
Improving Participation among Youth with Disabilities within Their Unique Socio-Cultural Context during COVID-19 Pandemic: Initial Evaluation


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Instruments
2.3.1. Demographic Questionnaire
2.3.2. Canadian Occupational Performance Measure (COPM)
2.3.3. The Participation and Environment Measure—Children and Youth (PEM-CY)
2.3.4. Functional Independence Measure (FIM)
2.3.5. Client Satisfaction Questionnaire (CSQ-8)
2.3.6. Semi-Structured Interviews
2.4. Procedure
Content and Intervention Process
2.5. Data Analysis
2.5.1. Quantitative Analysis
2.5.2. Qualitative Analysis
3. Results
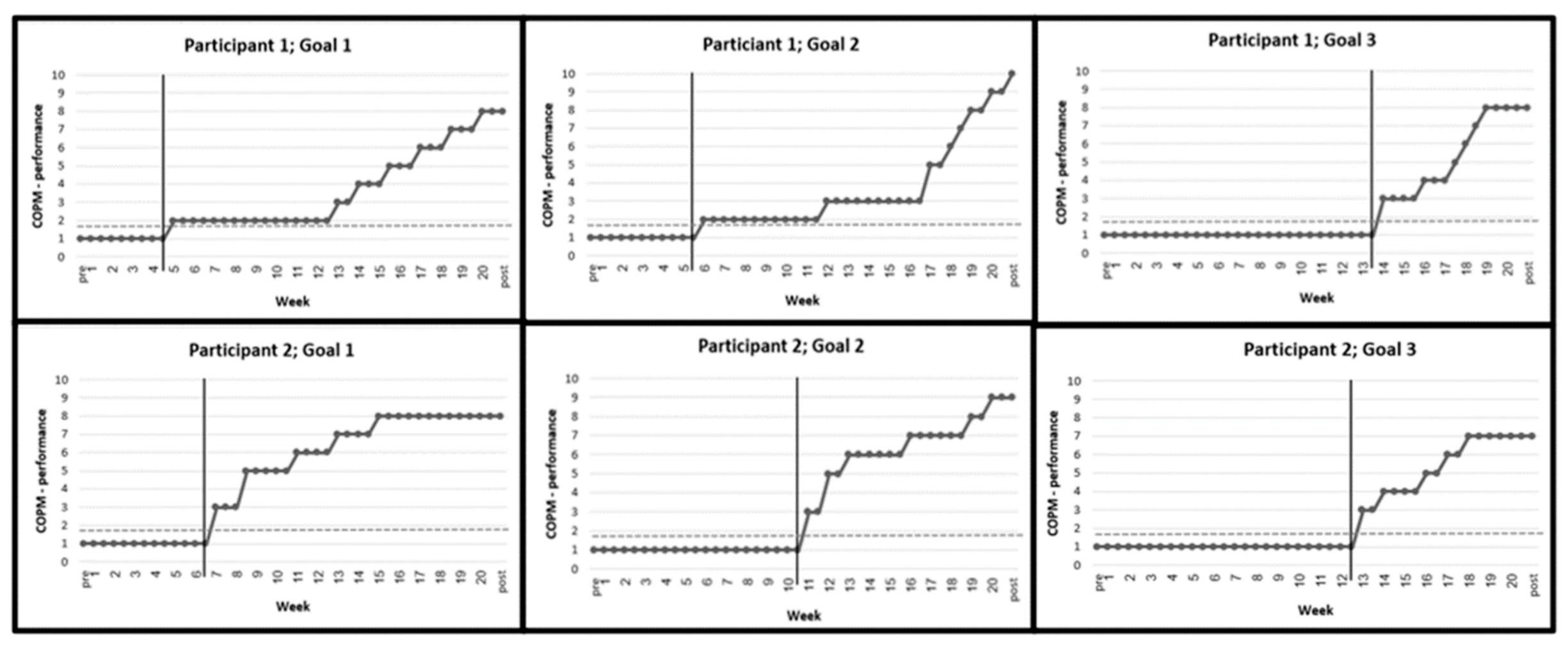
3.1. Changes in Performance Scores (COPM)
3.2. Level of Satisfaction
3.3. Changes in Participation Patterns
3.4. Qualitative Analysis
3.4.1. Personal Barriers
3.4.2. Environmental Barriers
3.4.3. Factors Supporting Intervention
3.4.4. Intervention Effects
4. Discussion
4.1. Clinical Implications
4.2. Limitations and Recommendations for Further Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Law, M. Participation in the occupations of everyday life. Am. J. Occup. Ther. 2002, 56, 640–649. [Google Scholar] [CrossRef]
- World Health Organization. International Classification of Functioning, Disability and Health (ICF); WHO: Geneva, Switzerland, 2001. [Google Scholar]
- Imms, C.; Adair, B.; Keen, D.; Ullenhag, A.; Rosenbaum, P.; Granlund, M. ‘Participation’: A systematic review of language, def-initions, and constructs used in intervention research with children with disabilities. Dev. Med. Child Neurol. 2016, 58, 29–38. [Google Scholar] [CrossRef]
- Coster, W.; Bedell, G.; Law, M.; Khetani, M.A.; Teplicky, R.; Liljenquist, K.; Gleason, K.; Kao, Y.C. Psychometric evaluation of the Participation and Environment Measure for Children and Youth. Dev. Med. Child Neurol. 2011, 53, 1030–1037. [Google Scholar] [CrossRef]
- Coster, W.; Law, M.; Bedell, G.; Liljenquist, K.; Kao, Y.C.; Khetani, M.; Teplicky, R. School participation, supports and barriers of students with and without disabilities. Child Care Health Dev. 2013, 39, 535–543. [Google Scholar] [CrossRef] [PubMed]
- Law, M.; Anaby, D.; Teplicky, R.; Khetani, M.A.; Coster, W.; Bedell, G. Participation in the home environment among children and youth with and without disabilities. Br. J. Occup. Ther. 2013, 76, 58–66. [Google Scholar] [CrossRef]
- Bedell, G.; Coster, W.; Law, M.; Liljenquist, K.; Kao, Y.C.; Teplicky, R.; Anaby, D.; Khetani, M.A. Community participation, supports, and barriers of school-age children with and without disabilities. Arch. Phys. Med. Rehabil. 2013, 94, 315–323. [Google Scholar] [CrossRef]
- Bult, M.K.; Verschuren, O.; Jongmans, M.J.; Lindeman, E.; Ketelaar, M. What influences participation in leisure activities of children and youth with physical disabilities? A systematic review. Res. Dev. Disabil. 2011, 32, 1521–1529. [Google Scholar] [CrossRef]
- Engel-Yeger, B.; Jarus, T.; Anaby, D.; Law, M. Differences in patterns of participation between youths with cerebral palsy and typically developing peers. Am. J. Occup. Ther. 2009, 63, 96–104. [Google Scholar] [CrossRef]
- Anaby, D.; Hand, C.; Bradley, L.; DiRezze, B.; Forhan, M.; DiGiacomo, A.; Law, M. The effect of the environment on participation of children and youth with disabilities: A scoping review. Disabil. Rehabil. 2013, 35, 1589–1598. [Google Scholar] [CrossRef]
- Hammel, J.; Magasi, S.; Heinemann, A.; Gray, D.B.; Stark, S.; Kisala, P.; Carlozzi, N.E.; Tulsky, D.; Garcia, S.F.; Hahn, E.A. Environmental barriers and supports to everyday participation: A qualitative insider perspective from people with disabilities. Arch. Phys. Med. Rehabil. 2015, 96, 578–588. [Google Scholar] [CrossRef]
- Law, M.; Anaby, D.R.; Teplicky, R.; Turner, L. Pathways and Resources for Engagement and Participation (PREP): A Practice Model for Occupational Therapists. 2016. Available online: https://www.canchild.ca/en/shop/25-prep (accessed on 1 October 2018).
- Shabat, T.; Fogel-Grinvald, H.; Anaby, D.; Golos, A. Participation profile of children and youth, aged 6–14, with and without ADHD, and the impact of environmental factors. Int. J. Environ. Res. Public Health 2021, 18, 537. [Google Scholar] [CrossRef]
- Anaby, D.R.; Law, M.C.; Majnemer, A.; Feldman, D. Opening doors participation of youth with physical disabilities: An in-tervention study. Can. J. Occup. Ther. 2016, 83, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Anaby, D.R.; Law, M.; Feldman, D.; Majnemer, A.; Avery, L. The effectiveness of the pathways and resources for engagement and participation (PREP) intervention: Improving participation of adolescents with physical disabilities. Dev. Med. Child Neurol. 2018, 60, 513–519. [Google Scholar] [CrossRef] [PubMed]
- Anaby, D.R.; Teplicky, R.; Turner, L.; Law, M.; Avery, L.; Majnemer, A.; Feldman, D. Pathways and resources for engagement and participation (PREP): Improving the participation of youth with disabilities in community-based occupations. Am. J. Occup. Ther. 2019, 73, 7311515320p1. [Google Scholar] [CrossRef]
- Killeen, H.; Anaby, D. The impact of parent involvement on improving participation of children born preterm: The story in the baseline. Contemp. Clin. Trials Commun. 2022, 28, 100942. [Google Scholar] [CrossRef] [PubMed]
- Anaby, D.R.; Vrotsou, K.; Kroksmark, U.; Ellegård, K. Changes in participation patterns of youth with physical disabilities following the pathways and resources for engagement and participation intervention: A time-geography approach. Scand. J. Occup. Ther. 2020, 27, 364–372. [Google Scholar] [CrossRef]
- Anaby, D.R.; Mercerat, C.; Tremblay, S. Enhancing youth participation using the PREP intervention: Parents’ perspectives. Int. J. Environ. Res. Public Health 2017, 14, 1005. [Google Scholar] [CrossRef]
- Sharabi, M.; Kay, A. The relative centrality of life domains among secular, traditionalist and ultra Orthodox (Haredi) men in Israel. Community Work Fam. 2021, 24, 60–76. [Google Scholar] [CrossRef]
- Band-Winterstein, T.; Freund, A. Is it enough to ‘Speak haredi’? cultural sensitivity in social workers encountering Jewish ul-tra-Orthodox clients in Israel. Br. J. Soc. Work 2015, 45, 968–987. [Google Scholar] [CrossRef]
- Novis Deutsch, N.; Rubin, O. Ultra-Orthodox women pursuing higher education: Motivations and challenges. Stud. High. Educ. 2019, 44, 1519–1538. [Google Scholar] [CrossRef]
- Kali, A.; Romi, S. Social Re Evaluation Model: A mechanism for evaluating the social capital of at risk adolescents in an ul-tra Orthodox collective society. Child Youth Serv. 2022, 43, 366–390. [Google Scholar] [CrossRef]
- Golos, A.; Mor, R.; Fisher, O.; Finkelstein, A. Clinicians’ views on the need for cultural adaptation of intervention for children with ADHD from the Ultra-Orthodox community. Occup. Ther. Int. 2021, 21, 1–13. [Google Scholar] [CrossRef]
- Edelstein, O.E.; Band-Winterstein, T.; Bachner, Y.G. The meaning of burden of care in a faith-based community: The case of ultra-Orthodox Jews (UOJ). Aging Ment. Health 2017, 21, 851–861. [Google Scholar] [CrossRef]
- Golos, A.; Sarid, M.; Weill, M.; Yochman, A.; Weintraub, N. The influence of environmental factors on the development of ul-tra-Orthodox preschool boys in Israel. Occup. Ther. Int. 2011, 18, 142–151. [Google Scholar] [CrossRef] [PubMed]
- Budman, J.; Maeir, A. Mothering a child with ADHD in the ultra Orthodox community. Int. J. Environ. Res. Public Health 2022, 19, 14483. [Google Scholar] [CrossRef]
- Patel, K. Mental health implications of COVID-19 on children with disabilities. Asian J. Psychiatr. 2020, 54, 102273. [Google Scholar] [CrossRef] [PubMed]
- Anaby, D.; Ryan, M.; Palisano, R.J.; Levin, M.F.; Gorter, J.W.; Avery, L.; Cormier, I.; Teplicky, R.; Coulter, J.; Hanes, J. Par-ticipation during a pandemic: Forging new pathways. Phys. Occup. Ther. Pediatr. 2021, 41, 115–119. [Google Scholar] [CrossRef]
- Ravens-Sieberer, U.; Kaman, A.; Erhart, M.; Devine, J.; Schlack, R.; Otto, C. Impact of the COVID-19 pandemic on quality of life and mental health in children and adolescents in Germany. Eur. Child Adolesc. Psychiatry 2022, 31, 879–889. [Google Scholar] [CrossRef]
- Masi, A.; Mendoza Diaz, A.; Tully, L.; Azim, S.I.; Woolfenden, S.; Efron, D.; Eapen, V. Impact of the COVID-19 pandemic on the well-being of children with neurodevelopmental disabilities and their parents. J. Paediatr. Child Health 2021, 57, 631–636. [Google Scholar] [CrossRef]
- Jesus, T.S.; Kamalakannan, S.; Bhattacharjya, S.; Bogdanova, S.; Arango-Lasprilla, J.C.; Bentley, J.; Gibson, B.E.; Papadimitriou, C. People with disabilities and other forms of vulnerability to the COVID-19 Pandemic: Study protocol for a scoping review and thematic analysis. Arch. Rehabil. Res. Clin. Transl. 2020, 2, 100079. [Google Scholar] [CrossRef]
- Shadish, W.R.; Rindskopf, D.M. Methods for evidence-based practice: Quantitative synthesis of single-subject designs. New Dir. Eval. 2007, 113, 95–109. [Google Scholar] [CrossRef]
- Iskandar, B.J.; Finnell, R.H. Spina Bifida. N. Engl. J. Med. 2022, 387, 1628. [Google Scholar] [CrossRef]
- Law, M.; Baptiste, S.; Carswell, A.; McCall, M.A.; Polatajko, H.J.; Pollack, N. The Canadian Occupational Performance Measure. Tor. Can. Assoc. Occup. Ther. 2005, 72, 298–300. [Google Scholar]
- McColl, M.A.; Paterson, M.; Davies, D.; Doubt, L.; Law, M. Validity and community utility of the Canadian Occupational Performance Measure. Can. J. Occup. Ther. 2000, 67, 22–30. [Google Scholar] [CrossRef]
- Coster, W.; Law, M.; Bedell, G.M. Participation and Environment Measure for Children and Youth (PEM-CY); Boston University: Boston, MA, USA, 2010. [Google Scholar]
- Coster, W.; Law, M.; Bedell, G.; Khetani, M.; Cousins, M.; Teplicky, R. Development of the participation and environment measure for children and youth: Conceptual basis. Disabil. Rehabil. 2012, 34, 238–246. [Google Scholar] [CrossRef]
- Granger, C.V. The emerging science of functional assessment: Our tool for outcomes analysis. Arch. Phys. Med. Rehabil. 1998, 79, 235–240. [Google Scholar] [CrossRef]
- Linacre, J.M.; Heinemann, A.W.; Wright, B.D.; Granger, C.V.; Hamilton, B.B. The structure and stability of the Functional Independence Measure. Arch. Phys. Med. Rehabil. 1994, 75, 127–132. [Google Scholar] [CrossRef]
- Attkisson, C.C.; Zwick, R. The Client Satisfaction Questionnaire: Psychometric properties and correlations with service utiliza-tion and psychotherapy outcome. Eval. Program Plan. 1982, 5, 233–237. [Google Scholar] [CrossRef] [PubMed]
- Larsen, D.L.; Attkisson, C.C.; Hargreaves, W.A.; Nguyen, T.D. Assessment of client/patient satisfaction: Development of a general scale. Eval. Program Plan. 1979, 2, 197–207. [Google Scholar] [CrossRef]
- IBM. SPSS Statistics for Macintosh, version 26.0; IBM Corp: Armonk, NY, USA, 2019. [Google Scholar]
- Law, M.; Anaby, D.; Imms, C.; Teplicky, R.; Turner, L. Improving the participation of youth with physical disabilities in com-munity activities: An interrupted time series design. Aust. Occup. Ther. J. 2015, 62, 105–115. [Google Scholar] [CrossRef]
- Ottenbacher, K.J. Reliability and accuracy of visually analyzing graphed datafrom single-subject designs. Am. J. Occup. Ther. 1986, 40, 464–469. [Google Scholar] [CrossRef] [PubMed]
- Crowe, M.; Inder, M.; Porter, R. Conducting qualitative research in mental health: Thematic and content analyses. Aust. New Zealand J. Psychiatry 2015, 49, 616–623. [Google Scholar] [CrossRef]
- Vaismoradi, M.; Jones, J.; Turunen, H.; Snelgrove, S. Theme development in qualitative content analysis and thematic analysis. J. Nurs. Educ. Pract. 2016, 6, 100–110. [Google Scholar] [CrossRef]
- Anaby, D.R.; Law, M.; Teplicky, R.; Turner, L. Focusing on the environment To improve youth participation: Experiences and perspectives of occupational therapists. Int. J. Environ. Res. Public Health 2015, 12, 13388–13398. [Google Scholar] [CrossRef]
- Hoehne, C.; Baranski, B.; Benmohammed, L.; Bienstock, L.; Menezes, N.; Margolese, N.; Anaby, D. Changes in overall partici-pation profile of youth with physical disabilities following the PREP intervention. Int. J. Environ. Res. Public Health 2020, 17, 3990. [Google Scholar] [CrossRef]
- Parker Harris, S.; Renko, M.; Caldwell, K. Social entrepreneurship as an employment pathway for people with disabilities: Ex-ploring political–economic and socio-cultural factors. Disabil. Soc. 2014, 29, 1275–1290. [Google Scholar] [CrossRef]
- Lucchetti, G.; Góes, L.G.; Amaral, S.G.; Ganadjian, G.T.; Andrade, I.; Almeida, P.O.A.; do Carmo, V.M.; Manso, M.E.G. Spirituality, religiosity and the mental health consequences of social isolation during Covid-19 pandemic. Int. J. Soc. Psychiatry 2020, 67, 672–679. [Google Scholar] [CrossRef]
- Novak, I.; Mcintyre, S.; Morgan, C.; Campbell, L.; Dark, L.; Morton, N.; Stumbles, E.; Wilson, S.-A.; Goldsmith, S. A systematic review of interventions for children with cerebral palsy: State of the evidence. Dev. Med. Child Neurol. 2013, 55, 885–910. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Goals | Barrier | Environmental Intervention Strategy | |
|---|---|---|---|
| Participant 1 | |||
| Goal 1: Buying sweets at the supermarket for the nephews | Activity: Activity demands | The participant lacked knowledge and experience in navigating within the supermarket, choosing the desired products, and managing money. | OT contacted city welfare department to recruit a tutor for practising shopping at the supermarket, deciding on criteria for selecting desired products, and practice in using money. |
| Participant: Emotional ability | Participant has low motivation and is afraid of new experiences. | OT guided the tutor to support and encourage the participant in practicing this activity, in order to increase his motivation. | |
| Goal 2: Preparing food for family members | Activity: Activity demands | Participant lacked prior knowledge how to organize preparation of food (cooking and baking). | OT guided the sister to rate the complexity of food preparation plans. |
| Environment: Social support | Participant’s mother restrained him from engaging in food preparation activities. | OT recruited the participant’s older sister to allow exposure and encourage the participant to be involved in food preparation. | |
| Goal 3: Participation in prayers in the synagogue | Participant: Emotional ability | The participant was afraid to leave his home and be among people. | OT contacted city welfare department to recruit a tutor for guidance and emotional support when leaving home for prayer at the synagogue. |
| Environment: Physical environment | Parents did not know of a synagogue near the house that was accessible for a wheelchair. | OT encouraged parents to look for an accessible synagogue near their house. | |
| Participant was unfamiliar with safe crossing rules on the road. | OT guided the tutor to accompany the participant and practise with him how to safely cross the road. | ||
| Participant 2 | |||
| Goal 1: Buy clothes with the sister. | Activity: Activity demands | Participant lacked knowledge and had difficulty choosing suitable clothes and managing money. | OT coordinated between the participant and her sister, so that she can be guided during the purchase. |
| Environment: Physical environment | Clothing stores near her home were not accessible for a wheelchair. | OT encouraged shopping in an accessible mall near her house. | |
| Goal 2: Preparing a dish for a family meal according to a recipe. | Activity: Activity demands | Participant had difficulty preparing dishes according to recipes and needed detailed and orderly explanations. | OT shared information with family about use of strategies to organize the required information (via table) and writing recipes. She also taught the mother how to choose easy recipes with the participant. |
| Environment: Physical environment | Products and kitchenware required to prepare food were not accessible to the participant seated in a wheelchair. | OT guided the family to organize and adjust the location of the required products and kitchenware in an accessible manner. | |
| Goal 3: Maintaining social interaction in meetings with peers. | Participant: Cognitive ability | Participant had difficulty initiating social interaction in meetings or telephone conversations with peers. | OT guided participant in strategies to prepare for social interaction by thinking of potential conversation topics. She also contacted an art teacher to conduct a joint creative activity for the participant and other girls. |
| Environment: Physical environment | Lack of accessible places for wheelchairs near the place of residence and at the friend’s house. | OT encouraged the participant and her family to initiate a weekly social gathering at her home. | |
| Category | Sub-Category |
|---|---|
| Personal barriers | (a). Social barriers: Difficulties in communication with peers. |
| (b). Emotional barriers: Feeling low self-efficacy and low motivation. | |
| (c). Cognitive barriers: Difficulties in understanding the activity’s demands. | |
| Environmental barriers | (a). Physical barriers: Lack of accessibility to the physical environment in the community. |
| (b). Social barriers: Attitudes of family and community members. | |
| (c). Cultural barriers: Customs of the UO community. | |
| Factors supporting intervention | (a). Encouragement and support provided by the OT and others. |
| (b). Mediating and imparting knowledge and strategies provided by the OT. | |
| (c). Accessibility and adaptation of the environment and/or the activity. | |
| (d). Practicing activities with others. | |
| (e). Acceptance by others. | |
| Intervention effects | (a). Improved independence. |
| (b). Improved initiative in activities. | |
| (c). Feeling happier and more enjoyment. | |
| (d). Improved confidence and a sense of competence. | |
| (e). Improved communication with others. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Golos, A.; Zyger, C.; Lavie-Pitaro, Y.; Anaby, D. Improving Participation among Youth with Disabilities within Their Unique Socio-Cultural Context during COVID-19 Pandemic: Initial Evaluation. Int. J. Environ. Res. Public Health 2023, 20, 3913. https://doi.org/10.3390/ijerph20053913
Golos A, Zyger C, Lavie-Pitaro Y, Anaby D. Improving Participation among Youth with Disabilities within Their Unique Socio-Cultural Context during COVID-19 Pandemic: Initial Evaluation. International Journal of Environmental Research and Public Health. 2023; 20(5):3913. https://doi.org/10.3390/ijerph20053913
Chicago/Turabian StyleGolos, Anat, Chani Zyger, Yael Lavie-Pitaro, and Dana Anaby. 2023. "Improving Participation among Youth with Disabilities within Their Unique Socio-Cultural Context during COVID-19 Pandemic: Initial Evaluation" International Journal of Environmental Research and Public Health 20, no. 5: 3913. https://doi.org/10.3390/ijerph20053913
APA StyleGolos, A., Zyger, C., Lavie-Pitaro, Y., & Anaby, D. (2023). Improving Participation among Youth with Disabilities within Their Unique Socio-Cultural Context during COVID-19 Pandemic: Initial Evaluation. International Journal of Environmental Research and Public Health, 20(5), 3913. https://doi.org/10.3390/ijerph20053913