
Association between Smoking and Periodontal Disease in South Korean Adults

 , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Data
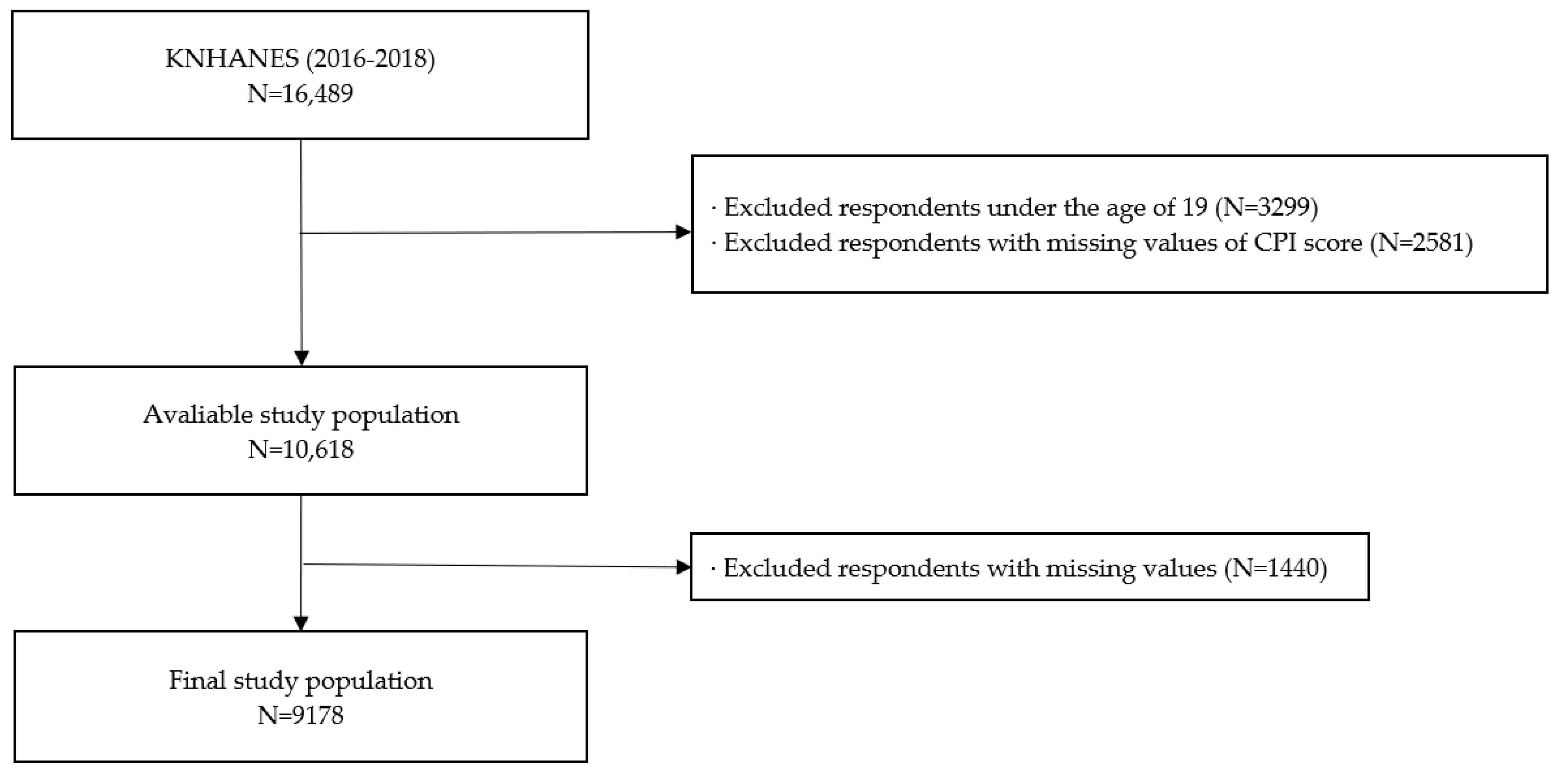
2.2. Study Population
2.3. Variables
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO World Health Organization. Fact Sheets of Tobacco. Available online: https://www.who.int/news-room/fact-sheets/detail/tobacco (accessed on 11 November 2021).
- IHME Global Burden of Disease Results-GBD Estimate of Oral Health. Available online: https://vizhub.healthdata.org/gbd-results/ (accessed on 11 November 2022).
- Varghese, C.; Troisi, G.; Schotte, K.; Prasad, V.M.; Claire, S.M.S. World No Tobacco Day 2019 puts the spotlight on lung health. J. Thorac. Dis. 2019, 11, 2639–2642. [Google Scholar] [CrossRef]
- Jeong, W.; Choi, D.W.; Kim, Y.K.; Lee, H.J.; Lee, S.A.; Park, E.C.; Jang, S.I. Associations of electronic and conventional cigarette use with periodontal disease in South Korean adults. J. Periodontol. 2020, 91, 55–64. [Google Scholar] [CrossRef] [PubMed]
- OECD. Organisation for Economic Co-operation and Development-Health Statistics 2021. Available online: https://data.oecd.org/searchresults/?q= (accessed on 16 January 2023).
- Lee, S.; Kimm, H.; Yun, J.E.; Jee, S.H. Public Health Challenges of Electronic Cigarettes in South Korea. J. Prev. Med. Public Health 2011, 44, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Inoue-Choi, M.; Hartge, P.; Liao, L.M.; Caporaso, N.; Freedman, N.D. Association between long-term low-intensity cigarette smoking and incidence of smoking-related cancer in the national institutes of health-AARP cohort. Int. J. Cancer 2017, 142, 271–280. [Google Scholar] [CrossRef] [PubMed]
- Huh, Y.; Han, K.; Choi, M.-J.; Kim, J.H.; Kim, S.M.; Nam, G.E. Association of Smoking Status With the Risk of Type 2 Diabetes Among Young Adults: A Nationwide Cohort Study in South Korea. Nicotine Tob. Res. 2022, 24, 1234–1240. [Google Scholar] [CrossRef]
- Will, J.C.; Galuska, D.A.; Ford, E.S.; Mokdad, A.; Calle, E.E. Cigarette smoking and diabetes mellitus: Evidence of a positive association from a large prospective cohort study. Int. J. Epidemiol. 2001, 30, 540–546. [Google Scholar] [CrossRef]
- Johnson, G.K.; Guthmiller, J.M. The impact of cigarette smoking on periodontal disease and treatment. Periodontology 2000 2007, 44, 178–194. [Google Scholar] [CrossRef]
- Gajendra, S.; McIntosh, S.; Ghosh, S. Effects of tobacco product use on oral health and the role of oral healthcare providers in cessation: A narrative review. Tob. Induc. Dis. 2023, 21, 12. [Google Scholar] [CrossRef]
- Agnihotri, R.; Gaur, S. Implications of tobacco smoking on the oral health of older adults. Geriatr. Gerontol. Int. 2014, 14, 526–540. [Google Scholar] [CrossRef]
- Hussein, B.J.; Khalil, A.M.; Atallah, H.N.; Ali, N.A. Assessment of salivary interleukin-17 and vitamin d levels in smokers with severe periodontitis patients and healthy individuals. J. Pharm. Negat. Results 2023, 2, 7147–7155. [Google Scholar]
- Kinane, D.; Chestnutt, I. Smoking and periodontal disease. Crit. Rev. Oral Biol. Med. 2000, 11, 356–365. [Google Scholar] [CrossRef] [PubMed]
- Fiorini, T.; Musskopf, M.L.; Oppermann, R.V.; Susin, C. Is There a Positive Effect of Smoking Cessation on Periodontal Health? A Systematic Review. J. Periodontol. 2014, 85, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Leite, F.R.; Nascimento, G.G.; Scheutz, F.; López, R. Effect of Smoking on Periodontitis: A Systematic Review and Meta-regression. Am. J. Prev. Med. 2018, 54, 831–841. [Google Scholar] [CrossRef]
- Han, D.-H.; Lim, S.; Kim, J.-B. The Association of Smoking and Diabetes With Periodontitis in a Korean Population. J. Periodontol. 2012, 83, 1397–1406. [Google Scholar] [CrossRef] [PubMed]
- Hong, M.-H. TRelationship between Oral Health Behavior, Chronic Disease and Periodontal Disease in Middle and Older Adults According to Gender. J. Korea Acad.-Ind. Coop. Soc. 2018, 19, 403–410. [Google Scholar]
- Petrenya, N.; Hopstock, L.A.; Holde, G.E.; Oscarson, N.; Jönsson, B. Relationship between periodontitis and risk of cardiovascular disease: Insights from the Tromsø Study. J. Periodontol. 2022, 93, 1353–1365. [Google Scholar] [CrossRef]
- Machuca, G.; Rosales, I.; LaCalle, J.R.; Machuca, C.; Bullon, P. Effect of Cigarette Smoking on Periodontal Status of Healthy Young Adults. J. Periodontol. 2000, 71, 73–78. [Google Scholar] [CrossRef]
- Jang, A.-Y.; Lee, J.-K.; Shin, J.; Lee, H.-Y. Association between Smoking and Periodontal Disease in Korean Adults: The Fifth Korea National Health and Nutrition Examination Survey (2010 and 2012). Korean J. Fam. Med. 2016, 37, 117–122. [Google Scholar] [CrossRef]
- Tomar, S.L.; Asma, S. Smoking-Attributable Periodontitis in the United States: Findings From NHANES III. J. Periodontol. 2000, 71, 743–751. [Google Scholar] [CrossRef]
- Reitsma, M.B.; Flor, L.S.; Mullany, E.C.; Gupta, V.; Hay, S.I.; Gakidou, E. Spatial, temporal, and demographic patterns in prevalence of smoking tobacco use and initiation among young people in 204 countries and territories, 1990–2019. Lancet Public Health 2021, 6, e472–e481. [Google Scholar] [CrossRef]
- Research, S. Position paper: Tobacco use and the periodontal patient. J. Periodontol. 1999, 70, 1419–1427. [Google Scholar]
- Apatzidou, D.A. The role of cigarette smoking in periodontal disease and treatment outcomes of dental implant therapy. Periodontology 2000 2022, 90, 45–61. [Google Scholar] [CrossRef] [PubMed]
- Haffajee, A.; Cugini, M.; Dibart, S.; Smith, C.; Kent Jr, R.; Socransky, S. The effect of SRP on the clinical and microbiological parameters of periodontal diseases. J. Clin. Periodontol. 1997, 24, 324–334. [Google Scholar] [CrossRef] [PubMed]
- Zambon, J.; Grossi, S.; Machtei, E.; Ho, A.; Dunford, R.; Genco, R. Cigarette Smoking Increases the Risk for Subgingival Infection With Periodontal Pathogens. J. Periodontol. 1996, 67, 1050–1054. [Google Scholar] [CrossRef] [PubMed]
- Giannopoulou, C.; Geinoz, A.; Cimasoni, G. Effects of nicotine on periodontal ligament fibroblasts in vitro. J. Clin. Periodontol. 1999, 26, 49–55. [Google Scholar] [CrossRef]
- Arcavi, L.; Benowitz, N.L. Cigarette smoking and infection. Arch. Intern. Med. 2004, 164, 2206–2216. [Google Scholar] [CrossRef]
- Selvaraj, S.; Naing, N.N.; Wan-Arfah, N.; Djearamane, S.; Wong, L.S.; Subramaniyan, V.; Fuloria, N.K.; Sekar, M.; Fuloria, S.; de Abreu, M.H.N.G. Epidemiological Factors of Periodontal Disease Among South Indian Adults. J. Multidiscip. Healthc. 2022, 15, 1547–1557. [Google Scholar] [CrossRef]
- Figueiredo, A.; Soares, S.; Lopes, H.; dos Santos, J.N.; Ramalho, L.M.P.; Cangussu, M.C.; Cury, P.R. Destructive periodontal disease in adult Indians from Northeast Brazil: Cross-sectional study of prevalence and risk indicators. J. Clin. Periodontol. 2013, 40, 1001–1006. [Google Scholar] [CrossRef]
- Zini, A.; Sgan-Cohen, H.D.; Marcenes, W. Socio-economic position, smoking, and plaque: A pathway to severe chronic periodontitis. J. Clin. Periodontol. 2010, 38, 229–235. [Google Scholar] [CrossRef]
- Lang, W.P.; Farghaly, M.M.; Ronis, D.L. The relation of preventive dental behaviors to periodontal health status. J. Clin. Periodontol. 1994, 21, 194–198. [Google Scholar] [CrossRef]
- Takami, Y.; Nakagaki, H.; Morita, I.; Tsuboi, S.; Takami, S.; Suzuki, N.; Niwa, H.; Ogura, Y. Blood Test Values and Community Periodontal Index Scores in Medical Checkup Recipients. J. Periodontol. 2003, 74, 1778–1784. [Google Scholar] [CrossRef] [PubMed]
- Ji, M.G. Relationship between adults’ smoking realities and periodontal disease-2009 Korea National Health and Nutrition Examination Survey data. J. Korea Inst. Electron. Commun. Sci. 2012, 7, 917–924. [Google Scholar]
- FCTC. WHO Framework Convention on Tobacco Control. Available online: https://fctc.who.int/publications/i/item/9241591013 (accessed on 16 January 2023).


{kind=link}
| Variables | Community Periodontal Index (CPI) | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Male | Female | ||||||||||||||
| Total | No | Yes | p-Value | Total | No | Yes | p-Value | ||||||||
| N | % | N | % | N | % | N | % | N | % | N | % | ||||
| Total (N = 9178) | 4161 | 45.3 | 1119 | 26.9 | 3042 | 73.1 | 5017 | 54.7 | 1874 | 37.4 | 3143 | 62.6 | |||
| Smoking Behavior | <0.0001 | 0.0130 | |||||||||||||
| Non-smoker | 1054 | 25.3 | 376 | 35.7 | 678 | 64.3 | 4391 | 87.5 | 1668 | 38.0 | 2723 | 62.0 | |||
| Ex-smoker | 1623 | 39.0 | 419 | 25.8 | 1204 | 74.2 | 344 | 6.9 | 123 | 35.8 | 221 | 64.2 | |||
| Current smoker | 1484 | 35.7 | 324 | 21.8 | 1160 | 78.2 | 282 | 5.6 | 83 | 29.4 | 199 | 70.6 | |||
| Age | <0.0001 | <0.0001 | |||||||||||||
| 20–29 | 645 | 15.5 | 276 | 42.8 | 369 | 57.2 | 688 | 13.7 | 361 | 52.5 | 327 | 47.5 | |||
| 30–39 | 800 | 19.2 | 250 | 31.3 | 550 | 68.8 | 1007 | 20.1 | 453 | 45.0 | 554 | 55.0 | |||
| 40–49 | 936 | 22.5 | 238 | 25.4 | 698 | 74.6 | 1215 | 24.2 | 447 | 36.8 | 768 | 63.2 | |||
| 50–59 | 810 | 19.5 | 175 | 21.6 | 635 | 78.4 | 1044 | 20.8 | 319 | 30.6 | 725 | 69.4 | |||
| 60–69 | 585 | 14.1 | 114 | 19.5 | 471 | 80.5 | 718 | 14.3 | 202 | 28.1 | 516 | 71.9 | |||
| ≥70 | 385 | 9.3 | 66 | 17.1 | 319 | 82.9 | 345 | 6.9 | 92 | 26.7 | 253 | 73.3 | |||
| Marital status | <0.0001 | <0.0001 | |||||||||||||
| Married | 2916 | 70.1 | 683 | 23.4 | 2233 | 76.6 | 3507 | 69.9 | 1234 | 35.2 | 2273 | 64.8 | |||
| Divorced | 146 | 3.5 | 30 | 20.5 | 116 | 79.5 | 302 | 6.0 | 80 | 26.5 | 222 | 73.5 | |||
| Single | 1099 | 26.4 | 406 | 36.9 | 693 | 63.1 | 1208 | 24.1 | 560 | 46.4 | 648 | 53.6 | |||
| Educational level | <0.0001 | <0.0001 | |||||||||||||
| Middle school | 673 | 16.2 | 85 | 12.6 | 588 | 87.4 | 1057 | 21.1 | 250 | 23.7 | 807 | 76.3 | |||
| High school | 1498 | 36.0 | 416 | 27.8 | 1082 | 72.2 | 1767 | 35.2 | 652 | 36.9 | 1115 | 63.1 | |||
| College | 1990 | 47.8 | 618 | 31.1 | 1372 | 68.9 | 2193 | 43.7 | 972 | 44.3 | 1221 | 55.7 | |||
| Household income | <0.0001 | <0.0001 | |||||||||||||
| Low | 477 | 11.5 | 93 | 19.5 | 384 | 80.5 | 632 | 12.6 | 179 | 28.3 | 453 | 71.7 | |||
| Mid-low | 939 | 22.6 | 230 | 24.5 | 709 | 75.5 | 1239 | 24.7 | 449 | 36.2 | 790 | 63.8 | |||
| Mid-high | 1280 | 30.8 | 345 | 27.0 | 935 | 73.0 | 1526 | 30.4 | 592 | 38.8 | 934 | 61.2 | |||
| High | 1465 | 35.2 | 451 | 30.8 | 1014 | 69.2 | 1620 | 32.3 | 654 | 40.4 | 966 | 59.6 | |||
| Region | <0.0001 | <0.0001 | |||||||||||||
| Metropolitan | 1973 | 47.4 | 533 | 27.0 | 1440 | 73.0 | 2437 | 48.6 | 927 | 38.0 | 1510 | 62.0 | |||
| Urban | 1556 | 37.4 | 479 | 30.8 | 1077 | 69.2 | 1891 | 37.7 | 798 | 42.2 | 1093 | 57.8 | |||
| Rural | 632 | 15.2 | 107 | 16.9 | 525 | 83.1 | 689 | 13.7 | 149 | 21.6 | 540 | 78.4 | |||
| Perceived stress level | 0.2388 | 0.1054 | |||||||||||||
| Low | 636 | 15.3 | 150 | 23.6 | 486 | 76.4 | 663 | 13.2 | 234 | 35.3 | 429 | 64.7 | |||
| Mid-low | 2433 | 58.5 | 667 | 27.4 | 1766 | 72.6 | 2858 | 57.0 | 1059 | 37.1 | 1799 | 62.9 | |||
| Mid-high | 934 | 22.4 | 259 | 27.7 | 675 | 72.3 | 1214 | 24.2 | 485 | 40.0 | 729 | 60.0 | |||
| High | 158 | 3.8 | 43 | 27.2 | 115 | 72.8 | 282 | 5.6 | 96 | 34.0 | 186 | 66.0 | |||
| Occupational categories | <0.0001 | <0.0001 | |||||||||||||
| White | 1433 | 34.4 | 463 | 32.3 | 970 | 67.7 | 1419 | 28.3 | 633 | 44.6 | 786 | 55.4 | |||
| Pink | 495 | 11.9 | 128 | 25.9 | 367 | 74.1 | 846 | 16.9 | 284 | 33.6 | 562 | 66.4 | |||
| Blue | 1309 | 31.5 | 229 | 17.5 | 1080 | 82.5 | 657 | 13.1 | 174 | 26.5 | 483 | 73.5 | |||
| Inoccupation | 924 | 22.2 | 299 | 32.4 | 625 | 67.6 | 2095 | 41.8 | 783 | 37.4 | 1312 | 62.6 | |||
| Current drinking status | <0.0001 | 0.7788 | |||||||||||||
| Never | 1019 | 24.5 | 274 | 26.9 | 745 | 73.1 | 2457 | 49.0 | 914 | 37.2 | 1543 | 62.8 | |||
| Monthly | 1640 | 39.4 | 515 | 31.4 | 1125 | 68.6 | 1847 | 36.8 | 700 | 37.9 | 1147 | 62.1 | |||
| Weekly | 1502 | 36.1 | 330 | 22.0 | 1172 | 78.0 | 713 | 14.2 | 260 | 36.5 | 453 | 63.5 | |||
| Physical activity | <0.0001 | 0.0002 | |||||||||||||
| Adequate | 2077 | 49.9 | 614 | 29.6 | 1463 | 70.4 | 2210 | 44.1 | 888 | 40.2 | 1322 | 59.8 | |||
| Inadequate | 2084 | 50.1 | 505 | 24.2 | 1579 | 75.8 | 2807 | 55.9 | 986 | 35.1 | 1821 | 64.9 | |||
| Teeth Brushing Frequency | <0.0001 | <0.0001 | |||||||||||||
| ≤1 | 464 | 11.2 | 102 | 22.0 | 362 | 78.0 | 164 | 3.3 | 43 | 26.2 | 121 | 73.8 | |||
| 2 | 1694 | 40.7 | 399 | 23.6 | 1295 | 76.4 | 1779 | 35.5 | 619 | 34.8 | 1160 | 65.2 | |||
| ≥3 | 2003 | 48.1 | 618 | 30.9 | 1385 | 69.1 | 3074 | 61.3 | 1212 | 39.4 | 1862 | 60.6 | |||
| Dental checkup status | <0.0001 | <0.0001 | |||||||||||||
| No | 2616 | 62.9 | 609 | 23.3 | 2007 | 76.7 | 3016 | 60.1 | 1004 | 33.3 | 2012 | 77.7 | |||
| Yes | 1545 | 37.1 | 510 | 33.0 | 1035 | 67.0 | 2001 | 39.9 | 870 | 24.0 | 1131 | 76.0 | |||
| Variables | Community Periodontal Index (CPI) | ||||
|---|---|---|---|---|---|
| Male | Female | ||||
| OR | 95% CIs | OR | 95% CIs | ||
| Smoking Behavior | |||||
| Non-smoker | 1.00 | 1.00 | |||
| Ex-smoker | 1.20 | (0.95–1.50) | 1.19 | (0.89–1.60) | |
| Current smoker | 1.78 * | (1.43–2.23) | 1.44 * | (1.04–1.99) | |
| Age | |||||
| 20–29 | 1.00 | 1.00 | |||
| 30–39 | 1.41 | (0.99–2.00) | 1.18 | (0.91–1.54) | |
| 40–49 | 1.77 * | (1.24–2.51) | 1.63 * | (1.24–2.15) | |
| 50–59 | 1.83 * | (1.24–2.69) | 1.93 * | (1.44–2.57) | |
| 60–69 | 2.36 * | (1.53–3.64) | 1.79 * | (1.27–2.52) | |
| ≥70 | 2.87 * | (1.70–4.83) | 1.88 * | (1.20–2.96) | |
| Marital status | |||||
| Married | 1.00 | 1.00 | |||
| Divorced | 0.77 | (0.51–1.17) | 1.36 | (0.97–1.92) | |
| Single | 0.86 | (0.64–1.14) | 0.79 * | (0.63–0.98) | |
| Educational level | |||||
| Middle school | 1.63 * | (1.15–2.23) | 1.59 * | (1.18–2.14) | |
| High school | 1.10 | (0.89–1.35) | 1.10 | (0.92–1.31) | |
| College | 1.00 | 1.00 | |||
| Household income | |||||
| Low | 1.47 * | (1.01–2.15) | 1.03 | (0.78–1.37) | |
| Mid-low | 1.15 | (0.90–1.46) | 0.99 | (0.82–1.21) | |
| Mid-high | 1.05 | (0.86–1.28) | 0.93 | (0.78–1.12) | |
| High | 1.00 | 1.00 | |||
| Region | |||||
| Metropolitan | 1.00 | 1.00 | |||
| Urban | 0.77 | (0.59–1.02) | 0.73 | (0.57–0.92) | |
| Rural | 1.39 | (0.91–2.10) | 1.78 * | (1.19–2.67) | |
| Perceived stress level | |||||
| Low | 1.00 | 1.00 | |||
| Mid-low | 0.89 | (0.69–1.14) | 1.02 | (0.83–1.26) | |
| Mid-high | 0.93 | (0.68–1.27) | 0.98 | (0.77–1.25) | |
| High | 0.94 | (0.59–1.50) | 1.25 | (0.881.77) | |
| Occupational categories | |||||
| White | 1.00 | 1.00 | |||
| Pink | 1.13 | (0.85–1.52) | 1.17 | (0.92–1.48) | |
| Blue | 1.48 * | (1.17–1.89) | 1.06 | (0.80–1.41) | |
| Inoccupation | 0.72 * | (0.57–0.91) | 1.00 | (0.83–1.20) | |
| Current drinking status | |||||
| Never | 1.00 | 1.00 | |||
| Monthly | 0.92 | (0.74–1.14) | 1.24 * | (1.07–1.43) | |
| Weekly | 1.21 | (0.95–1.55) | 1.17 | (0.95–1.45) | |
| Physical activity | |||||
| Adequate | 1.00 | 1.00 | |||
| Inadequate | 1.03 | (0.87–1.22) | 1.04 | (0.90–1.21) | |
| Teeth Brushing Frequency | |||||
| ≤1 | 1.17 | (0.87–1.57) | 1.57 * | (1.03–2.39) | |
| 2 | 1.21 * | (1.02–1.43) | 1.02 | (0.88–1.17) | |
| ≥3 | 1.00 | 1.00 | |||
| Dental checkup status | |||||
| No | 1.62 * | (1.36–1.93) | 1.60 * | (1.39–1.84) | |
| Yes | 1.00 | 1.00 | |||
| Variables | Community Periodontal Index (CPI) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Male | Female | |||||||||
| Non | Ex-Smoker | Current Smoker | Non | Ex-Smoker | Current Smoker | |||||
| OR | OR | 95% CIs | OR | 95% CIs | OR | OR | 95% CIs | OR | 95% CIs | |
| Age | ||||||||||
| 20–29 | 1.00 | 1.10 | (0.63–1.92) | 1.82 * | (1.16–2.86) | 1.00 | 0.83 | (0.45–1.55) | 0.87 | (0.41–1.83) |
| 30–39 | 1.00 | 1.40 | (0.85–2.31) | 1.78 * | (1.16–2.73) | 1.00 | 1.23 | (0.76–2.00) | 2.73 * | (1.45–5.17) |
| 40–49 | 1.00 | 1.31 | (0.84–2.04) | 2.21 * | (1.37–3.29) | 1.00 | 1.34 | (0.74–2.42) | 1.37 | (0.72–2.61) |
| 50–59 | 1.00 | 0.88 | (0.49–1.57) | 1.34 | (0.72–2.48) | 1.00 | 1.88 | (0.72–4.92) | 1.62 | (0.64–4.10) |
| 60–69 | 1.00 | 1.38 | (0.75–2.54) | 2.57 * | (1.10–6.03) | 1.00 | 0.98 | (0.32–1.71) | 1.76 | (0.36–8.70) |
| ≥70 | 1.00 | 1.59 | (0.68–3.71) | 2.71 | (0.68–10.71) | 1.00 | 3.56 | (0.45–28.27) | - | - |
| Marital status | ||||||||||
| Married | 1.00 | 1.26 | (0.96–1.65) | 1.91 * | (1.44–2.53) | 1.00 | 1.18 | (0.81–1.72) | 1.51 | (0.81–1.72) |
| Divorced | 1.00 | 0.07 * | (0.01–0.89) | 0.06 | (0.00–1.32) | 1.00 | 0.90 | (0.34–2.35) | 4.44 * | (1.49–13.27) |
| Single | 1.00 | 1.06 | (0.65–1.72) | 1.70 * | (1.18–2.43) | 1.00 | 1.14 | (0.70–1.86) | 1.07 | (0.61–1.87) |
| Educational level | ||||||||||
| Middle school | 1.00 | 1.70 | (0.87–3.30) | 3.15 * | (1.37–7.21) | 1.00 | 1.12 | (0.43–2.90) | 11.40 * | (2.93–44.45) |
| High school | 1.00 | 1.21 | (0.83–1.77) | 1.67 * | (1.14–2.44) | 1.00 | 1.14 | (0.68–1.93) | 1.25 | (0.77–2.03) |
| College | 1.00 | 1.14 | (0.85–1.52) | 1.76 * | (1.34–2.32) | 1.00 | 1.19 | (0.80–1.77) | 1.13 | (0.66–1.93) |
| Household income | ||||||||||
| Low | 1.00 | 0.78 | (0.37–1.67) | 1.95 | (0.84–4.55) | 1.00 | 1.28 | (0.44–3.72) | 2.73 | (0.95–7.87) |
| Mid-low | 1.00 | 1.38 * | (1.47–4.45) | 2.56 * | (1.47–4.47) | 1.00 | 1.45 | (0.83–2.54) | 1.61 | (0.85–3.05) |
| Mid-high | 1.00 | 1.17 | (0.78–1.74) | 1.82 * | (1.22–2.71) | 1.00 | 1.16 | (0.72–1.88) | 1.27 | (0.72–2.27) |
| High | 1.00 | 1.19 | (0.85–1.68) | 1.51 * | (1.09–2.11) | 1.00 | 1.04 | (0.61–1.77) | 1.14 | (0.60–2.17) |
| Region | ||||||||||
| Metropolitan | 1.00 | 1.39 * | (1.00–1.95) | 2.16 * | (1.57–2.95) | 1.00 | 1.19 | (0.80–1.77) | 0.95 | (0.59–1.55) |
| Urban | 1.00 | 1.22 | (0.88–1.70) | 1.75 * | (1.24–2.47) | 1.00 | 1.18 | (0.76–1.86) | 2.24 * | (1.32–3.80) |
| Rural | 1.00 | 0.43 | (0.19–1.00) | 0.74 | (0.35–1.59) | 1.00 | 1.19 | (0.32–4.40) | 1.48 | (0.67–3.29) |
| Perceived stress level | ||||||||||
| Low | 1.00 | 1.41 | (0.82–2.42) | 4.02 * | (1.96–8.27) | 1.00 | 1.52 | (0.59–3.91) | 1.96 | (0.63–6.12) |
| Mid-low | 1.00 | 1.16 | (0.87–1.54) | 1.72 * | (1.29–2.31) | 1.00 | 1.17 | (0.78–1.76) | 1.48 | (0.93–2.36) |
| Mid-high | 1.00 | 1.28 | (0.79–2.06) | 1.87 * | (1.18–2.96) | 1.00 | 1.18 | (0.64–2.19) | 1.25 | (0.70–2.23) |
| High | 1.00 | 0.55 | (0.13–2.37) | 0.75 | (0.23–2.43) | 1.00 | 0.93 | (0.40–2.16) | 1.29 | (0.51–3.27) |
| Occupational categories | ||||||||||
| White | 1.00 | 1.19 | (0.86–1.63) | 1.68 * | (1.21–2.33) | 1.00 | 1.21 | (0.76–1.93) | 1.23 | (0.64–2.38) |
| Pink | 1.00 | 0.72 | (0.33–1.54) | 1.29 | (0.71–2.36) | 1.00 | 0.95 | (0.46–1.97) | 1.57 | (0.79–3.12) |
| Blue | 1.00 | 1.08 | (0.71–1.65) | 1.80 * | (1.16–2.80) | 1.00 | 0.65 | (0.23–1.82) | 2.92 * | (1.07–1.82) |
| Inoccupation | 1.00 | 1.57 | (0.99–2.48) | 2.10 * | (1.28–3.43) | 1.00 | 1.44 | (0.91–2.28) | 1.26 | (0.75–2.28) |
| Current drinking status | ||||||||||
| Never | 1.00 | 1.48 | (0.98–2.23) | 1.90 * | (1.23–2.94) | 1.00 | 1.22 | (0.74–2.01) | 1.84 * | (1.01–3.38) |
| Monthly | 1.00 | 1.27 | (0.92–1.76) | 1.88 * | (1.37–2.57) | 1.00 | 1.32 | (0.87–1.99) | 1.12 | (0.67–1.89) |
| Weekly | 1.00 | 0.87 | (0.56–1.36) | 1.45 | (0.95–2.21) | 1.00 | 1.09 | (0.59–2.11) | 1.59 | (0.95–2.66) |
| Physical activity | ||||||||||
| Adequate | 1.00 | 1.12 | (0.83–1.50) | 1.83 * | (1.35–2.50) | 1.00 | 0.97 | (0.66–1.43) | 1.11 | (0.68–1.81) |
| Inadequate | 1.00 | 1.32 | (0.96–1.82) | 1.77 * | (1.30–2.42) | 1.00 | 1.43 | (0.96–2.21) | 1.88 * | (1.26–2.79) |
| Teeth Brushing Frequency | ||||||||||
| ≤1 | 1.00 | 1.12 | (0.52–2.39) | 1.32 | (0.62–2.84) | 1.00 | 4.59 | (0.64–32.98) | 3.18 | (0.59–17.18) |
| 2 | 1.00 | 1.52 * | (1.04–2.22) | 1.41 * | (1.48–3.05) | 1.00 | 1.26 | (0.83–1.92) | 1.21 | (0.71–2.05) |
| ≥3 | 1.00 | 1.05 | (0.77–1.42) | 1.70 * | (1.26–2.29) | 1.00 | 1.16 | (0.81–1.65) | 1.65 * | (1.08–2.51) |
| Dental checkup status | ||||||||||
| No | 1.00 | 1.06 | (0.79–1.43) | 1.73 * | (1.29–2.33) | 1.00 | 1.05 | (0.74–1.48) | 1.95 * | (1.29–2.95) |
| Yes | 1.00 | 1.39 * | (1.01–1.91) | 1.90 * | (1.40–2.59) | 1.00 | 1.57 * | (1.02–2.42) | 0.82 | (0.48–1.38) |
| Variables | Community Periodontal Index (CPI) | ||||
|---|---|---|---|---|---|
| Male | Female | ||||
| OR | 95% CIs | OR | 95% CIs | ||
| Pack-Years | |||||
| Non-smoker | 1.00 | 1.00 | |||
| Pack Years < 5 | 1.11 | (0.87–1.42) | 1.16 | (0.90–1.50) | |
| 5 ≤ Pack Years < 10 | 1.75 * | (1.34–2.27) | 1.71 | (0.94–3.13) | |
| 10 ≤ Pack Years < 15 | 1.47 * | (1.10–2.27) | 1.47 | (0.72–3.00) | |
| 15 ≤ Pack Years < 20 | 1.80 * | (1.27–2.56) | 1.96 | (0.62–6.18) | |
| 20 ≤ Pack Years | 1.84 * | (1.38–2.47) | 2.69 | (0.90–8.05) | |
| Smoking Cessation Status | |||||
| Non-smoker | 1.00 | 1.00 | |||
| Ex-smoker (5 yr. > Cessation) | 1.42 * | (1.04–1.96) | 1.11 * | (1.71–1.74) | |
| Ex-smoker (5 yr. ≤ Cessation < 10 yr.) | 1.69 * | (1.16–2.47) | 1.07 | (0.61–1.87) | |
| Ex-smoker (10 yr. ≤ Cessation) | 0.93 | (0.71–1.21) | 1.32 | (0.81–2.14) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sim, K.-Y.; Jang, Y.S.; Jang, Y.S.; Nerobkova, N.; Park, E.-C. Association between Smoking and Periodontal Disease in South Korean Adults. Int. J. Environ. Res. Public Health 2023, 20, 4423. https://doi.org/10.3390/ijerph20054423
Sim K-Y, Jang YS, Jang YS, Nerobkova N, Park E-C. Association between Smoking and Periodontal Disease in South Korean Adults. International Journal of Environmental Research and Public Health. 2023; 20(5):4423. https://doi.org/10.3390/ijerph20054423
Chicago/Turabian StyleSim, Ka-Yun, Yun Seo Jang, Ye Seul Jang, Nataliya Nerobkova, and Eun-Cheol Park. 2023. "Association between Smoking and Periodontal Disease in South Korean Adults" International Journal of Environmental Research and Public Health 20, no. 5: 4423. https://doi.org/10.3390/ijerph20054423
APA StyleSim, K.-Y., Jang, Y. S., Jang, Y. S., Nerobkova, N., & Park, E.-C. (2023). Association between Smoking and Periodontal Disease in South Korean Adults. International Journal of Environmental Research and Public Health, 20(5), 4423. https://doi.org/10.3390/ijerph20054423