
Intra-Oral Photograph Analysis for Gingivitis Screening in Orthodontic Patients


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Participants
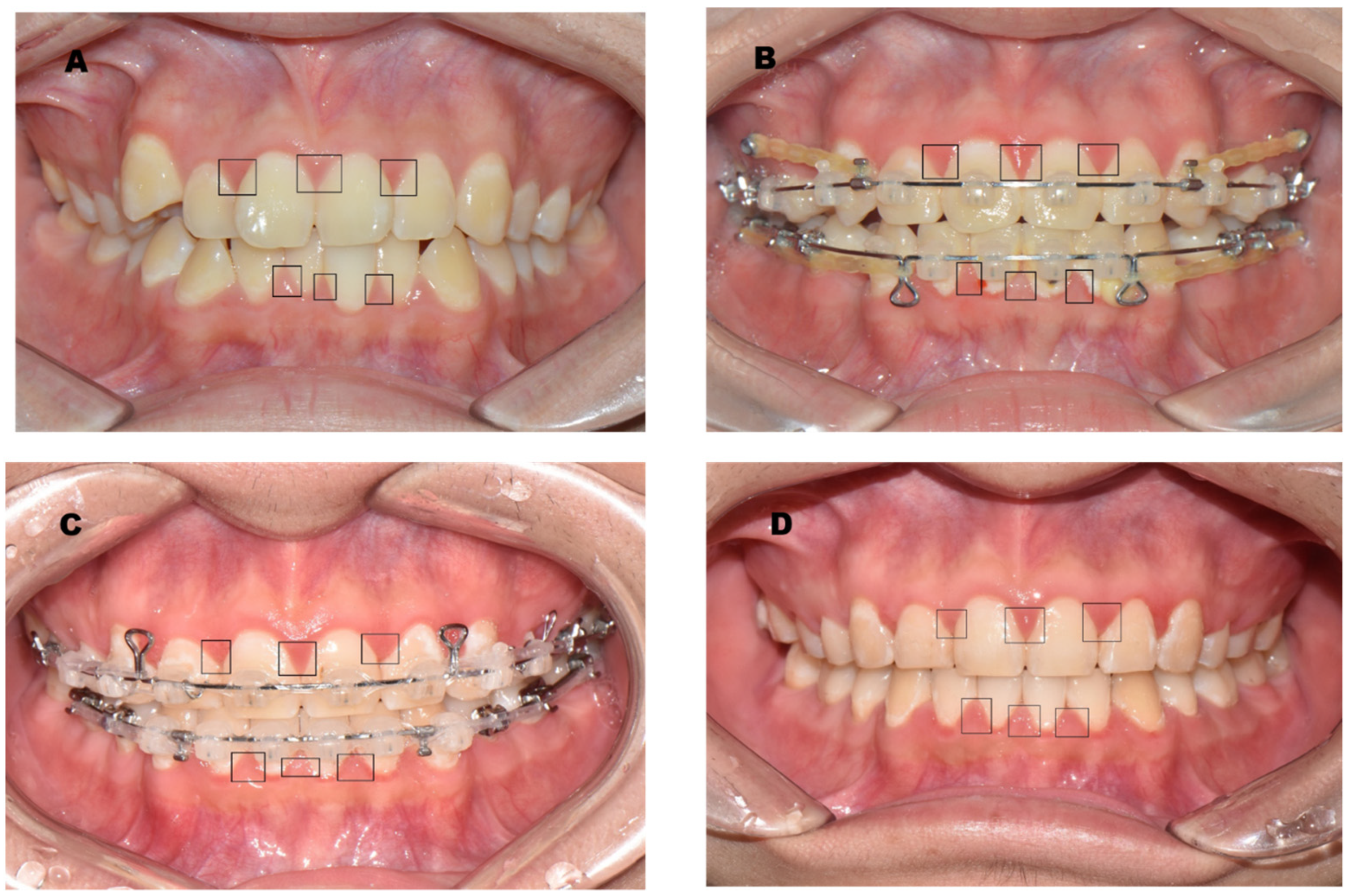
2.2. Targeted Gingiva
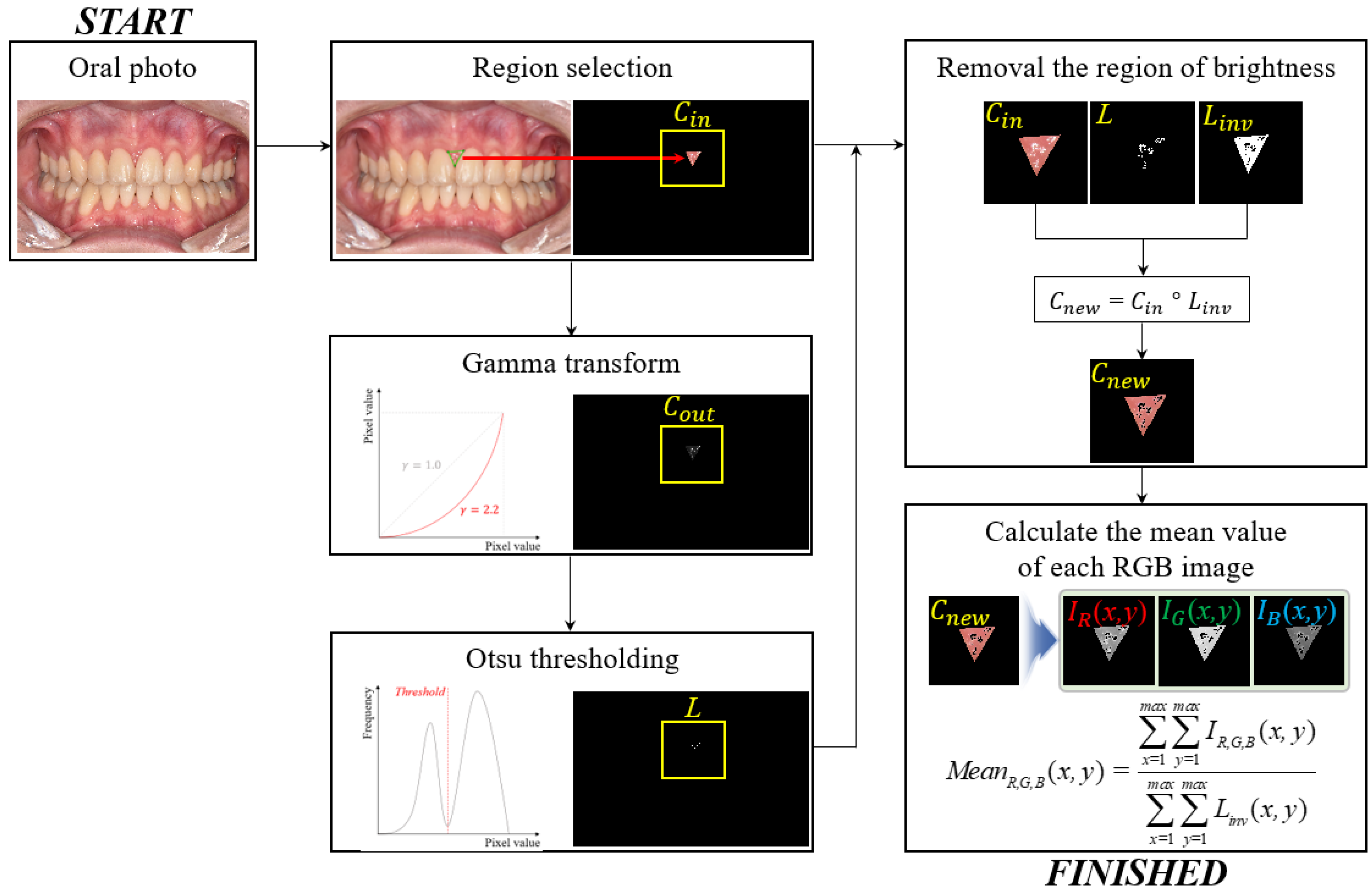
2.3. Proposed Framework to Measure the Redness
2.4. Modified Gingival Index (GI)
2.5. Statistical Methods
3. Results
3.1. General Characteristics
3.2. Gingival Index (GI)
3.3. R/G Ratio
3.4. Correlation between the GI and R/G Values
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Baelum, V. Dentistry and population approaches for preventing dental diseases. J. Dent. 2011, 39, S9–S19. [Google Scholar] [CrossRef]
- Landry, R.G.; Jean, M. Periodontal Screening and Recording (PSR) Index: Precursors, utility and limitations in a clinical setting. Int. Dent. J. 2002, 52, 35–40. [Google Scholar] [CrossRef]
- Eke, P.I.; Wei, L.; Borgnakke, W.S.; Thornton-Evans, G.; Zhang, X.Y.; Lu, H.; Mcguire, L.C.; Genco, R.J. Periodontitis prevalence in adults >= 65 years of age, in the USA. Periodontology 2000 2016, 72, 76–95. [Google Scholar] [CrossRef]
- Loe, H.; Silness, J. Periodontal disease in pregnancy I. Prevalence and severity. Acta Odontol. Scand. 1963, 21, 533–551. [Google Scholar] [CrossRef] [PubMed]
- Corbet, E.F.; Ho, D.K.L.; Lai, S.M.L. Radiographs in periodontal disease diagnosis and management. Aust. Dent. J. 2009, 54, S27–S43. [Google Scholar] [CrossRef]
- Highfield, J. Diagnosis and classification of periodontal disease. Aust. Dent. J. 2009, 54, S11–S26. [Google Scholar] [CrossRef]
- Schmalz, G.; Li, S.; Burkhardt, R.; Rinke, S.; Krause, F.; Haak, R.; Ziebolz, D. MicroRNAs as salivary markers for periodontal diseases: A new diagnostic approach? BioMed Res. Int. 2016, 2016, 1027525. [Google Scholar] [CrossRef]
- Xiang, X.; Sowa, M.G.; Lacopino, A.M.; Maev, R.G.; Hewko, M.D.; Man, A.; Liu, K.Z. An Update on Novel Non-Invasive Approaches for Periodontal Diagnosis. J. Periodontol. 2010, 81, 186–198. [Google Scholar] [CrossRef]
- Elashiry, M.; Meghil, M.M.; Cutler, C.W. From manual periodontal probing to digital 3-D imaging to endoscopic capillaroscopy: Recent advances in periodontal disease diagnosis. J. Periodontal Res. 2019, 54, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Trombelli, L.; Farina, R.; Silva, C.O.; Tatakis, D.N. Plaque-induced gingivitis: Case definition and diagnostic considerations. J. Clin. Periodontol. 2018, 45, S44–S67. [Google Scholar] [CrossRef] [PubMed]
- Revilla-León, M.; Gómez-Polo, M.; Barmak, A.B.; Inam, W.; Kan, J.Y.; Kois, J.C.; Akal, O. Artificial intelligence models for diagnosing gingivitis and periodontal disease: A systematic review. J. Prosthetic Dent. 2022, in press. [Google Scholar] [CrossRef]
- Chang, H.S.; Walsh, L.J.; Freer, T.J. Enamel demineralization during orthodontic treatment. Aetiology and prevention. Aust. Dent. J. 1997, 42, 322–327. [Google Scholar] [CrossRef]
- Paolantonio, M.; D’ercole, S.; Perinetti, G.; Tripodi, D.; Catamo, G.; Serra, E.; Bruè, C.; Piccolomini, R. Clinical and microbiological effects of different restorative materials on the periodontal tissues adjacent to subgingival class V restorations. J. Clin. Periodontol. 2004, 31, 200–207. [Google Scholar] [CrossRef]
- Freitas, A.O.; Marquezan, M.; Mda, C.N.; Alviano, D.S.; Maia, L.C. The influence of orthodontic fixed appliances on the oral microbiota: A systematic review. Dental Press J. Orthod. 2014, 19, 46–55. [Google Scholar] [CrossRef] [PubMed]
- Joss-Vassalli, I.; Grebenstein, C.; Topouzelis, N.; Sculean, A.; Katsaros, C. Orthodontic therapy and gingival recession: A systematic review. Orthod. Craniofacial Res. 2010, 13, 127–141. [Google Scholar] [CrossRef] [PubMed]
- Jiang, C.F.; Wang, C.Y.; Chiang, C.P. Comparative study of protoporphyrin IX fluorescence image enhancement methods to improve an optical imaging system for oral cancer detection. J. Biomed Opt. 2011, 16, 076006. [Google Scholar] [CrossRef]
- Malik, B.H.; Jabbour, J.M.; Cheng, S.; Cuenca, R.; Cheng, Y.S.L.; Wright, J.M.; Jo, J.A.; Maitland, K.C. A novel multimodal optical imaging system for early detection of oral cancer. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2016, 121, 290–300. [Google Scholar] [CrossRef] [PubMed]
- Abdel Gawad, A.L.; El-Sharkawy, Y.H.; El-Sherif, A.F. Classification of human teeth caries using custom non-invasive optical imaging system. Lasers Dent. Sci. 2017, 1, 73–81. [Google Scholar] [CrossRef]
- Teeuw, W.J.; Coelho, L.; Silva, A.; Van Der Palen, C.J.N.M.; Lessmann, F.G.J.M.; Van der Velden, U.; Loos, B.G. Validation of a dental image analyzer tool to measure alveolar bone loss in periodontitis patients. J. Periodontal Res. 2009, 44, 94–102. [Google Scholar] [CrossRef] [PubMed]
- Moutinho, R.P.; Coelho, L.; Silva, A.; Lobo Pereira, J.A.; Pinto, M.; Baptista, I.P. Validation of a dental image-analyzer tool to measure the radiographic defect angle of the intrabony defect in periodontitis patients. J. Periodontal Res. 2012, 47, 695–700. [Google Scholar] [CrossRef] [PubMed]
- Uthoff, R.D.; Song, B.; Sunny, S.; Patrick, S.; Suresh, A.; Kolur, T.; Keerthi, G.; Spires, O.; Anbarani, A.; Wilder-Smith, P.; et al. Point-of-care, smartphone-based, dual-modality, dual-view, oral cancer screening device with neural network classification for low-resource communities. PLoS ONE 2018, 13, e0207493. [Google Scholar] [CrossRef] [PubMed]
- Sela, E.I.; Hartati, S.; Harjoko, A.; Wardoyo, R.; Munakhir, M.S. Segmentation on the dental periapical X-ray images for osteoporosis screening. Int. J. Adv. Computer Sci. Appl. 2013, 4, 147–151. [Google Scholar]
- Djuričić, G.J.; Radulovic, M.; Sopta, J.P.; Nikitović, M.; Milošević, N.T. Fractal and Gray Level Cooccurrence Matrix Computational Analysis of Primary Osteosarcoma Magnetic Resonance Images Predicts the Chemotherapy Response. Front. Oncol. 2017, 7, 246. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Liu, X.; Zhang, L. A multichannel gray level co-occurrence matrix for multi/hyperspectral image texture representation. Remote Sens. 2014, 6, 8424–8445. [Google Scholar] [CrossRef]
- Faber, T.D.; Yoon, D.C.; Service, S.K.; White, S.C. Fourier and wavelet analyses of dental radiographs detect trabecular changes in osteoporosis. Bone 2004, 35, 403–411. [Google Scholar] [CrossRef] [PubMed]
- Lin, P.L.; Huang, P.W.; Huang, P.Y.; Hsu, H.C. Alveolar bone-loss area localization in periodontitis radiographs based on threshold segmentation with a hybrid feature fused of intensity and the H-value of fractional Brownian motion model. Comput. Methods Programs Biomed 2015, 121, 117–126. [Google Scholar] [CrossRef]
- Farhadian, M.; Shokouhi, P.; Torkzaban, P. A decision support system based on support vector machine for diagnosis of periodontal disease. BMC Res. Notes 2020, 13, 337. [Google Scholar] [CrossRef]
- Chang, J.; Chang, M.F.; Angelov, N.; Hsu, C.Y.; Meng, H.W.; Sheng, S.; Ayilavarapu, S. Application of deep machine learning for the radiographic diagnosis of periodontitis. Clin. Oral Investig. 2022, 26, 6629–6637. [Google Scholar] [CrossRef]
- Lee, J.H.; Kim, D.H.; Jeong, S.N.; Choi, S.H. Detection and diagnosis of dental caries using a deep learning-based convolutional neural network algorithm. J. Dent. 2018, 77, 106–111. [Google Scholar] [CrossRef]
- Krois, J.; Ekert, T.; Meinhold, L.; Golla, T.; Kharbot, B.; Wittemeier, A.; Schwendicke, F. Deep learning for the radiographic detection of periodontal bone loss. Sci. Rep. 2019, 9, 8495. [Google Scholar] [CrossRef]
- Li, W.; Liang, Y.; Zhang, X.; Liu, C.; He, L.; Miao, L.; Sun, W. A deep learning approach to automatic gingivitis screening based on classification and localization in RGB photos. Sci. Rep. 2021, 11, 16831. [Google Scholar] [CrossRef]
- Chang, H.J.; Lee, S.J.; Yong, T.H.; Shin, N.Y.; Jang, B.G.; Kim, J.E.; Yi, W.J. Deep learning hybrid method to automatically diagnose periodontal bone loss and stage periodontitis. Sci. Rep. 2020, 10, 7531. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Chen, Y.; Sun, W.; Brown, M.; Zhang, X.; Wang, S.; Miao, L. A gingivitis identification method based on contrast-limited adaptive histogram equalization, gray-level co-occurrence matrix, and extreme learning machine. Int. J. Imaging Sys. Tech. 2019, 29, 77–82. [Google Scholar] [CrossRef]
- Li, W.; Jiang, X.; Sun, W.; Wang, S.H.; Liu, C.; Zhang, X.; Miao, L. Gingivitis identification via multichannel gray-level co-occurrence matrix and particle swarm optimization neural network. Int. J. Imaging Sys. Tech. 2020, 30, 401–411. [Google Scholar] [CrossRef]
- Rahman, S.; Rahman, M.M.; Abdullah-Al-Wadud, M.; Al-Quaderi, G.D.; Shoyaib, M. An adaptive gamma correction for image enhancement. EURASIP J. Image Video Proc. 2016, 2016, 35. [Google Scholar] [CrossRef]
- Otsu, N. A threshold selection method from gray-level histograms. IEEE Trans. Syst. Man Cybern. 1979, 9, 62–66. [Google Scholar] [CrossRef]
- Tobias, G.; Spanier, A.B. Modified gingival index (MGI) classification using dental selfies. Appl. Sci. 2020, 10, 8923. [Google Scholar] [CrossRef]
- Armitage, G.C. The complete periodontal examination. Periodontology 2000 2004, 34, 22–33. [Google Scholar] [CrossRef]
- Pihlstrom, B.L. Periodontal risk assessment, diagnosis and treatment planning. Periodontology 2000 2001, 25, 37–58. [Google Scholar] [CrossRef]
- Bergströum, J. The topography of papillary gingiva in health and early gingivitis. J. Clin. Periodontol. 1984, 11, 423–431. [Google Scholar] [CrossRef]
- Rebelo, M.A.B.; Queiroz, A.C.D. Gingival indices: State of art. In Gingival Diseases-Their Aetiology, Prevention and Treatment; Panagakos, F.S., Davies, R.M., Eds.; IntechOpen Limited: London, UK, 2011; pp. 41–54. [Google Scholar]
- Ozlu, F.C.; Aktunc, E.; Yilmaz, H.; Karadeniz, E.I. Effectiveness of three different types of educational methods on implementation of proper oral hygiene behaviour prior to orthodontic treatment. Dent. Press J. Orthod. 2021, 26, e2119248. [Google Scholar] [CrossRef]
- Bardal, P.A.P.; Olympio, K.P.K.; Bastos, J.R.D.M.; Henriques, J.F.C.; Buzalaf, M.A.R. Educação e motivação em saúde bucal: Prevenindo doenças e promovendo saúde em pacientes sob tratamento ortodôntico. Dent. Press J. Orthod. 2011, 16, 95–102. [Google Scholar] [CrossRef]
- Patil, S.; Hedad, I.A.; Jafer, A.A.; Abutaleb, G.K.; Arishi, T.M.; Arishi, S.A.; Raj, A.T. Effectiveness of mobile phone applications in improving oral hygiene care and outcomes in orthodontic patients. J. Oral Bio Craniofacial Res. 2021, 11, 26–32. [Google Scholar] [CrossRef]
- Meyle, J.; Chapple, I. Molecular aspects of the pathogenesis of periodontitis. Periodontology 2000 2015, 69, 7–17. [Google Scholar] [CrossRef] [PubMed]
- Jönsson, B.; Öhrn, K.; Oscarson, N.; Lindberg, P. The effectiveness of an individually tailored oral health educational programme on oral hygiene behaviour in patients with periodontal disease: A blinded randomized-controlled clinical trial (one-year follow-up). J. Clin. Periodontol. 2009, 36, 1025–1034. [Google Scholar] [CrossRef] [PubMed]
- Brecx, M.C.; Schlegel, K.; Gehr, P.; Lang, N.P. Comparison between histological and clinical parameters during human experimental gingivitis. J. Periodontal Res. 1987, 22, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Rousson, M.; Brox, T.; Deriche, R. Active unsupervised texture segmentation on a diffusion based feature space. In Proceedings of the 2003 IEEE Computer Society Conference on Computer Vision and Pattern Recognition, Madison, WI, USA, 18–20 June 2003. [Google Scholar]
- Riaz, F.; Rehman, S.; Ajmal, M.; Hafiz, R.; Hassan, A.; Aljohani, N.R.; Coimbra, M. Gaussian mixture model based probabilistic modeling of images for medical image segmentation. IEEE Access 2020, 8, 16846–16856. [Google Scholar] [CrossRef]
- Navalpakkam, V.; Itti, L. An integrated model of top-down and bottom-up attention for optimizing detection speed. In Proceedings of the 2006 IEEE Computer Society Conference on Computer Vision and Pattern Recognition (CVPR’06), New York, NY, USA, 17–22 June 2006. [Google Scholar]
- Liu, L.; Bian, H.; Yagi, S.I.; Yang, X. A prior-knowledge-based threshold segmentation method of forward-looking sonar images for underwater linear object detection. Jpn. J. Appl. Phys. 2016, 55, 07KG06. [Google Scholar] [CrossRef]
- Li, J.; Levine, M.D.; An, X.; Xu, X.; He, H. Visual saliency based on scale-space analysis in the frequency domain. IEEE Trans. Pattern Anal. Mach. Intell. 2012, 35, 996–1010. [Google Scholar] [CrossRef]
- Craswell, N.; Szummer, M. Random walks on the click graph. In Proceedings of the 30th Annual International ACM SIGIR Conference on Research and Development in Information Retrieval, Amsterdam, The Netherlands, 23–27 July 2007; pp. 239–246. [Google Scholar]
- Minaee, S.; Boykov, Y.; Porikli, F.; Plaza, A.; Kehtarnavaz, N.; Terzopoulos, D. Image segmentation using deep learning: A survey. IEEE Trans. Pattern Anal. Mach. Intell. 2022, 44, 3523–3542. [Google Scholar] [CrossRef] [PubMed]
- Fagundes, N.C.F.; Carvalho, A.P.C.P.S.; Vilhena, K.F.B.; Magno, M.B.; Maia, L.C.; Lima, R.R. Periodontitis as a risk factor for stroke: A systematic review and meta-analysis. Vasc. Health Risk Manag. 2019, 15, 519. [Google Scholar] [CrossRef] [PubMed]
- Song, T.J.; Kim, J.W.; Kim, J. Oral health and changes in lipid profile: A nationwide cohort study. J. Clin. Periodontol. 2020, 47, 1437–1445. [Google Scholar] [CrossRef] [PubMed]
- Song, T.J.; Jeon, J.; Kim, J. Cardiovascular risks of periodontitis and oral hygiene indicators in patients with diabetes mellitus. Diab. Metabol. 2021, 47, 101252. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Score | Diagnosis | Modified Gingival Index Criteria | Color | Texture | Volume | Extent |
|---|---|---|---|---|---|---|
| 0 | Healthy | Absence of inflammation | Normal | Normal | Normal | None |
| 1 | Mild inflammation (partial unit) | Slight change in color, a little change in the texture of any portion of, but not the entire, marginal or papillary gingival unit | Slightly more reddish or bluish-reddish | Slightly glazy | Slight edema of the margin | Part of the gingival unit |
| 2 | Mild inflammation (entire unit) | Criteria as above but involving the entire marginal or papillary gingival unit | Slightly more reddish or bluish-reddish | Slightly glazy | Slight edema of the margin | Entire gingival unit |
| 3 | Moderate inflammation | Glazing, redness, edema, and/or hypertrophy of the marginal or papillary gingival unit | Red or reddish-blue | Glazy | Edema and /or hypertrophy of the margin | Entire gingival unit |
| 4 | Severe inflammation | Marked redness, edema, and/or hypertrophy of the marginal or papillary gingival unit, spontaneous bleeding congestion, or ulceration | Markedly red or reddish-blue | Spontaneous bleeding or ulceration | Edema and/or hypertrophy of the entire unit | Entire gingival unit |
| Characteristics | Items | N (%) |
|---|---|---|
| Sex | Male | 11 (44.0) |
| Female | 14 (56.0) | |
| Age | 20s | 19 (75.7) |
| 30s | 6 (24.3) | |
| Average period of orthodontic treatment (Unit: Month, mean ± SD) | 22.1 ± 13.0 | |
| Orthodontic devices | Metal bracket | 9 (36.0) |
| Ceramic bracket | 16 (64.0) | |
| Orthodontic Treatment | Tooth Region | Tooth Region | ||||
|---|---|---|---|---|---|---|
| #12-#13 | #11-#21 | #22-#23 | #43-#43 | #41-#31 | #32-#33 | |
| BO | 0.80 ± 0.71 | 0.57 ± 0.65 | 0.50 ± 0.76 | 0.57 ± 0.85 | 0.64 ± 1.01 | 0.54 ± 0.97 |
| MO | 0.82 ± 0.85 | 0.71 ± 0.91 | 0.64 ± 0.80 | 0.93 ± 0.83 | 1.00 ± 0.88 | 0.92 ± 0.86 |
| TO | 1.50 ± 1.09 | 1.50 ± 0.85 | 1.57 ± 0.94 | 1.79 ± 1.12 | 1.71 ± 0.91 | 1.92 ± 1.12 |
| IDO | 1.64 ± 0.86 | 1.79 ± 1.05 | 1.64 ± 0.77 | 1.86 ± 0.86 | 2.07 ± 0.92 | 1.85 ± 0.99 |
| p-value * | 0.002 | 0.001 | 0.001 | <0.001 | 0.001 | 0.001 |
| Orthodontic Treatment | Tooth Region | Tooth Region | ||||
|---|---|---|---|---|---|---|
| #12-#13 | #11-#21 | #22-#23 | #43-#43 | #41-#31 | #32-#33 | |
| BO | 1.76 ± 0.26 | 1.58 ± 0.15 | 1.83 ± 0.23 | 1.59 ± 0.16 | 1.54 ± 0.12 | 1.58 ± 0.17 |
| MO | 1.59 ± 0.20 | 1.48 ± 0.15 | 1.66 ± 0.20 | 1.51 ± 0.15 | 1.48 ± 0.13 | 1.51 ± 0.15 |
| TO | 1.71 ± 0.21 | 1.57 ± 0.13 | 1.79 ± 0.18 | 1.59 ± 0.13 | 1.59 ± 0.11 | 1.63 ± 0.15 |
| IDO | 1.81 ± 0.29 | 1.66 ± 0.20 | 1.88 ± 0.22 | 1.71 ± 0.16 | 1.67 ± 0.14 | 1.72 ± 0.17 |
| p-value * | <0.001 | <0.001 | 0.001 | <0.001 | <0.001 | <0.001 |
| Location | Orthodontic Treatment | Maxilla | Mandible | ||||||
|---|---|---|---|---|---|---|---|---|---|
| R/G_BO | R/G_MO | R/G_ TO | R/G_ IDO | R/G_BO | R/G_MO | R/G_ TO | R/G_ IDO | ||
| Maxilla | GI_BO | 0.43 | |||||||
| GI_MO | 0.63 * | ||||||||
| GI_TO | 0.70 ** | ||||||||
| GI_IDO | 0.87 ** | ||||||||
| Mandible | GI_BO | 0.41 | |||||||
| GI_MO | 0.40 | ||||||||
| GI_TO | 0.60 * | ||||||||
| GI_IDO | 0.73 ** | ||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, H.-N.; Kim, K.; Lee, Y. Intra-Oral Photograph Analysis for Gingivitis Screening in Orthodontic Patients. Int. J. Environ. Res. Public Health 2023, 20, 3705. https://doi.org/10.3390/ijerph20043705
Kim H-N, Kim K, Lee Y. Intra-Oral Photograph Analysis for Gingivitis Screening in Orthodontic Patients. International Journal of Environmental Research and Public Health. 2023; 20(4):3705. https://doi.org/10.3390/ijerph20043705
Chicago/Turabian StyleKim, Han-Na, Kyuseok Kim, and Youngjin Lee. 2023. "Intra-Oral Photograph Analysis for Gingivitis Screening in Orthodontic Patients" International Journal of Environmental Research and Public Health 20, no. 4: 3705. https://doi.org/10.3390/ijerph20043705
APA StyleKim, H.-N., Kim, K., & Lee, Y. (2023). Intra-Oral Photograph Analysis for Gingivitis Screening in Orthodontic Patients. International Journal of Environmental Research and Public Health, 20(4), 3705. https://doi.org/10.3390/ijerph20043705