
Economic Analysis of Border Control Policies during COVID-19 Pandemic: A Modelling Study to Inform Cross-Border Travel Policy between Singapore and Thailand

 , , , , ,
, , , , ,  ,
, 
Abstract
1. Introduction
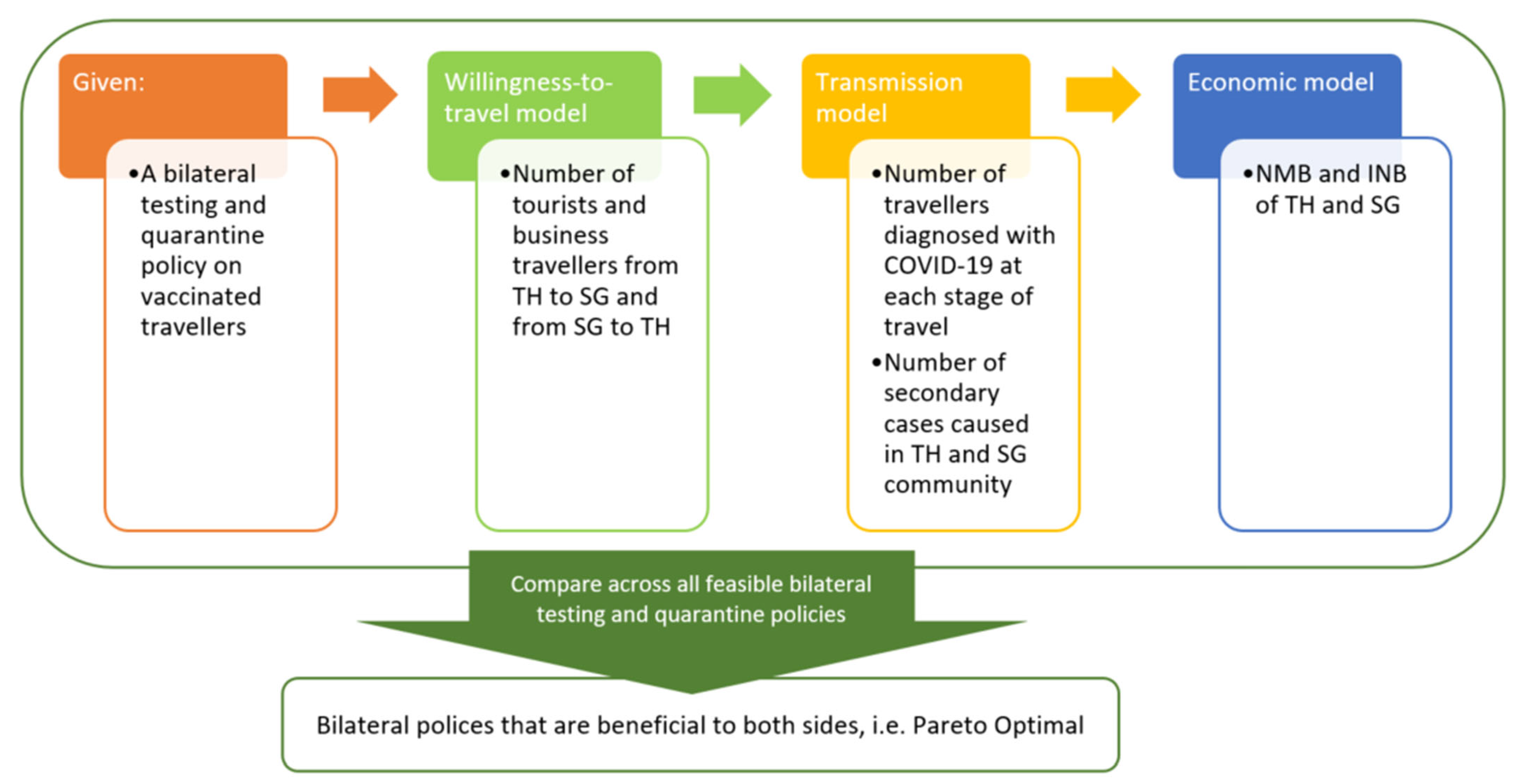
2. Materials and Methods
2.1. Study Population, Setting and Time Horizon
2.2. Comparators
2.3. Willingness-to-Travel Model
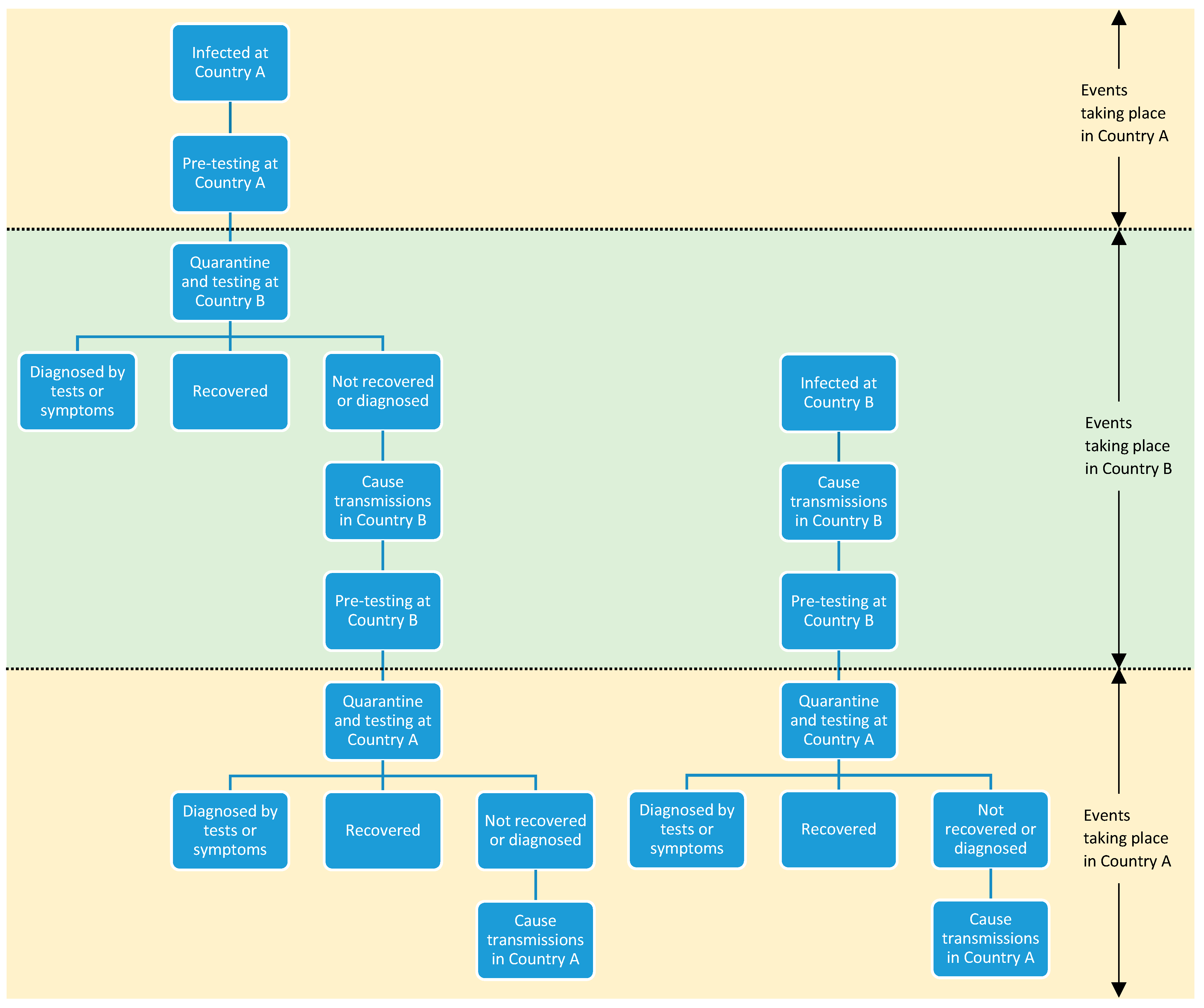
2.4. Transmission Model
2.5. Economic Model
2.6. Measurement and Valuation of Outcomes
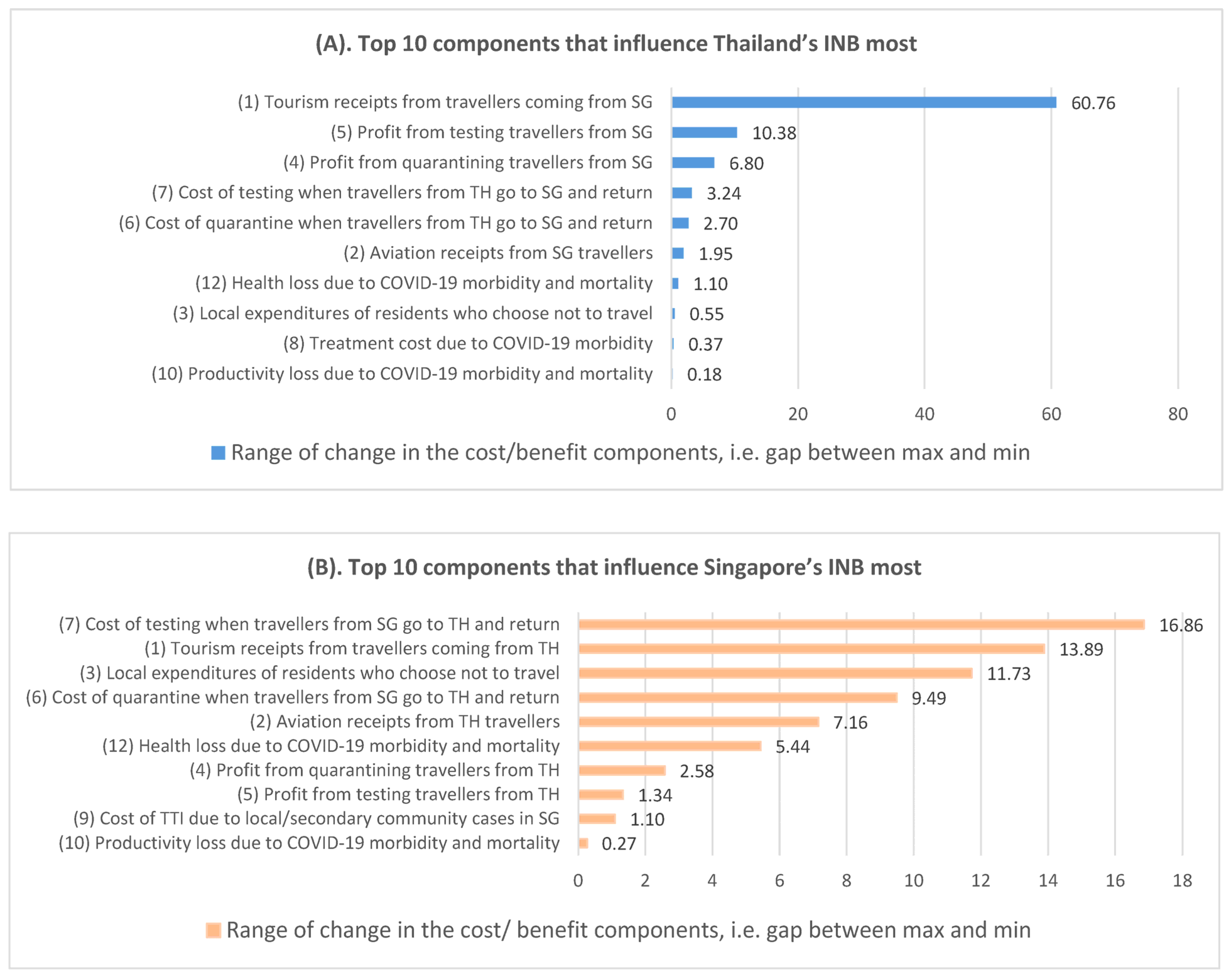
2.7. Deterministic Sensitivity Analysis (DSA)
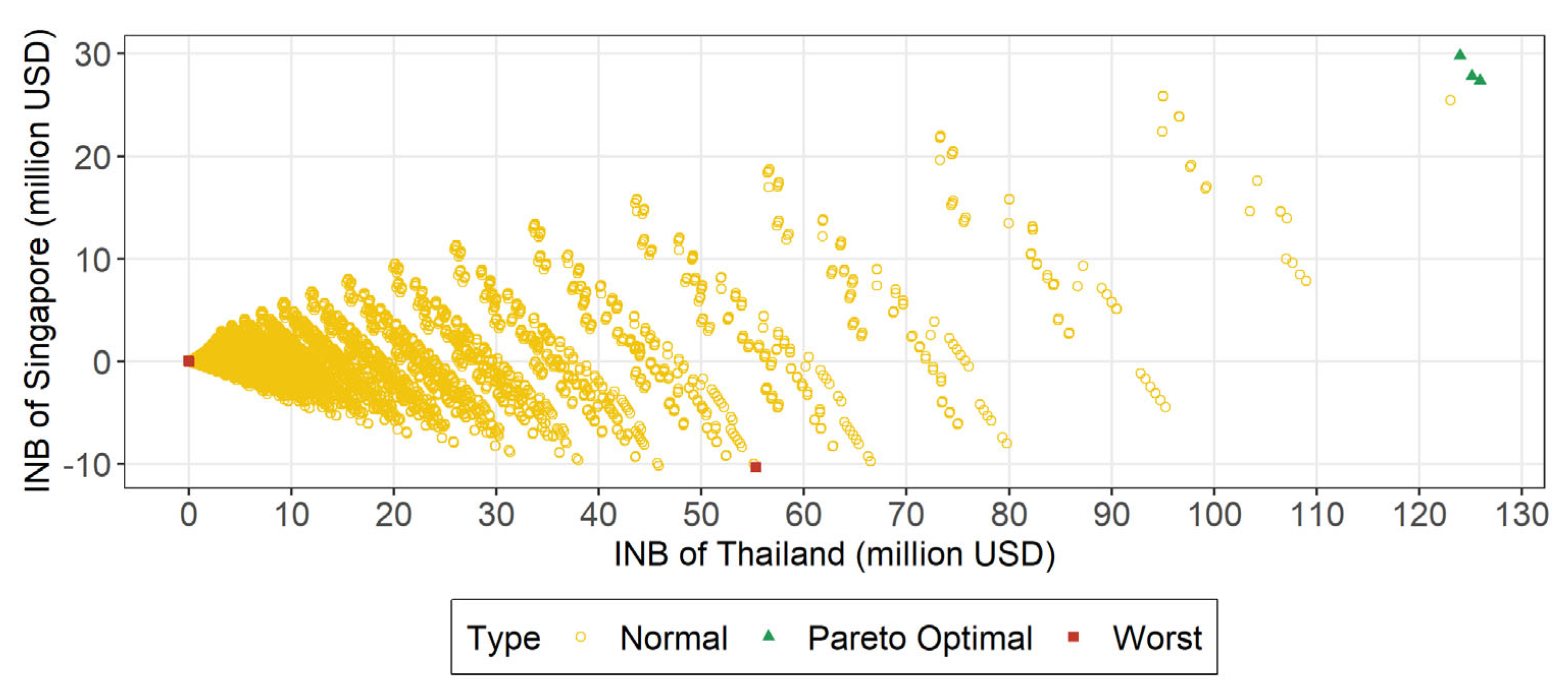
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Bank. International Tourism, Receipts (Current US$)—Thailand. 2022. Available online: https://data.worldbank.org/indicator/ST.INT.RCPT.CD?locations=TH (accessed on 15 March 2022).
- Singapore Toursim Board. Tourism Sector Performance Q4 2019 Report. 2022. Available online: https://www.stb.gov.sg/content/dam/stb/documents/statistics-marketing-insights/Quarterly-Tourism-Performance-Report/STB%20Q4%202019%20FA%20v7.pdf (accessed on 15 March 2022).
- Thailand, I.B. 2021. Available online: https://www.immigration.go.th/ (accessed on 1 October 2021).
- Board, S.T. Tourism Receipts by Major Components. 2022. Available online: https://tablebuilder.singstat.gov.sg/table/TS/M550361 (accessed on 1 March 2022).
- Lim, C.; McAleer, M. Modelling International Travel Demand from Singapore to Australia. Anatolia 2003, 14, 23–43. [Google Scholar] [CrossRef]
- Dickens, B.L.; Koo, J.R.; Lim, J.T.; Park, M.; Sun, H.; Sun, Y.; Zeng, Z.; Quaye, S.E.D.; Clapham, H.E.; Wee, H.L.; et al. Determining quarantine length and testing frequency for international border opening during the COVID-19 pandemic. J. Travel Med. 2021, 28, taab088. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health Singapore. COVID-19 Situation Report. 2021. Available online: https://covidsitrep.moh.gov.sg/ (accessed on 29 October 2021).
- Worldometer. Coronavirus—Thailand. 2021. Available online: https://www.worldometers.info/coronavirus/country/thailand/ (accessed on 29 October 2021).
- Ministry of Health Singapore. Update on Local COVID-19 Situation (28 October 2021). 2021. Available online: https://www.moh.gov.sg/news-highlights/details/update-on-local-covid-19-situation-(28-oct-2021) (accessed on 28 October 2021).
- Pfizer. Pfizer-BioNTech COVID-19 Vaccine (Also Known as BNT162b2). 2022. Available online: https://www.pfizer.com/products/product-detail/pfizer-biontech-covid-19-vaccine (accessed on 8 June 2022).
- European Medicines Agency. Comirnaty. 2022. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/comirnaty (accessed on 8 June 2022).
- European Medicines Agency. Spikevax (Previously COVID-19 Vaccine Moderna). 2022. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/spikevax (accessed on 8 June 2022).
- Thailand, M.o.P.H. COVID-19 Vaccine Thailand Presented in Report Format. 2021. Available online: https://ddc.moph.go.th/dcd/pagecontent.php?page=643&dept=dcd (accessed on 29 October 2021).
- European Medicines Agency. Vaxzevria (Previously COVID-19 Vaccine AstraZeneca). Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/vaxzevria-previously-covid-19-vaccine-astrazeneca (accessed on 8 June 2022).
- WHO. The Sinovac-CoronaVac COVID-19 Vaccine: What You Need to Know. 2022. Available online: https://www.who.int/news-room/feature-stories/detail/the-sinovac-covid-19-vaccine-what-you-need-to-know (accessed on 8 June 2022).
- Singapore Toursim Board. Singapore Tourism Analytics Network. 2022. Available online: http://www.singstat.gov.sg/find-data/search-by-theme/economy/national-accounts/publications-and-methodology (accessed on 15 June 2022).
- Teerawattananon, Y.; Chaikledkaew, U. Thai health technology assessment guideline development. J. Med. Assoc. Thail. 2008, 91 (Suppl. S2), S11–S15. [Google Scholar]
- Singapore Agency for Care Effctiveness. Health Technology Evaluation Processes and Methods. 2022. Available online: https://www.ace-hta.gov.sg/resources/process-methods (accessed on 8 June 2022).
- Van Ballegooijen, H.; Goossens, L.; Bruin, R.H.; Michels, R.; Krol, M. Concerns, quality of life, access to care and productivity of the general population during the first 8 weeks of the coronavirus lockdown in Belgium and the Netherlands. BMC Health Serv. Res. 2021, 21, 227. [Google Scholar] [CrossRef] [PubMed]
- Basu, A.; Gandhay, V.J. Quality-Adjusted Life-Year Losses Averted With Every COVID-19 Infection Prevented in the United States. Value Health 2021, 24, 632–640. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health Singapore. Remaining Vigilant Against the Omicron Variant. 2021. Available online: https://www.moh.gov.sg/news-highlights/details/remaining-vigilant-against-the-omicron-variant (accessed on 30 January 2023).
- Ministry of Health Singapore. COVID-19 Statistics. 2022. Available online: https://www.moh.gov.sg/covid-19/statistics (accessed on 30 January 2023).
- WHO. WHO Coronavirus (COVID-19) Dashboard. 2022. Available online: https://covid19.who.int/data (accessed on 30 January 2023).
- Department of Statistics Singapore. National Accounts—Singapore Supply, Use and Input-Output Tables 2017. 2022. Available online: https://www.singstat.gov.sg/find-data/search-by-theme/economy/national-accounts/latest-data (accessed on 30 January 2023).
- Sindechara, T. Economic Import Evaluation from Tourism in Designated Area for Sustainable Tourism; Thammasat University Research and Consultancy Institute: Bangkok, Thailand, 2017. [Google Scholar]
- Marseille, E.; Larson, B.; Kazi, D.S.; Kahn, J.G.; Rosen, S. Thresholds for the cost-effectiveness of interventions: Alternative approaches. Bull. World Health Organ. 2015, 93, 118–124. [Google Scholar] [CrossRef] [PubMed]
- Medina, A.F. Singapore Businesses Receive Boost as Border Restrictions to Ease. 2022. Available online: https://www.aseanbriefing.com/news/singapore-businesses-receive-boost-as-border-restrictions-to-ease/ (accessed on 8 June 2022).
- Walker, T. Thailand Reopens Borders for Tourists, Caution Still Remains. 2021. Available online: https://www.voanews.com/a/thailand-reopens-borders-for-tourists-caution-still-remains/6298173.html (accessed on 8 June 2022).
- Ministry of Foreign Affairs Singapore. Travel Page—Thailand. 2022. Available online: https://www.mfa.gov.sg/countries-regions/t/thailand/travel-page (accessed on 7 March 2022).
- ThaiEmbassy.com. The New Test and Go and the New Sandbox and Quarantine Program; Top 20 Questions on Thailand Pass and Travel to Thailand. 2022. Available online: https://www.thaiembassy.com/weekly-updates/the-new-test-and-go-and-the-new-sandbox-and-quarantine-program-top-20-questions-on-thailand-pass-and-travel-to-thailand (accessed on 14 May 2022).
- Supateerawanitt, A. Confirmed: Thailand to Drop Test & Go Entry Requirements from May 1. Available online: https://www.timeout.com/bangkok/news/confirmed-thailand-to-drop-test-go-entry-requirements-from-may-1-032122 (accessed on 14 May 2022).
- Thailand Reopening. 2022. Available online: https://tourismthailand.sg/ (accessed on 7 March 2022).
- Møller, G. VTL travel into Singapore made easier from 22 February. 2022. Available online: https://scandasia.com/vtl-travel-into-singapore-made-easier-from-22-february/ (accessed on 20 May 2022).
- Gov.sg. Streamlining Country/Region Classifications and Expanding VTLs. 2022. Available online: https://www.gov.sg/article/streamlining-country-or-region-classifications-and-expanding-vtls (accessed on 20 May 2022).
- Singapore, I.C.A. Travelling to Singapore—Overview. 2022. Available online: https://safetravel.ica.gov.sg/arriving/overview (accessed on 14 May 2022).
- Singapore Tourism Analytics Network. Tourism Receipts Statistics. Available online: https://stan.stb.gov.sg/content/stan/en/home.html (accessed on 18 February 2023).
- Peto, T.; UK COVID-19 Lateral Flow Oversight Team. COVID-19: Rapid antigen detection for SARS-CoV-2 by lateral flow assay: A national systematic evaluation of sensitivity and specificity for mass-testing. EClinicalMedicine 2021, 36, 100924. [Google Scholar] [CrossRef] [PubMed]
- Miller, T.E.; Garcia Beltran, W.F.; Bard, A.Z.; Gogakos, T.; Anahtar, M.N.; Astudillo, M.G.; Yang, D.; Thierauf, J.; Fisch, A.S.; Mahowald, G.K.; et al. Clinical sensitivity and interpretation of PCR and serological COVID-19 diagnostics for patients presenting to the hospital. FASEB J. 2020, 34, 13877–13884. [Google Scholar] [CrossRef] [PubMed]
- Oran, D.P.; Topol, E.J. Prevalence of asymptomatic SARS-CoV-2 infection: A narrative review. Ann. Intern. Med. 2020, 173, 362–367. [Google Scholar] [CrossRef] [PubMed]
- Wycliffe, W.E.; Heng, T.C.; Chan, M.; Tong, T.T.; Pada, S.K.; Archuleta, S.; Tat, O.S.; Jiashen, L.; Choon, R.F.K.; Cheng, T.K.; et al. Age and chest radiography as possible parameters for rapid triage in COVID-19 outbreak surge. Res. Sq. 2020. [Google Scholar] [CrossRef]
- O’Driscoll, M.; Santos, G.R.D.; Wang, L.; Cummings, D.A.T.; Azman, A.S.; Paireau, J.; Fontanet, A.; Cauchemez, S.; Salje, H. Age-specific mortality and immunity patterns of SARS-CoV-2. Nature 2021, 590, 140–145. [Google Scholar] [CrossRef] [PubMed]
- Sheikh, A.; McMenamin, J.; Taylor, B.; Robertson, C. SARS-CoV-2 Delta VOC in Scotland: Demographics, risk of hospital admission, and vaccine effectiveness. Lancet 2021, 397, 2461–2462. [Google Scholar] [CrossRef] [PubMed]
- SARS-Cov-2 Variants of Concern and Variants under Investigation in England; Public Health England: London, UK, 2021.
- Lopez Bernal, J.; Andrews, N.; Gower, C.; Gallagher, E.; Simmons, R.; Thelwall, S.; Stowe, J.; Tessier, E.; Groves, N.; Dabrera, G.; et al. Effectiveness of COVID-19 vaccines against hospital admission with the Delta (B.1.617.2) variant. N. Engl. J. Med. 2021, 388, 672. [Google Scholar]
- AstraZeneca. AZD1222 US Phase III Trial Met Primary Efficacy Endpoint in Preventing COVID-19 at Interim Analysis. 2021. Available online: https://www.astrazeneca.com/media-centre/press-releases/2021/astrazeneca-us-vaccine-trial-met-primary-endpoint.html (accessed on 15 July 2021).
- Abdin, E.; Subramaniam, M.; Vaingankar, J.A.; Luo, N.; Chong, S.A. Population norms for the EQ-5D index scores using Singapore preference weights. Qual. Life Res. 2015, 24, 1545–1553. [Google Scholar] [CrossRef] [PubMed]
- Wong, E.L.; Ho, K.F.; Wong, S.Y.; Cheung, A.W.; Yau, P.S.; Dong, D.; Yeoh, E.K. Views on workplace policies and its impact on health-related quality of life during coronavirus disease (COVID-19) pandemic: Cross-sectional survey of employees. Int. J. Health Policy Manag. 2022, 11, 344–353. [Google Scholar] [CrossRef] [PubMed]
- Herrero, L. How Contagious Is Delta? How Long Are You Infectious? Is It More Deadly? A Quick Guide to the Latest Science. The Conversation. Available online: https://theconversation.com/how-contagious-is-delta-how-long-are-you-infectious-is-it-more-deadly-a-quick-guide-to-the-latest-science-165538 (accessed on 15 October 2021).
- Jones, T.C.; Biele, G.; Mühlemann, B.; Veith, T.; Schneider, J.; Beheim-Schwarzbach, J.; Bleicker, T.; Tesch, J.; Schmidt, M.L.; Sander, L.E.; et al. Estimating infectiousness throughout SARS-CoV-2 infection course. Science 2021, 373, eabi5273. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Strategy Number | Pre-Test | Entry Test | Exit Test | Test during Quarantine | ||
|---|---|---|---|---|---|---|
| Weekly | Every 3 Days | Daily | ||||
| S1 | ART | ART | ART | ART | ||
| S2 | ART | ART | ART | ART | ||
| S3 | ART | ART | ART | ART | ||
| S4 | ART | ART | ART | |||
| S5 | PCR | PCR | PCR | ART | ||
| S6 | PCR | PCR | PCR | ART | ||
| S7 | PCR | PCR | PCR | ART | ||
| S8 | PCR | PCR | PCR | |||
| S9 | Quarantine only | |||||
| Traveler-related economic benefits/costs |
|
| COVID-19-case-related medical costs |
|
| COVID-19 cases-related non-medical costs |
|
| COVID-19 cases-related health loss |
|
| TH Testing | SG Testing | TH Quarantine Length (Days) | SG Quarantine Length (Days) | Imported Cases | Secondary Cases | Inbound Travelers | Returning Outbound Travelers | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ICU Cases among Travelers | ICU Cases among Secondary Cases | Deaths among Travelers | Deaths among Secondary Cases | ICU Cases among Travelers | ICU Cases among Secondary Cases | Deaths among Travelers | Deaths among Secondary Cases | |||||||
| TH | S4 | S4 | 0 | 0 | 54.158 | 159.116 | 0.024 | 0.876 | 0.007 | 0.382 | 0.024 | 1.518 | 0.014 | 0.661 |
| S4 | S9 | 0 | 0 | 28.152 | 161.187 | 0.010 | 0.878 | 0.003 | 0.382 | 0.022 | 1.548 | 0.015 | 0.674 | |
| S9 | S4 | 0 | 0 | 149.931 | 546.419 | 0.086 | 4.773 | 0.027 | 2.078 | 0.037 | 3.450 | 0.014 | 1.503 | |
| SG | S4 | S4 | 0 | 0 | 23.231 | 18.274 | 0.014 | 0.011 | 0.005 | 0.005 | 0.131 | 0.170 | 0.048 | 0.073 |
| S4 | S9 | 0 | 0 | 29.686 | 102.709 | 0.018 | 0.055 | 0.007 | 0.024 | 0.145 | 0.962 | 0.048 | 0.416 | |
| S9 | S4 | 0 | 0 | 22.996 | 40.661 | 0.001 | 0.011 | 0.000 | 0.005 | 0.101 | 0.392 | 0.058 | 0.169 | |
| Condition | TH Strategy | SG Strategy | TH Quarantine Days | SG Quarantine Days | TH INB (Millions) | SG INB (Millions) | TH Critical Cases | SG Critical Cases | Total Cases | Total Deaths |
|---|---|---|---|---|---|---|---|---|---|---|
| Base Case | S4 | S4 | 0 | 0 | 125.943 | 27.363 | 2.44 | 0.33 | 254.78 | 1.20 |
| S4 | S9 | 0 | 0 | 125.139 | 27.782 | 2.46 | 1.18 | 321.73 | 1.57 | |
| S9 | S4 | 0 | 0 | 123.973 | 29.776 | 8.35 | 0.50 | 760.01 | 3.85 | |
| Daily infection rate (1.5×) | S4 | S4 | 0 | 0 | 125.528 | 28.046 | 3.64 | 0.49 | 380.63 | 1.79 |
| S9 | S4 | 0 | 0 | 123.178 | 30.427 | 12.50 | 0.75 | 1138.38 | 5.77 | |
| R0 (R0 = 10) | S4 | S4 | 0 | 0 | 125.750 | 27.210 | 3.47 | 0.40 | 330.80 | 1.68 |
| S9 | S4 | 0 | 0 | 123.311 | 29.436 | 11.87 | 0.68 | 1011.61 | 5.46 | |
| Vaccine coverage (SG: 92%, TH 76%) | S4 | S9 | 0 | 0 | 140.156 | 59.513 | 2.13 | 1.15 | 492.92 | 1.42 |
| S4 | S4 | 0 | 0 | 140.056 | 59.784 | 2.12 | 0.37 | 398.86 | 1.08 | |
| S9 | S4 | 0 | 0 | 138.747 | 62.375 | 6.31 | 0.47 | 1008.41 | 2.95 | |
| Percentage reduction in number of travelers with one more day of quarantine (0.5×) | S4 | S4 | 0 | 0 | 116.373 | 29.659 | 2.44 | 0.33 | 254.78 | 1.20 |
| S4 | S9 | 0 | 0 | 115.569 | 30.079 | 2.46 | 1.18 | 321.73 | 1.57 | |
| S9 | S4 | 0 | 0 | 114.403 | 32.073 | 8.35 | 0.50 | 760.01 | 3.85 | |
| Percentage reduction in number of travelers with one more day of quarantine (1.5×) | S4 | S4 | 0 | 0 | 126.361 | 27.390 | 2.44 | 0.33 | 254.78 | 1.20 |
| S4 | S9 | 0 | 0 | 125.557 | 27.809 | 2.46 | 1.18 | 321.73 | 1.57 | |
| S9 | S4 | 0 | 0 | 124.391 | 29.803 | 8.35 | 0.50 | 760.01 | 3.85 | |
| Spillover effect of tourism sector (SG: 2.35, TH 2.09) | S4 | S4 | 0 | 0 | 193.990 | 55.635 | 2.44 | 0.33 | 254.78 | 1.20 |
| S4 | S9 | 0 | 0 | 193.188 | 56.064 | 2.46 | 1.18 | 321.73 | 1.57 | |
| S9 | S4 | 0 | 0 | 192.202 | 58.075 | 8.35 | 0.50 | 760.01 | 3.85 | |
| Vaccinated and unvaccinated travelers permitted | S4 | S9 | 0 | 0 | 152.067 | 74.497 | 10.11 | 5.02 | 956.70 | 6.71 |
| S4 | S4 | 0 | 0 | 151.549 | 75.965 | 10.37 | 3.09 | 811.20 | 5.93 | |
| S9 | S4 | 0 | 0 | 148.717 | 78.057 | 26.66 | 1.97 | 1955.17 | 12.37 | |
| Medical cost of COVID cases (2×) | S4 | S4 | 0 | 0 | 125.843 | 27.451 | 2.44 | 0.33 | 254.78 | 1.20 |
| S4 | S9 | 0 | 0 | 125.038 | 27.814 | 2.46 | 1.18 | 321.73 | 1.57 | |
| S9 | S4 | 0 | 0 | 123.630 | 29.854 | 8.35 | 0.50 | 760.01 | 3.85 | |
| Percentage productivity loss due to quarantine (0%) | S4 | S4 | 0 | 0 | 125.947 | 27.344 | 2.44 | 0.33 | 254.78 | 1.20 |
| S4 | S9 | 0 | 0 | 125.143 | 27.801 | 2.46 | 1.18 | 321.73 | 1.57 | |
| S9 | S4 | 0 | 0 | 124.002 | 29.733 | 8.35 | 0.50 | 760.01 | 3.85 | |
| QALY loss saved from vaccination for symptomatic cases (0%) | S4 | S4 | 0 | 0 | 125.938 | 27.379 | 2.44 | 0.33 | 254.78 | 1.20 |
| S4 | S9 | 0 | 0 | 125.134 | 27.743 | 2.46 | 1.18 | 321.73 | 1.57 | |
| S9 | S4 | 0 | 0 | 123.962 | 29.758 | 8.35 | 0.50 | 760.01 | 3.85 | |
| CET (3 GDP per capita) | S4 | S4 | 0 | 0 | 125.332 | 30.339 | 2.44 | 0.33 | 254.78 | 1.20 |
| S9 | S4 | 0 | 0 | 121.904 | 31.768 | 8.35 | 0.50 | 760.01 | 3.85 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cai, C.G.X.; Lim, N.W.-H.; Huynh, V.A.; Ananthakrishnan, A.; Dabak, S.V.; Dickens, B.S.L.; Faradiba, D.; KC, S.; Morton, A.; Park, M.; et al. Economic Analysis of Border Control Policies during COVID-19 Pandemic: A Modelling Study to Inform Cross-Border Travel Policy between Singapore and Thailand. Int. J. Environ. Res. Public Health 2023, 20, 4011. https://doi.org/10.3390/ijerph20054011
Cai CGX, Lim NW-H, Huynh VA, Ananthakrishnan A, Dabak SV, Dickens BSL, Faradiba D, KC S, Morton A, Park M, et al. Economic Analysis of Border Control Policies during COVID-19 Pandemic: A Modelling Study to Inform Cross-Border Travel Policy between Singapore and Thailand. International Journal of Environmental Research and Public Health. 2023; 20(5):4011. https://doi.org/10.3390/ijerph20054011
Chicago/Turabian StyleCai, Celestine Grace Xueting, Nigel Wei-Han Lim, Vinh Anh Huynh, Aparna Ananthakrishnan, Saudamini Vishwanath Dabak, Borame Sue Lee Dickens, Dian Faradiba, Sarin KC, Alec Morton, Minah Park, and et al. 2023. "Economic Analysis of Border Control Policies during COVID-19 Pandemic: A Modelling Study to Inform Cross-Border Travel Policy between Singapore and Thailand" International Journal of Environmental Research and Public Health 20, no. 5: 4011. https://doi.org/10.3390/ijerph20054011
APA StyleCai, C. G. X., Lim, N. W.-H., Huynh, V. A., Ananthakrishnan, A., Dabak, S. V., Dickens, B. S. L., Faradiba, D., KC, S., Morton, A., Park, M., Rachatan, C., Sittimart, M., Wee, H.-L., Lou, J., & Teerawattananon, Y. (2023). Economic Analysis of Border Control Policies during COVID-19 Pandemic: A Modelling Study to Inform Cross-Border Travel Policy between Singapore and Thailand. International Journal of Environmental Research and Public Health, 20(5), 4011. https://doi.org/10.3390/ijerph20054011