

Heart Rate Recovery Assessed by Cardiopulmonary Exercise Testing in Patients with Cardiovascular Disease: Relationship with Prognosis


Abstract
1. Introduction
2. Materials and Methods
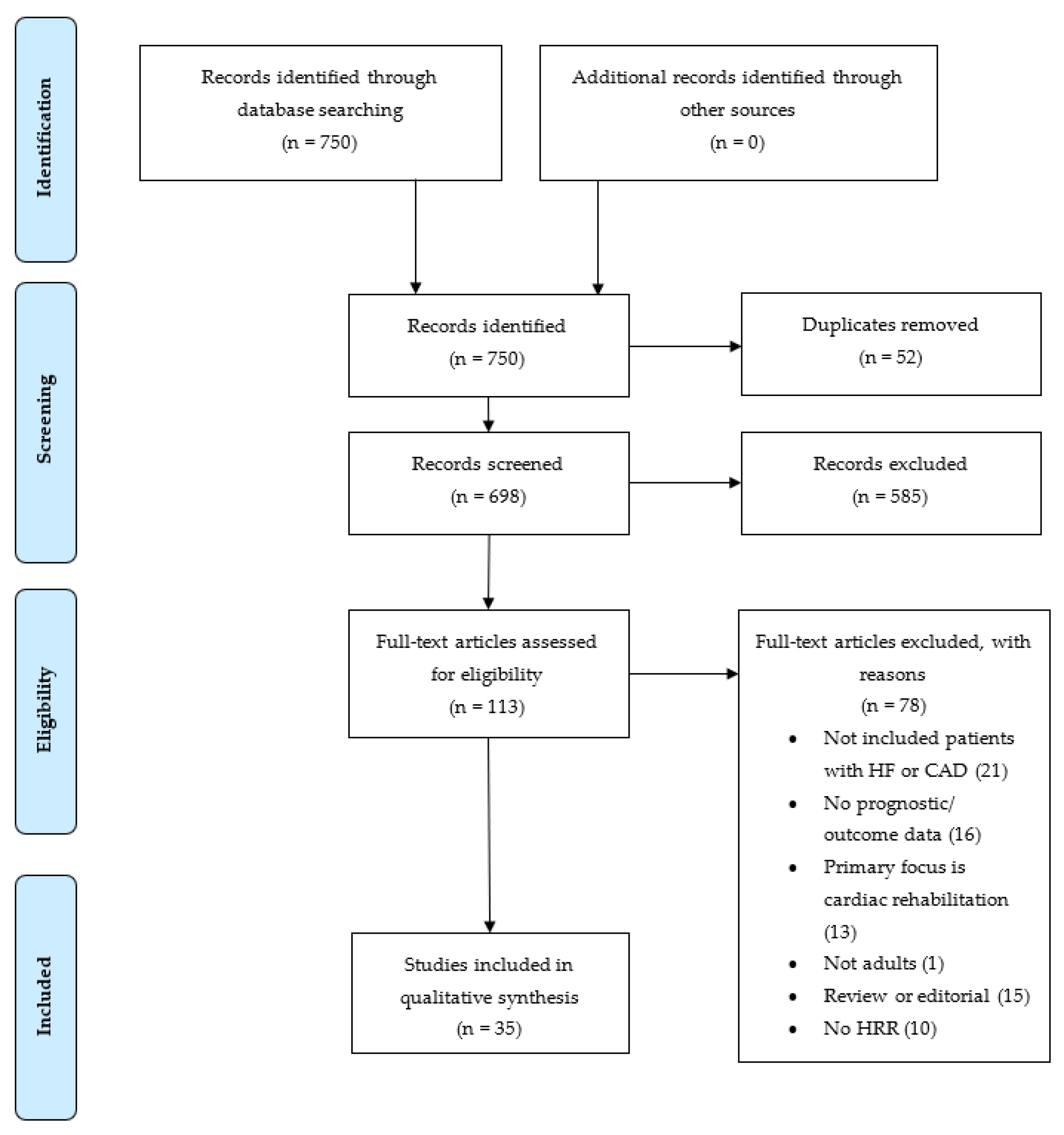
2.1. Literature Search Strategy
2.1.1. Data Sources
2.1.2. Study Selection
3. Literature Review
3.1. Mechanisms
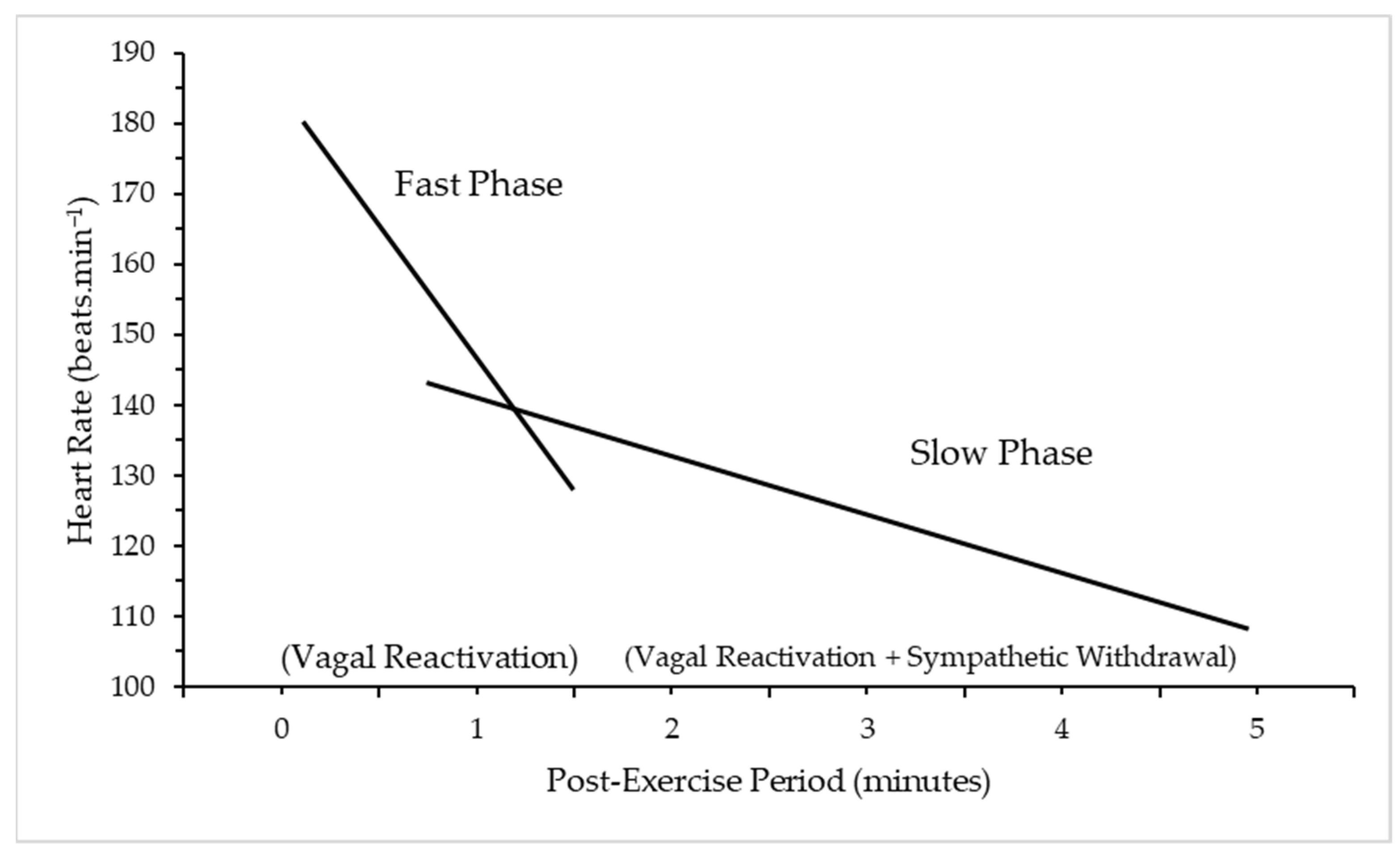
3.1.1. Background Physiology
3.1.2. Heart Rate Recovery
3.2. Heart Rate Recovery
3.2.1. Defining HRR
3.2.2. Time-Points and Thresholds of HR
3.3. Methodological Differences
3.3.1. Exercise Mode
3.3.2. Exercise Protocol
3.3.3. Recovery
Active Cool Down
Passive Cool-Down
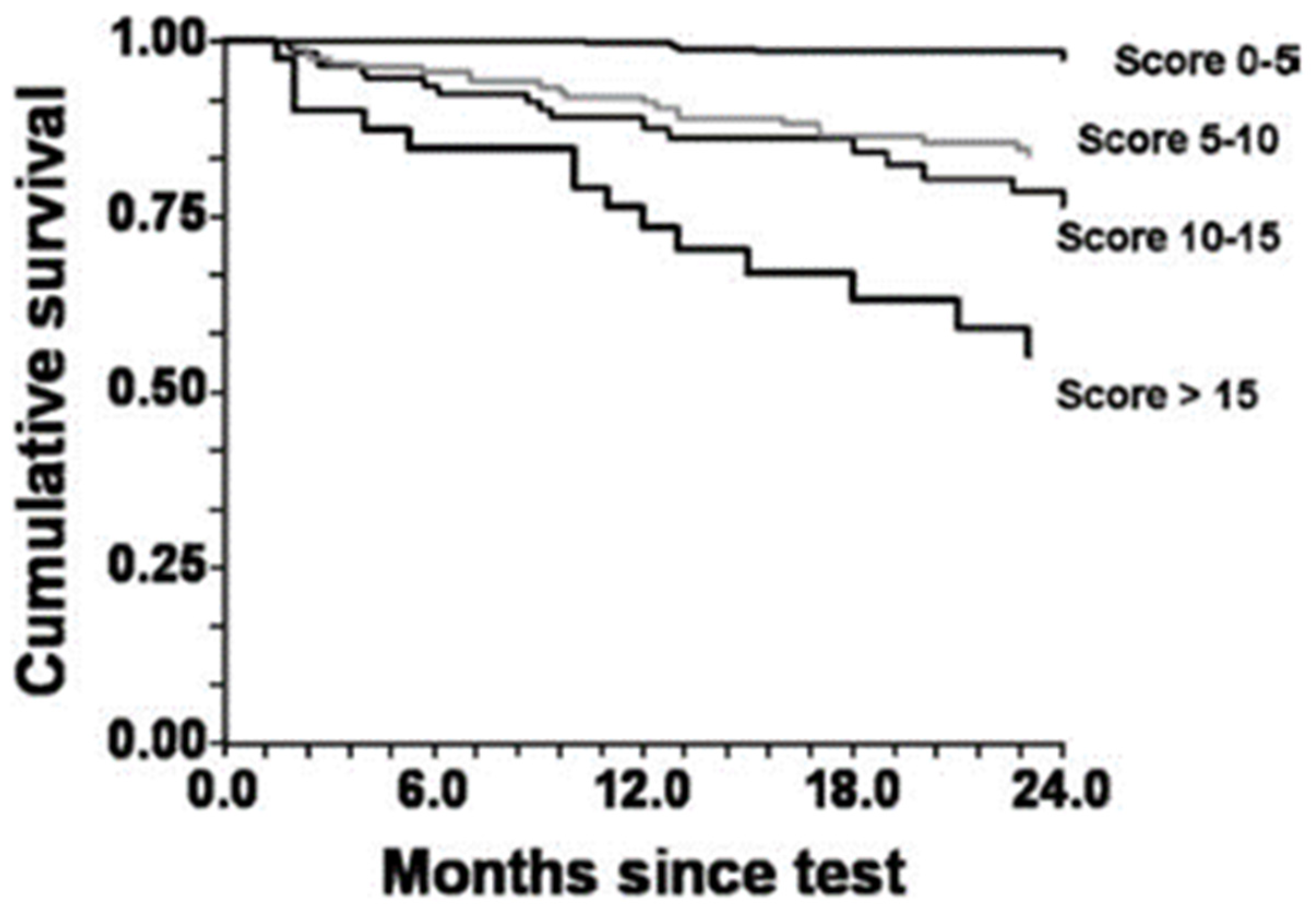
3.4. Prognosis
3.4.1. Heart Failure
All-Cause Mortality
Cardiovascular Mortality
3.4.2. Coronary Artery Disease
All-Cause Mortality
Cardiovascular Mortality
3.5. Pharmacological Impact
4. Practical Applications
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Cardiovascular Diseases (CVDs) [Internet]. 2021. Available online: http://www.who.int/mediacentre/factsheets/fs317/en/index.html (accessed on 12 December 2020).
- Hunt, S.A.; Baker, D.W.; Chin, M.H.; Cinquegrani, M.P.; Feldman, A.M.; Francis, G.S.; Ganiats, T.G.; Goldstein, S.; Gregoratos, G.; Jessup, M.L.; et al. ACC/AHA guidelines for the evaluation and management of chronic heart failure in the adult: Executive summary: A report of the american college of cardiology/american heart association task force on practice guidelines (committee to revise the 1995 guidelines for the evaluation and management of heart failure) developed in collaboration with the international society for heart and lung transplantation endorsed by the heart failure society of america. J. Am. Coll. Cardiol. 2001, 104, 2996–3007. [Google Scholar] [CrossRef]
- American Thoracic Society; American College of Chest Physicians. ATS/ACCP Statement on cardiopulmonary exercise testing. Am. J. Respir. Crit. Care Med. 2003, 167, 211–277. [Google Scholar] [CrossRef] [PubMed]
- Gibbons, R.J.; Balady, G.J.; Beasley, J.W.; Bricker, J.T.; Duvernoy, W.F.; Froelicher, V.F.; Mark, D.; Marwick, T.H.; McCallister, B.D.; Thompson, P.D.; et al. ACC/AHA guidelines for exercise testing: Executive summary. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on Exercise Testing). Circulation 1997, 96, 345–354. [Google Scholar] [CrossRef]
- Otto, C.; Nishimura, R.; Bonow, R.; Carabello, B.; Erwin, J., 3rd; Gentile, F.; Jneid, H.; Krieger, E.; Mack, M.; McLeod, C.; et al. 2020 ACC/AHA Guideline for the Management of Patients with Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2020, 143, E72–E227. [Google Scholar]
- Tzanis, G.S.; Dimopoulos, S.K.; Nanas, S.N. Recovery Kinetics: “There Is Nothing New Except What Has Been Forgotten”. JACC Heart Fail. 2016, 4, 909. [Google Scholar] [CrossRef]
- Imai, K.; Sato, H.; Hori, M.; Kusuoka, H.; Ozaki, H.; Yokoyama, H.; Takeda, H.; Inoue, M.; Kamada, T. Vagally mediated heart rate recovery after exercise is accelerated in athletes but blunted in patients with chronic heart failure. J. Am. Coll. Cardiol. 1994, 24, 1529–1535. [Google Scholar] [CrossRef]
- Buchheit, M.; Papelier, Y.; Laursen, P.B.; Ahmaidi, S. Noninvasive assessment of cardiac parasympathetic function: Postexercise heart rate recovery or heart rate variability? Am. J. Physiol.—Heart Circ. Physiol. 2007, 293, 8–10. [Google Scholar] [CrossRef]
- Shetler, K.; Marcus, R.; Froelicher, V.F.; Vora, S.; Kalisetti, D.; Prakash, M.; Do, D.; Myers, J. Heart rate recovery: Validation and methodologic issues. J. Am. Coll. Cardiol. 2001, 38, 1980–1987. [Google Scholar] [CrossRef]
- Lauer, M.S.; Blackstone, E.H.; Young, J.B.; Topol, E. Cause of death in clinical research: Time for a reassessment? J. Am. Coll. Cardiol. 1999, 34, 618–620. [Google Scholar] [CrossRef]
- Valentini, M.; Parati, G. Variables Influencing Heart Rate. Prog. Cardiovasc. Dis. 2009, 52, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Kluess, H.A.; Wood, R.H.; Welsch, M.A. Vagal modulation of the heart and central hemodynamics during handgrip exercise. Am. J. Physiol. Circ. Physiol. 2000, 278, H1648–H1652. [Google Scholar] [CrossRef]
- Cole, C.R.; Blackstone, E.H.; Pashkow, F.J.; Snader, C.E.; Lauer, M.S. Heart-Rate Recovery Immediately after Exercise as a Predictor of Mortality. N. Engl. J. Med. 1999, 341, 1351–1357. [Google Scholar] [CrossRef]
- Yanagisawa, S.; Miki, K.; Yasuda, N.; Hirai, T.; Suzuki, N.; Tanaka, T. The prognostic value of treadmill exercise testing in very elderly patients: Heart rate recovery as a predictor of mortality in octogenarians. Eur. Soc. Cardiol. 2010, 13, 114–120. [Google Scholar] [CrossRef]
- Nishime, E.O.; Cole, C.R.; Blackstone, E.H.; Pashkow, F.J.; Lauer, M. Heart Rate Recovery and Treadmill Exercise Score as Predictors of Mortality in Patients Referred for Exercise ECG. J. Am. Med. Assoc. 2000, 284, 1392–1398. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, J.; Thamilarasan, M.; Blackstone, E.H.; Thomas, J.D.; Lauer, M. Heart rate recovery immediately after treadmill exercise and left ventricular systolic dysfunction as predictors of mortality: The case of stress echocardiography. Circulation 2001, 104, 1911–1916. [Google Scholar] [CrossRef]
- Peçanha, T.; Silva-Júnior, N.D.; Forjaz, C.L.d.M. Heart rate recovery: Autonomic determinants, methods of assessment and association with mortality and cardiovascular diseases. Clin. Physiol. Funct. Imaging. 2014, 34, 327–339. [Google Scholar] [CrossRef] [PubMed]
- Arena, R.; Guazzi, M.; Myers, J.; Peberdy, M.A. Prognostic value of heart rate recovery in patients with heart failure. Am. Heart J. 2006, 151, 851.e7–851.e13. [Google Scholar] [CrossRef] [PubMed]
- Sheppard, R.; Racine, N.; Roof, A.; Ducharme, A.; Blanchet, M.; White, M. Heart rate recovery—A potential marker of clinical outcomes in heart failure patients receiving beta-blocker therapy. Can. J. Cardiol. 2007, 23, 1135–1138. [Google Scholar] [CrossRef]
- Arena, R.; Myers, J.; Abella, J.; Peberdy, M.A.; Bensimhon, D.; Chase, P.; Guazzi, M. The prognostic value of the heart rate response during exercise and recovery in patients with heart failure: Influence of beta-blockade. Int. J. Cardiol. 2010, 138, 166–173. [Google Scholar] [CrossRef]
- Nissinen, S.I.; Mäkikallio, T.H.; Seppänen, T.; Tapanainen, J.M.; Salo, M.; Tulppo, M.P.; Huikuri, H.V. Heart rate recovery after exercise as a predictor of mortality among survivors of acute myocardial infarction. Am. J. Cardiol. 2003, 91, 711–714. [Google Scholar] [CrossRef]
- Gorelik, D.D.; Hadley, D.; Myers, J.; Froelicher, V. Is there a better way to predict death using heart rate recovery? Clin. Cardiol. 2006, 29, 399–404. [Google Scholar] [CrossRef] [PubMed]
- Hajdusek, P.; Kotrc, M.; Kautzner, J.; Melenovsky, V.; Benesova, E.; Jarolim, P.; Benes, J. Heart rate response to exercise in heart failure patients: The prognostic role of metabolic–chronotropic relation and heart rate recovery. Int. J. Cardiol. 2016, 228, 588–593. [Google Scholar] [CrossRef]
- Nanas, S.; Anastasiou-Nana, M.; Dimopoulos, S.; Sakellariou, D.; Alexopoulos, G.; Kapsimalakou, S.; Papazoglou, P.; Tsolakis, E.; Papazachou, O.; Roussos, C.; et al. Early heart rate recovery after exercise predicts mortality in patients with chronic heart failure. Int. J. Cardiol. 2006, 110, 393–400. [Google Scholar] [CrossRef] [PubMed]
- Bilsel, T.; Terzi, S.; Akbulut, T.; Sayar, N.; Hobikoglu, G.; Yesilcimen, K. Abnormal Heart Rate Recovery Immediately After Cardiopulmonary Exercise Testing in Heart Failure Patients. Int. Heart J. 2006, 47, 431–440. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Messinger-Rapport, B.; Snader, C.E.P.; Blackstone, E.H.; Yu, D.; Lauer, M.S. Value of Exercise Capacity and Heart Rate Recovery in Older People. J. Am. Geriatr. Soc. 2003, 51, 63–68. [Google Scholar] [CrossRef]
- Vivekananthan, D.P.; Blackstone, E.H.; Pothier, C.E.; Lauer, M.S. Heart rate recovery after exercise is apredictor of mortality, independent of the angiographic severity of coronary disease. J. Am. Coll. Cardiol. 2003, 42, 831–838. [Google Scholar] [CrossRef]
- Lipinski, M.J.; Vetrovec, G.W.; Froelicher, V.F. Importance of the first two minutes of heart rate recovery after exercise treadmill testing in predicting mortality and the presence of coronary artery disease in men. Am. J. Cardiol. 2004, 93, 445–449. [Google Scholar] [CrossRef]
- Goda, A.; Koike, A.; Iwamoto, M.H.; Nagayama, O.; Yamaguchi, K.; Tajima, A.; Sawada, H.; Itoh, H.; Isobe, M.; Aizawa, T. Prognostic Value of Heart Rate Profiles During Cardiopulmonary Exercise Testing in Patients With Cardiac Disease. Int. Heart J. 2009, 50, 59–71. [Google Scholar] [CrossRef]
- Lipinski, M.J.; Vetrovec, G.W.; Gorelik, D.; Froelicher, V.F. The Importance of Heart Rate Recovery in Patients With Heart Failure or Left Ventricular Systolic Dysfunction. J. Card. Fail. 2005, 11, 624–630. [Google Scholar] [CrossRef]
- Hermansen, L.; Saltin, B. Oxygen uptake during maximal treadmill and bicycle exercise. J. Appl. Physiol. 1969, 26, 31–37. [Google Scholar] [CrossRef]
- Cahalin, L.P.; Arena, R.; Labate, V.; Bandera, F.; Lavie, C.J.; Guazzi, M. Heart rate recovery after the 6 min walk test rather than distance ambulated is a powerful prognostic indicator in heart failure with reduced and preserved ejection fraction: A comparison with cardiopulmonary exercise testing. Eur. J. Heart Fail. 2013, 15, 519–527. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y.-D.; Dewland, T.A.; Wencker, D.; Katz, S.D. Post-Exercise Heart Rate Recovery Independently Predicts Mortality Risk in Patients With Chronic Heart Failure. J. Card. Fail. 2009, 15, 850–855. [Google Scholar] [CrossRef] [PubMed]
- Cahalin, L.P.; Forman, D.E.; Chase, P.; Guazzi, M.; Myers, J.; Bensimhon, D.; Peberdy, M.A.; Ashley, E.; West, E.; Arena, R. The prognostic significance of heart rate recovery is not dependent upon maximal effort in patients with heart failure. Int. J. Cardiol. 2013, 168, 1496–1501. [Google Scholar] [CrossRef] [PubMed]
- Dufay-Bougon, C.; Belin, A.; Dahdouh, Z.S.; Barthelemy, S.; Mabire, J.-P.; Sabatier, R.; Milliez, P.; Grollier, G. The prognostic value of the cardiopulmonary exercise test in patients with heart failure who have been treated with beta-blockers. Turk. Kardiyol. Dern. Ars. 2013, 41, 105–112. [Google Scholar] [CrossRef][Green Version]
- Ritt, L.E.; Oliveira, R.B.; Myers, J.; Arena, R.; Peberdy, M.A.; Bensimhon, D.; Chase, P.; Forman, D.; Guazzi, M. Patients with heart failure in the “intermediate Range” of peak oxygen uptake: Additive value of heart rate recovery and the minute ventilation/carbon dioxide output slope in predicting mortality. J. Cardiopulm. Rehabil. Prev. 2012, 32, 141–146. [Google Scholar] [CrossRef]
- Myers, J.; Arena, R.; Dewey, F.; Bensimhon, D.; Abella, J.; Hsu, L.; Chase, P.; Guazzi, M.; Peberdy, M.A. A cardiopulmonary exercise testing score for predicting outcomes in patients with heart failure. Am. Heart J. 2008, 156, 1177–1183. [Google Scholar] [CrossRef]
- Karjalainen, J.J.; Kiviniemi, A.M.; Hautala, A.J.; Piira, O.-P.; Lepojärvi, E.S.; Peltola, M.A.; Ukkola, O.H.; Hedberg, P.S.; Huikuri, H.V.; Tulppo, M.P. Determinants and Prognostic Value of Cardiovascular Autonomic Function in Coronary Artery Disease Patients With and Without Type 2 Diabetes. Diabetes Care 2013, 37, 286–294. [Google Scholar] [CrossRef]
- Cruickshank, J. Are we misunderstanding beta-blockers. Int. J. Cardiol. 2007, 120, 10–27. [Google Scholar] [CrossRef]
- Yaylali, Y.T.; Fındıkoglu, G.; Yurtdas, M.; Konukcu, S.; Senol, H. The effects of baseline heart rate recovery normality and exercise training protocol on heart rate recovery in patients with heart failure. Anatol. J. Cardiol. 2015, 15, 727–734. [Google Scholar] [CrossRef]
- Anderson, L.; Thompson, D.; Oldridge, N.; Zwisler, A.-D.; Rees, K.; Martin, N.; Taylor, R. Exercise-based cardiac rehabilitation for coronary heart disease. Cochrane Database Syst. Rev. 2016, 2016, CD001800. [Google Scholar] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Absolute | Relative |
|---|---|
| Acute myocardial infarctions (<2 days) | Left main coronary stenosis |
| Unstable angina | Moderate stenotic valvular disease |
| Uncontrolled cardiac arrhythmias causing symptoms of hemodynamic compromise | Electrolyte abnormalities |
| Symptomatic severe aortic stenosis | Severe arterial hypertension |
| Uncontrolled symptomatic heart failure | Tachyarrhythmias or bradyarrhythmias |
| Acute pulmonary embolus or pulmonary infection | Hypertrophic cardiomyopathy and other forms of outflow tract obstruction |
| Acute myocarditis and pericarditis | Mental or physical impairment, leading to inability to exercise adequately |
| Acute aortic dissection | High-degree atrioventricular block |
| HRR | Cut-Point (bpm) | Predictive Accuracy | Sensitivity | Specificity |
|---|---|---|---|---|
| 1 min HRR | ||||
| LVSD alone + no BB | Abnormal <9 | 61% | 35% | 78% |
| LVSD alone + BB | Abnormal <9 | 62% | 44% | 72% |
| HF + no BB | Abnormal <9 | 69% | 65% | 73% |
| HF+ BB | Abnormal <9 | 72% | 64% | 79% |
| Neither + no BB | Abnormal <10 | 63% | 54% | 66% |
| Neither + no BB | Abnormal <10 | 64% | 52% | 68% |
| 2 min HRR | ||||
| LVSD alone + no BB | Abnormal <27 | 69% | 48% | 82% |
| LVSD alone + BB | Abnormal <23 | 70% | 56% | 78% |
| HF + no BB | Abnormal <24 | 64% | 51% | 78% |
| HF + BB | Abnormal <23 | 64% | 45% | 79% |
| Neither + no BB | Abnormal <24 | 71% | 31% | 86% |
| Neither + no BB | Abnormal <17 | 77% | 25% | 94% |
| 5 min HRR | ||||
| LVSD alone + no BB | Abnormal <33 | 65% | 30% | 88% |
| LVSD alone + BB | Abnormal <30 | 69% | 51% | 79% |
| HF + no BB | Abnormal <37 | 65% | 54% | 78% |
| HF + BB | Abnormal <36 | 60% | 55% | 64% |
| Neither + no BB | Abnormal <32 | 72% | 21% | 90% |
| Neither + no BB | Abnormal <32 | 67% | 43% | 75% |
| Cycle Ergometer | Treadmill Ergometer | |
|---|---|---|
| Maximal oxygen uptake | Lower | Higher |
| Work rate measurement | Yes | No |
| Blood gas collection | Easier | More difficult |
| Noise and artifacts | Less | More |
| Safety | Safer | Less safe |
| Weight bearing in obese | Less | More |
| Degree of leg muscle training | Less | More |
| More appropriate for | Patients | Active healthy subjects |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dewar, A.; Kass, L.; Stephens, R.C.M.; Tetlow, N.; Desai, T. Heart Rate Recovery Assessed by Cardiopulmonary Exercise Testing in Patients with Cardiovascular Disease: Relationship with Prognosis. Int. J. Environ. Res. Public Health 2023, 20, 4678. https://doi.org/10.3390/ijerph20064678
Dewar A, Kass L, Stephens RCM, Tetlow N, Desai T. Heart Rate Recovery Assessed by Cardiopulmonary Exercise Testing in Patients with Cardiovascular Disease: Relationship with Prognosis. International Journal of Environmental Research and Public Health. 2023; 20(6):4678. https://doi.org/10.3390/ijerph20064678
Chicago/Turabian StyleDewar, Amy, Lindsy Kass, Robert C. M. Stephens, Nicholas Tetlow, and Terun Desai. 2023. "Heart Rate Recovery Assessed by Cardiopulmonary Exercise Testing in Patients with Cardiovascular Disease: Relationship with Prognosis" International Journal of Environmental Research and Public Health 20, no. 6: 4678. https://doi.org/10.3390/ijerph20064678
APA StyleDewar, A., Kass, L., Stephens, R. C. M., Tetlow, N., & Desai, T. (2023). Heart Rate Recovery Assessed by Cardiopulmonary Exercise Testing in Patients with Cardiovascular Disease: Relationship with Prognosis. International Journal of Environmental Research and Public Health, 20(6), 4678. https://doi.org/10.3390/ijerph20064678