
Association between Periodontal Disease and Cognitive Impairment in Adults

 , ,
, ,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Search Strategy
2.3. Selection Criteria
2.4. Data Extraction and Synthesis
2.5. Methodological Quality Assessment
3. Results
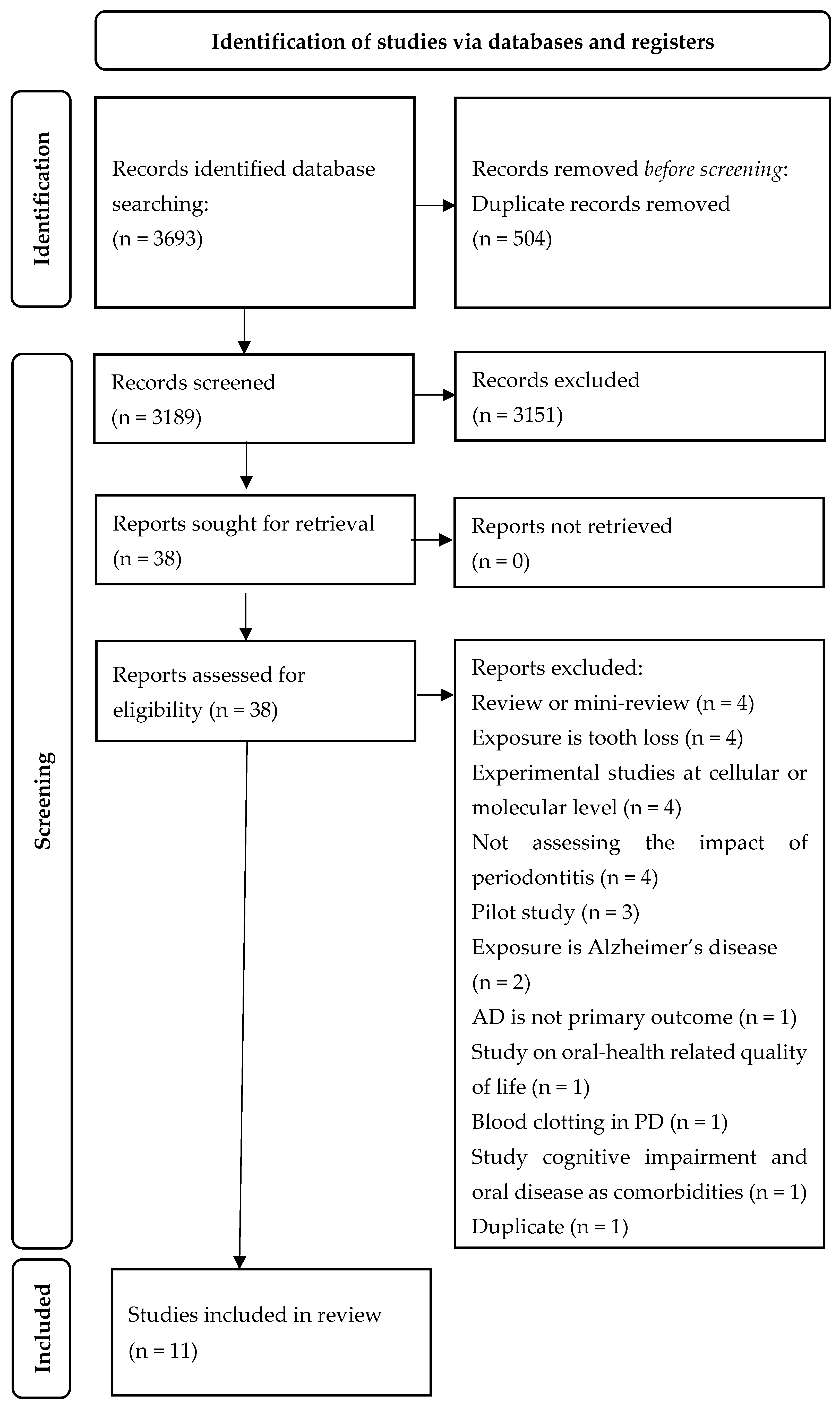
3.1. Study Selection
3.2. Study Characteristics
3.3. Risk of Bias in Studies
3.4. Association between Chronic Periodontitis and Cognitive Impairment
3.4.1. Association between Chronic Periodontitis According to Its International Classifications and Cognitive Impairment
3.4.2. Association between Chronic Periodontitis According to Its Clinical Measurement and Cognitive Impairment
3.4.3. Association between Periodontitis Induced Inflammatory Biomarkers and Cognitive Impairment
3.4.4. Association between Serological Marker (IgG) of Periodontitis and Cognitive Impairment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Löe, H.; Anerud, A.; Boysen, H.; Morrison, E. Natural History of Periodontal Disease in Man. J. Clin. Periodontol. 1986, 13, 431–440. [Google Scholar] [CrossRef]
- Hajishengallis, G.; Darveau, R.P.; Curtis, M.A. The Keystone-Pathogen Hypothesis. Nat. Rev. Microbiol. 2012, 10, 717–725. [Google Scholar] [CrossRef]
- Wilson, J.J.; Burgess, R.; Mao, Y.-Q.; Luo, S.; Tang, H.; Jones, V.S.; Weisheng, B.; Huang, R.-Y.; Chen, X.; Huang, R.-P. Chapter Seven—Antibody Arrays in Biomarker Discovery. In Advances in Clinical Chemistry; Makowski, G.S., Ed.; Elsevier: Amsterdam, The Netherlands, 2015; Volume 69, pp. 255–324. ISBN 0065-2423. [Google Scholar]
- Haffajee, A.D.; Socransky, S.S.; Dzink, J.L.; Taubman, M.A.; Ebersole, J.L.; Smith, D.J. Clinical, Microbiological and Immunological Features of Subjects with Destructive Periodontal Diseases. J. Clin. Periodontol. 1988, 15, 240–246. [Google Scholar] [CrossRef]
- Position Paper: Epidemiology of Periodontal Diseases. J. Periodontol. 2005, 76, 1406–1419. [CrossRef]
- Carrizales-Sepúlveda, E.F.; Ordaz-Farías, A.; Vera-Pineda, R.; Flores-Ramírez, R. Periodontal Disease, Systemic Inflammation and the Risk of Cardiovascular Disease. Heart Lung Circ. 2018, 27, 1327–1334. [Google Scholar] [CrossRef]
- González-Sanmiguel, J.; Schuh, C.M.A.P.; Muñoz-Montesino, C.; Contreras-Kallens, P.; Aguayo, L.G.; Aguayo, S. Complex Interaction between Resident Microbiota and Misfolded Proteins: Role in Neuroinflammation and Neurodegeneration. Cells 2020, 9, 2476. [Google Scholar] [CrossRef]
- Kovacs, G.G. Chapter 21—Concepts and Classification of Neurodegenerative Diseases. In Handbook of Clinical Neurology; Kovacs, G.G., Alafuzoff, I., Eds.; Elsevier: Amsterdam, The Netherlands, 2018; Volume 145, pp. 301–307. ISBN 0072-9752. [Google Scholar]
- Bartus Raymond, T.; Dean Reginald, L.; Bernard, B.; Lippa Arnold, S. The Cholinergic Hypothesis of Geriatric Memory Dysfunction. Science 1982, 217, 408–414. [Google Scholar] [CrossRef]
- Hardy, J.; Allsop, D. Amyloid Deposition as the Central Event in the Aetiology of Alzheimer’s Disease. Trends Pharmacol. Sci. 1991, 12, 383–388. [Google Scholar] [CrossRef]
- Krstic, D.; Knuesel, I. Deciphering the Mechanism Underlying Late-Onset Alzheimer Disease. Nat. Rev. Neurol. 2013, 9, 25–34. [Google Scholar] [CrossRef]
- Alzheimer, A. Uber Eine Eigenartige Erkrankung Der Hirnrinde. Allgemeine. J. Psychiatry Forensic Med. -Phychish 1907, 64, 146–148. [Google Scholar]
- Miklossy, J. Emerging Roles of Pathogens in Alzheimer Disease. Expert Rev. Mol. Med. 2011, 13, e30. [Google Scholar] [CrossRef]
- He, W.; Goodkind, D.; Kowal, P.R. An Aging World: 2015; U.S. Census Bureau: Suitland, MD, USA, 2016.
- National Institutes of Health. Global Health and Aging; National Institutes of Health: Washington, DC, USA, 2018.
- Lin, R.-T.; Lai, C.-L.; Tai, C.-T.; Liu, C.-K.; Yen, Y.-Y.; Howng, S.-L. Prevalence and Subtypes of Dementia in Southern Taiwan: Impact of Age, Sex, Education, and Urbanization. J. Neurol. Sci. 1998, 160, 67–75. [Google Scholar] [CrossRef]
- Lindhe, J.; Ranney, R.; Lamster, I.; Charles, A.; Chung, C.-P.; Flemmig, T.; Kinane, D.; Listgarten, M.; Löe, H.; Schoor, R.; et al. Consensus Report: Chronic Periodontitis. Ann. Periodontol. 1999, 4, 38. [Google Scholar] [CrossRef]
- Hajishengallis, G. Immunomicrobial Pathogenesis of Periodontitis: Keystones, Pathobionts, and Host Response. Trends Immunol. 2014, 35, 3–11. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses; Ottawa Hospital Research Institute: Ottawa, ON, Canada, 2000. [Google Scholar]
- Anglin, R.E.S.; Samaan, Z.; Walter, S.D.; McDonald, S.D. Vitamin D Deficiency and Depression in Adults: Systematic Review and Meta-Analysis. Br. J. Psychiatry 2013, 202, 100–107. [Google Scholar] [CrossRef]
- Abou Abbas, L.; Salameh, P.; Nasser, W.; Nasser, Z.; Godin, I. Obesity and Symptoms of Depression among Adults in Selected Countries of the Middle East: A Systematic Review and Meta-Analysis. Clin. Obes. 2015, 5, 2–11. [Google Scholar] [CrossRef]
- Wang, J.-H.; Wu, Y.-J.; Tee, B.L.; Lo, R.Y. Medical Comorbidity in Alzheimer’s Disease: A Nested Case-Control Study. J. Alzheimer’s Dis. 2018, 63, 773–781. [Google Scholar] [CrossRef]
- Chen, C.K.; Wu, Y.T.; Chang, Y.C. Association between Chronic Periodontitis and the Risk of Alzheimer’s Disease: A Retrospective, Population-Based, Matched-Cohort Study. Alzheimers Res. Ther. 2017, 9, 1–7. [Google Scholar] [CrossRef]
- Choi, S.; Kim, K.; Chang, J.; Kim, S.M.; Kim, S.J.; Cho, H.J.; Park, S.M. Association of Chronic Periodontitis on Alzheimer’s Disease or Vascular Dementia. J. Am. Geriatr. Soc. 2019, 67, 1234–1239. [Google Scholar] [CrossRef]
- Demmer, R.T.; Norby, F.L.; Lakshminarayan, K.; Walker, K.A.; Pankow, J.S.; Folsom, A.R.; Mosley, T.; Beck, J.; Lutsey, P.L. Periodontal Disease and Incident Dementia The Atherosclerosis Risk in Communities Study (ARIC). Neurology 2020, 95, E1660–E1671. [Google Scholar] [CrossRef]
- Sparks Stein, P.; Steffen, M.J.; Smith, C.; Jicha, G.; Ebersole, J.L.; Abner, E.; Dawson, D. 3rd Serum Antibodies to Periodontal Pathogens Are a Risk Factor for Alzheimer’s Disease. Alzheimer’s Dement. J. Alzheimer’s Assoc. 2012, 8, 196–203. [Google Scholar] [CrossRef] [PubMed]
- Stewart, R.; Weyant, R.J.; Garcia, M.E.; Harris, T.; Launer, L.J.; Satterfield, S.; Sirnonsick, E.M.; Yaffe, K.; Newman, A.B. Adverse Oral Health and Cognitive Decline: The Health, Aging and Body Composition Study. J. Am. Geriatr. Soc. 2013, 61, 177–184. [Google Scholar] [CrossRef]
- Tzeng, N.S.; Chung, C.H.; Yeh, C.B.; Huang, R.Y.; Yuh, D.Y.; Huang, S.Y.; Lu, R.B.; Chang, H.A.; Kao, Y.C.; Chiang, W.S.; et al. Are Chronic Periodontitis and Gingivitis Associated with Dementia? A Nationwide, Retrospective, Matched-Cohort Study in Taiwan. Neuroepidemiology 2016, 47, 82–93. [Google Scholar] [CrossRef]
- Hategan, S.I.; Kamer, S.A.; Craig, R.G.; Sinescu, C.; de Leon, M.J.; Jianu, D.C.; Marian, C.; Bora, B.I.; Dan, T.F.; Birdac, C.D.; et al. Cognitive Dysfunction in Young Subjects with Periodontal Disease. Neurol. Sci. 2021, 1–9. [Google Scholar] [CrossRef]
- Kamer, A.R.; Morse, D.E.; Holm-Pedersen, P.; Mortensen, E.L.; Avlund, K. Periodontal Inflammation in Relation to Cognitive Function in an Older Adult Danish Population. J. Alzheimers Dis. 2012, 28, 613–624. [Google Scholar] [CrossRef]
- Noble, J.M.; Borrell, L.N.; Papapanou, P.N.; Elkind, M.S.V.; Scarmeas, N.; Wright, C.B. Periodontitis Is Associated with Cognitive Impairment among Older Adults: Analysis of NHANES-III. J. Neurol. Neurosurg. Psychiatry 2009, 80, 1206–1211. [Google Scholar] [CrossRef]
- Gil Montoya, J.A.; Barrios, R.; Sanchez-Lara, I.; Ramos, P.; Carnero, C.; Fornieles, F.; Montes, J.; Santana, S.; de Dios Luna, J.; Gonzalez-Moles, M.A. Systemic Inflammatory Impact of Periodontitis on Cognitive Impairment. Gerodontology 2020, 37, 11–18. [Google Scholar] [CrossRef]
- Shin, H.S.; Shin, M.S.; Ahn, Y.B.; Choi, B.Y.; Nam, J.H.; Kim, H.D. Periodontitis Is Associated with Cognitive Impairment in Elderly Koreans: Results from the Yangpyeong Cohort Study. J. Am. Geriatr. Soc. 2016, 64, 162–167. [Google Scholar] [CrossRef]
- Highfield, J. Diagnosis and Classification of Periodontal Disease. Aust. Dent. J. 2009, 54, S11–S26. [Google Scholar] [CrossRef]
- Mariotti, A.; Hefti, A.F. Defining Periodontal Health. BMC Oral Health 2015, 15 (Suppl. S1), S6. [Google Scholar] [CrossRef] [PubMed]
- Swardfager, W.; Lanctôt, K.; Rothenburg, L.; Wong, A.; Cappell, J.; Herrmann, N. A Meta-Analysis of Cytokines in Alzheimer’s Disease. Biol. Psychiatry 2010, 68, 930–941. [Google Scholar] [CrossRef]
- Anuradha, U.; Kumar, A.; Singh, R.K. The Clinical Correlation of Proinflammatory and Anti-Inflammatory Biomarkers with Alzheimer Disease: A Meta-Analysis. Neurol. Sci. 2022, 43, 285–298. [Google Scholar] [CrossRef]
- Park, J.-C.; Han, S.-H.; Mook-Jung, I. Peripheral Inflammatory Biomarkers in Alzheimer’s Disease: A Brief Review. BMB Rep. 2020, 53, 10. [Google Scholar] [CrossRef] [PubMed]
- Baruch, K.; Rosenzweig, N.; Kertser, A.; Deczkowska, A.; Sharif, A.M.; Spinrad, A.; Tsitsou-Kampeli, A.; Sarel, A.; Cahalon, L.; Schwartz, M. Breaking Immune Tolerance by Targeting Foxp3(+) Regulatory T Cells Mitigates Alzheimer’s Disease Pathology. Nat. Commun. 2015, 6, 7967. [Google Scholar] [CrossRef]
- Zheng, S.; Yu, S.; Fan, X.; Zhang, Y.; Sun, Y.; Lin, L.; Wang, H.; Pan, Y.; Li, C. Porphyromonas Gingivalis Survival Skills: Immune Evasion. J. Periodontal Res. 2021, 56, 1007–1018. [Google Scholar] [CrossRef]
- Hajishengallis, G.; Diaz, P.I. Porphyromonas Gingivalis: Immune Subversion Activities and Role in Periodontal Dysbiosis. Curr. Oral Health Rep. 2020, 7, 12–21. [Google Scholar] [CrossRef]
- Ho, M.-H.; Hasturk, H.; Young, D.F.; Xie, H. In Vivo and Ex Vivo Actions of a Novel P. Gingivalis Inhibitor on Multi-Species Biofilm, Inflammatory Response, and Periodontal Bone Loss. Mol. Oral Microbiol. 2020, 35, 193–201. [Google Scholar] [CrossRef]
- Olsen, I.; Taubman, M.A.; Singhrao, S.K. Porphyromonas Gingivalis Suppresses Adaptive Immunity in Periodontitis, Atherosclerosis, and Alzheimer’s Disease. J. Oral Microbiol. 2016, 8, 33029. [Google Scholar] [CrossRef]
- Baron, R.; Nemirovsky, A.; Harpaz, I.; Cohen, H.; Owens, T.; Monsonego, A. IFN-Gamma Enhances Neurogenesis in Wild-Type Mice and in a Mouse Model of Alzheimer’s Disease. FASEB J. Off. Publ. Fed. Am. Soc. Exp. Biol. 2008, 22, 2843–2852. [Google Scholar] [CrossRef]
- Pyrc, K.; Milewska, A.; Kantyka, T.; Sroka, A.; Maresz, K.; Kozieł, J.; Nguyen, K.-A.; Enghild, J.J.; Knudsen, A.D.; Potempa, J. Inactivation of Epidermal Growth Factor by Porphyromonas Gingivalis as a Potential Mechanism for Periodontal Tissue Damage. Infect. Immun. 2013, 81, 55–64. [Google Scholar] [CrossRef]
- Aw, J.; Scholz, G.M.; Huq, N.L.; Huynh, J.; O’Brien-Simpson, N.M.; Reynolds, E.C. Interplay between Porphyromonas Gingivalis and EGF Signalling in the Regulation of CXCL14. Cell. Microbiol. 2018, 20, e12837. [Google Scholar] [CrossRef]
- Thomas, R.; Morris, A.W.J.; Tai, L.M. Epidermal Growth Factor Prevents APOE4-Induced Cognitive and Cerebrovascular Deficits in Female Mice. Heliyon 2017, 3, e00319. [Google Scholar] [CrossRef]
- Thomas, R.; Zuchowska, P.; Morris, A.W.J.; Marottoli, F.M.; Sunny, S.; Deaton, R.; Gann, P.H.; Tai, L.M. Epidermal Growth Factor Prevents APOE4 and Amyloid-Beta-Induced Cognitive and Cerebrovascular Deficits in Female Mice. Acta Neuropathol. Commun. 2016, 4, 111. [Google Scholar] [CrossRef]
- Zaldua, S.; Damen, F.C.; Pisharody, R.; Thomas, R.; Fan, K.D.; Ekkurthi, G.K.; Scheinman, S.B.; Alahmadi, S.; Marottoli, F.M.; Alford, S.; et al. Epidermal Growth Factor Treatment of Female Mice That Express APOE4 at an Age of Advanced Pathology Mitigates Behavioral and Cerebrovascular Dysfunction. Heliyon 2020, 6, e03919. [Google Scholar] [CrossRef]
- Vaz, M.; Domingues, C.; Trindade, D.; Barra, C.; Oliveira, J.M.; Rosa, I.M.; da Cruz E Silva, O.A.B.; Henriques, A.G. IL-8 and MCP-1 Impact on Tau Phosphorylation and Phosphatase Activity. Curr. Alzheimer Res. 2020, 17, 985–1000. [Google Scholar] [CrossRef]
- Hu, W.T.; Howell, J.C.; Ozturk, T.; Gangishetti, U.; Kollhoff, A.L.; Hatcher-Martin, J.M.; Anderson, A.M.; Tyor, W.R. CSF Cytokines in Aging, Multiple Sclerosis, and Dementia. Front. Immunol. 2019, 10, 480. [Google Scholar] [CrossRef]
- Alsadany, M.A.; Shehata, H.H.; Mohamad, M.I.; Mahfouz, R.G. Histone Deacetylases Enzyme, Copper, and IL-8 Levels in Patients with Alzheimer’s Disease. Am. J. Alzheimer’s Dis. Other Dement. 2013, 28, 54–61. [Google Scholar] [CrossRef]
- Michlmayr, D.; McKimmie, C.S. Role of CXCL10 in Central Nervous System Inflammation. Int. J. Interferon Cytokine Mediat. Res. 2014, 6, 1. [Google Scholar]
- Bradburn, S.; McPhee, J.; Bagley, L.; Carroll, M.; Slevin, M.; Al-Shanti, N.; Barnouin, Y.; Hogrel, J.-Y.; Pääsuke, M.; Gapeyeva, H.; et al. Dysregulation of C-X-C Motif Ligand 10 during Aging and Association with Cognitive Performance. Neurobiol. Aging 2018, 63, 54–64. [Google Scholar] [CrossRef]
- Rocha, N.P.; Scalzo, P.L.; Barbosa, I.G.; Souza, M.S.; Morato, I.B.; Vieira, E.L.M.; Christo, P.P.; Teixeira, A.L.; Reis, H.J. Cognitive Status Correlates with CXCL10/IP-10 Levels in Parkinson’s Disease. Park. Dis. 2014, 2014, 903796. [Google Scholar] [CrossRef] [PubMed]
- Mohd Hasni, D.S.; Lim, S.M.; Chin, A.V.; Tan, M.P.; Poi, P.J.H.; Kamaruzzaman, S.B.; Majeed, A.B.A.; Ramasamy, K. Peripheral Cytokines, C-X-C Motif Ligand10 and Interleukin-13, Are Associated with Malaysian Alzheimer’s Disease. Geriatr. Gerontol. Int. 2017, 17, 839–846. [Google Scholar] [CrossRef] [PubMed]
- Dufour, J.H.; Dziejman, M.; Liu, M.T.; Leung, J.H.; Lane, T.E.; Luster, A.D. IFN-γ-Inducible Protein 10 (IP-10; CXCL10)-Deficient Mice Reveal a Role for IP-10 in Effector T Cell Generation and Trafficking. J. Immunol. 2002, 168, 3195–3204. [Google Scholar] [CrossRef]
- Jauregui, C.E.; Wang, Q.; Wright, C.J.; Takeuchi, H.; Uriarte, S.M.; Lamont, R.J. Suppression of T-Cell Chemokines by Porphyromonas Gingivalis. Infect. Immun. 2013, 81, 2288–2295. [Google Scholar] [CrossRef]
- Oido-Mori, M.; Rezzonico, R.; Wang, P.L.; Kowashi, Y.; Dayer, J.M.; Baehni, P.C.; Chizzolini, C. Porphyromonas Gingivalis Gingipain-R Enhances Interleukin-8 but Decreases Gamma Interferon-Inducible Protein 10 Production by Human Gingival Fibroblasts in Response to T-Cell Contact. Infect. Immun. 2001, 69, 4493–4501. [Google Scholar] [CrossRef]
- Ekhlassi, S.; Scruggs, L.Y.; Garza, T.; Montufar-Solis, D.; Moretti, A.J.; Klein, J.R. Porphyromonas Gingivalis Lipopolysaccharide Induces Tumor Necrosis Factor-Alpha and Interleukin-6 Secretion, and CCL25 Gene Expression, in Mouse Primary Gingival Cell Lines: Interleukin-6-Driven Activation of CCL2. J. Periodontal Res. 2008, 43, 431–439. [Google Scholar] [CrossRef] [PubMed]
- Grenier, D.; Cazalis, J.; Gagnon, G. Response of Periodontitis and Healthy Patients in a Porphyromonas Gingivalis-Stimulated Whole-Blood Model. J. Investig. Clin. Dent. 2011, 2, 38–42. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, N.; Honda, T.; Domon, H.; Nakajima, T.; Tabeta, K.; Yamazaki, K. Interleukin-1 Receptor-Associated Kinase-M in Gingival Epithelial Cells Attenuates the Inflammatory Response Elicited by Porphyromonas Gingivalis. J. Periodontal Res. 2010, 45, 512–519. [Google Scholar] [CrossRef]
- Sanchez-Sanchez, J.L.; Giudici, K.V.; Guyonnet, S.; Delrieu, J.; Li, Y.; Bateman, R.J.; Parini, A.; Vellas, B.; de Souto Barreto, P.; Vellas, B.; et al. Plasma MCP-1 and Changes on Cognitive Function in Community-Dwelling Older Adults. Alzheimer’s Res. Ther. 2022, 14, 5. [Google Scholar] [CrossRef]
- Joly-Amado, A.; Hunter, J.; Quadri, Z.; Zamudio, F.; Rocha-Rangel, P.V.; Chan, D.; Kesarwani, A.; Nash, K.; Lee, D.C.; Morgan, D.; et al. CCL2 Overexpression in the Brain Promotes Glial Activation and Accelerates Tau Pathology in a Mouse Model of Tauopathy. Front. Immunol. 2020, 11, 997. [Google Scholar] [CrossRef]
- Gao, A.; Van Dyke, T. Role of Suppressors of Cytokine Signaling 3 in Bone Inflammatory Responses. Front. Immunol. 2014, 4, 506. [Google Scholar] [CrossRef]
- Huang, Z.-B.; Sheng, G.-Q. Interleukin-1β with Learning and Memory. Neurosci. Bull. 2010, 26, 455–468. [Google Scholar] [CrossRef]
- Ng, A.; Tam, W.W.; Zhang, M.W.; Ho, C.S.; Husain, S.F.; McIntyre, R.S.; Ho, R.C. IL-1β, IL-6, TNF- α and CRP in Elderly Patients with Depression or Alzheimer’s Disease: Systematic Review and Meta-Analysis. Sci. Rep. 2018, 8, 12050. [Google Scholar] [CrossRef]
- Mendiola, A.S.; Cardona, A.E. The IL-1β Phenomena in Neuroinflammatory Diseases. J. Neural Transm. 2018, 125, 781–795. [Google Scholar] [CrossRef]
- Laugisch, O.; Johnen, A.; Maldonado, A.; Ehmke, B.; Burgin, W.; Olsen, I.; Potempa, J.; Sculean, A.; Duning, T.; Eick, S. Periodontal Pathogens and Associated Intrathecal Antibodies in Early Stages of Alzheimer’s Disease. J. Alzheimers Dis. 2018, 66, 105–114. [Google Scholar] [CrossRef]
- Riviere, G.R.; Riviere, K.H.; Smith, K.S. Molecular and Immunological Evidence of Oral Treponema in the Human Brain and Their Association with Alzheimer’s Disease. Oral Microbiol. Immunol. 2002, 17, 113–118. [Google Scholar] [CrossRef]
- Kolaczkowska, E.; Kubes, P. Neutrophil Recruitment and Function in Health and Inflammation. Nat. Rev. Immunol. 2013, 13, 159–175. [Google Scholar] [CrossRef]
- Pelletier, M.; Maggi, L.; Micheletti, A.; Lazzeri, E.; Tamassia, N.; Costantini, C.; Cosmi, L.; Lunardi, C.; Annunziato, F.; Romagnani, S.; et al. Evidence for a Cross-Talk between Human Neutrophils and Th17 Cells. Blood 2010, 115, 335–343. [Google Scholar] [CrossRef]
- Teixeira, F.B.; Saito, M.T.; Matheus, F.C.; Prediger, R.D.; Yamada, E.S.; Maia, C.S.F.; Lima, R.R. Periodontitis and Alzheimer’s Disease: A Possible Comorbidity between Oral Chronic Inflammatory Condition and Neuroinflammation. Front. Aging Neurosci. 2017, 9, 327. [Google Scholar] [CrossRef]
- Sochocka, M.; Sobczynski, M.; Sender-Janeczek, A.; Zwolinska, K.; Blachowicz, O.; Tomczyk, T.; Zietek, M.; Leszek, J. Association between Periodontal Health Status and Cognitive Abilities. The Role of Cytokine Profile and Systemic Inflammation. Curr. Alzheimer Res. 2017, 14, 978–990. [Google Scholar] [CrossRef]
- Adams, B.; Nunes, J.M.; Page, M.J.; Roberts, T.; Carr, J.; Nell, T.A.; Kell, D.B.; Pretorius, E. Parkinson’s Disease: A Systemic Inflammatory Disease Accompanied by Bacterial Inflammagens. Front. Aging Neurosci. 2019, 11, 210. [Google Scholar] [CrossRef]
- Kamer, A.R.; Craig, R.G.; Dasanayake, A.P.; Brys, M.; Glodzik-Sobanska, L.; de Leon, M.J. Inflammation and Alzheimer’s Disease: Possible Role of Periodontal Diseases. Alzheimer’s Dement. 2008, 4, 242–250. [Google Scholar] [CrossRef]
- Kornman, K.S.; Page, R.C.; Tonetti, M.S. The Host Response to the Microbial Challenge in Periodontitis: Assembling the Players. Periodontology 2000 1997, 14, 33–53. [Google Scholar] [CrossRef]
- Gomes-Filho, I.S.; Freitas Coelho, J.M.; da Cruz, S.S.; Passos, J.S.; Teixeira de Freitas, C.O.; Aragão Farias, N.S.; Amorim da Silva, R.; Silva Pereira, M.N.; Lima, T.L.; Barreto, M.L. Chronic Periodontitis and C-Reactive Protein Levels. J. Periodontol. 2011, 82, 969–978. [Google Scholar] [CrossRef]
- Miller, A.J.; Luheshi, G.N.; Rothwell, N.J.; Hopkins, S.J. Local Cytokine Induction by LPS in the Rat Air Pouch and Its Relationship to the Febrile Response. Am. J. Physiol. -Regul. Integr. Comp. Physiol. 1997, 272, R857–R861. [Google Scholar] [CrossRef]
- Farah, R.; Haraty, H.; Salame, Z.; Fares, Y.; Ojcius, D.M.; Said Sadier, N. Salivary Biomarkers for the Diagnosis and Monitoring of Neurological Diseases. Biomed. J. 2018, 41, 63–87. [Google Scholar] [CrossRef]
- Engelhart, M.J.; Geerlings, M.I.; Meijer, J.; Kiliaan, A.; Ruitenberg, A.; van Swieten, J.C.; Stijnen, T.; Hofman, A.; Witteman, J.C.M.; Breteler, M.M.B. Inflammatory Proteins in Plasma and the Risk of Dementia: The Rotterdam Study. Arch. Neurol. 2004, 61, 668–672. [Google Scholar] [CrossRef]
- Yaffe, K.; Kanaya, A.; Lindquist, K.; Simonsick, E.M.; Harris, T.; Shorr, R.I.; Tylavsky, F.A.; Newman, A.B. The Metabolic Syndrome, Inflammation, and Risk of Cognitive Decline. JAMA 2004, 292, 2237–2242. [Google Scholar] [CrossRef]
- Perry, V.H.; Teeling, J. Microglia and Macrophages of the Central Nervous System: The Contribution of Microglia Priming and Systemic Inflammation to Chronic Neurodegeneration. Semin. Immunopathol. 2013, 35, 601–612. [Google Scholar] [CrossRef]
- Poole, S.; Singhrao, S.K.; Kesavalu, L.; Curtis, M.A.; Crean, S. Determining the Presence of Periodontopathic Virulence Factors in Short-Term Postmortem Alzheimer’s Disease Brain Tissue. J. Alzheimers Dis. 2013, 36, 665–677. [Google Scholar] [CrossRef]
- Sato, N.; Matsumoto, T.; Kawaguchi, S.; Seya, K.; Matsumiya, T.; Ding, J.L.; Aizawa, T.; Imaizumi, T. Porphyromonas Gingivalis Lipopolysaccharide Induces Interleukin-6 and c-c Motif Chemokine Ligand 2 Expression in Cultured HCMEC/D3 Human Brain Microvascular Endothelial Cells. Gerodontology 2022, 39, 139–147. [Google Scholar] [CrossRef]
- Qian, X.S.; Zhang, S.; Duan, L.; Yang, F.C.; Zhang, K.; Yan, F.H.; Ge, S. Periodontitis Deteriorates Cognitive Function and Impairs Neurons and Glia in a Mouse Model of Alzheimer’s Disease. J. Alzheimers Dis. 2021, 79, 1785–1800. [Google Scholar] [CrossRef]
- Mancini, M.; Grappasonni, I.; Scuri, S.; Amenta, F. Oral Health in Alzheimers Disease: A Review. Curr. Alzheimer Res. 2010, 7, 368–373. [Google Scholar] [CrossRef]
- Song, J.W.; Chung, K.C. Observational Studies: Cohort and Case-Control Studies. Plast. Reconstr. Surg. 2010, 126, 2234. [Google Scholar] [CrossRef]


{kind=link}
| Author | Study Design | Sample Characteristics (Size, Controls, Location) | Diagnosis | Exposure Biomarker(s)/Measure(s) | Outcome | Results |
|---|---|---|---|---|---|---|
| Montoya et al. [33] | Case-control | n = 309 Cases = 178 Controls = 131 Spain | periodontitis |
| mild cognitive impairment | EGF, fractalkine, IL-10, IL-5, IL-6, IL-7, IL-8, IP-10, MCP-1, MCP-1α, MCP-1β, and TNF-α were significantly and negatively associated with cognitive impairment, while G-CSF, IL1- Ra, and TNF-β were significantly and positively associated with this condition |
| Noble et al. [32] | Cross-sectional | n = 2355 USA | Periodontal disease caused by P. gingivalis | Serum P gingivalis IgG reported by ELISA | Cognitive impairment | The highest P. gingivalis IgG group was more likely to have poor delayed verbal memory and impaired subtraction |
| Shin et al. [34] | Case-control | n = 189 Cases = 65 controls = 124 Korea | history of periodontitis (HOP) | Radiographic alveolar bone loss (RABL) | Cognitive impairment | Participants with HOP were 2.1 times as likely to have cognitive impairment as those without |
| Sparks Stein et al. [27] | Cohort | n = 158 Cases = 81 Controls = 77 Kentucky, USA | Periodontal pathogens | IgG antibody levels to seven oral bacteria | Cognitive impairment | Antibody levels to F. nucleatum and P. intermedia were significantly increased at baseline serum draw in the patients with AD compared with control |
| Stewart et al. [28] | Prospective cohort study | N = 1171 Health ABC Study USA | Decline in oral health | number of teeth, number of occluding pairs of teeth, probing depth, loss of attachment, mean gingival index, mean plaque score, and number of sites with bleeding on probing | Cognitive impairment | Strong associations were found for gingival inflammation and 3MS decline measured from Year 1 to 3 or from Year 1 to 5 |
| Tzeng et al. [29] | Retrospective matched cohort design. | N = 8828 Chronic periodontitis and gingivitis = 2207 Controls = 6621 Taiwan | Chronic periodontitis and gingivitis | ICD-9-CM codes: 523.4 (chronic periodontitis) and 523.1 (chronic gingivitis) | Dementia | Patients with newly diagnosed chronic periodontitis and gingivitis had an increased risk of dementia |
| C. K. Chen et al. [24] | Retrospective cohort study | N = 27,963 patients with CP = 9291 patients without CP = 18,672 Taiwan | Chronic periodontitis | Clinical assessment according to ICD-9-CM diagnostic criteria code 523.4 | Alzheimer’s disease | 10-year chronic periodontitis was associated with a 1.707-fold increase in the risk of developing Alzheimer’s disease |
| Choi et al. [25] | Retrospective cohort study | N = 262,349 (NHIS-HEALS) South Korea | Chronic periodontitis |
| Alzheimer’s disease | Chronic periodontitis patients had an elevated risk for overall dementia, Alzheimer’s disease, and vascular dementia |
| Demmer et al. [26] | Longitudinal cohort | n = 8275 (ARIC) United states | Periodontal disease | Probing depth, gingival recession and assessed bleeding on probing at six sites per tooth | Dementia and Mild Cognitive Impairment (MCI) | Periodontal disease was modestly associated with incident MCI and dementia |
| Hategan et al. [30] | Cross-sectional | N = 40 western Romania | Periodontitis |
| cognitive dysfunction and Alzheimer’s disease |
|
| Kamer et al. [31] | Cross-sectional | N = 152, Denmark | Periodontal inflammation | Each tooth was assessed by inspection, probing, and scored using a Modified Community Periodontal Index (MCPI) | Cognitive dysfunction | Subjects with periodontal inflammation had significantly lower DST and BDT (tests requiring memory) scores compared to those without periodontal inflammation |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Said-Sadier, N.; Sayegh, B.; Farah, R.; Abbas, L.A.; Dweik, R.; Tang, N.; Ojcius, D.M. Association between Periodontal Disease and Cognitive Impairment in Adults. Int. J. Environ. Res. Public Health 2023, 20, 4707. https://doi.org/10.3390/ijerph20064707
Said-Sadier N, Sayegh B, Farah R, Abbas LA, Dweik R, Tang N, Ojcius DM. Association between Periodontal Disease and Cognitive Impairment in Adults. International Journal of Environmental Research and Public Health. 2023; 20(6):4707. https://doi.org/10.3390/ijerph20064707
Chicago/Turabian StyleSaid-Sadier, Najwane, Batoul Sayegh, Raymond Farah, Linda Abou Abbas, Rania Dweik, Norina Tang, and David M. Ojcius. 2023. "Association between Periodontal Disease and Cognitive Impairment in Adults" International Journal of Environmental Research and Public Health 20, no. 6: 4707. https://doi.org/10.3390/ijerph20064707
APA StyleSaid-Sadier, N., Sayegh, B., Farah, R., Abbas, L. A., Dweik, R., Tang, N., & Ojcius, D. M. (2023). Association between Periodontal Disease and Cognitive Impairment in Adults. International Journal of Environmental Research and Public Health, 20(6), 4707. https://doi.org/10.3390/ijerph20064707