

Longitudinal Effects of Screen Time on Depressive Symptoms among Swedish Adolescents: The Moderating and Mediating Role of Coping Engagement Behavior
 ,
,
Abstract

1. Introduction
2. Methods and Materials
2.1. Study Design, Participants and Ethical Considerations
2.2. Procedures and Measurements
2.3. Statistical Analyses
3. Results
3.1. Interaction between Screen Time, Depressive Symptoms and Coping Styles
3.2. Effect Size Interpretation
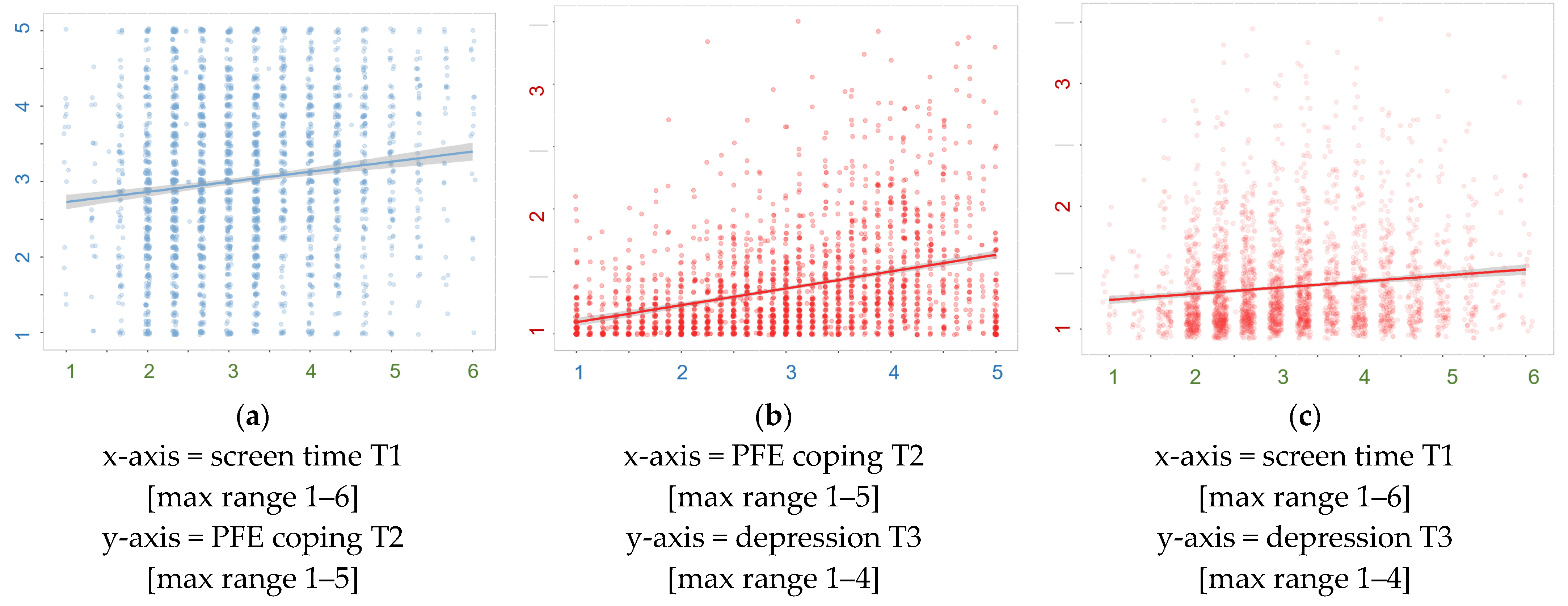
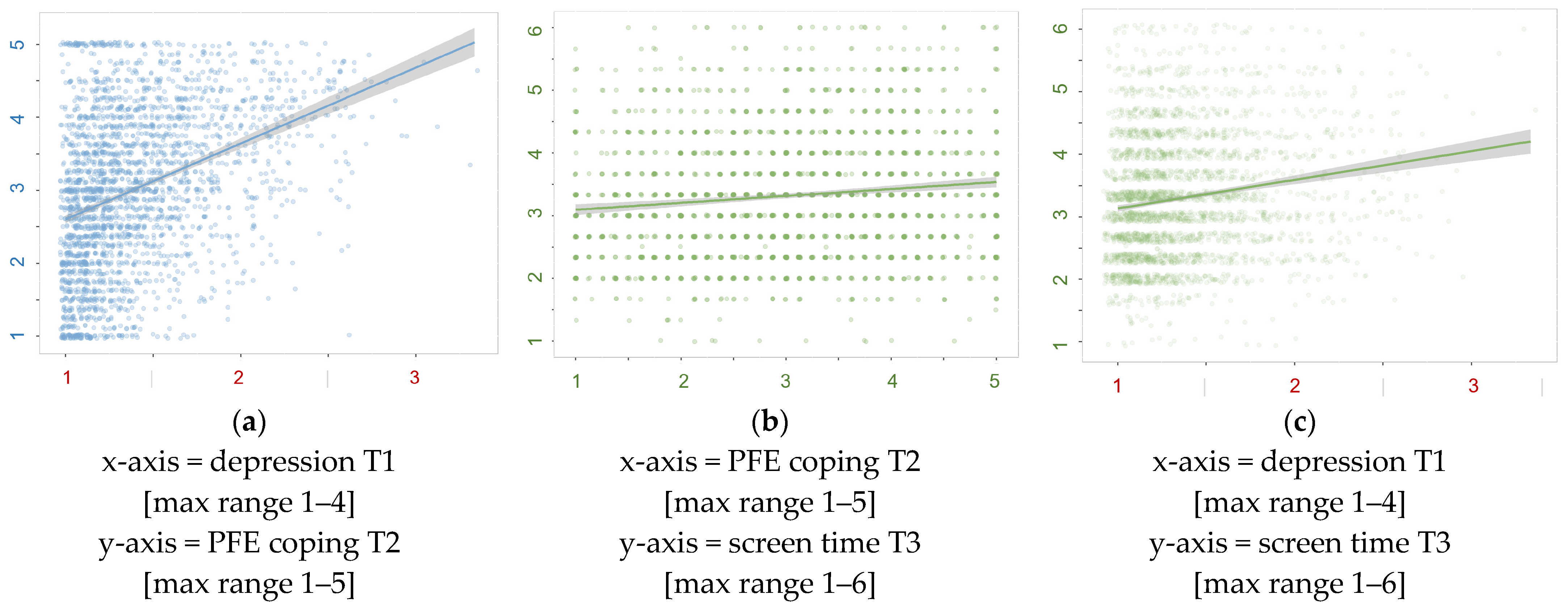
3.3. Pathway Analysis (Post Hoc)
4. Discussion
4.1. Main Findings
4.2. Theoretical Explanations
4.3. Strengths and Limitations
4.4. Implications for Practice and Prevention
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Statistical and Psychometrical Details

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Scale | Cronbach Alpha α | Hierarchical Omega ωh | Total Omega ωt |
|---|---|---|---|
| Screen time T1 | 0.772 | 0.797 | 1.0 |
| Screen time T2 | 0.804 | 0.818 | 1.0 |
| Screen time T3 | 0.799 | 0.813 | 1.0 |
| PFE coping T1 | 0.886 | 0.693 | 0.943 |
| PFE coping T2 | 0.900 | 0.706 | 0.951 |
| PFE coping T3 | 0.906 | 0.730 | 0.955 |
| EFE coping T1 | 0.887 | 0.695 | 0.947 |
| EFE coping T2 | 0.898 | 0.718 | 0.953 |
| EFE coping T3 | 0.903 | 0.707 | 0.955 |
| Depression T1 | 0.908 | 0.786 | 0.931 |
| Depression T2 | 0.915 | 0.751 | 0.935 |
| Depression T3 | 0.923 | 0.792 | 0.941 |
| Scale | T1 Screen | T2 Screen | T3 Screen | T1 PFE | T2 PFE | T3 PFE | T1 EFE | T2 EFE | T3 EFE | T1 Dep | T2 Dep | T3 Dep |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| T1 Screen | 1 | 0.58 | 0.51 | 0.15 | 0.12 | 0.11 | 0.08 | 0.05 | 0.06 | 0.21 | 0.15 | 0.12 |
| T2 Screen | 1 | 0.59 | 0.13 | 0.15 | 0.13 | 0.09 | 0.06 | 0.08 | 0.17 | 0.17 | 0.13 | |
| T3 Screen | 1 | 0.09 | 0.11 | 0.14 | 0.04 | 0.05 | 0.07 | 0.16 | 0.16 | 0.16 | ||
| T1 PFE | 1 | 0.47 | 0.41 | 0.59 | 0.29 | 0.25 | 0.39 | 0.30 | 0.24 | |||
| T2 PFE | 1 | 0.47 | 0.27 | 0.59 | 0.29 | 0.30 | 0.33 | 0.27 | ||||
| T3 PFE | 1 | 0.23 | 0.27 | 0.55 | 0.28 | 0.28 | 0.32 | |||||
| T1 EFE | 1 | 0.42 | 0.37 | 0.17 | 0.13 | 0.11 | ||||||
| T2 EFE | 1 | 0.44 | 0.14 | 0.15 | 0.13 | |||||||
| T3 EFE | 1 | 0.11 | 0.12 | 0.15 | ||||||||
| T1 Dep | 1 | 0.72 | 0.60 | |||||||||
| T2 Dep | 1 | 0.70 | ||||||||||
| T3 Dep | 1 |


| ROW | T1 VAR | T2 VAR | T3 VAR | IV | DV | B | BETA | p |
|---|---|---|---|---|---|---|---|---|
| 1 | St1 | St2 | Screen_t1 | Screen_t2 | 0.533 | 0.557 | <0.001 | |
| 2 | St2 | St3 | Screen_t2 | Screen_t3 | 0.421 | 0.430 | <0.001 | |
| 3 | St1 | St3 | Screen_t1 | Screen_t3 | 0.227 | 0.243 | <0.001 | |
| 4 | Ct1 | Ct2 | PFE_t1 | PFE_t2 | 0.390 | 0.396 | <0.001 | |
| 5 | Ct2 | Ct3 | PFE_t2 | PFE_t3 | 0.299 | 0.302 | <0.001 | |
| 6 | Ct1 | Ct3 | PFE_t1 | PFE_t3 | 0.224 | 0.229 | <0.001 | |
| 7 | Dt1 | Dt2 | Dep_t1 | Dep_t2 | 0.671 | 0.708 | <0.001 | |
| 8 | Dt2 | Dt3 | Dep_t2 | Dep_t3 | 0.566 | 0.549 | <0.001 | |
| 9 | Dt1 | Dt3 | Dep_t1 | Dep_t3 | 0.205 | 0.209 | <0.001 | |
| 10 (A-path) | St1 | Ct2 | Screen_t1 | PFE_t2 | 0.031 | 0.032 | 0.079 | |
| 11 | St1 | Dt2 | Screen_t1 | Dep_t2 | −0.001 | −0.004 | 0.782 | |
| 12 | Ct1 | St2 | PFE_t1 | Screen_t2 | 0.021 | 0.022 | 0.230 | |
| 13 | Ct1 | Dt2 | PFE_t1 | Dep_t2 | 0.009 | 0.024 | 0.110 | |
| 14 | Dt1 | St2 | Dep_t1 | Screen_t2 | 0.128 | 0.050 | 0.009 | |
| 15 (A-path) | Dt1 | Ct2 | Dep_t1 | PFE_t2 | 0.369 | 0.140 | 0.000 | |
| 16 | St2 | Ct3 | Screen_t2 | PFE_t3 | 0.020 | 0.021 | 0.347 | |
| 17 | St2 | Dt3 | Screen_t2 | Dep_t3 | 0.005 | 0.013 | 0.444 | |
| 18 (B-path) | Ct2 | St3 | PFE_t2 | Screen_t3 | −0.006 | −0.007 | 0.719 | |
| 19 (B-path) | Ct2 | Dt3 | PFE_t2 | Dep_t3 | 0.011 | 0.030 | 0.063 | |
| 20 | Dt2 | St3 | Dep_t2 | Screen_t3 | 0.148 | 0.056 | 0.017 | |
| 21 | Dt2 | Ct3 | Dep_t2 | PFE_t3 | 0.270 | 0.098 | 0.001 | |
| 22 | St1 | Ct3 | Screen_t1 | PFE_t3 | 0.005 | 0.005 | 0.797 | |
| 23 (C-path) | St1 | Dt3 | Screen_t1 | Dep_t3 | −0.007 | −0.018 | 0.280 | |
| 24 | Ct1 | St3 | PFE_t1 | Screen_t3 | −0.011 | −0.012 | 0.520 | |
| 25 | Ct1 | Dt3 | PFE_t1 | Dep_t3 | −0.006 | −0.016 | 0.328 | |
| 26 (C-path) | Dt1 | St3 | Dep_t1 | Screen_t3 | 0.018 | 0.007 | 0.767 | |
| 27 | Dt1 | Ct3 | Dep_t1 | PFE_t3 | 0.032 | 0.012 | 0.630 |
| Nr | T1 VAR | T1 TYPE | T2 VAR | T2 TYPE | T3 VAR | T3 TYPE | IV | DV | B | BETA | p |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 28 | St1 | Med | Ct2 | Ct2 | Med | Dt3 | m2_dc × m1_cs | m2_m1_dcs | 0.000 | 0.001 | 0.018 |
| 29 | St1 | Med | Dt2 | Dt2 | Med | Ct3 | m2_cd × m1_ds | m2_m1_cds | 0.000 | 0.000 | 0.817 |
| 30 | Ct1 | Med | St2 | St2 | Med | Dt3 | m2_ds × m1_sc | m2_m1_dsc | 0.000 | 0.000 | 0.635 |
| 32 | Dt1 | Med | St2 | St2 | Med | Ct3 | m2_cs × m1_sd | m2_m1_csd | 0.003 | 0.001 | 0.279 |
| 32 | Ct1 | Med | Dt2 | Dt2 | Med | St3 | m2_sd × m1_dc | m2_m1_sdc | 0.001 | 0.001 | 0.163 |
| 33 | Dt1 | Med | Ct2 | Ct2 | Med | St3 | m2_sc × m1_cd | m2_m1_scd | −0.002 | −0.001 | 0.771 |
| 34 | St1 | Total | Ct2 | Total | Dt3 | Total | d_ds + (m2_dc × m1_cs) | total_dcs | −0.006 | −0.017 | 0.307 |
| 35 | St1 | Total | Dt2 | Total | Ct3 | Total | d_cs + (m2_cd × m1_ds) | total_cds | 0.005 | 0.005 | 0.810 |
| 36 | Ct1 | Total | St2 | Total | Dt3 | Total | d_dc + (m2_ds × m1_sc) | total_dsc | −0.006 | −0.016 | 0.337 |
| 37 | Ct1 | Total | Dt2 | Total | St3 | Total | d_sc + (m2_sd × m1_dc) | total_sdc | −0.010 | −0.011 | 0.569 |
| 38 | Dt1 | Total | St2 | Total | Ct3 | Total | d_cd + (m2_cs × m1_sd) | total_csd | 0.035 | 0.013 | 0.603 |
| 39 | Dt1 | Total | Ct2 | Total | St3 | Total | d_sd + (m2_sc × m1_cd) | total_scd | 0.016 | 0.006 | 0.796 |
| Nr | T1 VAR | T1 COV | T2 VAR | T2 COV | T3 VAR | T3 COV | IV | DV | B | BETA | p |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 40 | St1 | St1 | Screen_t1 | Screen_t1 | 1.049 | 1.000 | <0.001 | ||||
| 41 | Ct1 | Ct1 | PFE_t1 | PFE_t1 | 1.033 | 1.000 | <0.001 | ||||
| 42 | Ct1 | St1 | PFE_t1 | Screen_t1 | 0.159 | 0.153 | <0.001 | ||||
| 43 | Dt1 | Dt1 | Dep_t1 | Dep_t1 | 0.144 | 1.000 | <0.001 | ||||
| 44 | Dt1 | St1 | Dep_t1 | Screen_t1 | 0.083 | 0.213 | <0.001 | ||||
| 45 | Dt1 | Ct1 | Dep_t1 | PFE_t1 | 0.155 | 0.403 | <0.001 | ||||
| 46 | St2 | St2 | Screen_t2 | Screen_t2 | 0.643 | 0.671 | <0.001 | ||||
| 47 | Ct2 | Ct2 | PFE_t2 | PFE_t2 | 0.775 | 0.773 | <0.001 | ||||
| 48 | Ct2 | St2 | PFE_t2 | Screen_t2 | 0.057 | 0.081 | <0.001 | ||||
| 49 | Dt2 | Dt2 | Dep_t2 | Dep_t2 | 0.063 | 0.486 | <0.001 | ||||
| 50 | Dt2 | St2 | Dep_t2 | Screen_t2 | 0.022 | 0.110 | <0.001 | ||||
| 51 | Dt2 | Ct2 | Dep_t2 | PFE_t2 | 0.049 | 0.224 | <0.001 | ||||
| 52 | St3 | St3 | Screen_t3 | Screen_t3 | 0.570 | 0.622 | <0.001 | ||||
| 53 | Ct3 | Ct3 | PFE_t3 | PFE_t3 | 0.728 | 0.737 | <0.001 | ||||
| 54 | Ct3 | St3 | PFE_t3 | Screen_t3 | 0.037 | 0.058 | <0.001 | ||||
| 55 | Dt3 | Dt3 | Dep_t3 | Dep_t3 | 0.067 | 0.483 | <0.001 | ||||
| 56 | Dt3 | St3 | Dep_t3 | Screen_t3 | 0.022 | 0.113 | <0.001 | ||||
| 57 | Dt3 | Ct3 | Dep_t3 | PFE_t3 | 0.055 | 0.249 | <0.001 |
References
- Castelpietra, G.; Knudsen, A.K.S.; Agardh, E.E.; Armocida, B.; Beghi, M.; Iburg, K.M.; Logroscino, G.; Ma, R.; Starace, F.; Steel, N.; et al. The Burden of Mental Disorders, Substance Use Disorders and Self-Harm among Young People in Europe, 1990–2019: Findings from the Global Burden of Disease Study 2019. Lancet Reg. Health Eur. 2022, 16, 100341. [Google Scholar] [CrossRef]
- Kessler, R.C.; Amminger, G.P.; Aguilar-Gaxiola, S.; Alonso, J.; Lee, S.; Ustün, T.B. Age of Onset of Mental Disorders: A Review of Recent Literature. Curr. Opin. Psychiatry 2007, 20, 359–364. [Google Scholar] [CrossRef]
- Fichter, M.M.; Kohlboeck, G.; Quadflieg, N.; Wyschkon, A.; Esser, G. From Childhood to Adult Age: 18-Year Longitudinal Results and Prediction of the Course of Mental Disorders in the Community. Soc. Psychiatry Psychiatr. Epidemiol. 2009, 44, 792–803. [Google Scholar] [CrossRef]
- The National Board of Health and Welfare. The Development of Mental Ill-Health among Children and Young Adults: Up Util 2016; The National Board of Health and Welfare: Stockholm, Sweden, 2017; p. 26. (In Swedish) [Google Scholar]
- Public Health Agency of Sweden. Why Have Mental Health Problems Increased among Children and Youth in Sweden? The Development during the Period 1985–2014; Public Health Agency of Sweden: Solna, Sweden, 2018. (In Swedish) [Google Scholar]
- The National Board of Health and Welfare. Long-Term Consequences of Being Afflicted with Depression or Anxiety Syndrome in Young Age; The National Board of Health and Welfare: Stockholm, Sweden, 2021; p. 9. (In Swedish) [Google Scholar]
- Fineberg, N.; Demetrovics, Z.; Stein, D.; Ioannidis, K.; Potenza, M.; Grünblatt, E.; Brand, M.; Billieux, J.; Carmi, L.; King, D.; et al. Manifesto for a European Research Network into Problematic Usage of the Internet. Eur. Neuropsychopharmacol. 2018, 28, 1232–1246. [Google Scholar] [CrossRef]
- World Health Organization. Public Health Implications of Excessive Use of the Internet, Computers, Smartphones and Similar Electronic Devices: Meeting Report, Main Meeting Hall, Foundation for Promotion of Cancer Research, National Cancer Research Centre, Tokyo, Japan, 27–29 August 2014; World Health Organization: Geneva, Switzerland, 2015; ISBN 978-92-4-150936-7. [Google Scholar]
- World Health Organization. Preventing Suicide: A Global Imperative; World Health Organization: Geneva, Switzerland, 2014; ISBN 978-92-4-156477-9. [Google Scholar]
- Hawton, K.; van Heeringen, K. Suicide. Lancet Lond. Engl. 2009, 373, 1372–1381. [Google Scholar] [CrossRef]
- Twenge, J.M.; Martin, G.N. Gender Differences in Associations between Digital Media Use and Psychological Well-being: Evidence from Three Large Datasets. J. Adolesc. 2020, 79, 91–102. [Google Scholar] [CrossRef]
- Oswald, T.K.; Rumbold, A.R.; Kedzior, S.G.E.; Moore, V.M. Psychological Impacts of “Screen Time” and “Green Time” for Children and Adolescents: A Systematic Scoping Review. PLoS ONE 2020, 15, e0237725. [Google Scholar] [CrossRef]
- Männikkö, N.; Ruotsalainen, H.; Miettunen, J.; Marttila-Tornio, K.; Kääriäinen, M. Parental Socioeconomic Status, Adolescents’ Screen Time and Sports Participation through Externalizing and Internalizing Characteristics. Heliyon 2020, 6, e03415. [Google Scholar] [CrossRef]
- Savolainen, I.; Oksanen, A.; Kaakinen, M.; Sirola, A.; Paek, H.-J. The Role of Perceived Loneliness in Youth Addictive Behaviors: Cross-National Survey Study. JMIR Ment. Health 2020, 7, e14035. [Google Scholar] [CrossRef]
- Paulus, F.W.; Ohmann, S.; von Gontard, A.; Popow, C. Internet Gaming Disorder in Children and Adolescents: A Systematic Review. Dev. Med. Child Neurol. 2018, 60, 645–659. [Google Scholar] [CrossRef]
- Sahu, M.; Gandhi, S.; Sharma, M.K. Mobile Phone Addiction Among Children and Adolescents: A Systematic Review. J. Addict. Nurs. 2019, 30, 261–268. [Google Scholar] [CrossRef]
- Nielsen, P.; Favez, N.; Liddle, H.; Rigter, H. Linking Parental Mediation Practices to Adolescents’ Problematic Online Screen Use: A Systematic Literature Review. J. Behav. Addict. 2019, 8, 649–663. [Google Scholar] [CrossRef]
- Seo, D.G.; Park, Y.; Kim, M.K.; Park, J. Mobile Phone Dependency and Its Impacts on Adolescents’ Social and Academic Behaviors. Comput. Hum. Behav. 2016, 63, 282–292. [Google Scholar] [CrossRef]
- Moge, C.E.; Romano, D.M. Contextualising Video Game Engagement and Addiction in Mental Health: The Mediating Roles of Coping and Social Support. Heliyon 2020, 6, e05340. [Google Scholar] [CrossRef]
- Kaess, M.; Klar, J.; Kindler, J.; Parzer, P.; Brunner, R.; Carli, V.; Sarchiapone, M.; Hoven, C.W.; Apter, A.; Balazs, J.; et al. Excessive and Pathological Internet Use—Risk-Behavior or Psychopathology? Addict. Behav. 2021, 123, 107045. [Google Scholar] [CrossRef]
- Tang, S.; Werner-Seidler, A.; Torok, M.; Mackinnon, A.J.; Christensen, H. The Relationship between Screen Time and Mental Health in Young People: A Systematic Review of Longitudinal Studies. Clin. Psychol. Rev. 2021, 86, 102021. [Google Scholar] [CrossRef]
- Alonzo, R.; Hussain, J.; Stranges, S.; Anderson, K.K. Interplay between Social Media Use, Sleep Quality, and Mental Health in Youth: A Systematic Review. Sleep Med. Rev. 2021, 56, 101414. [Google Scholar] [CrossRef]
- Houghton, S.; Lawrence, D.; Hunter, S.C.; Rosenberg, M.; Zadow, C.; Wood, L.; Shilton, T. Reciprocal Relationships between Trajectories of Depressive Symptoms and Screen Media Use during Adolescence. J. Youth Adolesc. 2018, 47, 2453–2467. [Google Scholar] [CrossRef]
- Boers, E.; Afzali, M.H.; Newton, N.; Conrod, P. Association of Screen Time and Depression in Adolescence. JAMA Pediatr. 2019, 173, 853–859. [Google Scholar] [CrossRef]
- Fung, I.C.-H.; Blankenship, E.B.; Ahweyevu, J.O.; Cooper, L.K.; Duke, C.H.; Carswell, S.L.; Jackson, A.M.; Jenkins, J.C.; Duncan, E.A.; Liang, H.; et al. Public Health Implications of Image-Based Social Media: A Systematic Review of Instagram, Pinterest, Tumblr, and Flickr. Perm. J. 2020, 24, 307. [Google Scholar] [CrossRef]
- Marchant, A.; Hawton, K.; Stewart, A.; Montgomery, P.; Singaravelu, V.; Lloyd, K.; Purdy, N.; Daine, K.; John, A. A Systematic Review of the Relationship between Internet Use, Self-Harm and Suicidal Behaviour in Young People: The Good, the Bad and the Unknown. PLoS ONE 2017, 12, e0181722. [Google Scholar] [CrossRef]
- Hökby, S.; Hadlaczky, G.; Westerlund, J.; Wasserman, D.; Balazs, J.; Germanavicius, A.; Machín, N.; Meszaros, G.; Sarchiapone, M.; Värnik, A.; et al. Are Mental Health Effects of Internet Use Attributable to the Web-Based Content or Perceived Consequences of Usage? A Longitudinal Study of European Adolescents. JMIR Ment. Health 2016, 3, e31. [Google Scholar] [CrossRef]
- Hale, L.; Guan, S. Screen Time and Sleep among School-Aged Children and Adolescents: A Systematic Literature Review. Sleep Med. Rev. 2015, 21, 50–58. [Google Scholar] [CrossRef]
- Guerrero, M.D.; Barnes, J.D.; Chaput, J.-P.; Tremblay, M.S. Screen Time and Problem Behaviors in Children: Exploring the Mediating Role of Sleep Duration. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 105. [Google Scholar] [CrossRef]
- Yang, J.; Fu, X.; Liao, X.; Li, Y. Association of Problematic Smartphone Use with Poor Sleep Quality, Depression, and Anxiety: A Systematic Review and Meta-Analysis. Psychiatry Res. 2020, 284, 112686. [Google Scholar] [CrossRef]
- Viner, R.M.; Gireesh, A.; Stiglic, N.; Hudson, L.D.; Goddings, A.-L.; Ward, J.L.; Nicholls, D.E. Roles of Cyberbullying, Sleep, and Physical Activity in Mediating the Effects of Social Media Use on Mental Health and Wellbeing among Young People in England: A Secondary Analysis of Longitudinal Data. Lancet Child Adolesc. Health 2019, 3, 685–696. [Google Scholar] [CrossRef]
- Sampasa-Kanyinga, H.; Colman, I.; Goldfield, G.S.; Janssen, I.; Wang, J.; Podinic, I.; Tremblay, M.S.; Saunders, T.J.; Sampson, M.; Chaput, J.-P. Combinations of Physical Activity, Sedentary Time, and Sleep Duration and Their Associations with Depressive Symptoms and Other Mental Health Problems in Children and Adolescents: A Systematic Review. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 72. [Google Scholar] [CrossRef]
- Twenge, J.M.; Farley, E. Not All Screen Time Is Created Equal: Associations with Mental Health Vary by Activity and Gender. Soc. Psychiatry Psychiatr. Epidemiol. 2021, 56, 207–217. [Google Scholar] [CrossRef]
- Wang, X.; Li, Y.; Fan, H. The Associations between Screen Time-Based Sedentary Behavior and Depression: A Systematic Review and Meta-Analysis. BMC Public Health 2019, 19, 1524. [Google Scholar] [CrossRef]
- Zink, J.; Belcher, B.R.; Imm, K.; Leventhal, A.M. The Relationship between Screen-Based Sedentary Behaviors and Symptoms of Depression and Anxiety in Youth: A Systematic Review of Moderating Variables. BMC Public Health 2020, 20, 472. [Google Scholar] [CrossRef]
- Archer, T.; Wentz, K. Internet-Video Gaming: Symptoms, Epidemiology, Neurophysiology and Interventional Aspects. J. Child Adolesc. Behav. 2017, 5, 345. [Google Scholar] [CrossRef]
- Shin, M.; Juventin, M.; Wai Chu, J.T.; Manor, Y.; Kemps, E. Online Media Consumption and Depression in Young People: A Systematic Review and Meta-Analysis. Comput. Hum. Behav. 2022, 128, 107129. [Google Scholar] [CrossRef]
- Shahidin, S.H.; Midin, M.; Sidi, H.; Choy, C.L.; Nik Jaafar, N.R.; Mohd Salleh Sahimi, H.; Che Roos, N.A. The Relationship between Emotion Regulation (ER) and Problematic Smartphone Use (PSU): A Systematic Review and Meta-Analyses. Int. J. Environ. Res. Public. Health 2022, 19, 15848. [Google Scholar] [CrossRef]
- McNicol, M.L.; Thorsteinsson, E.B. Internet Addiction, Psychological Distress, and Coping Responses Among Adolescents and Adults. Cyberpsychol. Behav. Soc. Netw. 2017, 20, 296–304. [Google Scholar] [CrossRef]
- Bányai, F.; Zsila, Á.; Kökönyei, G.; Griffiths, M.D.; Demetrovics, Z.; Király, O. The Moderating Role of Coping Mechanisms and Being an E-Sport Player Between Psychiatric Symptoms and Gaming Disorder: Online Survey. JMIR Ment. Health 2021, 8, e21115. [Google Scholar] [CrossRef]
- Tamres, L.K.; Janicki, D.; Helgeson, V.S. Sex Differences in Coping Behavior: A Meta-Analytic Review and an Examination of Relative Coping. Personal. Soc. Psychol. Rev. 2002, 6, 2–30. [Google Scholar] [CrossRef]
- Connor-Smith, J.K.; Flachsbart, C. Relations between Personality and Coping: A Meta-Analysis. J. Pers. Soc. Psychol. 2007, 93, 1080–1107. [Google Scholar] [CrossRef]
- Carver, C.S.; Connor-Smith, J. Personality and Coping. Annu. Rev. Psychol. 2010, 61, 679–704. [Google Scholar] [CrossRef]
- Kelly, M.M.; Tyrka, A.R.; Price, L.H.; Carpenter, L.L. Sex Differences in the Use of Coping Strategies: Predictors of Anxiety and Depressive Symptoms. Depress. Anxiety 2008, 25, 839–846. [Google Scholar] [CrossRef]
- Wasserman, D.; Hoven, C.W.; Wasserman, C.; Wall, M.; Eisenberg, R.; Hadlaczky, G.; Kelleher, I.; Sarchiapone, M.; Apter, A.; Balazs, J.; et al. School-Based Suicide Prevention Programmes: The SEYLE Cluster-Randomised, Controlled Trial. Lancet 2015, 385, 1536–1544. [Google Scholar] [CrossRef]
- Paykel, E.S.; Myers, J.K.; Lindenthal, J.J.; Tanner, J. Suicidal Feelings in the General Population: A Prevalence Study. Br. J. Psychiatry 1974, 124, 460–469. [Google Scholar] [CrossRef]
- Fonseca-Pedrero, E.; Pérez de Albéniz, A. Assessment of suicidal behavior in adolescents: The Paykel suicide scale. Papeles Psicól. Psychol. Pap. 2020, 41, 106–115. [Google Scholar] [CrossRef]
- Swedish Research Council for Health, Working Life and Welfare. Adolescents’ and Young Adults’ Living Conditions in Sweden: A Review of the Knowledge with Focus on Inequality; Swedish Research Council for Health, Working Life and Welfare: Stockholm, Sweden, 2018; p. 120. (In Swedish) [Google Scholar]
- Beck, A.T.; Steer, R.A.; Brown, G.K. Manual for the BDI-II; The Psychological Corporation: San Antonio, TX, USA, 1996; pp. 10–1037. [Google Scholar]
- Wang, Y.-P.; Gorenstein, C. Psychometric Properties of the Beck Depression Inventory-II: A Comprehensive Review. Rev. Bras. Psiquiatr. Sao Paulo Braz. 1999 2013, 35, 416–431. [Google Scholar] [CrossRef]
- Tobin, D.L. Scoring Information for the CSI-S: Coping Strategies Inventory 32 Item. Available online: https://pdfcoffee.com/coping-strategies-inventory-32-item-pdf-free.html (accessed on 22 November 2022).
- Tobin, D.L. User’s Manual for the Coping Strategies Inventory; Ohio University: Athens, OH, USA, 1984. [Google Scholar]
- Tobin, D.L.; Holroyd, K.A.; Reynolds, R.V.; Wigal, J.K. The Hierarchical Factor Structure of the Coping Strategies Inventory. Cogn. Ther. Res. 1989, 13, 343–361. [Google Scholar] [CrossRef]
- Kattimani, S.; Sarkar, S.; Rajkumar, R.P.; Menon, V. Stressful Life Events, Hopelessness, and Coping Strategies among Impulsive Suicide Attempters. J. Neurosci. Rural Pract. 2015, 6, 171–176. [Google Scholar] [CrossRef]
- Speyer, E.; Morgenstern, H.; Hayashino, Y.; Kerr, P.G.; Rayner, H.; Robinson, B.M.; Pisoni, R.L. Reliability and Validity of the Coping Strategy Inventory-Short Form Applied to Hemodialysis Patients in 13 Countries: Results from the Dialysis Outcomes and Practice Patterns Study (DOPPS). J. Psychosom. Res. 2016, 91, 12–19. [Google Scholar] [CrossRef]
- Addison, C.; Campbell-Jenkins, B.; Sarpong, D.; Kibler, J.; Singh, M.; Dubbert, P.; Wilson, G.; Payne, T.; Taylor, H. Psychometric Evaluation of a Coping Strategies Inventory Short-Form (CSI-SF) in the Jackson Heart Study Cohort. Int. J. Environ. Res. Public. Health 2007, 4, 289–295. [Google Scholar] [CrossRef]
- Asendorpf, J.B.; van de Schoot, R.; Denissen, J.J.A.; Hutteman, R. Reducing Bias Due to Systematic Attrition in Longitudinal Studies: The Benefits of Multiple Imputation. Int. J. Behav. Dev. 2014, 38, 453–460. [Google Scholar] [CrossRef]
- Kalkbrenner, M.T. Alpha, Omega, and H Internal Consistency Reliability Estimates: Reviewing These Options and When to Use Them. Couns. Outcome Res. Eval. 2021, 14, 77–88. [Google Scholar] [CrossRef]
- Garson, D.G. Longitudinal Analysis, 2013th ed.; Statistical Associates Blue Book Series; Statistical Associates Publishing: Asheboro, NC, USA, 2013. [Google Scholar]
- Garson, D.G. Generalized Linear Models/Generalized Estimating Equations, 2013th ed.; Statistical Associates Blue Book Series; Statistical Associates Publishing: Asheboro, NC, USA, 2013. [Google Scholar]
- Rosseel, Y. Lavaan: An R Package for Structural Equation Modeling. J. Stat. Softw. 2012, 48, 1–36. [Google Scholar] [CrossRef]
- Rosseel, Y. Lavaan Latent Variable Analysis. Available online: https://lavaan.ugent.be/tutorial/index.html (accessed on 22 November 2022).
- Ryan, R.M.; Rigby, C.S.; Przybylski, A. The Motivational Pull of Video Games: A Self-Determination Theory Approach. Motiv. Emot. 2006, 30, 344–360. [Google Scholar] [CrossRef]
- Lobel, A. The Relation Between Gaming and the Development of Emotion Regulation Skills. Ph.D. Thesis, Radboud University Nijmegen, Nijmegen, The Netherlands, 2016. [Google Scholar]
- Pelletier-Baldelli, A.; Ives, L.; Mittal, V.A. Increased Internet Use and Poorer Ability to Manage Emotions in Youth at High-Risk for Psychosis. Schizophr. Res. Cogn. 2015, 2, 220–226. [Google Scholar] [CrossRef]
- Snodgrass, J.G.; Lacy, M.G.; Dengah, H.J.F.; Eisenhauer, S.; Batchelder, G.; Cookson, R.J. A Vacation from Your Mind: Problematic Online Gaming Is a Stress Response. Comput. Hum. Behav. 2014, 38, 248–260. [Google Scholar] [CrossRef]
- Yldz, M. Emotion Regulation Strategies as Predictors of Internet Addiction and Smartphone Addiction in Adolescents. J. Educ. Sci. Psychol. 2017, 12, 66–78. [Google Scholar]
- Sohn, S.Y.; Rees, P.; Wildridge, B.; Kalk, N.J.; Carter, B. Prevalence of Problematic Smartphone Usage and Associated Mental Health Outcomes amongst Children and Young People: A Systematic Review, Meta-Analysis and GRADE of the Evidence. BMC Psychiatry 2019, 19, 356. [Google Scholar] [CrossRef]
- King, D.L.; Chamberlain, S.R.; Carragher, N.; Billieux, J.; Stein, D.; Mueller, K.; Potenza, M.N.; Rumpf, H.J.; Saunders, J.; Starcevic, V.; et al. Screening and Assessment Tools for Gaming Disorder: A Comprehensive Systematic Review. Clin. Psychol. Rev. 2020, 77, 101831. [Google Scholar] [CrossRef]
- Allebeck, P. The Prevention Paradox or the Inequality Paradox? Eur. J. Public Health 2008, 18, 215. [Google Scholar] [CrossRef]
- Zhang, J.-T.; Ma, S.-S.; Li, C.-S.R.; Liu, L.; Xia, C.-C.; Lan, J.; Wang, L.-J.; Liu, B.; Yao, Y.-W.; Fang, X.-Y. Craving Behavioral Intervention for Internet Gaming Disorder: Remediation of Functional Connectivity of the Ventral Striatum: CBI Remediated FC of VS in IGD. Addict. Biol. 2018, 23, 337–346. [Google Scholar] [CrossRef]



| Parameter | b | 95% CI (Wald) | S.E. | p | PVMR Difference 1 |
|---|---|---|---|---|---|
| Intercept | 0.347 * | 0.295 to 0.400 | 0.0268 | <0.001 | |
| TIME = 3 | −0.029 * | −0.047 to −0.01 | 0.0093 | 0.002 | −0.055 |
| TIME = 2 | −0.012 | −0.028 to 0.003 | 0.0079 | 0.125 | n.s. |
| TIME = 1 (ref) | Ref. | Ref. | Ref. | Ref. | Ref. |
| (Gender = Girls) | 0.131 * | 0.119 to 0.142 | 0.0059 | <0.001 | +0.201 |
| (Gender = Boys) | Ref. | Ref. | Ref. | Ref. | Ref. |
| Socioeconomic status (SES) | −0.063 * | −0.071 to −0.054 | 0.0041 | <0.001 | 1-unit −0.100; Max-Min −0.399 |
| Screen time | 0.005 | −0.009 to 0.019 | 0.007 | 0.469 | n.s. |
| Problem-Focused Coping (PFE) | 0.030 * | 0.014 to 0.046 | 0.0081 | <0.001 | 1-unit +0.097; Max-Min +0.292 |
| Emotion-Focused Coping (EFE) | −0.001 | −0.016 to 0.014 | 0.0074 | 0.895 | n.s. |
| (Time = 3) × Screen time × PFE | 0.009 * | 0.003 to 0.015 | 0.0029 | 0.003 | 1-unit +0.065; Max-Min +0.447 |
| (Time = 2) × Screen time × PFE | 0.009 * | 0.003 to 0.014 | 0.0026 | 0.001 | 1-unit +0.057; Max-Min +0.375 |
| (Time = 1) × Screen time × PFE | 0.011 * | 0.006 to 0.017 | 0.0027 | <0.001 | 1-unit +0.076; Max-Min +0.519 |
| (Time = 3) × Screen time × EFE | −0.002 | −0.007 to 0.004 | 0.0027 | 0.559 | n.s. |
| (Time = 2) × Screen time × EFE | −0.003 | −0.008 to 0.002 | 0.0024 | 0.263 | n.s. |
| (Time = 1) × Screen time × EFE | −0.003 | −0.008 to 0.002 | 0.0024 | 0.262 | n.s. |
| PVMR Values 1 | Screen Time 1–1.99 | Screen Time 2–2.99 | Screen Time 3–3.99 | Screen Time 4–4.99 | Screen Time 5–6.00 |
|---|---|---|---|---|---|
| PFE 1–1.99 | 1.18 | 1.19 | 1.20 | 1.22 | 1.25 |
| PFE 2–2.99 | 1.23 | 1.26 | 1.29 | 1.32 | 1.35 |
| PFE 3–3.99 | 1.30 | 1.34 | 1.39 | 1.43 | 1.49 |
| PFE 4–5.00 | 1.40 | 1.42 | 1.48 | 1.55 | 1.63 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hökby, S.; Westerlund, J.; Alvarsson, J.; Carli, V.; Hadlaczky, G. Longitudinal Effects of Screen Time on Depressive Symptoms among Swedish Adolescents: The Moderating and Mediating Role of Coping Engagement Behavior. Int. J. Environ. Res. Public Health 2023, 20, 3771. https://doi.org/10.3390/ijerph20043771
Hökby S, Westerlund J, Alvarsson J, Carli V, Hadlaczky G. Longitudinal Effects of Screen Time on Depressive Symptoms among Swedish Adolescents: The Moderating and Mediating Role of Coping Engagement Behavior. International Journal of Environmental Research and Public Health. 2023; 20(4):3771. https://doi.org/10.3390/ijerph20043771
Chicago/Turabian StyleHökby, Sebastian, Joakim Westerlund, Jesper Alvarsson, Vladimir Carli, and Gergö Hadlaczky. 2023. "Longitudinal Effects of Screen Time on Depressive Symptoms among Swedish Adolescents: The Moderating and Mediating Role of Coping Engagement Behavior" International Journal of Environmental Research and Public Health 20, no. 4: 3771. https://doi.org/10.3390/ijerph20043771
APA StyleHökby, S., Westerlund, J., Alvarsson, J., Carli, V., & Hadlaczky, G. (2023). Longitudinal Effects of Screen Time on Depressive Symptoms among Swedish Adolescents: The Moderating and Mediating Role of Coping Engagement Behavior. International Journal of Environmental Research and Public Health, 20(4), 3771. https://doi.org/10.3390/ijerph20043771