
The Influence of Visual Input on Electromyographic Activity and Patterns of Masticatory and Cervical Spine Muscles in Emmetropic Caucasian Subjects by Gender

 ,
, 
 ,
,
Abstract
1. Introduction
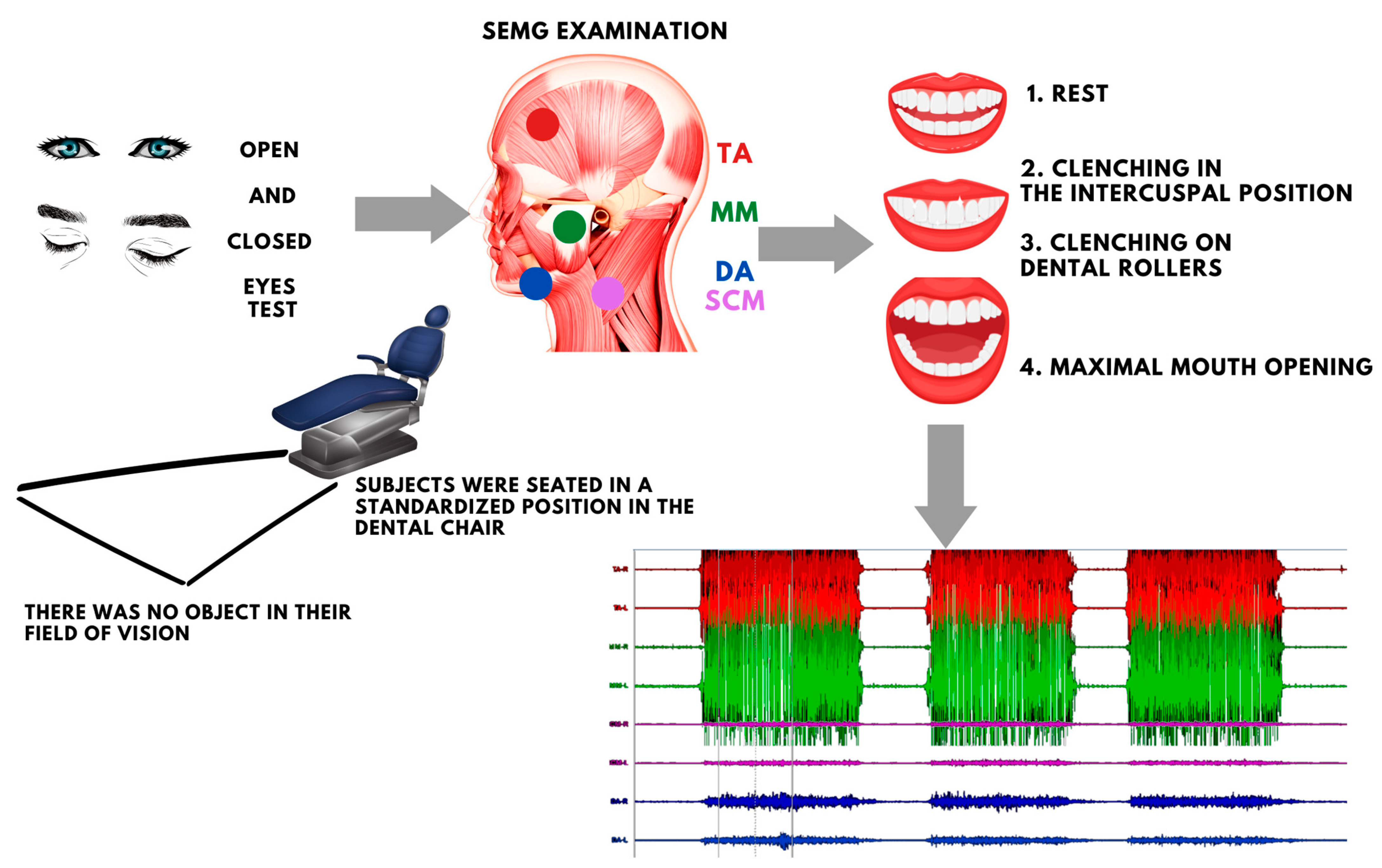
2. Materials and Methods
- no refractive error;
- no ocular and optic nerve diseases;
- absence of temporomandibular disorders according to the two-axis Research Diagnostic Criteria for Temporomandibular Disorders (RDC/TMD) [18];
- absence of musculoskeletal and connective tissue diseases and absence of myofascial trigger points as determined by the gold standard diagnostic criteria set by Travell and Simons [19] (within the temporalis muscle (TA), the masseter muscle (MM), the sternocleidomastoid muscle (SCM), the digastric muscle (DA), the upper part of the trapezius muscle),
- absence of malignancy (regardless of type and location);
- absence of metal implants (regardless of type and location).
- The exclusion criteria:
- intraocular pressure above 20 mmHg as determined by the Tono-Pen XL (Medtronic Solan, FL, USA) [7];
- no visual acuity of 1.0 as assessed by the Snellen chart on monocular examination [20];
- any malocclusion;
- oral inflammation;
- orthodontic treatment;
- race other than Caucasian;
- trauma and surgical treatment of the head and neck within the last 6 months.
- at rest (10 s);
- during maximal voluntary clenching in the intercuspal position (as hard as possible; 3 × 3 s, 2 s rest between);
- during maximal voluntary clenching on dental rollers (as hard as possible; 3 × 3 s, 2 s rest between);
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ludwig, P.E.; Jessu, R.; Czyz, C.N. Physiology, Eye. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- de Nava, A.S.L.; Somani, A.N.; Salini, B. Physiology, Vision. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Mohammed Dhaiban, T.S.; Ummer, F.P.; Khudadad, H.; Veettil, S.T. Types and Presentation of Refractive Error among Individuals Aged 0–30 Years: Hospital-Based Cross-Sectional Study, Yemen. Adv. Med. 2021, 2021, e5557761. [Google Scholar] [CrossRef]
- Zieliński, G.; Filipiak, Z.; Ginszt, M.; Matysik-Woźniak, A.; Rejdak, R.; Gawda, P. The Organ of Vision and the Stomatognathic System—Review of Association Studies and Evidence-Based Discussion. Brain Sci. 2021, 12, 14. [Google Scholar] [CrossRef]
- Zieliński, G.; Matysik-Woźniak, A.; Baszczowski, M.; Rapa, M.; Ginszt, M.; Zawadka, M.; Szkutnik, J.; Rejdak, R.; Gawda, P. Effects of Visual Input on Changes in the Bioelectrical Activity of the Cervical and Masticatory Muscles in Myopic Subjects. Sci. Rep. 2022, 12, 9435. [Google Scholar] [CrossRef]
- Zieliński, G.; Matysik-Woźniak, A.; Rapa, M.; Baszczowski, M.; Ginszt, M.; Zawadka, M.; Szkutnik, J.; Rejdak, R.; Gawda, P. The Influence of Visual Input on Electromyographic Patterns of Masticatory and Cervical Spine Muscles in Subjects with Myopia. J. Clin. Med. 2021, 10, 5376. [Google Scholar] [CrossRef]
- Zieliński, G.; Wójcicki, M.; Rapa, M.; Matysik-Woźniak, A.; Baszczowski, M.; Ginszt, M.; Litko-Rola, M.; Szkutnik, J.; Różyło-Kalinowska, I.; Rejdak, R.; et al. Masticatory Muscle Thickness and Activity Correlates to Eyeball Length, Intraocular Pressure, Retinal and Choroidal Thickness in Healthy Women versus Women with Myopia. J. Pers. Med. 2022, 12, 626. [Google Scholar] [CrossRef]
- Zieliński, G.; Baszczowski, M.; Rapa, M.; Matysik-Woźniak, A.; Zawadka, M.; Szkutnik, J.; Gawda, P.; Rejdak, R.; Majcher, P.; Ginszt, M. The Axial Length of the Eyeball and Bioelectrical Activity of Masticatory and Neck Muscles: A Preliminary Report. Pain Res. Manag. 2022, 2022, 6115782. [Google Scholar] [CrossRef] [PubMed]
- Ovenseri-Ogbomo, G.; Osuagwu, U.L.; Ekpenyong, B.N.; Agho, K.; Ekure, E.; Ndep, A.O.; Ocansey, S.; Mashige, K.P.; Naidoo, K.S.; Ogbuehi, K.C. Systematic Review and Meta-Analysis of Myopia Prevalence in African School Children. PLoS ONE 2022, 17, e0263335. [Google Scholar] [CrossRef] [PubMed]
- Widmalm, S.E.; Ericsson, S.G. The Influence of Eye Closure on Muscle Activity in the Anterior Temporal Region. J. Oral Rehabil. 1983, 10, 25–29. [Google Scholar] [CrossRef] [PubMed]
- Miralles, R.; Valenzuela, S.; Ramirez, P.; Santander, H.; Palazzi, C.; Ormeño, G.; Zúñiga, C. Visual Input Effect on EMG Activity of Sternocleidomastoid and Masseter Muscles in Healthy Subjects and in Patients with Myogenic Cranio-Cervical-Mandibular Dysfunction. Cranio J. Craniomandib. Pract. 1998, 16, 168–184. [Google Scholar] [CrossRef]
- Monaco, A.; Cattaneo, R.; Spadaro, A.; Giannoni, M.; Di Martino, S.; Gatto, R. Visual Input Effect on EMG Activity of Masticatory and Postural Muscles in Healthy and in Myopic Children. Eur. J. Paediatr. Dent. 2006, 7, 18–22. [Google Scholar]
- Spadaro, A.; Monaco, A.; Cattaneo, R.; Masci, C.; Gatto, R. Effect on Anterior Temporalis Surface EMG of Eyes Open-Closed Condition. Eur. J. Paediatr. Dent. 2010, 11, 210–212. [Google Scholar] [PubMed]
- Ciavarella, D.; Palazzo, A.; De Lillo, A.; Lo Russo, L.; Paduano, S.; Laino, L.; Chimenti, C.; Frezza, F.; Lo Muzio, L. Influence of Vision on Masticatory Muscles Function: Surface Electromyographic Evaluation. Ann. Stomatol. 2014, 5, 61–65. [Google Scholar] [CrossRef]
- Mazzetto, M.O.; Rodrigues, C.A.; Magri, L.V.; Melchior, M.O.; Paiva, G. Severity of TMD Related to Age, Sex and Electromyographic Analysis. Braz. Dent. J. 2014, 25, 54–58. [Google Scholar] [CrossRef]
- Llorente, L.; Barbero, S.; Cano, D.; Dorronsoro, C.; Marcos, S. Myopic versus Hyperopic Eyes: Axial Length, Corneal Shape and Optical Aberrations. J. Vis. 2004, 4, 5. [Google Scholar] [CrossRef] [PubMed]
- Meng, W.; Butterworth, J.; Malecaze, F.; Calvas, P. Axial Length of Myopia: A Review of Current Research. Ophthalmologica 2011, 225, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Osiewicz, M.; Lobbezoo, F.; Loster, B.; Wilkosz, M.; Naeije, M.; Ohrbach, R. Research Diagnostic Criteria for Temporomandibular Disorders (RDC/TMD)—The Polish Version of a Dual-Axis System for the Diagnosis of TMD.* RDC/TMD Form. Open J. Stomatol. 2013, 66, 576–649. [Google Scholar] [CrossRef]
- Simons, D.G.; Travell, J.G.; Simons, L.S. Travell & Simons’ Myofascial Pain and Dysfunction: Upper Half of Body; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 1999; Volume 1, pp. 371–384. ISBN 0-683-08363-5. [Google Scholar]
- Azzam, D.; Ronquillo, Y. Snellen Chart. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Zieliński, G.; Baszczowski, M.; Ginszt, M.; Rapa, M.; Matysik-Woźniak, A.; Szkutnik, J.; Rejdak, R.; Gawda, P. Analysis of Changes in Electromyographic Masticatory Muscle Activity in Relation to the Selected Correction of Refractive Error. Ann. Agric. Environ. Med. 2022, 3, 457–462. [Google Scholar] [CrossRef]
- Hermens, H.J.; Freriks, B.; Disselhorst-Klug, C.; Rau, G. Development of Recommendations for SEMG Sensors and Sensor Placement Procedures. J. Electromyogr. Kinesiol. 2000, 10, 361–374. [Google Scholar] [CrossRef]
- Wieczorek, A.; Loster, J.; Loster, B.W. Relationship between Occlusal Force Distribution and the Activity of Masseter and Anterior Temporalis Muscles in Asymptomatic Young Adults. BioMed Res. Int. 2013, 2013, 354017. [Google Scholar] [CrossRef]
- Wieczorek, A.; Loster, J.E. Activity of the Masticatory Muscles and Occlusal Contacts in Young Adults with and without Orthodontic Treatment. BMC Oral Health 2015, 15, 116. [Google Scholar] [CrossRef]
- Ginszt, M.; Zieliński, G.; Szkutnik, J.; Wójcicki, M.; Baszczowski, M.; Litko-Rola, M.; Rózyło-Kalinowska, I.; Majcher, P. The Effects of Wearing a Medical Mask on the Masticatory and Neck Muscle Activity in Healthy Young Women. J. Clin. Med. 2022, 11, 303. [Google Scholar] [CrossRef]
- Naeije, M.; McCarroll, R.S.; Weijs, W.A. Electromyographic Activity of the Human Masticatory Muscles during Submaximal Clenching in the Inter-Cuspal Position. J. Oral Rehabil. 1989, 16, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Lakens, D. Calculating and Reporting Effect Sizes to Facilitate Cumulative Science: A Practical Primer for t-Tests and ANOVAs. Front. Psychol. 2013, 4, 863. [Google Scholar] [CrossRef] [PubMed]
- Fritz, C.O.; Morris, P.E.; Richler, J.J. Effect Size Estimates: Current Use, Calculations, and Interpretation. J. Exp. Psychol. Gen. 2012, 141, 2–18. [Google Scholar] [CrossRef]
- Hazra, A. Using the Confidence Interval Confidently. J. Thorac. Dis. 2017, 9, 4125–4130. [Google Scholar] [CrossRef] [PubMed]
- Kang, H. Sample Size Determination and Power Analysis Using the G*Power Software. J. Educ. Eval. Health Prof. 2021, 18, 17. [Google Scholar] [CrossRef] [PubMed]
- Somisetty, S.; Das, J.M. Neuroanatomy, Vestibulo-Ocular Reflex. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Zhang, X.; Bai, Y.; Chen, T.; Wang, W.; Han, X.; Li, S.; Liu, Q.; Wen, C. A Show of Ewald’s Law: I Horizontal Semicircular Canal Benign Paroxysmal Positional Vertigo. Front. Neurol. 2021, 12, 632489. [Google Scholar] [CrossRef]
- Stack, B.; Sims, A. The Relationship between Posture and Equilibrium and the Auriculotemporal Nerve in Patients with Disturbed Gait and Balance. Cranio J. Craniomandib. Pract. 2009, 27, 248–260. [Google Scholar] [CrossRef]
- Stecco, C.; Hammer, W.I. Functional Atlas of the Human Fascial System; Elsevier Ltd.: Edinburgh, Scotland, 2015; pp. 103–139. ISBN 978-0-7020-4430-4. [Google Scholar]
- Luong, T.Q.; Shu, Y.-H.; Modjtahedi, B.S.; Fong, D.S.; Choudry, N.; Tanaka, Y.; Nau, C.L. Racial and Ethnic Differences in Myopia Progression in a Large, Diverse Cohort of Pediatric Patients. Investig. Ophthalmol. Vis. Sci. 2020, 61, 20. [Google Scholar] [CrossRef]
- Rudnicka, A.R.; Owen, C.G.; Nightingale, C.M.; Cook, D.G.; Whincup, P.H. Ethnic Differences in the Prevalence of Myopia and Ocular Biometry in 10- and 11-Year-Old Children: The Child Heart and Health Study in England (CHASE). Investig. Ophthalmol. Vis. Sci. 2010, 51, 6270–6276. [Google Scholar] [CrossRef]
- Diéguez-Pérez, M.; Fernández-Molina, A.; Burgueño-Torres, L. Influence of Occlusion and Mandibular Position on Foot Support and Head Posture in Adult Patients. CRANIO® 2022, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Fernández Molina, A.; Burgueño-Torres, L.; Diéguez-Pérez, M. Influence of the Mandibular Position on Various Postural Anatomical Segments. CRANIO® 2021, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Vozzi, F.; Favero, L.; Peretta, R.; Guarda-Nardini, L.; Cocilovo, F.; Manfredini, D. Indexes of Jaw Muscle Function in Asymptomatic Individuals with Different Occlusal Features. Clin. Exp. Dent. Res. 2018, 4, 263–267. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Women | Men | ||||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||
| n | 32.00 | 18.00 | |||
| Age (years) | 23.09 | 1.89 | 23.67 | 2.45 | |
| Height (cm) | 167.38 | 7.17 | 179.72 | 4.74 | |
| Weight (kg) | 59.90 | 8.72 | 78.50 | 6.82 | |
| Body Mass Index | 21.38 | 2.96 | 24.31 | 1.93 | |
| Visual Acuity | R | 1.0 | 1.0 | ||
| L | 1.0 | 1.0 | |||
| Intraocular Pressure (mmHg) | R | 15.61 | 3.70 | 14.50 | 3.17 |
| L | 14.44 | 3.90 | 14.40 | 3.81 | |
| Axial Length (mm) | R | 23.48 | 0.53 | 23.95 | 0.63 |
| L | 23.46 | 0.52 | 23.95 | 0.60 | |
| Mandibular Range Of Motion (mm) | Abduction Without Pain | 49.44 | 4.66 | 53.28 | 6.73 |
| Active Abduction | 50.69 | 5.71 | 54.39 | 6.18 | |
| Passive Abduction | 52.97 | 5.88 | 57.17 | 6.21 | |
| Mandibular Movement to The Right | 9.16 | 2.85 | 9.89 | 2.93 | |
| Mandibular Movement to The Left | 10.03 | 2.72 | 9.67 | 2.54 | |
| Protrusion | 8.72 | 2.76 | 8.56 | 1.98 | |
| Open Eye | Closed Eye | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Z | P | CI 95% | |||
| Rest | TA-R | 2.34 | 1.95 | 1.85 | 0.89 | 0.43 | 0.67 | −0.57 | 0.29 |
| TA-L | 2.27 | 1.52 | 2.00 | 1.58 | 1.18 | 0.24 | −0.74 | 0.22 | |
| TA mean | 2.30 | 1.54 | 1.92 | 1.12 | 0.73 | 0.47 | −0.69 | 0.21 | |
| MM-R | 1.99 | 0.82 | 2.05 | 1.06 | 0.16 | 0.87 | −0.45 | 0.42 | |
| MM-L | 2.06 | 0.77 | 2.24 | 1.52 | 0.21 | 0.83 | −0.47 | 0.36 | |
| MM mean | 2.02 | 0.74 | 2.15 | 1.00 | −0.03 | 0.98 | −0.40 | 0.40 | |
| SCM-R | 1.16 | 0.31 | 1.42 | 0.62 | −1.55 | 0.12 | −0.03 | 0.38 | |
| SCM-L | 1.21 | 0.28 | 1.40 | 0.59 | −0.85 | 0.39 | −0.09 | 0.25 | |
| SCM mean | 1.19 | 0.25 | 1.41 | 0.51 | −1.56 | 0.12 | −0.04 | 0.33 | |
| DA-R | 1.80 | 0.92 | 1.78 | 0.66 | −0.62 | 0.53 | −0.21 | 0.43 | |
| DA-L | 1.74 | 0.85 | 1.66 | 0.71 | 0.11 | 0.91 | −0.30 | 0.27 | |
| DA mean | 1.77 | 0.86 | 1.72 | 0.64 | −0.19 | 0.85 | −0.24 | 0.36 | |
| Clenching in The Intercuspal Position | TA-R | 167.40 | 98.62 | 148.17 | 83.93 | 0.64 | 0.52 | −56.60 | 28.60 |
| TA-L | 149.59 | 72.71 | 137.48 | 64.42 | 0.68 | 0.50 | −46.50 | 23.90 | |
| TA mean | 158.49 | 81.56 | 142.82 | 72.11 | 0.76 | 0.45 | −50.50 | 26.80 | |
| MM-R | 167.43 | 94.37 | 142.62 | 84.51 | 1.23 | 0.22 | −60.10 | 16.40 | |
| MM-L | 164.69 | 103.30 | 134.35 | 84.37 | 1.26 | 0.21 | −63.90 | 15.10 | |
| MM mean | 166.06 | 95.45 | 138.48 | 81.51 | 1.26 | 0.21 | −61.15 | 14.70 | |
| SCM-R | 11.60 | 6.96 | 9.45 | 6.26 | 1.56 | 0.12 | −4.70 | 0.60 | |
| SCM-L | 12.26 | 9.61 | 9.73 | 7.06 | 1.26 | 0.21 | −5.00 | 1.10 | |
| SCM mean | 11.93 | 7.72 | 9.59 | 5.99 | 1.28 | 0.20 | −4.90 | 0.90 | |
| DA-R | 23.53 | 14.92 | 20.25 | 13.57 | 1.09 | 0.28 | −8.00 | 2.50 | |
| DA-L | 24.65 | 18.70 | 19.84 | 16.79 | 1.52 | 0.13 | −9.00 | 1.20 | |
| DA mean | 24.09 | 15.50 | 20.05 | 13.95 | 1.34 | 0.18 | −9.05 | 1.55 | |
| Clenching on Dental Cotton Rollers | TA-R | 149.47 | 91.32 | 147.11 | 88.71 | −0.01 | 0.99 | −45.10 | 41.40 |
| TA-L | 139.13 | 72.32 | 135.68 | 69.44 | 0.11 | 0.91 | −34.80 | 30.70 | |
| TA mean | 144.30 | 78.40 | 141.39 | 75.18 | 0.15 | 0.88 | −41.00 | 36.05 | |
| MM-R | 183.66 | 98.79 | 170.86 | 84.63 | 0.42 | 0.67 | −57.40 | 37.70 | |
| MM-L | 182.63 | 91.12 | 168.66 | 85.87 | 0.66 | 0.51 | −58.50 | 32.70 | |
| MM mean | 183.14 | 91.99 | 169.76 | 81.07 | 0.51 | 0.61 | −57.75 | 33.50 | |
| SCM-R | 13.95 | 6.39 | 13.05 | 6.97 | 0.74 | 0.46 | −3.80 | 1.80 | |
| SCM-L | 14.44 | 9.71 | 13.24 | 9.18 | 0.82 | 0.41 | −4.50 | 2.40 | |
| SCM mean | 14.20 | 7.51 | 13.15 | 7.50 | 0.88 | 0.38 | −3.85 | 2.20 | |
| DA-R | 25.39 | 9.78 | 22.08 | 10.06 | 1.48 | 0.14 | −8.90 | 1.30 | |
| DA-L | 27.84 | 15.64 | 22.83 | 15.00 | 2.20 | 0.03 * ES = 0.32 | −9.40 | −0.80 | |
| DA mean | 26.62 | 11.10 | 22.45 | 10.94 | 1.99 | 0.04 * ES = 0.29 | −9.05 | −0.25 | |
| Maximum Mouth Opening | TA-R | 5.53 | 3.31 | 5.33 | 2.79 | 0.26 | 0.79 | −1.40 | 1.20 |
| TA-L | 5.20 | 2.85 | 4.49 | 1.73 | 0.76 | 0.45 | −1.50 | 0.70 | |
| TA mean | 5.36 | 2.73 | 4.91 | 2.02 | 0.52 | 0.61 | −1.50 | 0.90 | |
| MM-R | 7.81 | 6.18 | 7.47 | 4.89 | −0.12 | 0.90 | −1.50 | 1.60 | |
| MM-L | 7.63 | 5.33 | 7.30 | 4.81 | 0.03 | 0.97 | −1.40 | 1.50 | |
| MM mean | 7.72 | 5.29 | 7.38 | 4.35 | −0.08 | 0.94 | −1.40 | 1.60 | |
| SCM-R | 6.91 | 3.74 | 7.05 | 3.50 | −0.24 | 0.81 | −1.60 | 1.90 | |
| SCM-L | 6.17 | 3.14 | 6.80 | 3.32 | −0.82 | 0.41 | −0.90 | 2.10 | |
| SCM mean | 6.54 | 3.34 | 6.93 | 3.25 | −0.43 | 0.67 | −1.15 | 1.95 | |
| DA-R | 68.11 | 38.00 | 74.00 | 42.48 | −0.40 | 0.69 | −15.50 | 24.20 | |
| DA-L | 69.70 | 43.82 | 74.89 | 43.98 | −0.60 | 0.55 | −16.60 | 27.80 | |
| DA mean | 68.90 | 39.90 | 74.45 | 41.36 | −0.54 | 0.59 | −16.25 | 27.00 | |
| Open Eye | Closed Eye | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Z | P | CI 95% | |||
| Rest | AsI-TA | 0.00 | 0.25 | 0.01 | 0.21 | 0.00 | 1.00 | −0.11 | 0.11 |
| AsI-MM | −0.02 | 0.16 | −0.02 | 0.25 | −0.34 | 0.74 | −0.08 | 0.12 | |
| AsI-SCM | −0.02 | 0.13 | 0.01 | 0.17 | −1.05 | 0.29 | −0.03 | 0.11 | |
| AsI-DA | 0.01 | 0.09 | 0.04 | 0.11 | −1.40 | 0.16 | −0.01 | 0.08 | |
| AcI-R | 0.00 | 0.34 | 0.04 | 0.33 | −0.56 | 0.57 | −0.13 | 0.22 | |
| AcI-L | 0.01 | 0.31 | 0.07 | 0.37 | −0.40 | 0.69 | −0.12 | 0.24 | |
| AcI mean | 0.00 | 0.31 | 0.07 | 0.34 | −0.78 | 0.44 | −0.10 | 0.23 | |
| Clenching in The Intercuspal Position | AsI-TA | 0.05 | 0.20 | 0.02 | 0.18 | 0.50 | 0.61 | −0.11 | 0.06 |
| AsI-MM | 0.03 | 0.14 | 0.05 | 0.15 | −0.22 | 0.82 | −0.05 | 0.07 | |
| AsI-SCM | 0.01 | 0.18 | 0.02 | 0.21 | −0.19 | 0.85 | −0.08 | 0.10 | |
| AsI-DA | 0.00 | 0.21 | 0.03 | 0.22 | −0.80 | 0.42 | −0.06 | 0.15 | |
| AcI-R | 0.00 | 0.23 | −0.03 | 0.23 | 0.80 | 0.42 | −0.14 | 0.07 | |
| AcI-L | 0.02 | 0.28 | −0.05 | 0.25 | 1.07 | 0.29 | −0.19 | 0.06 | |
| AcI mean | 0.01 | 0.23 | −0.04 | 0.21 | 0.85 | 0.39 | −0.15 | 0.06 | |
| Clenching on Dental Cotton Rollers | AsI-TA | 0.00 | 0.19 | 0.02 | 0.22 | −0.30 | 0.76 | −0.08 | 0.10 |
| AsI-MM | −0.01 | 0.13 | 0.00 | 0.15 | −0.19 | 0.85 | −0.05 | 0.08 | |
| AsI-SCM | 0.02 | 0.18 | 0.04 | 0.20 | −0.15 | 0.88 | −0.08 | 0.12 | |
| AsI-DA | −0.03 | 0.20 | 0.00 | 0.22 | −0.56 | 0.58 | −0.08 | 0.14 | |
| AcI-R | 0.12 | 0.23 | 0.11 | 0.21 | 0.53 | 0.60 | −0.13 | 0.10 | |
| AcI-L | 0.14 | 0.21 | 0.12 | 0.20 | 0.54 | 0.59 | −0.12 | 0.09 | |
| AcI mean | 0.13 | 0.19 | 0.11 | 0.18 | 0.34 | 0.73 | −0.12 | 0.08 | |
| Maximum Mouth Opening | AsI-TA | 0.03 | 0.17 | 0.06 | 0.17 | −0.49 | 0.62 | −0.06 | 0.11 |
| AsI-MM | 0.00 | 0.16 | 0.01 | 0.17 | −0.62 | 0.54 | −0.05 | 0.09 | |
| AsI-SCM | 0.05 | 0.13 | 0.02 | 0.17 | 0.59 | 0.55 | −0.10 | 0.05 | |
| AsI-DA | 0.00 | 0.11 | 0.00 | 0.13 | 0.09 | 0.93 | −0.06 | 0.05 | |
| AcI-R | 0.13 | 0.28 | 0.14 | 0.21 | 0.06 | 0.95 | −0.12 | 0.11 | |
| AcI-L | 0.16 | 0.22 | 0.19 | 0.19 | −0.36 | 0.72 | −0.07 | 0.10 | |
| AcI mean | 0.14 | 0.24 | 0.17 | 0.17 | −0.11 | 0.91 | −0.09 | 0.10 | |
| Open Eye | Closed Eye | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Z | P | CI 95% | |||
| Rest | TA-R | 2.63 | 2.01 | 2.30 | 1.98 | 0.43 | 0.67 | −1.66 | 0.37 |
| TA-L | 2.21 | 1.72 | 1.74 | 1.16 | 0.41 | 0.68 | −1.09 | 0.36 | |
| TA mean | 2.42 | 1.63 | 2.02 | 1.42 | 0.65 | 0.52 | −1.23 | 0.33 | |
| MM-R | 3.19 | 2.57 | 2.74 | 1.87 | 0.16 | 0.87 | −1.31 | 0.90 | |
| MM-L | 2.54 | 1.45 | 2.39 | 1.49 | 0.46 | 0.65 | −1.02 | 0.75 | |
| MM mean | 2.86 | 1.87 | 2.57 | 1.54 | 0.36 | 0.72 | −1.23 | 0.76 | |
| SCM-R | 1.13 | 0.39 | 1.19 | 0.49 | −0.21 | 0.84 | −0.22 | 0.27 | |
| SCM-L | 1.30 | 0.33 | 1.25 | 0.37 | 0.27 | 0.79 | −0.30 | 0.21 | |
| SCM mean | 1.22 | 0.33 | 1.22 | 0.40 | −0.02 | 0.99 | −0.25 | 0.25 | |
| DA-R | 1.48 | 0.56 | 1.40 | 0.53 | 0.25 | 0.80 | −0.45 | 0.31 | |
| DA-L | 1.47 | 0.54 | 1.39 | 0.49 | 0.25 | 0.80 | −0.43 | 0.31 | |
| DA mean | 1.47 | 0.54 | 1.39 | 0.51 | 0.18 | 0.85 | −0.42 | 0.29 | |
| Clenching in The Intercuspal Position | TA-R | 156.25 | 65.99 | 143.74 | 56.16 | 0.90 | 0.37 | −57.70 | 34.90 |
| TA-L | 142.98 | 72.78 | 132.44 | 63.16 | 0.55 | 0.58 | −60.70 | 34.90 | |
| TA mean | 149.62 | 66.13 | 138.09 | 54.70 | 0.65 | 0.52 | −0.42 | 0.29 | |
| MM-R | 171.81 | 109.05 | 144.59 | 102.25 | 0.87 | 0.38 | −87.90 | 27.40 | |
| MM-L | 150.90 | 87.45 | 133.01 | 77.24 | 0.38 | 0.70 | −74.60 | 40.10 | |
| MM mean | 161.35 | 93.27 | 138.80 | 83.42 | 0.68 | 0.50 | −68.40 | 24.15 | |
| SCM-R | 11.17 | 7.40 | 9.38 | 5.54 | 0.82 | 0.41 | −4.40 | 1.80 | |
| SCM-L | 14.24 | 14.68 | 11.10 | 10.29 | 0.84 | 0.40 | −5.90 | 2.90 | |
| SCM mean | 12.71 | 10.74 | 10.24 | 7.67 | 1.03 | 0.30 | −5.60 | 2.05 | |
| DA-R | 19.88 | 14.98 | 17.28 | 14.92 | 0.60 | 0.55 | −9.30 | 4.30 | |
| DA-L | 18.76 | 12.08 | 16.76 | 12.40 | 0.71 | 0.48 | −9.10 | 4.60 | |
| DA mean | 19.32 | 13.32 | 17.02 | 13.41 | 0.78 | 0.43 | −7.35 | 3.40 | |
| Clenching on Dental Cotton Rollers | TA-R | 152.24 | 73.08 | 148.84 | 62.24 | −0.05 | 0.96 | −51.20 | 50.60 |
| TA-L | 140.56 | 57.72 | 140.38 | 57.92 | −0.17 | 0.86 | −40.00 | 42.90 | |
| TA mean | 146.40 | 62.88 | 144.61 | 57.96 | 0.14 | 0.89 | −41.80 | 44.90 | |
| MM-R | 193.12 | 73.16 | 187.03 | 89.92 | 0.63 | 0.53 | −61.10 | 35.60 | |
| MM-L | 177.98 | 66.32 | 170.36 | 64.20 | 0.36 | 0.72 | −48.70 | 37.10 | |
| MM mean | 185.55 | 58.40 | 178.69 | 69.86 | 0.74 | 0.46 | −56.10 | 33.00 | |
| SCM-R | 12.68 | 7.36 | 11.39 | 6.84 | 0.63 | 0.53 | −5.80 | 3.00 | |
| SCM-L | 15.44 | 12.52 | 14.45 | 11.91 | 0.63 | 0.53 | −5.30 | 3.70 | |
| SCM mean | 14.06 | 9.51 | 12.92 | 8.95 | 0.74 | 0.46 | −5.00 | 3.35 | |
| DA-R | 19.19 | 10.33 | 16.96 | 8.47 | 0.53 | 0.59 | −7.90 | 4.40 | |
| DA-L | 18.74 | 7.91 | 16.39 | 6.22 | 0.70 | 0.48 | −7.90 | 4.30 | |
| DA mean | 18.96 | 8.58 | 16.68 | 6.77 | 0.56 | 0.58 | −8.05 | 4.35 | |
| Maximum Mouth Opening | TA-R | 8.47 | 9.81 | 5.82 | 4.83 | 0.33 | 0.74 | −2.50 | 1.40 |
| TA-L | 8.30 | 8.52 | 5.70 | 4.87 | 0.71 | 0.48 | −3.60 | 1.80 | |
| TA mean | 8.39 | 8.37 | 5.76 | 4.66 | 0.62 | 0.54 | −3.40 | 1.45 | |
| MM-R | 13.89 | 16.58 | 16.87 | 23.43 | −0.22 | 0.82 | −5.30 | 6.40 | |
| MM-L | 11.99 | 12.21 | 14.38 | 23.26 | −0.30 | 0.76 | −4.70 | 4.60 | |
| MM mean | 12.94 | 13.57 | 15.63 | 15.14 | −0.74 | 0.46 | −4.20 | 8.15 | |
| SCM-R | 13.29 | 10.49 | 12.03 | 11.10 | 0.49 | 0.62 | −7.80 | 4.20 | |
| SCM-L | 16.09 | 18.58 | 13.86 | 15.72 | 0.28 | 0.78 | −7.70 | 4.90 | |
| SCM mean | 14.69 | 13.02 | 12.94 | 11.76 | 0.46 | 0.65 | −7.85 | 4.55 | |
| DA-R | 50.18 | 43.19 | 50.60 | 46.69 | −0.10 | 0.92 | −34.20 | 35.70 | |
| DA-L | 44.28 | 36.88 | 43.85 | 39.40 | 0.00 | 1.00 | −26.30 | 22.50 | |
| DA mean | 47.23 | 39.89 | 47.22 | 42.92 | −0.10 | 0.92 | −29.75 | 26.35 | |
| Open Eye | Closed Eye | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Z | P | CI 95% | |||
| Rest | AsI-TA | 0.07 | 0.26 | 0.08 | 0.23 | 0.02 | 0.99 | −0.15 | 0.17 |
| AsI-MM | 0.05 | 0.22 | 0.05 | 0.20 | 0.11 | 0.91 | −0.16 | 0.13 | |
| AsI-SCM | −0.08 | 0.11 | −0.04 | 0.12 | −0.90 | 0.37 | −0.05 | 0.12 | |
| AsI-DA | 0.00 | 0.09 | 0.00 | 0.05 | 0.55 | 0.58 | −0.06 | 0.04 | |
| AcI-R | 0.08 | 0.36 | 0.11 | 0.37 | −0.40 | 0.69 | −0.25 | 0.29 | |
| AcI-L | 0.12 | 0.28 | 0.15 | 0.28 | 0.02 | 0.99 | −0.17 | 0.24 | |
| AcI mean | 0.09 | 0.31 | 0.13 | 0.32 | −0.52 | 0.60 | −0.17 | 0.26 | |
| Clenching in The Intercuspal Position | AsI-TA | 0.07 | 0.14 | 0.06 | 0.16 | 0.43 | 0.67 | −0.13 | 0.09 |
| AsI-MM | 0.08 | 0.24 | 0.04 | 0.27 | 0.81 | 0.42 | −0.19 | 0.09 | |
| AsI-SCM | −0.05 | 0.22 | −0.01 | 0.27 | −0.36 | 0.72 | −0.15 | 0.18 | |
| AsI-DA | 0.01 | 0.16 | 0.00 | 0.19 | 0.00 | 1.00 | −0.12 | 0.12 | |
| AcI-R | −0.01 | 0.28 | −0.07 | 0.31 | 0.46 | 0.65 | −0.27 | 0.14 | |
| AcI-L | −0.02 | 0.26 | −0.07 | 0.27 | 0.52 | 0.60 | −0.19 | 0.11 | |
| AcI mean | 0.00 | 0.25 | −0.06 | 0.25 | 0.59 | 0.56 | −0.21 | 0.13 | |
| Clenching on Dental Cotton Rollers | AsI-TA | 0.02 | 0.11 | 0.02 | 0.11 | −0.02 | 0.99 | −0.08 | 0.09 |
| AsI-MM | 0.04 | 0.19 | 0.03 | 0.17 | 0.11 | 0.91 | −0.12 | 0.11 | |
| AsI-SCM | −0.07 | 0.21 | −0.09 | 0.22 | 0.40 | 0.69 | −0.15 | 0.13 | |
| AsI-DA | 0.00 | 0.16 | 0.00 | 0.18 | 0.02 | 0.98 | −0.11 | 0.16 | |
| AcI-R | 0.14 | 0.26 | 0.12 | 0.24 | 0.46 | 0.65 | −0.21 | 0.14 | |
| AcI-L | 0.13 | 0.19 | 0.11 | 0.20 | 0.68 | 0.50 | −0.13 | 0.07 | |
| AcI mean | 0.14 | 0.20 | 0.12 | 0.20 | 0.46 | 0.65 | −0.15 | 0.09 | |
| Maximum Mouth Opening | AsI-TA | 0.01 | 0.22 | 0.04 | 0.18 | 0.17 | 0.86 | −0.12 | 0.13 |
| AsI-MM | 0.02 | 0.21 | 0.04 | 0.39 | −0.11 | 0.91 | −0.16 | 0.17 | |
| AsI-SCM | −0.04 | 0.24 | −0.03 | 0.24 | −0.11 | 0.91 | −0.16 | 0.16 | |
| AsI-DA | 0.05 | 0.10 | 0.05 | 0.09 | 0.10 | 0.92 | −0.09 | 0.08 | |
| AcI-R | 0.17 | 0.31 | 0.26 | 0.37 | −0.87 | 0.38 | −0.17 | 0.31 | |
| AcI-L | 0.16 | 0.27 | 0.29 | 0.29 | −1.15 | 0.25 | −0.09 | 0.30 | |
| AcI mean | 0.17 | 0.27 | 0.32 | 0.35 | −1.12 | 0.26 | −0.11 | 0.36 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zieliński, G.; Matysik-Woźniak, A.; Rapa, M.; Baszczowski, M.; Pająk, B.; Ginszt, M.; Szkutnik, J.; Rejdak, R.; Gawda, P. The Influence of Visual Input on Electromyographic Activity and Patterns of Masticatory and Cervical Spine Muscles in Emmetropic Caucasian Subjects by Gender. Int. J. Environ. Res. Public Health 2023, 20, 4112. https://doi.org/10.3390/ijerph20054112
Zieliński G, Matysik-Woźniak A, Rapa M, Baszczowski M, Pająk B, Ginszt M, Szkutnik J, Rejdak R, Gawda P. The Influence of Visual Input on Electromyographic Activity and Patterns of Masticatory and Cervical Spine Muscles in Emmetropic Caucasian Subjects by Gender. International Journal of Environmental Research and Public Health. 2023; 20(5):4112. https://doi.org/10.3390/ijerph20054112
Chicago/Turabian StyleZieliński, Grzegorz, Anna Matysik-Woźniak, Maria Rapa, Michał Baszczowski, Beata Pająk, Michał Ginszt, Jacek Szkutnik, Robert Rejdak, and Piotr Gawda. 2023. "The Influence of Visual Input on Electromyographic Activity and Patterns of Masticatory and Cervical Spine Muscles in Emmetropic Caucasian Subjects by Gender" International Journal of Environmental Research and Public Health 20, no. 5: 4112. https://doi.org/10.3390/ijerph20054112
APA StyleZieliński, G., Matysik-Woźniak, A., Rapa, M., Baszczowski, M., Pająk, B., Ginszt, M., Szkutnik, J., Rejdak, R., & Gawda, P. (2023). The Influence of Visual Input on Electromyographic Activity and Patterns of Masticatory and Cervical Spine Muscles in Emmetropic Caucasian Subjects by Gender. International Journal of Environmental Research and Public Health, 20(5), 4112. https://doi.org/10.3390/ijerph20054112