
Hepatitis B Virus in West African Children: Systematic Review and Meta-Analysis of HIV and Other Factors Associated with Hepatitis B Infection

 , , , , ,
, , , , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Inclusion Criteria and Exclusion Reasons
2.2. Data Sources and Study Screening Strategies
2.3. Description of the Study Area
2.4. Data Extraction
2.5. Quality Assessment
2.6. Data Analysis
3. Results
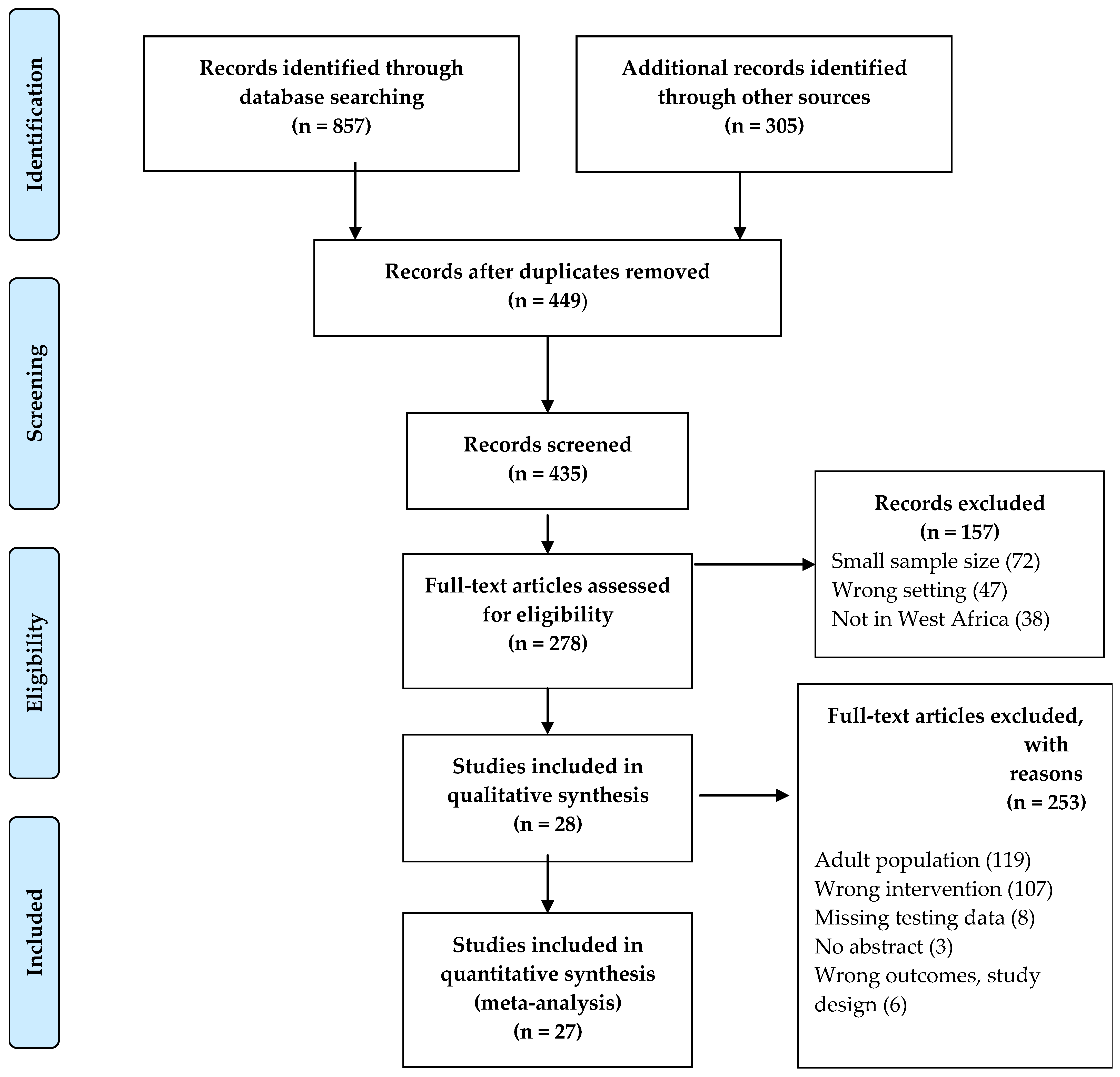
3.1. Study Selection
3.2. Characteristics of the Systematic Review Studies
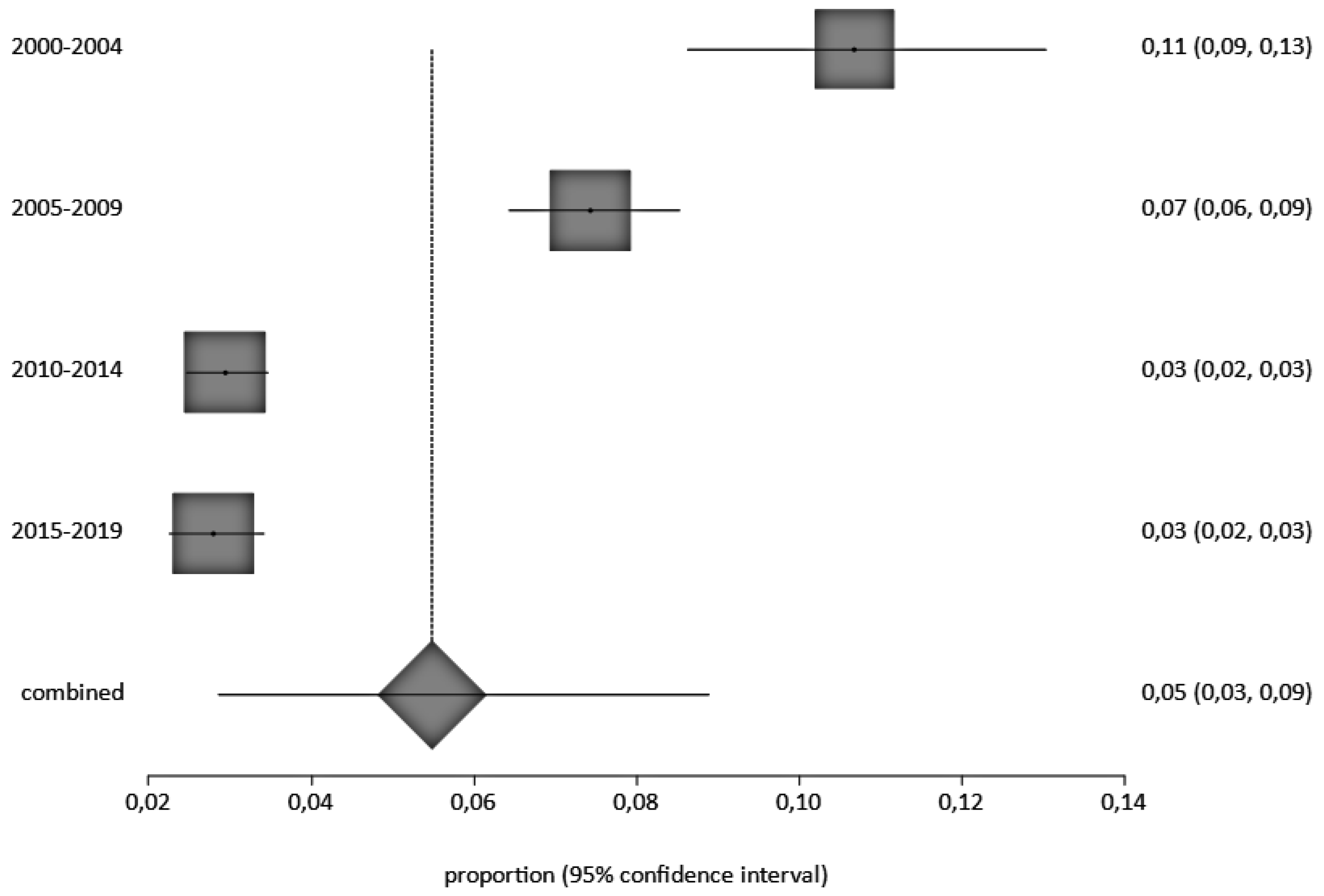
3.3. Overall Pooled HBV Prevalence in Children in West Africa and Publication Bias
3.4. Sensitivity Analysis
3.5. HBV Prevalence in Children with or without Risk Factors
3.6. Risk Factors of HBV Infection in Children
3.7. HBV Prevalence in Hospital and Community Settings
3.8. HBV Prevalence by HIV Status in Children
HBV Prevalence among Vaccinated and Unvaccinated Children
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Progress Report on HIV, Viral Hepatitis and Sexually Transmitted Infections, 2021: Accountability for the Global Health Sector Strategies 2016–2021: Actions for Impact: Web Annex 2: Data Methods; WHO: Geneva, Switzerland, 2021.
- Edmunds, W.J.; Medley, G.F.; Nokes, D.J.; Hall, A.J.; Whittle, H.C. The Influence of Age on the Development of the Hepatitis B Carrier State. Proc. Biol. Sci. 1993, 253, 197–201. [Google Scholar] [CrossRef] [PubMed]
- Hussein, M.K.; Dorothy, N.; Ponsiano, O.; Ali, K.; Abdul, W.; Hakim, S. Prevalence and Predictors of Hepatitis B Virus (HBV) Infection in East Africa: Evidence from a Systematic Review and Meta-Analysis of Epidemiological Studies Published from 2005 to 2020. Arch. Public Health 2021, 79, 167. [Google Scholar]
- Baumberger, S. Prevention of Mother to Child Transmission of Hepatitis B: A Global Challenge. Master’s Thesis, UiT Norges Arktiske Universitet, Tromsø, Norway, 2016. [Google Scholar]
- Razavi-Shearer, D.; Gamkrelidze, I.; Nguyen, M.H.; Chen, D.-S.; Van Damme, P.; Abbas, Z.; Abdulla, M.; Abou Rached, A.; Adda, D.; Aho, I.; et al. Global Prevalence, Treatment, and Prevention of Hepatitis B Virus Infection in 2016: A Modelling Study. Lancet Gastroenterol. Hepatol. 2018, 3, 383–403. [Google Scholar] [CrossRef] [PubMed]
- Platt, L.; French, C.E.; McGowan, C.R.; Sabin, K.; Gower, E.; Trickey, A.; McDonald, B.; Ong, J.; Stone, J.; Easterbrook, P.; et al. Prevalence and Burden of HBV Co-Infection among People Living with HIV: A Global Systematic Review and Meta-Analysis. J. Viral Hepat. 2020, 27, 294–315. [Google Scholar] [CrossRef] [PubMed]
- Coffie, P.A.; Patassi, A.; Doumbia, A.; Bado, G.; Messou, E.; Minga, A.; Allah-Kouadio, E.; Zannou, D.M.; Seydi, M.; Kakou, A.R.; et al. Changes in Viral Hepatitis B Screening Practices over Time in West African HIV Clinics. Med. Mal. Infect. 2017, 47, 394–400. [Google Scholar] [CrossRef]
- Zampino, R.; Boemio, A.; Sagnelli, C.; Alessio, L.; Adinolfi, L.E.; Sagnelli, E.; Coppola, N. Hepatitis B Virus Burden in Developing Countries. World J. Gastroenterol. 2015, 21, 11941–11953. [Google Scholar] [CrossRef]
- HIV/AIDS (UNAIDS), J.U.N.P. on Global HIV & AIDS Statistics-2019 Fact Sheet, 2019. Available online: https://www.unaids.org/sites/default/files/media_asset/2019-UNAIDS-data_en.pdf (accessed on 28 December 2022).
- McMahon, B.J. The Natural History of Chronic Hepatitis B Virus Infection. Hepatology 2009, 49, S45–S55. [Google Scholar] [CrossRef]
- Shimakawa, Y.; Yan, H.-J.; Tsuchiya, N.; Bottomley, C.; Hall, A.J. Association of Early Age at Establishment of Chronic Hepatitis B Infection with Persistent Viral Replication, Liver Cirrhosis and Hepatocellular Carcinoma: A Systematic Review. PLoS ONE 2013, 8, e69430. [Google Scholar] [CrossRef]
- Larouze, B.; Saimot, G.; Lustbader, E.D.; London, W.T.; Werner, B.G.; Payet, M.; Blumberg, B.S. Host Responses to Hepatitis-B Infection in Patients with Primary Hepatic Carcinoma and Their Families: A Case/Control Study in Senegal, West Africa. Lancet 1976, 308, 534–538. [Google Scholar] [CrossRef]
- Sadoh, A.E.; Sadoh, W.E.; Iduoriyekemwen, N.J. HIV Co-Infection with Hepatitis B and C Viruses among Nigerian Children in an Antiretroviral Treatment Programme. S. Afr. J. Child Health 2011, 5, 7–10. [Google Scholar]
- Wen, W.-H.; Lai, M.-W.; Chang, M.-H. A Review of Strategies to Prevent Mother-to-Infant Transmission of Hepatitis B Virus Infection. Expert Rev. Gastroenterol. Hepatol. 2016, 10, 317–330. [Google Scholar] [CrossRef]
- Beasley, R.P.; Trepo, C.; Stevens, C.E.; Szmuness, W. The e Antigen and Vertical Transmission of Hepatitis B Surface Antigen. Am. J. Epidemiol. 1977, 105, 94–98. [Google Scholar] [CrossRef]
- Kao, J.-H. Hepatitis B Vaccination and Prevention of Hepatocellular Carcinoma. Best Pract. Res. Clin. Gastroenterol. 2015, 29, 907–917. [Google Scholar] [CrossRef] [PubMed]
- Hepatitis B Vaccination|CDC. Available online: https://www.cdc.gov/vaccines/vpd/hepb/index.html (accessed on 4 December 2022).
- Covidence—Better Systematic Review Management. Available online: https://www.covidence.org/ (accessed on 4 December 2022).
- World Population to Reach 8 Billion This Year, as Growth Rate Slows. Available online: https://news.un.org/en/story/2022/07/1122272 (accessed on 28 December 2022).
- Abesig, J.; Chen, Y.; Wang, H.; Sompo, F.M.; Wu, I.X.Y. Prevalence of Viral Hepatitis B in Ghana between 2015 and 2019: A Systematic Review and Meta-Analysis. PLoS ONE 2020, 15, e0234348. [Google Scholar] [CrossRef]
- Proportion Meta-Analysis—StatsDirect. Available online: https://www.statsdirect.com/help/default.htm#meta_analysis/proportion.htm (accessed on 4 December 2022).
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring Inconsistency in Meta-Analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in Meta-Analysis Detected by a Simple, Graphical Test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Adoga, M.P.; Gyar, S.D.; Pechulano, S.; Bashayi, O.D.; Emiasegen, S.E.; Zungwe, T.; Iperepolu, O.H.; Agupugo, C.; Agwale, S.M. Hepatitis B Virus Infections in Apparently Healthy Urban Nigerians: Data from Pre-Vaccination Tests. J. Infect Dev. Ctries 2010, 4, 397–400. [Google Scholar] [CrossRef] [PubMed]
- Ouattara, A.; Assi, C.; Soro, D.; Allah-Kouadio, E.; Lohouès-Kouacou, M.J.; Camara, B.M. Seroprevalence of Viral Hepatitis Markers B in Secondary School in Abidjan: Advocacy for a Catch-up Vaccination. Open J. Gastroenterol. 2019, 9, 7. [Google Scholar] [CrossRef]
- Omeje, K.N.; Ibekwe, R.C.; Ojukwu, J.O.; Una, A.F.; Ibe, B.C. Risk Factors for Hepatitis B Surface Antigenaemia among Secondary School Students in Abakaliki, South Eastern Nigeria. Niger. J. Paediatr. 2017, 44, 14–21. [Google Scholar] [CrossRef]
- Bukbuk, D.N.; Denue, B.A.; Ngoshe, I.; Dawurung, J.; Oderinde, S. Hepatitis B Surface Antigenaemia among High Risk Groups in Northeastern Nigeria. Niger. Med. Pract. 2016, 69, 77–82. [Google Scholar] [CrossRef]
- Adeoye, O.A.; Oniyangi, O.; Ojuawo, I.A. Prevalence and Risk Factors of Hepatitis b Infection in HIV Infected Children Seen at National Hospital Abuja. Niger. J. Paediatr. 2021, 48, 62–65. [Google Scholar] [CrossRef]
- Anigilaje, E.A.; Olutola, A. Prevalence and Clinical and Immunoviralogical Profile of Human Immunodeficiency Virus-Hepatitis B Coinfection among Children in an Antiretroviral Therapy Programme in Benue State, Nigeria. Hindawi 2013, 2013, 7. [Google Scholar] [CrossRef]
- Barro, M.; Valea, D.; Ouermi, S.A.; Sessouma, S.; Sanogo, B.; Ouattara, I.A.B.; Ouedraogo, A.S.; Nacro, B.; Moyen, G. Serological Profile of Hepatitis B in Children after the Introduction of Its Vaccination in Burkina Faso. Pediatr. Rep. 2019, 11, 75–77. [Google Scholar] [CrossRef] [PubMed]
- d’Almeida, M.; Adedemy, J.D.; Agossou, J.; Noudamadjo, A.; Agossou, C.; Agossou, R.; Koumakpai-Adeothy, S. Frequency of HIV and Viral Hepatitis B Co-Infection in Children Aged 1 to 15 Years Attended in a Hospital Environment in Parakou (Benin). Curr. Pediatr. Res. 2015, 19, 81–89. [Google Scholar]
- Ezeilo, M.C.; Engwa, G.A.; Iroha, R.I.; Odimegwu, D.C. Seroprevalence and Associated Risk Factors of Hepatitis B Virus Infection Among Children in Enugu Metropolis. Virol. Res. Treat. 2018, 9, 1–7. [Google Scholar] [CrossRef]
- Ikpeme, E.E.; Etukudo, O.M.; Ekrikpo, U.E. Seroprevalence of HBV and HIV Co-Infection in Children and Outcomes Following Highly Active Antiretroviral Therapy (HAART) in Uyo, South-South Nigeria. Afr. Health Sci. 2013, 13, 955–961. [Google Scholar] [CrossRef]
- Lô, G.; Sow-Sall, A.; Diop-Ndiaye, H.; Babacar, N.; Diouf, N.N.; Daffé, S.M.; Ndao, B.; Thiam, M.; Mbow, M.; Soumboundou, M.B.; et al. Hepatitis B Virus (HBV) Infection amongst Children in Senegal: Current Prevalence and Seroprotection Level. Pan. Afr. Med. J. 2019, 32, 140. [Google Scholar] [CrossRef] [PubMed]
- Alikor, E.A.; Erharbor, O.N. Seroprevalences of Hepatitus B Surface Antigenaemia in Children in a Tertiary Health Institution in the Niger Delta of Nigeria. Niger. J. Med. 2007, 16, 326–329. [Google Scholar] [CrossRef]
- Ekouevi, D.K.; Larrouy, L.; Gbeasor-Komlanvi, F.A.; Mackiewicz, V.; Tchankoni, M.K.; Bitty-Anderson, A.M.; Gnatou, G.Y.-S.; Sadio, A.; Salou, M.; Dagnra, C.A.; et al. Prevalence of Hepatitis B among Childbearing Women and Infant Born to HBV-Positive Mothers in Togo. BMC Infect. Dis. 2020, 20, 839. [Google Scholar] [CrossRef] [PubMed]
- Nacro, B.; Dao, B.; Dahourou, H. HBs Antigen in Children with Suspicion of HIV Infection. J. Trop. Pediatr. 2001, 47, 303–304. [Google Scholar] [CrossRef]
- Nwolisa, E.; Mbanefo, F.; Ezeogu, J.; Amadi, P. Prevalence of Hepatitis B Co-Infection amongst HIV Infected Children Attending a Care and Treatment Centre in Owerri, South-Eastern Nigeria. Pan. Afr. Med. J. 2013, 14, 89. [Google Scholar] [CrossRef] [PubMed]
- Toyé, R.M.; Cohen, D.; Pujol, F.H.; Sow-Sall, A.; Lô, G.; Hoshino, K.; Mizokami, M.; Zoulim, F.; Lemoine, M.; Touré-Kane, C.; et al. Hepatitis B Virus Genotype Study in West Africa Reveals an Expanding Clade of Subgenotype A4. Microorganisms 2021, 9, 623. [Google Scholar] [CrossRef] [PubMed]
- Ashir, G.M.; Rabasa, A.I.; Gofama, M.M.; Bukbuk, D.; Abubakar, H.; Farouk, G.A. Study of Hepatic Functions and Prevalence of Hepatitis B Surface Antigenaemia in Nigerian Children with Human Immunodeficiency Virus Infection. Niger. J. Med. 2009, 18, 260–262. [Google Scholar] [CrossRef] [PubMed]
- Apiung, T.; Ndanu, T.A.; Mingle, J.A.; Sagoe, K.W. Hepatitis B Virus Surface Antigen and Antibody Markers in Children at a Major Paediatric Hospital after the Pentavalent DTP-HBV-Hib Vaccination. Ghana Med. J. 2017, 51, 13–19. [Google Scholar] [CrossRef] [PubMed]
- Sadoh, A.E.; Ofili, A. Hepatitis B Infection among Nigerian Children Admitted to a Children’s Emergency Room. Afr. Health Sci. 2014, 14, 377–383. [Google Scholar] [CrossRef] [PubMed]
- Hagan, O.C.K.; Nsiah, P.; Obiri-Yeboah, D.; Yirdong, F.; Annan, I.; Eliason, S.; Nuvor, S.V. Impact of Universal Childhood Vaccination against Hepatitis B in Ghana: A Pilot Study. J. Public Health Afr. 2018, 9, 721. [Google Scholar] [CrossRef]
- Ba, A.; Ndiaye, F.K.; Djeng, Y.J.; Cames, C.; Diack, A.; N’diaye, O. Impact of Highly Active Antiretroviral Therapy on Chronic Hepatitis B Serological Markers among Senegalese HIV Co-Infected Children. Int. J. MCH AIDS 2019, 8, 131–137. [Google Scholar] [CrossRef]
- Quaye, T.; Narkwa, P.W.; Domfeh, S.A.; Kattah, G.; Mutocheluh, M. Immunosurveillance and Molecular Detection of Hepatitis B Virus Infection amongst Vaccinated Children in the West Gonja District in Savanna Region of Ghana. PLoS ONE 2021, 16, e0257103. [Google Scholar] [CrossRef] [PubMed]
- Gueye, S.B.; Diop-Ndiaye, H.; Lo, G.; Mintsa, S.; Guindo, I.; Dia, A.; Sow-Sall, A.; Gaye-Diallo, A.; Mboup, S.; Touré-Kane, C. HBV Carriage in Children Born from HIV-Seropositive Mothers in Senegal: The Need of Birth-Dose HBV Vaccination. J. Med. Virol. 2016, 88, 815–819. [Google Scholar] [CrossRef]
- Sanou, A.M.; Ilboudo, A.K.; Meda, C.Z.; Togozia, A.; Coulibaly, A.; Cisse, A.; Sagna, T.; Kania, D.; Tarnagda, Z. Hepatitis B Vaccination in Burkina Faso: Prevalence of HBsAg Carriage and Immune Response in Children in the Western Region. J. Infect. Dev. Ctries 2018, 12, 1002–1008. [Google Scholar] [CrossRef]
- Périères, L.; Protopopescu, C.; Lo, G.; Marcellin, F.; Ba, E.H.; Coste, M.; Touré Kane, C.; Diallo, A.; Sokhna, C.; Boyer, S.; et al. Sibling Status, Home Birth, Tattoos and Stitches Are Risk Factors for Chronic Hepatitis B Virus Infection in Senegalese Children: A Cross-Sectional Survey. J. Viral. Hepat. 2021, 28, 1515–1525. [Google Scholar] [CrossRef] [PubMed]
- Odusanya, O.O.; Alufohai, F.E.; Meurice, F.P.; Wellens, R.; Weil, J.; Ahonkhai, V.I. Prevalence of Hepatitis B Surface Antigen in Vaccinated Children and Controls in Rural Nigeria. Int. J. Infect. Dis. 2005, 9, 139–143. [Google Scholar] [CrossRef] [PubMed]
- Ikobah, J.; Okpara, H.; Elemi, I.; Ogarepe, Y.; Udoh, E.; Ekanem, E. The Prevalence of Hepatitis B Virus Infection in Nigerian Children Prior to Vaccine Introduction into the National Programme on Immunization Schedule. Pan. Afr. Med. J. 2016, 23, 128. [Google Scholar] [CrossRef] [PubMed]
- Ott, J.J.; Stevens, G.A.; Groeger, J.; Wiersma, S.T. Global Epidemiology of Hepatitis B Virus Infection: New Estimates of Age-Specific HBsAg Seroprevalence and Endemicity. Vaccine 2012, 30, 2212–2219. [Google Scholar] [CrossRef] [PubMed]
- Moturi, E.; Tevi-Benissan, C.; Hagan, J.E.; Shendale, S.; Mayenga, D.; Murokora, D.; Patel, M.; Hennessey, K.; Mihigo, R. Implementing a Birth Dose of Hepatitis B Vaccine in Africa: Findings from Assessments in 5 Countries. J. Immunol. Sci. 2018, 5, 31–40. [Google Scholar] [CrossRef]
- Schweitzer, A.; Horn, J.; Mikolajczyk, R.T.; Krause, G.; Ott, J.J. Estimations of Worldwide Prevalence of Chronic Hepatitis B Virus Infection: A Systematic Review of Data Published between 1965 and 2013. Lancet 2015, 386, 1546–1555. [Google Scholar] [CrossRef]
- Kafeero, H.M.; Ndagire, D.; Ocama, P.; Walusansa, A.; Sendagire, H. Sero-Prevalence of Human Immunodeficiency Virus-Hepatitis B Virus (HIV-HBV) Co-Infection among Pregnant Women Attending Antenatal Care (ANC) in Sub-Saharan Africa (SSA) and the Associated Risk Factors: A Systematic Review and Meta-Analysis. Virol. J. 2020, 17, 170. [Google Scholar] [CrossRef]
- World Health Organization. World Health Statistics 2021; World Health Organization: Geneva, Switzerland, 2021.
- Gupta, S.; Singh, S. Hepatitis B and C Virus Co-Infections in Human Immunodeficiency Virus Positive North Indian Patients. World J. Gastroenterol. 2006, 12, 6879–6883. [Google Scholar] [CrossRef]
- Mustapha, S.K.; Jibrin, Y.B. The Prevalence of Hepatitis B Surface Antigenaemia in Patients with Human Immunodeficiency Virus (HIV) Infection in Gombe, Nigeria. Ann. Afr. Med. 2004, 3, 10–12. [Google Scholar]
- Otegbayo, J.A.; Taiwo, B.O.; Akingbola, T.S.; Odaibo, G.N.; Adedapo, K.S.; Penugonda, S.; Adewole, I.F.; Olaleye, D.O.; Murphy, R.; Kanki, P. Prevalence of Hepatitis B and C Seropositivity in a Nigerian Cohort of HIV-Infected Patients. Ann. Hepatol. 2008, 7, 152–156. [Google Scholar] [CrossRef]
- Telatela, S.P.; Matee, M.I.; Munubhi, E.K. Seroprevalence of Hepatitis B and C Viral Co-Infections among Children Infected with Human Immunodeficiency Virus Attending the Paediatric HIV Care and Treatment Center at Muhimbili National Hospital in Dar-Es-Salaam, Tanzania. BMC Public Health 2007, 7, 338. [Google Scholar] [CrossRef]
- Peebles, K.; Nchimba, L.; Chilengi, R.; Bolton Moore, C.; Mubiana-Mbewe, M.; Vinikoor, M.J. Pediatric HIV–HBV Coinfection in Lusaka, Zambia: Prevalence and Short-Term Treatment Outcomes. J. Trop. Pediatr. 2015, 61, 464–467. [Google Scholar] [CrossRef]
- Rouet, F.; Chaix, M.-L.; Inwoley, A.; Anaky, M.-F.; Fassinou, P.; Kpozehouen, A.; Rouzioux, C.; Blanche, S.; Msellati, P.; Programme Enfant Yopougon (Agence Nationale de Recherches sur le SIDA et les Hépatites Virales B et C 1244/1278). Frequent Occurrence of Chronic Hepatitis B Virus Infection among West African HIV Type-1-Infected Children. Clin. Infect. Dis. 2008, 46, 361–366. [Google Scholar] [CrossRef]
- Ott, J.J.; Horn, J.; Krause, G.; Mikolajczyk, R.T. Time Trends of Chronic HBV Infection over Prior Decades—A Global Analysis. J. Hepatol. 2017, 66, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Boisson, A.; Goel, V.; Yotebieng, M.; Parr, J.B.; Fried, B.; Thompson, P. Implementation Approaches for Introducing and Overcoming Barriers to Hepatitis B Birth-Dose Vaccine in Sub-Saharan Africa. Glob. Health Sci Pract. 2022, 10, e2100277. [Google Scholar] [CrossRef] [PubMed]
- Whittle, H.; Jaffar, S.; Wansbrough, M.; Mendy, M.; Dumpis, U.; Collinson, A.; Hall, A. Observational Study of Vaccine Efficacy 14 Years after Trial of Hepatitis B Vaccination in Gambian Children. BMJ 2002, 325, 569. [Google Scholar] [CrossRef] [PubMed]
- Reda, A.A.; Arafa, M.A.; Youssry, A.A.; Wandan, E.H.; Ab de Ati, M.; Daebees, H. Epidemiologic Evaluation of the Immunity against Hepatitis B in Alexandria, Egypt. Eur. J. Epidemiol. 2003, 18, 1007–1011. [Google Scholar] [CrossRef]
- Sellier, P.O.; Maylin, S.; Berçot, B.; Chopin, D.; Lopes, A.; Simoneau, G.; Evans, J.; Delcey, V.; Bénifla, J.-L.; Simon, F. Prospective Interventional Study of Tenofovir in Pregnancy to Prevent Vertical Transmission of Hepatitis B in Highly Viremic Women. Eur. J. Gastroenterol. Hepatol. 2017, 29, 259–263. [Google Scholar] [CrossRef]
- World Health Organization. Hepatitis B Vaccines: WHO Position Paper—July 2017. Wkly. Epidemiol. Rec. 2017, 92, 369–392. [Google Scholar]
- Howell, J.; Lemoine, M.; Thursz, M. Prevention of Materno-Foetal Transmission of Hepatitis B in Sub-Saharan Africa: The Evidence, Current Practice and Future Challenges. J. Viral. Hepat. 2014, 21, 381–396. [Google Scholar] [CrossRef]
- 85% of Africans Live on Less than $5.50 per Day. Available online: https://blogs.worldbank.org/opendata/85-africans-live-less-550-day (accessed on 4 December 2022).
- Immunization Coverage. Available online: https://www.who.int/news-room/fact-sheets/detail/immunization-coverage (accessed on 17 February 2023).
- Muhoza, P. Routine Vaccination Coverage—Worldwide, 2020. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1495. [Google Scholar] [CrossRef] [PubMed]
- Introduction of HepB Birth Dose. Available online: https://immunizationdata.who.int/pages/vaccine-intro-by-antigen/hepb_bd.html?ISO_3_CODE=&YEAR= (accessed on 17 February 2023).
- Ekra, D.; Herbinger, K.H.; Konate, S.; Leblond, A.; Fretz, C.; Cilote, V.; Douai, C.; Da Silva, A.; Gessner, B.D.; Chauvin, P. A Non-Randomized Vaccine Effectiveness Trial of Accelerated Infant Hepatitis B Immunization Schedules with a First Dose at Birth or Age 6 Weeks in Côte d’Ivoire. Vaccine 2008, 26, 2753–2761. [Google Scholar] [CrossRef] [PubMed]
- Shimakawa, Y.; Veillon, P.; Birguel, J.; Pivert, A.; Sauvage, V.; Guillou-Guillemette, H.L.; Roger, S.; Njouom, R.; Ducancelle, A.; Amta, P.; et al. Residual Risk of Mother-to-Child Transmission of Hepatitis B Virus Infection despite Timely Birth-Dose Vaccination in Cameroon (ANRS 12303): A Single-Centre, Longitudinal Observational Study. Lancet Glob Health 2022, 10, e521–e529. [Google Scholar] [CrossRef] [PubMed]
- Ni, Y.-H.; Chen, D.-S. Hepatitis B Vaccination in Children: The Taiwan Experience. Pathol. Biol. 2010, 58, 296–300. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Li, M.; Hutton, D.W.; Wagner, A.L.; Yao, Y.; Zhu, W.; Cao, L.; Tang, S.; Pan, J.; Wang, Y.; et al. Impact of the National Hepatitis B Immunization Program in China: A Modeling Study. Infect. Dis. Poverty 2022, 11, 106. [Google Scholar] [CrossRef] [PubMed]
- Posuwan, N.; Wanlapakorn, N.; Sa-nguanmoo, P.; Wasitthankasem, R.; Vichaiwattana, P.; Klinfueng, S.; Vuthitanachot, V.; Sae-lao, S.; Foonoi, M.; Fakthongyoo, A.; et al. The Success of a Universal Hepatitis B Immunization Program as Part of Thailand’s EPI after 22 Years’ Implementation. PLoS ONE 2016, 11, e0150499. [Google Scholar] [CrossRef] [PubMed]
- Charles, R.; Vallée, J.; Tissot, C.; Lucht, F.; Botelho-Nevers, E. Vaccination Errors in General Practice: Creation of a Preventive Checklist Based on a Multimodal Analysis of Declared Errors. Fam. Pract. 2016, 33, 432–438. [Google Scholar] [CrossRef] [PubMed]
- Elsheikh, R.M.; Daak, A.A.; Elsheikh, M.A.; Karsany, M.S.; Adam, I. Hepatitis B Virus and Hepatitis C Virus in Pregnant Sudanese Women. Virol. J. 2007, 4, 104. [Google Scholar] [CrossRef]
- Chen, H.-L.; Zha, M.-L.; Cai, J.-Y.; Qin, G. Maternal Viral Load and Hepatitis B Virus Mother-to-Child Transmission Risk: A Systematic Review and Meta-Analysis. Hepatol. Res. 2018, 48, 788–801. [Google Scholar] [CrossRef]
- Akinbodewa, A.A.; Gbadegesin, B.A.; Adejumo, O.A.; Ahmed, S.D.; Uwameiye, O.; Dada, S.A.; Okunola, O.; Osho, P.O. A Multicentre Study of Awareness and Practice of Vaccination Against Infectious Diseases Among Haemo-Dialysis Subjects in Nigeria. West Afr. J. Med. 2019, 36, 239–245. [Google Scholar]
- Pan, C.Q.; Duan, Z.; Dai, E.; Zhang, S.; Han, G.; Wang, Y.; Zhang, H.; Zou, H.; Zhu, B.; Zhao, W.; et al. Tenofovir to Prevent Hepatitis B Transmission in Mothers with High Viral Load. N. Engl. J. Med. 2016, 374, 2324–2334. [Google Scholar] [CrossRef] [PubMed]
- Yazie, T.D.; Tebeje, M.G. An Updated Systematic Review and Meta-Analysis of the Prevalence of Hepatitis B Virus in Ethiopia. BMC Infect. Dis. 2019, 19, 917. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Men, P.; Xiao, Y.; Gao, P.; Lv, M.; Yuan, Q.; Chen, W.; Bai, S.; Wu, J. Hepatitis B Infection in the General Population of China: A Systematic Review and Meta-Analysis. BMC Infect. Dis. 2019, 19, 811. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1st Author [Reference] | Study Setting | Study Year | Publication Year | Country | Study Type | Sample Size | Number AgHBs+ | Prevalence of AgHB+ (%) | Diagnostic Method | Sample Type | Score Quality |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Studies in Hospital Settings | |||||||||||
| Adeoye OA [28] | Urban | 2012 | 2021 | Nigeria | Cross-sectional | 261 | 3 | 1.1 | ELISA | SERA | 7 |
| Anigilaje EA [29] | Urban | 2008–2012 | 2013 | Nigeria | Cross-sectional | 395 | 31 | 7.8 | ELISA | SERA | 10 |
| Barro M [30] | Urban | 2013 | 2019 | Burkina Faso | Cohort | 2015 | 53 | 2.6 | ELISA | PLASMA | 9 |
| d’Almeida M [31] | Urban | 2014 | 2015 | Benin | Cross-sectional | 104 | 10 | 9.6 | RDT | PLASMA | 9 |
| Ezeilo MC [32] | Urban | 2017 | 2018 | Nigeria | Cross-sectional | 270 | 31 | 22.5 | ELISA | PLASMA | 7 |
| Ikpeme EE [33] | Urban | 2010–2011 | 2013 | Nigeria | Cohort | 166 | 10 | 6.0 | ELISA | SERA | 9 |
| Bukbuk DN [27] | Urban | 2009–2010 | 2016 | Nigeria | Cohort | 177 | 44 | 24.9 | ELISA | SERA | 6 |
| LO G [34] | Urban | 2016 | 2019 | Senegal | Cross-sectional | 295 | 3 | 1.1 | ELISA | SERA | 9 |
| Edward AD [35] | Urban | 2004 | 2007 | Nigeria | Retrospective | 251 | 31 | 12 | ELISA | SERA | 7 |
| Ekouevi DK [36] | Urban | 2017 | 2020 | Togo | Cross-sectional | 210 | 3 | 1.3 | RDT | SERA | 7 |
| Nacro B [37] | Urban | 2001 | 2001 | Burkina Faso | Cross-sectional | 103 | 41 | 39.8 | RDT | SERA | 8 |
| Nwolisa E [38] | Urban | 2010 | 2013 | Nigeria | Cross-sectional | 139 | 8 | 5.8 | RDT | SERA | 6 |
| Toyé RM [39] | Urban | 2015 | 2021 | Senegal | Retrospective | 613 | 25 | 4.1 | RDT | SERA | 8 |
| Ashir GM [40] | Urban | 2007 | 2009 | Nigeria | Cross-sectional | 284 | 54 | 2.8 | ELISA | SERA | 7 |
| Apiung T [41] | Urban | 2012–2013 | 2017 | Ghana | Cross-sectional | 424 | 3 | 0.05 | ELISA | PLASMA | 7 |
| Sadoh AE [42] | Urban | 2011 | 2014 | Nigeria | Cross-sectional | 150 | 21 | 13.9 | ELISA | SERA | 8 |
| Hagan OCK [43] | Urban | 2012–2013 | 2018 | Ghana | Cross-sectional | 387 | 11 | 2.8 | ELISA | SERA | 7 |
| Ba A [44] | Urban | 2013–2015 | 2018 | Senegal | Cross-sectional | 252 | 7 | 2.8 | ELISA | SERA | 7 |
| Quaye T [45] | Urban | 2019 | 2021 | Ghana | Cross-sectional | 350 | 5 | 1.4 | ELISA | SERA | 8 |
| Studies in Community Settings | |||||||||||
| Gueye SB [46] | Urban | 2007–2012 | 2016 | Senegal | Retrospective | 930 | 28 | 3.0 | ELISA | TOTAL BLOOD | 7 |
| Omeje KN [26] | Urban | 2010–2011 | 2017 | Nigeria | Cross-sectional | 208 | 6 | 2.8 | RDT | SERA | 5 |
| Sanou AM [47] | Rural | 2015 | 2018 | Burkina Faso | Cross-sectional | 265 | 9 | 3.4 | RDT | SERA | 6 |
| Périères L [48] | Rural | 2018–2019 | 2021 | Senegal | Cross-sectional | 1327 | 17 | 1.2 | ELISA | SERA | 10 |
| Ouattara A [25] | Urban | 2006 | 2019 | Cote d’Ivoire | Cross-sectional | 282 | 15 | 5.3 | ELISA | SERA | 9 |
| Odusanya OO [49] | Rural/Urban | 2001 | 2005 | Nigeria | Case control | 223 | 3 | 1.2 | ELISA | SERA | 8 |
| Odusanya OO [49] | Rural/Urban | 2001 | 2005 | Nigeria | Case control | 219 | 10 | 4.6 | ELISA | SERA | 8 |
| Ikobah J [50] | Urban | 2014 | 2016 | Nigeria | Cross-sectional | 595 | 6 | 0.6 | RDT | SERA | 7 |
| Adoga, MP [24] | Urban | 2008–2009 | 2010 | Nigeria | Cohort | 409 | 12 | 2.9 | ELISA | SERA/PLASMA | 8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fofana, D.B.; Somboro, A.M.; Maiga, M.; Kampo, M.I.; Diakité, B.; Cissoko, Y.; McFall, S.M.; Hawkins, C.A.; Maiga, A.I.; Sylla, M.; et al. Hepatitis B Virus in West African Children: Systematic Review and Meta-Analysis of HIV and Other Factors Associated with Hepatitis B Infection. Int. J. Environ. Res. Public Health 2023, 20, 4142. https://doi.org/10.3390/ijerph20054142
Fofana DB, Somboro AM, Maiga M, Kampo MI, Diakité B, Cissoko Y, McFall SM, Hawkins CA, Maiga AI, Sylla M, et al. Hepatitis B Virus in West African Children: Systematic Review and Meta-Analysis of HIV and Other Factors Associated with Hepatitis B Infection. International Journal of Environmental Research and Public Health. 2023; 20(5):4142. https://doi.org/10.3390/ijerph20054142
Chicago/Turabian StyleFofana, Djeneba B., Anou M. Somboro, Mamoudou Maiga, Mamadou I. Kampo, Brehima Diakité, Yacouba Cissoko, Sally M. McFall, Claudia A. Hawkins, Almoustapha I. Maiga, Mariam Sylla, and et al. 2023. "Hepatitis B Virus in West African Children: Systematic Review and Meta-Analysis of HIV and Other Factors Associated with Hepatitis B Infection" International Journal of Environmental Research and Public Health 20, no. 5: 4142. https://doi.org/10.3390/ijerph20054142
APA StyleFofana, D. B., Somboro, A. M., Maiga, M., Kampo, M. I., Diakité, B., Cissoko, Y., McFall, S. M., Hawkins, C. A., Maiga, A. I., Sylla, M., Gozlan, J., El-Sayed, M. H., Morand-Joubert, L., Murphy, R. L., Diakité, M., & Holl, J. L. (2023). Hepatitis B Virus in West African Children: Systematic Review and Meta-Analysis of HIV and Other Factors Associated with Hepatitis B Infection. International Journal of Environmental Research and Public Health, 20(5), 4142. https://doi.org/10.3390/ijerph20054142