liga für Kinder- und Jugendgesundheit. Bericht zur Lage der Kinder- und Jugendgesundheit in Österreich 2019; Österreichische Liga für Kinder- und Jugendgesundheit: Vienna, Austria, 2019. [Google Scholar]
- Fliedl, R.; Ecker, B.; Karwautz, A. Kinder- und jugendpsychiatrische Versorgung 2019 in Österreich—Stufen der Versorgung, Ist-Stand und Ausblick. Neuropsychiatrie 2020, 34, 179–188. [Google Scholar] [CrossRef] [PubMed]
- Wagner, G.; Zeiler, M.; Waldherr, K.; Philipp, J.; Truttmann, S.; Dür, W.; Treasure, J.L.; Karwautz, A.F.K. Mental health problems in Austrian adolescents: A nationwide, two-stage epidemiological study applying DSM-5 criteria. Eur. Child Adolesc. Psychiatry 2017, 26, 1483–1499. [Google Scholar] [CrossRef]
- Grassl, R.; Marte, E. Unterversorgung mit Kinder- und jugendpsychiatrischen Fachambulatorien in Österreich, die Mindestanforderungen erfüllen können. Neuropsychiatrie 2022, 36, 165–172. [Google Scholar] [CrossRef]
- Thun-Hohenstein, L. Kinder- und Jugendpsychiatrische Versorgung in Österreich—Ein Update. In Kinder und Jugendliche im besten Gesundheitssystem der Welt; Springer: Vienna, Austria, 2011; pp. 83–90. [Google Scholar]
- Plener, P.L.; Klier, C.M.; Thun-Hohenstein, L.; Sevecke, K. Psychische Versorgung von Kindern und Jugendlichen in Österreich neu aufstellen: Dringender Handlungsbedarf besteht JETZT! Neuropsychiatrie 2021, 35, 213–215. [Google Scholar] [CrossRef]
- Koubek, D.; Krönke, H.; Karwautz, A. Die aktuelle Situation der kinder- und jugendpsychiatrischen Versorgung in Österreich im niedergelassenen Bereich. Neuropsychiatrie 2022, 36, 160–164. [Google Scholar] [CrossRef]
- Österreichischer Berufsverband für Psychotherapie. Berufspolitik. Stand der Psychotherapie in Österreich. Available online: https://www.psychotherapie.at/oebvp/berufspolitik (accessed on 13 December 2022).
- Burgenland.ORF.at. Psychotherapie auf Krankenschein: Lange Wartezeiten. Available online: https://burgenland.orf.at/stories/3123255/ (accessed on 13 December 2022).
- Brühl, U. Kinderliga Warnt vor Blackout in der Psychotherapie; Kurier: Vienna, Austria, 2022. [Google Scholar]
- Österreichischer Berufsverband für Psychotherapie. PsychotherapeutInnen mit Weiterbildung in Säuglings-, Kinder und Jugendlichenpsychotherapie. Available online: https://www.psychotherapie.at/skj-pt (accessed on 13 December 2022).
- Magson, N.R.; Freeman, J.Y.A.; Rapee, R.M.; Richardson, C.E.; Oar, E.L.; Fardouly, J. Risk and protective factors for prospective changes in adolescent mental health during the COVID-19 pandemic. J. Youth Adolesc. 2021, 50, 44–57. [Google Scholar] [CrossRef]
- Mendolia, S.; Suziedelyte, A.; Zhu, A. Have girls been left behind during the COVID-19 pandemic? Gender differences in pandemic effects on children’s mental wellbeing. Econ. Lett. 2022, 214, 110458. [Google Scholar] [CrossRef]
- Halldorsdottir, T.; Thorisdottir, I.E.; Meyers, C.C.A.; Asgeirsdottir, B.B.; Kristjansson, A.L.; Valdimarsdottir, H.B.; Allegrante, J.P.; Sigfusdottir, I.D. Adolescent well-being amid the COVID-19 pandemic: Are girls struggling more than boys? JCPP Adv. 2021, 1, e12027. [Google Scholar] [CrossRef]
- Chen, F.; Zheng, D.; Liu, J.; Gong, Y.; Guan, Z.; Lou, D. Depression and anxiety among adolescents during COVID-19: A cross-sectional study. Brain Behav. Immun. 2020, 88, 36–38. [Google Scholar] [CrossRef] [PubMed]
- Kapetanovic, S.; Gurdal, S.; Ander, B.; Sorbring, E. Reported changes in adolescent psychosocial functioning during the COVID-19 outbreak. Adolescents 2021, 1, 10–20. [Google Scholar] [CrossRef]
- Thorisdottir, I.E.; Asgeirsdottir, B.B.; Kristjansson, A.L.; Valdimarsdottir, H.B.; Jonsdottir Tolgyes, E.M.; Sigfusson, J.; Allegrante, J.P.; Sigfusdottir, I.D.; Halldorsdottir, T. Depressive symptoms, mental wellbeing, and substance use among adolescents before and during the COVID-19 pandemic in Iceland: A longitudinal, population-based study. Lancet Psychiatry 2021, 8, 663–672. [Google Scholar] [CrossRef]
- Zhou, S.J.; Zhang, L.G.; Wang, L.L.; Guo, Z.C.; Wang, J.Q.; Chen, J.C.; Liu, M.; Chen, X.; Chen, J.X. Prevalence and socio-demographic correlates of psychological health problems in Chinese adolescents during the outbreak of COVID-19. Eur. Child Adolesc. Psychiatry 2020, 29, 749–758. [Google Scholar] [CrossRef]
- Cusack, J.; Deane, F.P.; Wilson, C.J.; Ciarrochi, J. Emotional expression, perceptions of therapy, and help-seeking intentions in men attending therapy services. Psychol. Men Masc. 2006, 7, 69–82. [Google Scholar] [CrossRef]
- Hale, S.; Grogan, S.; Willott, S. Male GPs’ views on men seeking medical help: A qualitative study. Br. J. Health Psychol. 2010, 15, 697–713. [Google Scholar] [CrossRef]
- McCusker, M.G.; Galupo, M.P. The impact of men seeking help for depression on perceptions of masculine and feminine characteristics. Psychol. Men Masc. 2011, 12, 275–284. [Google Scholar] [CrossRef]
- Möller-Leimkühler, A.M. Barriers to help-seeking by men: A review of sociocultural and clinical literature with particular reference to depression. J. Affect. Disord. 2002, 71, 1–9. [Google Scholar] [CrossRef]
- Yousaf, O.; Grunfeld, E.A.; Hunter, M.S. A systematic review of the factors associated with delays in medical and psychological help-seeking among men. Health Psychol. Rev. 2015, 9, 264–276. [Google Scholar] [CrossRef] [PubMed]
- Blazina, C.; Watkins Jr, C.E. Masculine gender role conflict: Effects on college men’s psychological well-being, chemical substance usage, and attitudes towards help-seeking. J. Couns. Psychol. 1996, 43, 461–465. [Google Scholar] [CrossRef]
- Chan, R.K.; Hayashi, K. Gender roles and help-seeking behaviour: Promoting professional help among Japanese men. J. Soc. Work. 2010, 10, 243–262. [Google Scholar] [CrossRef]
- Good, G.E.; Dell, D.M.; Mintz, L.B. Male role and gender role conflict: Relations to help seeking in men. J. Couns. Psychol. 1989, 36, 295–300. [Google Scholar] [CrossRef]
- Johnson, J.L.; Oliffe, J.L.; Kelly, M.T.; Galdas, P.; Ogrodniczuk, J.S. Men’s discourses of help-seeking in the context of depression. Sociol. Health Illn. 2012, 34, 345–361. [Google Scholar] [CrossRef] [PubMed]
- Mansfield, A.K.; Addis, M.E.; Courtenay, W. Measurement of men’s help seeking: Development and evaluation of the barriers to help seeking scale. Psychol. Men Masc. 2005, 6, 95–108. [Google Scholar] [CrossRef]
- O’Brien, R.; Hunt, K.; Hart, G. ‘It’s caveman stuff, but that is to a certain extent how guys still operate’: Men’s accounts of masculinity and help seeking. Soc. Sci. Med. 2005, 61, 503–516. [Google Scholar] [CrossRef]
- Pederson, E.L.; Vogel, D.L. Male gender role conflict and willingness to seek counseling: Testing a mediation model on college-aged men. J. Couns. Psychol. 2007, 54, 373–384. [Google Scholar] [CrossRef]
- Rochlen, A.B.; Paterniti, D.A.; Epstein, R.M.; Duberstein, P.; Willeford, L.; Kravitz, R.L. Barriers in diagnosing and treating men with depression: A focus group report. Am. J. Men’s Health 2010, 4, 167–175. [Google Scholar] [CrossRef]
- Steinfeldt, J.A.; Steinfeldt, M.C. Gender role conflict, athletic identity, and help-seeking among high school football players. J. Appl. Sport Psychol. 2010, 22, 262–273. [Google Scholar] [CrossRef]
- Coles, R.; Watkins, F.; Swami, V.; Jones, S.; Woolf, S.; Stanistreet, D. What men really want: A qualitative investigation of men’s health needs from the Halton and St Helens Primary Care Trust men’s health promotion project. Br. J. Health Psychol. 2010, 15, 921–939. [Google Scholar] [CrossRef]
- Smith, J.A.; Braunack-Mayer, A.; Wittert, G.; Warin, M. “I’ve been independent for so damn long!”: Independence, masculinity and aging in a help seeking context. J. Aging Stud. 2007, 21, 325–335. [Google Scholar] [CrossRef]
- Noone, J.H.; Stephens, C. Men, masculine identities, and health care utilisation. Sociol. Health Illn. 2008, 30, 711–725. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.A.; Braunack-Mayer, A.; Wittert, G.; Warin, M. “It’s sort of like being a detective”: Understanding how Australian men self-monitor their health prior to seeking help. BMC Health Serv. Res. 2008, 8, 56. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.A.; Braunack-Mayer, A.J.; Wittert, G.A.; Warin, M.J. Qualities men value when communicating with general practitioners: Implications for primary care settings. Med. J. Aust. 2008, 189, 618–621. [Google Scholar] [CrossRef] [PubMed]
- Akey, J.E.; Rintamaki, L.S.; Kane, T.L. Health Belief Model deterrents of social support seeking among people coping with eating disorders. J. Affect. Disord. 2013, 145, 246–252. [Google Scholar] [CrossRef]
- Leavey, G.; Vallianatou, C.; Johnson-Sabine, E.; Rae, S.; Gunputh, V. Psychosocial barriers to engagement with an eating disorder service: A qualitative analysis of failure to attend. Eat. Disord. 2011, 19, 425–440. [Google Scholar] [CrossRef]
- Mond, J.M.; Hay, P.J.; Paxton, S.J.; Rodgers, B.; Darby, A.; Nillson, J.; Quirk, F.; Owen, C. Eating disorders “mental health literacy” in low risk, high risk and symptomatic women: Implications for health promotion programs. Eat. Disord. 2010, 18, 267–285. [Google Scholar] [CrossRef]
- Becker, A.E.; Franko, D.L.; Nussbaum, K.; Herzog, D.B. Secondary prevention for eating disorders: The impact of education, screening, and referral in a college-based screening program. Int. J. Eat. Disord. 2004, 36, 157–162. [Google Scholar] [CrossRef]
- Gulliksen, K.S.; Nordbø, R.H.S.; Espeset, E.M.S.; Skårderud, F.; Holte, A. The process of help-seeking in anorexia nervosa: Patients’ perspective of first contact with health services. Eat. Disord. 2015, 23, 206–222. [Google Scholar] [CrossRef]
- Reyes-Rodríguez, M.L.; Ramírez, J.; Davis, K.; Patrice, K.; Bulik, C.M. Exploring barriers and facilitators in eating disorders treatment among Latinas in the United States. J. Lat. Psychol. 2013, 1, 112–131. [Google Scholar] [CrossRef]
- Roehrig, J.P.; McLean, C.P. A comparison of stigma toward eating disorders versus depression. Int. J. Eat. Disord. 2010, 43, 671–674. [Google Scholar] [CrossRef]
- Becker, A.E.; Hadley Arrindell, A.; Perloe, A.; Fay, K.; Striegel-Moore, R.H. A qualitative study of perceived social barriers to care for eating disorders: Perspectives from ethnically diverse health care consumers. Int. J. Eat. Disord. 2010, 43, 633–647. [Google Scholar] [CrossRef] [PubMed]
- Ali, K.; Farrer, L.; Fassnacht, D.B.; Gulliver, A.; Bauer, S.; Griffiths, K.M. Perceived barriers and facilitators towards help-seeking for eating disorders: A systematic review. Int. J. Eat. Disord. 2017, 50, 9–21. [Google Scholar] [CrossRef] [PubMed]
- Hepworth, N.; Paxton, S.J. Pathways to help-seeking in bulimia nervosa and binge eating problems: A concept mapping approach. Int. J. Eat. Disord. 2007, 40, 493–504. [Google Scholar] [CrossRef] [PubMed]
- Tavolacci, M.-P.; Déchelotte, P.; Ladner, J. Eating disorders among college students in France: Characteristics, help-and care-seeking. Int. J. Environ. Res. Public Health 2020, 17, 5914. [Google Scholar] [CrossRef]
- Böhme, M.; Thomas, V. Beratung zwischen Tür und Angel: Das unterschätzte Ehrenamt der Vertrauenslehrer: Innen. In Entwicklungen im Lehramt für Gesundheit und Pflege: Ergebnisse Qualitativer Forschung; Mabuse-Verlag: Frankfurt, Germany, 2022; pp. 174–179. [Google Scholar]
- Solomon, P. Peer support/peer provided services underlying processes, benefits, and critical ingredients. Psychiatr. Rehabil. J. 2004, 27, 392–401. [Google Scholar] [CrossRef] [PubMed]
- Savage, H.; Murray, J.; Hatch, S.L.; Hotopf, M.; Evans-Lacko, S.; Brown, J.S. Exploring professional help-seeking for mental disorders. Qual. Health Res. 2016, 26, 1662–1673. [Google Scholar] [CrossRef]
- Brown, J.; Evans-Lacko, S.; Aschan, L.; Henderson, M.J.; Hatch, S.L.; Hotopf, M. Seeking informal and formal help for mental health problems in the community: A secondary analysis from a psychiatric morbidity survey in South London. BMC Psychiatry 2014, 14, 275. [Google Scholar] [CrossRef]
- Byrom, N. An evaluation of a peer support intervention for student mental health. J. Ment. Health 2018, 27, 240–246. [Google Scholar] [CrossRef]


{kind=link}
| Gender | Age | ||||||
|---|---|---|---|---|---|---|---|
| Female | Male | Diverse | Statistics | 14–17 Years | 18–20 Years | Statistics | |
| N | 477 | 122 | 17 | 439 | 177 | ||
| Depression, % | 72.7% | 45.1% | 94.1% | χ²(2;616) = 39.616; | 66.5% | 71.2% | χ²(1;616) = 1.262; |
| (n) | 347 | 55 | 16 | p < 0.001 | 292 | 126 | p = 0.261 |
| Anxiety, % | 57.0% | 35.2% | 70.6% | χ²(2;616) = 20.106; | 51.3% | 62.7% | χ²(1;616) = 6.681; |
| (n) | 279 | 45 | 12 | p < 0.001 | 225 | 111 | p = 0.010 |
| Insomnia, % | 33.5% | 20.5% | 41.2% | χ²(2;616) = 8.530; | 28.7% | 37.3% | χ²(1;616) = 4.335; |
| (n) | 160 | 25 | 7 | p = 0.014 | 126 | 66 | p = 0.037 |
| High Stress, % | 43.4% | 22.1% | 64.7% | χ²(2;616) = 22.877; | 40.3% | 38.4% | χ²(1;616) = 0.190; |
| (n) | 207 | 27 | 11 | p < 0.001 | 177 | 68 | p = 0.663 |
| Disordered Eating, % | 56.9% | 32.2% | 43.8% | χ²(2;608) = 23.869; | 52.4% | 47.5% | χ²(1;608) = 1.307; |
| (n) | 268 | 39 | 7 | p < 0.001 | 230 | 84 | p = 0.235 |
| Alcohol Abuse, % | 16.8% | 21.5% | 11.8% | χ²(2;615) = 1.889; | 16.2% | 20.9% | χ²(1;615) = 1.918; |
| (n) | 80 | 26 | 2 | p = 0.389 | 71 | 37 | p = 0.166 |
| Male-Divers | Female-Divers | Female-Male | ||||
|---|---|---|---|---|---|---|
| χ² | p | χ² | p | χ² | p | |
| Depression (PHQ-9) | 14.358 | <0.001 | 3.848 | 0.050 | 33.686 | <0.001 |
| Anxiety (GAD-7) | 7.006 | 0.008 | 0.992 | 0.319 | 18.262 | <0.001 |
| Insomnia (ISI) | 3.602 | 0.058 | 0.427 | 0.513 | 7.752 | 0.005 |
| Eating Disorders (SCOFF) | 0.841 | 0.359 | 1.089 | 0.297 | 23.466 | <0.001 |
| High Stress (PSS-10) | 13.615 | <0.001 | 3.023 | 0.082 | 18.456 | <0.001 |
| Support Wish | Professional Help | Someone to Talk to | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Yes, % | n | Statistics | Yes, % | n | Statistics | Yes, % | n | Statistics | |
| Gender | χ²(2;606) = 22.479 p < 0.001 | χ²(2;616) = 4.290 p = 0.117 | Fisher’s Exact Test p = 0.115 | ||||||
| Female | 51.4% | 241 | 21.4% | 102 | 11.9% | 57 | |||
| Male | 28.9% | 35 | 13.9% | 17 | 5.70% | 7 | |||
| Diverse | 68.8% | 11 | 29.4% | 5 | 0.0% | 0 | |||
| Age | χ²(21;606) = 0.315 p = 0.575 | χ²(1;616) = 6.375 p = 0.012 | χ²(1;606) = 4.650 p = 0.031 | ||||||
| 14–17 years | 70.0% | 201 | 62.1% | 77 | 82.8% | 53 | |||
| 18–20 years | 30.0% | 86 | 37.9% | 47 | 17.2% | 11 | |||
| Depression (PHQ-9) | χ²(1;606) = 50.415 p < 0.001 | χ²(1;616) = 14.762 p < 0.001 | χ²(1;616) = 0.529 p = 0.467 | ||||||
| Below cut-off | 26.5% | 52 | 11.1% | 22 | 9.1% | 18 | |||
| Above cut-off | 57.3% | 235 | 24.4% | 102 | 11.0% | 46 | |||
| Anxiety (GAD-7) | χ²(1;606) = 44.406 p < 0.001 | χ²(1;606) = 32.763 p < 0.001 | χ²(1;616) = 0.256 p = 0.613 | ||||||
| Below cut-off | 32.5% | 89 | 10.0% | 28 | 11.1% | 31 | |||
| Above cut-off | 59.6% | 198 | 28.6% | 96 | 9.8% | 33 | |||
| Insomnia (ISI) | χ²(1;606) = 10.544 p = 0.001 | χ²(1;616) = 2.543 p = 0.111 | χ²(1;616) < 0.001 p = 0.988 | ||||||
| Below cut-off | 42.9% | 179 | 18.4% | 78 | 10.4% | 44 | |||
| Above cut-off | 57.1% | 108 | 24.0% | 46 | 10.4% | 20 | |||
| Eating Disorders (SCOFF) | χ²(1;606) = 14.968 p < 0.001 | χ²(1;608) = 0.998 p = 0.318 | χ²(1;608) = 4.417 p = 0.036 | ||||||
| Below cut-off | 39.2% | 115 | 18.7% | 55 | 7.8% | 23 | |||
| Above cut-off | 55.0% | 172 | 22.0% | 69 | 13.1% | 41 | |||
| High Stress (PSS) | χ²(1;606) = 61.971 p < 0.001 | χ²(1;616) = 32.300 p < 0.001 | χ²(1;616) = 0.915 p = 0.339 | ||||||
| Below cut-off | 34.3% | 125 | 12.7% | 47 | 9.4% | 35 | |||
| Above cut-off | 66.9% | 162 | 31.4% | 77 | 11.8% | 29 | |||
| Alcohol Abuse (CAGE) | χ²(1;606) = 2.443 p = 0.118 | χ²(1;615) = 3.642 p = 0.064 | χ²(1;615) = 0.374 p = 0.541 | ||||||
| Below cut-off | 45.9% | 229 | 18.7% | 95 | 10.1% | 51 | |||
| Above cut-off | 54.2% | 58 | 26.9% | 29 | 12.0% | 13 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haider, K.; Humer, E.; Weber, M.; Pieh, C.; Ghorab, T.; Dale, R.; Dinhof, C.; Gächter, A.; Probst, T.; Jesser, A. An Assessment of Austrian School Students’ Mental Health and Their Wish for Support: A Mixed Methods Approach. Int. J. Environ. Res. Public Health 2023, 20, 4749. https://doi.org/10.3390/ijerph20064749
Haider K, Humer E, Weber M, Pieh C, Ghorab T, Dale R, Dinhof C, Gächter A, Probst T, Jesser A. An Assessment of Austrian School Students’ Mental Health and Their Wish for Support: A Mixed Methods Approach. International Journal of Environmental Research and Public Health. 2023; 20(6):4749. https://doi.org/10.3390/ijerph20064749
Chicago/Turabian StyleHaider, Katja, Elke Humer, Magdalena Weber, Christoph Pieh, Tiam Ghorab, Rachel Dale, Carina Dinhof, Afsaneh Gächter, Thomas Probst, and Andrea Jesser. 2023. "An Assessment of Austrian School Students’ Mental Health and Their Wish for Support: A Mixed Methods Approach" International Journal of Environmental Research and Public Health 20, no. 6: 4749. https://doi.org/10.3390/ijerph20064749
APA StyleHaider, K., Humer, E., Weber, M., Pieh, C., Ghorab, T., Dale, R., Dinhof, C., Gächter, A., Probst, T., & Jesser, A. (2023). An Assessment of Austrian School Students’ Mental Health and Their Wish for Support: A Mixed Methods Approach. International Journal of Environmental Research and Public Health, 20(6), 4749. https://doi.org/10.3390/ijerph20064749