
Peer Intervention following Suicide-Related Emergency Department Presentation: Evaluation of the PAUSE Pilot Program


Abstract
1. Introduction
1.1. Peer Worker Intervention Models
1.2. Brook RED
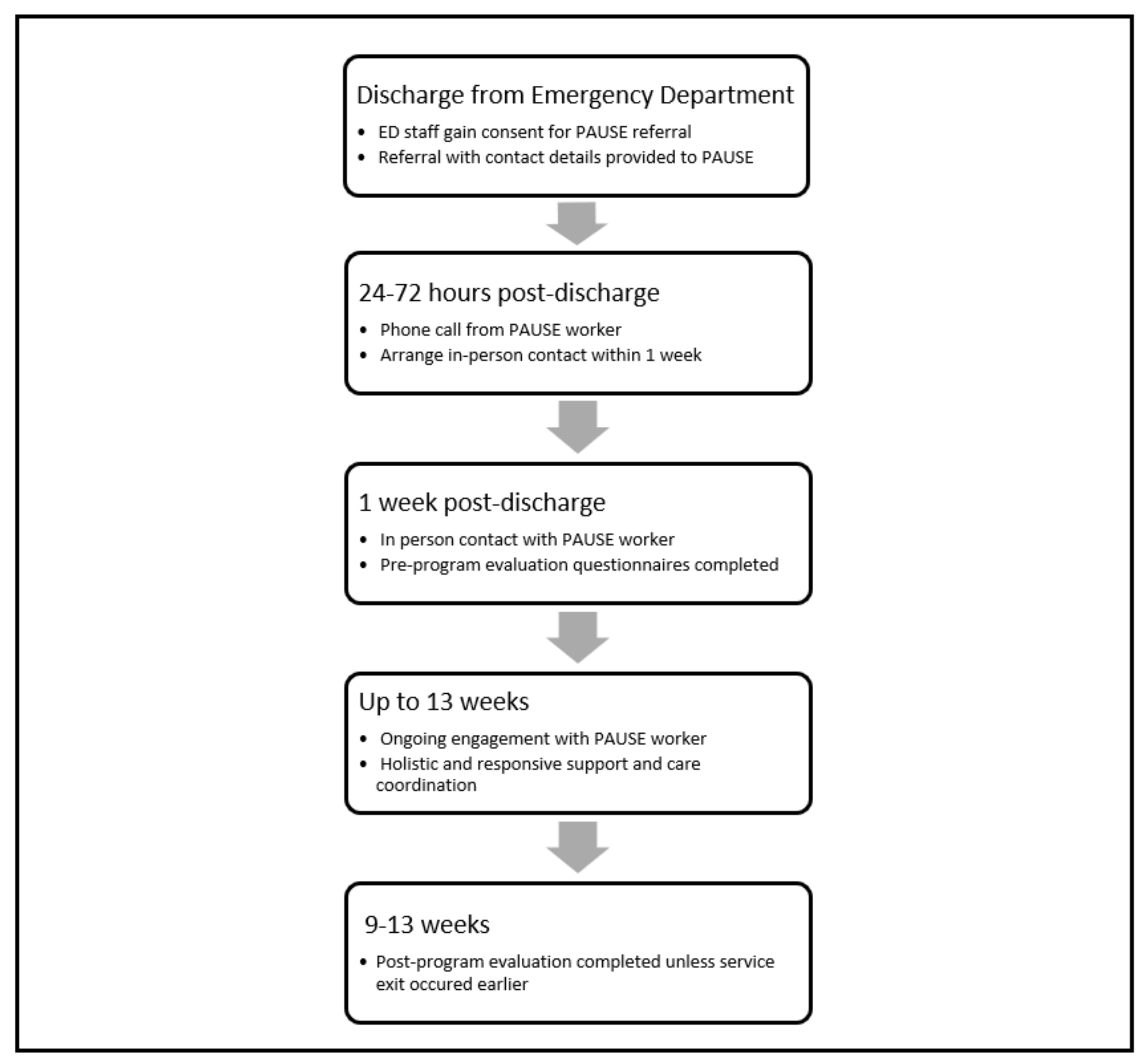
1.3. PAUSE Program
2. Materials and Methods
2.1. Participants and Study Population
2.2. Evaluation Questionnaire
2.2.1. General Health Questionnaire Suicide Scale (GHQ-28-SS)
2.2.2. Adult Hope Scale (AHS)
2.2.3. Kessler Psychological Distress Scale—10 (K10)
2.3. Statistical Analyses
2.4. PAUSE Experience Questionnaire
2.5. Semi-Structured Interviews
3. Results
3.1. Participants
3.2. Evaluation Questionnaires
3.2.1. Suicidal Ideation
3.2.2. Hope
3.2.3. Psychological Distress
3.3. PAUSE Experience Questionnaire
3.4. Semi-Structured Interviews
“I got referred to the PAUSE program and I’ve now actually reached that point where I’ve not hurt myself at all.”
3.4.1. PAUSE Workers Provided Holistic and Responsive Assistance
“She’s setting up an appointment for me to get some financial counselling. She has set up appointments with my psychologist and my psychiatrist, but like she just wants to help, so she was like, well sounds like you need a medication review with some counsellors. I gave her their information and she helped to arrange everything, that was very helpful.”
“I haven’t actually reached that point as often where I really, really need to go to them. To the point where I really sort of contact for moral support sort of, “have you been through this, how did you deal with it? Okay, do you reckon that might work for me? You know. Just a casual talk.”
3.4.2. PAUSE Workers Better Understood Participants Due to Their Lived Experience
3.4.3. Treated like a Person Rather Than a Client by PAUSE Workers
“It’s not like a formal setting where you’re with a psychologist or something, it’s like a weird in-between, just talking to someone, and talking to a professional. It’s a lot calmer and you feel like you can open up a bit better.”
3.4.4. PAUSE Facilitated Ongoing Social Connection
“If I thought I unfortunately may end up back in hospital, I know that there’s always that number. I find that comforting. Whereas with a psychologist and stuff like that, you obviously can’t do that.”
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bostwick, J.M.; Pabbati, C.; Geske, J.R.; Mckean, A.J. Suicide Attempt as a Risk Factor for Completed Suicide: Even More Lethal Than We Knew. Am. J. Psychiatry 2016, 173, 1094–1100. [Google Scholar] [CrossRef]
- Leske, S.; Adam, G.; Catakovic, A.; Weir, B.; Kõlves, K. Suicide in Queensland: Annual Report 2022. Available online: https://www.griffith.edu.au/__data/assets/pdf_file/0033/1639473/AISRAP-Annual-Report-2022.pdf (accessed on 18 November 2022).
- Olfson, M.; Wall, M.; Wang, S.; Crystal, S.; Liu, S.-M.; Gerhard, T.; Blanco, C. Short-term Suicide Risk After Psychiatric Hospital Discharge. JAMA Psychiatry 2016, 73, 1119–1126. [Google Scholar] [CrossRef]
- Chung, D.; Ryan, C.J.; Hadzi-Pavlovic, D.; Singh, S.P.; Stanton, C.; Large, M.M. Suicide Rates After Discharge from Psychiatric Facilities. JAMA Psychiatry 2017, 74, 694–702. [Google Scholar] [CrossRef]
- Qin, P.; Nordentoft, M. Suicide Risk in Relation to Psychiatric Hospitalization. Arch. Gen. Psychiatry 2005, 62, 427–432. [Google Scholar] [CrossRef]
- Hunt, I.M.; Kapur, N.; Webb, R.; Robinson, J.; Burns, J.; Shaw, J.; Appleby, L. Suicide in recently discharged psychiatric patients: A case-control study. Psychol. Med. 2009, 39, 443–449. [Google Scholar] [CrossRef]
- National Mental Health Commission. Fifth-National-Mental-Health-and-Suicide-Prevention-Plan. 2017; pp. 1–84. Available online: https://www.mentalhealthcommission.gov.au/getmedia/0209d27b-1873-4245-b6e5-49e770084b81/Fifth-National-Mental-Health-and-Suicide-Prevention-Plan.pdf (accessed on 10 June 2019).
- Falcone, G.; Nardella, A.; Lamis, D.A.; Erbuto, D.; Girardi, P.; Pompili, M. Taking care of suicidal patients with new technologies and reaching-out means in the post-discharge period. World J. Psychiatry 2017, 7, 163–176. [Google Scholar] [CrossRef]
- Scanlan, J.N.; Hancock, N.; Honey, A. Evaluation of a peer-delivered, transitional and post-discharge support program following psychiatric hospitalisation. BMC Psychiatry 2017, 17, 307. [Google Scholar] [CrossRef]
- Sveticic, J.; De Leo, D. The hypothesis of a continuum in suicidality: A discussion on its validity and practical implications. Ment. Illn. 2012, 4, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Segal-Engelchin, D.; Kfir-Levin, N.; Neustaedter, S.B.; Mirsky, J. Mental Pain Among Female Suicide Attempt Survivors in Israel: An Exploratory Qualitative Study. Int. J. Ment. Health Addict. 2015, 13, 423–434. [Google Scholar] [CrossRef]
- Peterson, D.H.M.; Collings, S.C. “It’s either do it or die”: The role of self-management of suicidality in people with experience of mental illness. Cris. J. Cris. Interv. Suicide Prev. 2015, 36, 173–178. [Google Scholar] [CrossRef] [PubMed]
- Milner, A.; Page, A.; LaMontagne, A.D. Cause and effect in studies on unemployment, mental health and suicide: A meta-analytic and conceptual review. Psychol. Med. 2014, 44, 909–917. [Google Scholar] [CrossRef] [PubMed]
- Cavanaugh, C.E.; Messing, J.T.; Del-Colle, M.; O’Sullivan, C.; Campbell, J.C. Prevalence and Correlates of Suicidal Behavior among Adult Female Victims of Intimate Partner Violence. Suicide Life-Threat. Behav. 2011, 41, 372–383. [Google Scholar] [CrossRef] [PubMed]
- Bickley, H.; Hunt, I.M.; Windfuhr, K.; Shaw, J.; Appleby, L.; Kapur, N. Suicide Within Two Weeks of Discharge from Psychiatric Inpatient Care: A Case-Control Study. Psychiatr. Serv. 2013, 64, 653–659. [Google Scholar] [CrossRef] [PubMed]
- De Leo, D. DSM-V and the Future of Suicidology. Crisis 2011, 32, 233–239. [Google Scholar] [CrossRef]
- Hawgood, J.; De Leo, D. Suicide Prediction—A Shift in Paradigm Is Needed. Crisis 2016, 37, 251–255. [Google Scholar] [CrossRef]
- Davidson, L.; Chinman, M.; Sells, D.; Rowe, M. Peer Support Among Adults with Serious Mental Illness: A Report from the Field. Schizophr. Bull. 2006, 32, 443–450. [Google Scholar] [CrossRef]
- Ehrlich, C.; Slattery, M.; Vilic, G.; Chester, P.; Crompton, D. What happens when peer support workers are introduced as members of community-based clinical mental health service delivery teams: A qualitative study. J. Interprof. Care 2019, 34, 107–115. [Google Scholar] [CrossRef]
- Pitt, V.; Lowe, D.; Hill, S.; Prictor, M.; Hetrick, S.E.; Ryan, R.; Berends, L. Consumer-providers of care for adult clients of statutory mental health services. Cochrane Database Syst. Rev. 2013, 2013, CD004807. [Google Scholar] [CrossRef]
- Fuhr, D.C.; Salisbury, T.T.; De Silva, M.J.; Atif, N.; van Ginneken, N.; Rahman, A.; Patel, V. Effectiveness of peer-delivered interventions for severe mental illness and depression on clinical and psychosocial outcomes: A systematic review and meta-analysis. Soc. Psychiatry Psychiatr. Epidemiol. 2014, 49, 1691–1702. [Google Scholar] [CrossRef]
- Gillard, S.; Foster, R.; Gibson, S.; Goldsmith, L.; Marks, J.; White, S. Describing a principles-based approach to developing and evaluating peer worker roles as peer support moves into mainstream mental health services. Ment. Health Soc. Incl. 2017, 21, 133–143. [Google Scholar] [CrossRef]
- Klee, A.; Chinman, M.; Kearney, L. Peer specialist services: New frontiers and new roles. Psychol. Serv. 2019, 16, 353–359. [Google Scholar] [CrossRef] [PubMed]
- Gill, K.J.; Burns-Lynch, W.; Murphy, A.A.; Swarbrick, M. Delineation of the job role. J. Rehabil. 2009, 75, 23. [Google Scholar]
- Chinman, M.; George, P.; Dougherty, R.H.; Daniels, A.S.; Ghose, S.S.; Swift, A.; Delphin-Rittmon, M.E. Peer Support Services for Individuals with Serious Mental Illnesses: Assessing the Evidence. Psychiatr. Serv. 2014, 65, 429–441. [Google Scholar] [CrossRef] [PubMed]
- Macdonald, S.; Sampson, C.; Turley, R.; Biddle, L.; Ring, N.; Begley, R.; Evans, R. Patients’ Experiences of Emergency Hospital Care Following Self-Harm: Systematic Review and Thematic Synthesis of Qualitative Research. Qual. Health Res. 2020, 30, 471–485. [Google Scholar] [CrossRef]
- Lindgren, B.-M.; Svedin, C.G.; Werkö, S. A Systematic Literature Review of Experiences of Professional Care and Support Among People Who Self-Harm. Arch. Suicide Res. 2018, 22, 173–192. [Google Scholar] [CrossRef]
- Bellamy, C.; Schmutte, T.; Davidson, L. An update on the growing evidence base for peer support. Ment. Health Soc. Incl. 2017, 21, 161–167. [Google Scholar] [CrossRef]
- Solomon, P. Peer Support/Peer Provided Services Underlying Processes, Benefits, and Critical Ingredients. Psychiatr. Rehabil. J. 2004, 27, 392–401. [Google Scholar] [CrossRef]
- Gillard, S.; Gibson, S.; Holley, J.; Lucock, M. Developing a change model for peer worker interventions in mental health services: A qualitative research study. Epidemiol. Psychiatr. Sci. 2014, 24, 435–445. [Google Scholar] [CrossRef]
- Rimkeviciene, J.; Hawgood, J.; O’Gorman, J.; De Leo, D. Personal Stigma in Suicide Attempters. Death Stud. 2015, 39, 592–599. [Google Scholar] [CrossRef]
- Chen, C.H.; Tseng, Y.F.; Chou, F.H.; Wang, S.Y. Effects of support group intervention in postnatally distressed women: A controlled study in Taiwan. J. Psychosom. Res. 2000, 49, 395–399. [Google Scholar] [CrossRef]
- Preyde, M.; Ardal, F. Effectiveness of a parent “buddy” program for mothers of very preterm infants in a neonatal intensive care unit. Can. Med. Assoc. J. 2003, 168, 969–973. [Google Scholar]
- Forchuk, C.; Martin, M.-L.; Chan, Y.L.; Jensen, E. Therapeutic relationships: From psychiatric hospital to community. J. Psychiatr. Ment. Health Nurs. 2005, 12, 556–564. [Google Scholar] [CrossRef] [PubMed]
- Pfeiffer, P.N.; King, C.; Ilgen, M.; Ganoczy, D.; Clive, R.; Garlick, J.; Abraham, K.; Kim, H.M.; Vega, E.; Ahmedani, B.; et al. Development and pilot study of a suicide prevention intervention delivered by peer support specialists. Psychol. Serv. 2019, 16, 360–371. [Google Scholar] [CrossRef] [PubMed]
- Lawn, S.; Smith, A.; Hunter, K. Mental health peer support for hospital avoidance and early discharge: An Australian example of consumer driven and operated service. J. Ment. Health 2008, 17, 498–508. [Google Scholar] [CrossRef]
- Huisman, A.; van Bergen, D.D. Peer specialists in suicide prevention: Possibilities and pitfalls. Psychol. Serv. 2019, 16, 372–380. [Google Scholar] [CrossRef]
- Gibson, M.; Crompton, D. Peer-Support after Suicide-Related Emergency Presentation: Evaluation of the PAUSE Pilot. 2020. Available online: https://51889018-c1d2-4dd3-bafc-dba0c7d13f0c.usrfiles.com/ugd/518890_efbbac9c43734515a66255d5d7eeeec3.pdf (accessed on 10 February 2022).
- Byrne, L.; Wykes, T. A role for lived experience mental health leadership in the age of COVID-19. J. Ment. Health 2020, 29, 243–246. [Google Scholar] [CrossRef]
- Brasier, C.; Roennfeldt, H.; Hamilton, B.; Martel, A.; Hill, N.; Stratford, A.; Buchanan-Hagen, S.; Byrne, L.; Castle, D.; Cocks, N.; et al. Peer support work for people experiencing mental distress attending the emergency department: Exploring the potential. Emerg. Med. Australas. 2022, 34, 78–84. [Google Scholar] [CrossRef]
- Cutcliffe, J.R.; Links, P.S.; Harder, H.G.; Balderson, K.; Bergmans, Y.; Eynan, R.; Ambreen, M.; Nisenbaum, R. Understanding the Risks of Recent Discharge. Crisis 2012, 33, 21–29. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics (ABS). Logan 2021 Census All Persons QuickStats. 2021. Available online: https://www.abs.gov.au/census/find-census-data/quickstats/2021/LGA34590 (accessed on 10 February 2022).
- Watson, D.; Goldney, R.; Fisher, L.; Merritt, M. The Measurement of Suicidal Ideation. Crisis 2001, 22, 12–14. [Google Scholar] [CrossRef]
- Goldney, R.D.; Winefield, A.H.; Tiggemann, M.; Winefield, H.R.; Smith, S. Suicidal ideation in a young adult population. Acta Psychiatr. Scand. 1989, 79, 481–489. [Google Scholar] [CrossRef]
- Cook, J.A.; Steigman, P.; Pickett, S.; Diehl, S.; Fox, A.; Shipley, P.; MacFarlane, R.; Grey, D.D.; Burke-Miller, J.K. Randomized controlled trial of peer-led recovery education using Building Recovery of Individual Dreams and Goals through Education and Support (BRIDGES). Schizophr. Res. 2012, 136, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Anestis, M.D.; Moberg, F.B.; Arnau, R.C. Hope and the Interpersonal-Psychological Theory of Suicidal Behavior: Replication and Extension of Prior Findings. Suicide Life-Threat. Behav. 2014, 44, 175–187. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Barker, P.R.; Colpe, L.J.; Epstein, J.F.; Gfroerer, J.C.; Hiripi, E.; Howes, M.J.; Normand, S.-L.T.; Manderscheid, R.W.; Walters, E.E.; et al. Screening for Serious Mental Illness in the General Population. Arch. Gen. Psychiatry 2003, 60, 184–189. [Google Scholar] [CrossRef] [PubMed]
- Andersen, L.S.; Grimsrud, A.; Myer, L.; Williams, D.R.; Stein, D.J.; Seedat, S. The psychometric properties of the K10 and K6 scales in screening for mood and anxiety disorders in the South African Stress and Health study. Int. J. Methods Psychiatr. Res. 2011, 20, 215–223. [Google Scholar] [CrossRef]
- Andrews, G.; Slade, T. Interpreting scores on the Kessler Psychological Distress Scale (K10). Aust. New Zealand J. Public Health 2001, 25, 494–497. [Google Scholar] [CrossRef]
- Sunderland, M.; Mahoney, A.; Andrews, G. Investigating the Factor Structure of the Kessler Psychological Distress Scale in Community and Clinical Samples of the Australian Population. J. Psychopathol. Behav. Assess. 2012, 34, 253–259. [Google Scholar] [CrossRef]
- Chinman, M.; McCarthy, S.; Mitchell-Miland, C.; Daniels, K.; Youk, A.; Edelen, M. Early stages of development of a peer specialist fidelity measure. Psychiatr. Rehabil. J. 2016, 39, 256–265. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Schlichthorst, M.; Ozols, I.; Reifels, L.; Morgan, A. Lived experience peer support programs for suicide prevention: A systematic scoping review. Int. J. Ment. Health Syst. 2020, 14, 65. [Google Scholar] [CrossRef]
- Gidugu, V.; Rogers, E.S.; Harrington, S.; Maru, M.; Johnson, G.; Cohee, J.; Hinkel, J. Individual Peer Support: A Qualitative Study of Mechanisms of Its Effectiveness. Community Ment. Health J. 2015, 51, 445–452. [Google Scholar] [CrossRef]
- Bowden, M.; McCoy, A.; Reavley, N. Suicidality and suicide prevention in culturally and linguistically diverse (CALD) communities: A systematic review. Int. J. Ment. Health 2019, 49, 293–320. [Google Scholar] [CrossRef]
- Johnson, R.B.; Oxendine, S.; Taub, D.J.; Robertson, J. Suicide Prevention for LGBT Students. New Dir. Stud. Serv. 2013, 2013, 55–69. [Google Scholar] [CrossRef]
- Cleary, A. Help-seeking patterns and attitudes to treatment amongst men who attempted suicide. J. Ment. Health 2017, 26, 220–224. [Google Scholar] [CrossRef] [PubMed]
- Schrijvers, D.L.; Bollen, J.; Sabbe, B.G. The gender paradox in suicidal behavior and its impact on the suicidal process. J. Affect. Disord. 2012, 138, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Rutz, W.; Rihmer, Z. Suicidality in men-practical issues, challenges, solutions. J. Men’s Heal Gend. 2007, 4, 393–401. [Google Scholar] [CrossRef]
- Struszczyk, S.; Galdas, P.M.; Tiffin, P.A. Men and suicide prevention: A scoping review. J. Ment. Health 2019, 28, 80–88. [Google Scholar] [CrossRef] [PubMed]
- Tsai, J.; Cao, X. Association between suicide attempts and homelessness in a population-based sample of US veterans and non-veterans. J. Epidemiol. Community Health 2019, 73, 346–352. [Google Scholar] [CrossRef]
- De Berardis, D.; Martinotti, G.; Di Giannantonio, M. Editorial: Understanding the Complex Phenomenon of Suicide: From Research to Clinical Practice. Front. Psychiatry 2018, 9, 61. [Google Scholar] [CrossRef]


{kind=link}
| Referred N | Engaged N | X2 | df | p | |
|---|---|---|---|---|---|
| Gender | 1.528 | 1 | 0.466 | ||
| Men | 127 | 54 | |||
| Women | 186 | 88 | |||
| Indigenous status | 3.376 | 1 | 0.066 | ||
| First Nations | 16 | 4 | |||
| Non-Indigenous | 232 | 113 | |||
| CALD background | 1.615 | 1 | 0.204 | ||
| CALD identification | 37 | 22 | |||
| Other | 265 | 120 | |||
| Referral Reason | 1.887 | 2 | 0.389 | ||
| Mental illness history | 58 | 23 | |||
| Situational crisis | 81 | 41 | |||
| Both | 58 | 29 |
| Outcome Measure | N | M | SD |
|---|---|---|---|
| GHQ-28-SS | 53 | 9.15 | 3.02 |
| AHS | 53 | 31.1 | 14.16 |
| K10 | 36 | 32.99 | 7.89 |
| Variable | N | Pre | Post | Wilcoxon Signed-Rank Test | |||
|---|---|---|---|---|---|---|---|
| M | SD | M | SD | Z | p | ||
| GHQ-SS | 33 | 9.30 | 3.15 | 4.52 | 3.09 | 4.842 | <0.001 * |
| AHS | 32 | 32.49 | 13.2 | 39.19 | 11.04 | 2.789 | 0.005 * |
| K10 | 21 | 38.48 | 9.37 | 32.05 | 10.85 | 2.627 | 0.009 * |
| Peer Action | Experienced by Participants | Action Effectiveness | ||
|---|---|---|---|---|
| Not at All | A Little/Fairly | Very Helpful | ||
| My PAUSE worker shared aspects of their own illness or recovery story with me. | 82.4% | 0% | 42.3% | 57.7% |
| My PAUSE worker told me about strategies that they have tried or used. | 86.1% | 7.4% | 40.7 | 51.9% |
| My PAUSE worker understood my experiences because they have had similar experiences. | 85.7% | 0% | 33.3% | 66.7% |
| My PAUSE worker made me feel like the work I do toward my recovery is valid and valued. | 100% | 3.4% | 13.8% | 82.8% |
| I felt a sense of belonging with my PAUSE worker. | 94.3% | 0% | 22.2% | 77.8% |
| I felt a sense of connection with my PAUSE worker. | 100% | 0% | 27.6% | 72.4% |
| My PAUSE worker learned some things from me when we worked together. | 91.4% | 0% | 38.4% | 61.5% |
| My peer worker helped me to see that I have a lot of skills for recovery and life. | 94.4% | 0% | 39.3% | 60.7% |
| Knowing that my peer worker has overcome challenges made me feel like I could too. | 91.7% | 10.3% | 24.1% | 65.5% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gibson, M.; Moreau, N.; Balzamo, E.; Crompton, D. Peer Intervention following Suicide-Related Emergency Department Presentation: Evaluation of the PAUSE Pilot Program. Int. J. Environ. Res. Public Health 2023, 20, 3763. https://doi.org/10.3390/ijerph20043763
Gibson M, Moreau N, Balzamo E, Crompton D. Peer Intervention following Suicide-Related Emergency Department Presentation: Evaluation of the PAUSE Pilot Program. International Journal of Environmental Research and Public Health. 2023; 20(4):3763. https://doi.org/10.3390/ijerph20043763
Chicago/Turabian StyleGibson, Mandy, Nick Moreau, Eschleigh Balzamo, and David Crompton. 2023. "Peer Intervention following Suicide-Related Emergency Department Presentation: Evaluation of the PAUSE Pilot Program" International Journal of Environmental Research and Public Health 20, no. 4: 3763. https://doi.org/10.3390/ijerph20043763
APA StyleGibson, M., Moreau, N., Balzamo, E., & Crompton, D. (2023). Peer Intervention following Suicide-Related Emergency Department Presentation: Evaluation of the PAUSE Pilot Program. International Journal of Environmental Research and Public Health, 20(4), 3763. https://doi.org/10.3390/ijerph20043763