
Perception of Remote Learning by Fixed Prosthodontic Students at a Romanian Faculty of Dentistry

 , , , ,
, , , , 
Abstract
1. Introduction
2. Materials and Methods
2.1. New Teaching Methods
2.2. Sample and Questionnaire
2.3. Statistical Study
3. Results
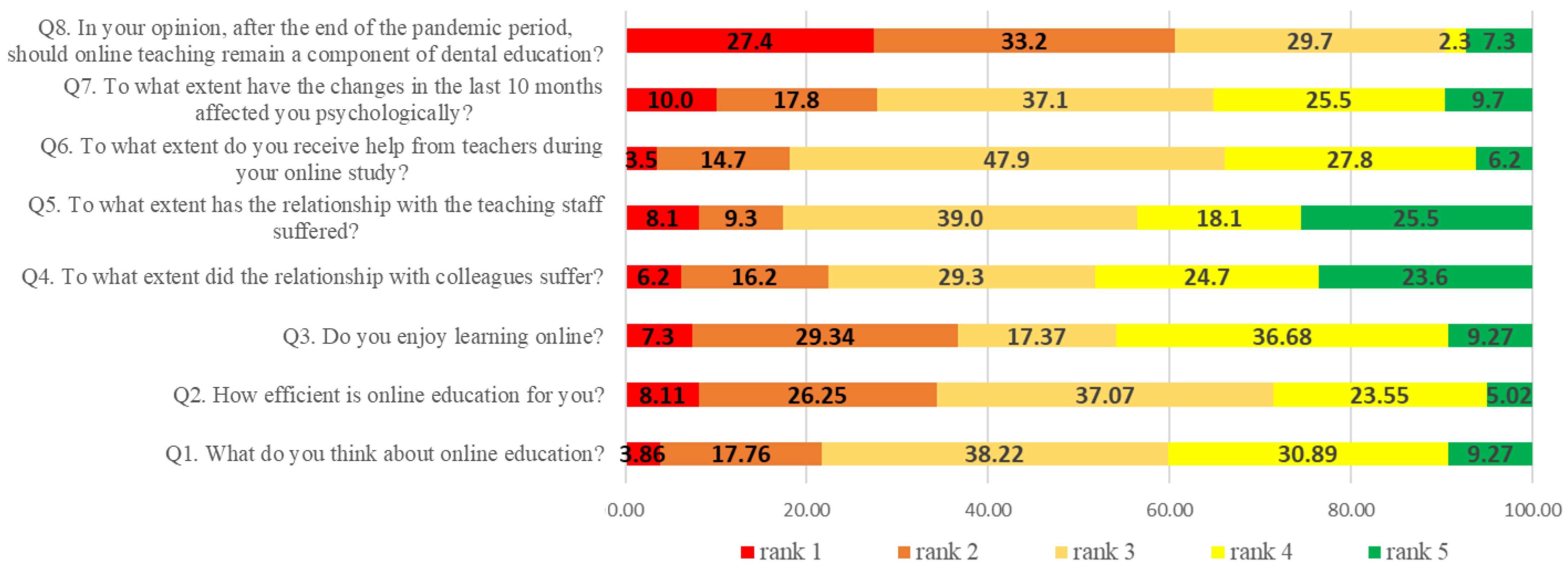
3.1. Student Perception and Feedback on Remote Learning and Its Impact
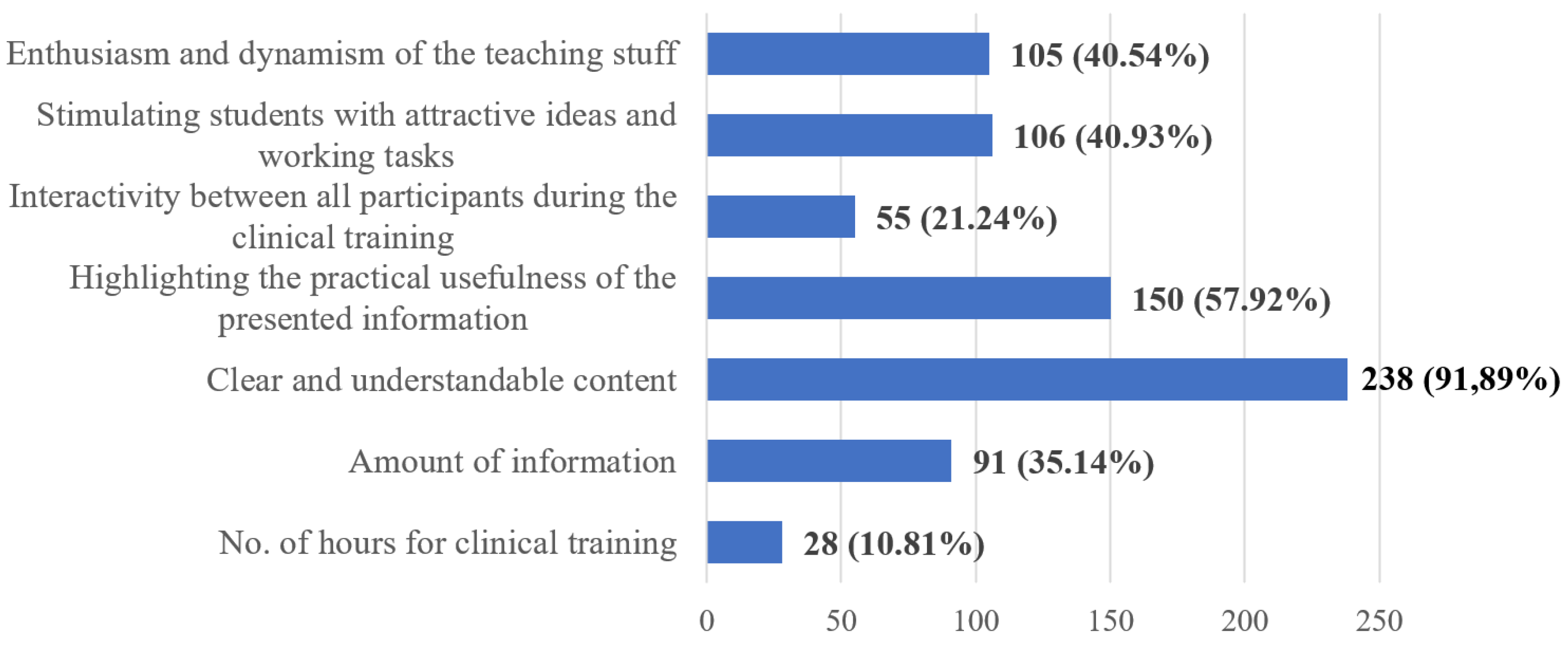
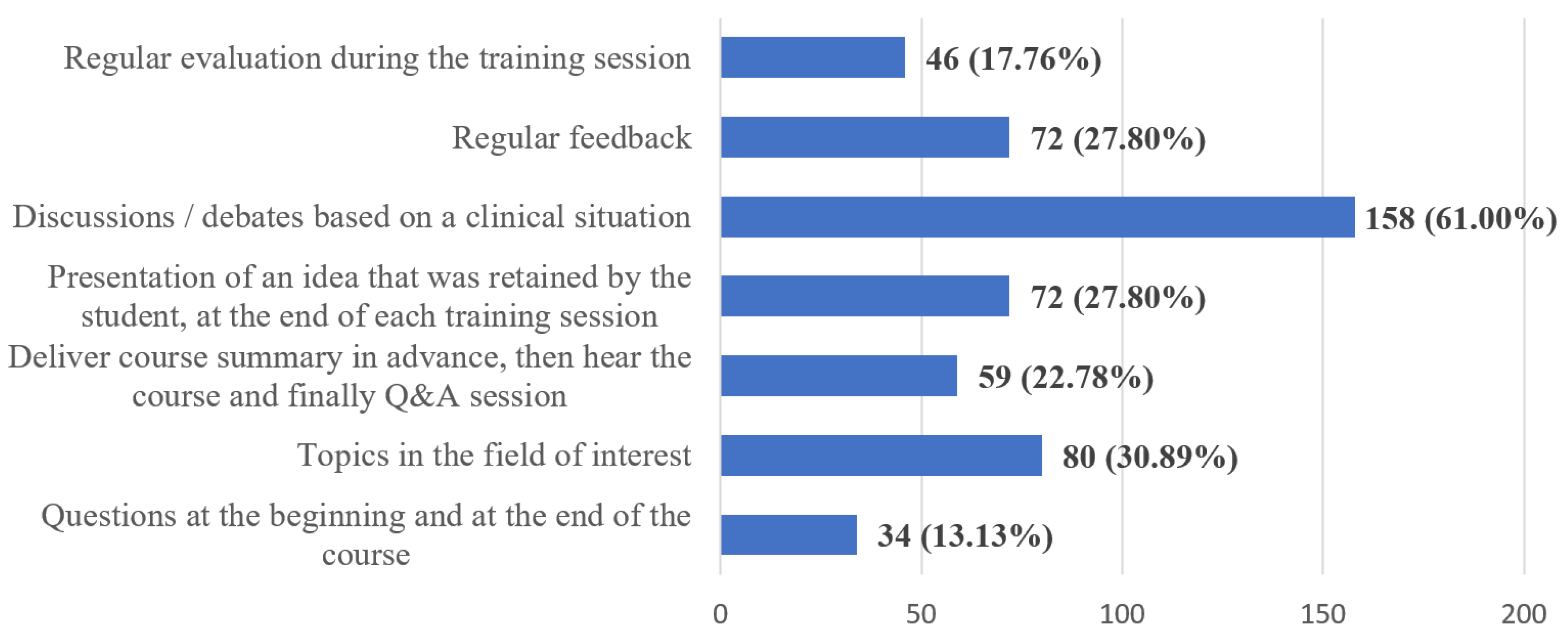
3.2. Student Perception and Feedback on Remote Teaching, Learning and Assessment at the Fixed Prosthodontics Disciplines for Both Theoretical Knowledge and Practical Skills
3.3. Open-Ended Questions–Students’ Suggestions and Opinions on Didactic Activity at the Fixed Prosthodontics Disciplines
4. Discussion
- a.
- flexibility—being disconnected from the creation and transmission of the training material, the trainee can access it at any time, any place and using the preferred device. After downloading the material, some or all of the content can be played at the student’s discretion, so as to facilitate the learning process.
- b.
- engagement—the content is more engaging than the mere reading of a textbook, further supporting the learning process.
- c.
- wide accessibility—the content can be accessed anywhere in the world, thus reaching a much wider audience compared with on-site delivered lectures.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. WHO Director-General’s Statement on IHR Emergency Committee on Novel Coronavirus (2019-nCoV). Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-statement-on-ihr-emergency-committee-on-novel-coronavirus-(2019-ncov) (accessed on 19 June 2022).
- WHO. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19. 11 March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 19 June 2022).
- WHO. Coronavirus Disease (COVID-19) Pandemic. Available online: https://www.euro.who.int/en/health-topics/health-emergencies/coronavirus-covid-19/novel-coronavirus-2019-ncov (accessed on 19 June 2022).
- WHO. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19. 13 March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-mission-briefing-on-covid-19---13-march-2020 (accessed on 19 June 2022).
- Painter, M.; Qiu, T. Political Beliefs affect Compliance with Government Mandates. J. Econ. Behav. Organ. Forthcom. 2021, 185, 688–701. [Google Scholar] [CrossRef]
- Cao, W.J.; Fang, Z.W.; Hou, G.Q.; Han, M.; Xu, X.R.; Dong, J.X.; Zheng, J.Z. The psychological impact of the COVID-19 epidemic on college students in China. Psychiatry Res. 2020, 287, 5. [Google Scholar] [CrossRef]
- Wang, C.; Cheng, Z.; Yue, X.-G.; McAleer, M. Risk Management of COVID-19 by Universities in China. J. Risk Financ. Manag. 2020, 13, 36. [Google Scholar] [CrossRef]
- Gaudin, A.; Arbab-Chirani, R.; Pérez, F. Effect of COVID-19 on Dental Education and Practice in France. Front. Dent. Med. 2020, 1, 5. [Google Scholar] [CrossRef]
- Hodges, C.; Moore, S.; Lockee, B.; Trust, T.; Bond, A. The difference between emergency remote teaching and online learning. Educ. Rev. 2020. Available online: https://er.educause.edu/articles/2020/3/the-difference-between-emergency-remote-teaching-and-online-learning (accessed on 19 June 2022).
- Witze, A. Universities will never be the same after the coronavirus crisis. Nature 2020, 582, 162–164. [Google Scholar] [CrossRef]
- Butnaru, G.I.; Niță, V.; Anichiti, A.; Brînză, G. The Effectiveness of Online Education during COVID-19 Pandemic—A Comparative Analysis between the Perceptions of Academic Students and High School Students from Romania. Sustainability 2021, 13, 5311. [Google Scholar] [CrossRef]
- Kim, E.-J.; Kim, J.J.; Han, S.-H. Understanding Student Acceptance of Online Learning Systems in Higher Education: Application of Social Psychology Theories with Consideration of User Innovativeness. Sustainability 2021, 13, 896. [Google Scholar] [CrossRef]
- Viner, R.M.; Russell, S.J.; Croker, H.; Packer, J.; Ward, J.; Stansfield, C.; Mytton, O.; Bonell, C.; Booy, R. School closure and management practices during coronavirus outbreaks including COVID-19: A rapid systematic review. Lancet Child Adolesc. Health 2020, 4, 397–404. [Google Scholar] [CrossRef]
- Deogade, S.C.; Naitam, D. COVID-19 and dental aerosols: The infection connection. Avicenna J. Med. 2021, 11, 107–109. [Google Scholar] [CrossRef]
- Epstein, J.B.; Chow, K.; Mathias, R. Dental procedure aerosols and COVID-19. Lancet Infect. Dis. 2021, 21, e73. [Google Scholar] [CrossRef]
- Gambarini, G.; Galli, M.; Gambarini, E.; Di Nardo, D.; Seracchiani, M.; Obino, F.V.; Patil, S.; Bhandi, S.; Miccoli, G.; Testarelli, L. Fine Aerosols and Perceived Risk of COVID-19 among Italian Dental Practitioners: An Experimental Survey. J. Contemp. Dent. Pract. 2020, 21, 599–603. [Google Scholar] [CrossRef]
- Harrel, S.K. Airborne spread of disease—The implications for dentistry. J. Calif. Dent. Assoc. 2004, 32, 901–906. [Google Scholar]
- Harrel, S.K.; Molinari, J. Aerosols and splatter in dentistry: A brief review of the literature and infection control implications. J. Am. Dent. Assoc. 2004, 135, 429–437. [Google Scholar] [CrossRef]
- Forna, N.C. COVID-19 challenges in dental health care and dental schools. Rom. J. Oral Rehab. 2020, 12, 6–12. [Google Scholar]
- CDC, U.; Guidance for Dental Settings. Interim Infection Prevention and Control Guidance for Dental Settings during the COVID-19 Response. Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/dental-settings.html (accessed on 20 July 2021).
- Farooq, I.; Ali, S. COVID-19 outbreak and its monetary implications for dental practices, hospitals and healthcare workers. Postgrad Med. J. 2020, 96, 791–792. [Google Scholar] [CrossRef]
- Ali, S.; Farooq, I.; Abdelsalam, M.; AlHumaid, J. Current Clinical Dental Practice Guidelines and the Financial Impact of COVID-19 on Dental Care Providers. Eur. J. Dent. 2020, 14, S140–S145. [Google Scholar] [CrossRef]
- Machado, R.A.; Bonan, P.R.F.; Perez, D.; Martelli JÚnior, H. COVID-19 pandemic and the impact on dental education: Discussing current and future perspectives. Braz. Oral Res. 2020, 34, e083. [Google Scholar] [CrossRef]
- Chavarría-Bolaños, D.; Gómez-Fernández, A.; Dittel-Jiménez, C.; Montero-Aguilar, M. E-Learning in Dental Schools in the Times of COVID-19: A Review and Analysis of an Educational Resource in Times of the COVID-19 Pandemic. Odovtos Int. J. Dent. Sci. 2020, 22, 69–86. [Google Scholar] [CrossRef]
- Singh, H.K.; Joshi, A.; Malepati, R.N.; Najeeb, S.; Balakrishna, P.; Pannerselvam, N.K.; Singh, Y.K.; Ganne, P. A survey of E-learning methods in nursing and medical education during COVID-19 pandemic in India. Nurse Educ. Today 2021, 99, 104796. [Google Scholar] [CrossRef]
- Parmelee, D.; Michaelsen, L.K.; Cook, S.; Hudes, P.D. Team-based learning: A practical guide: AMEE guide no. 65. Med. Teach. 2012, 34, e275–e287. [Google Scholar] [CrossRef]
- Wang, H.; Xuan, J.; Liu, L.; Shen, X.; Xiong, Y. Problem-based learning and case-based learning in dental education. Ann. Transl. Med. 2021, 9, 1137. [Google Scholar] [CrossRef]
- Jiang, Z.; Zhu, D.; Li, J.; Ren, L.; Pu, R.; Yang, G. Online dental teaching practices during the COVID-19 pandemic: A cross-sectional online survey from China. BMC Oral Health 2021, 21, 189. [Google Scholar] [CrossRef]
- Lewin, K.M. Contingent reflections on coronavirus and priorities for educational planning and development. Prospects 2020, 49, 17–24. [Google Scholar] [CrossRef]
- UMF_Iasi. Available online: https://www.umfiasi.ro/en/academic/facultati/Dental-medicine/Pages/Educational-plans.aspx (accessed on 10 January 2022).
- Starr, T.N.; Greaney, A.J.; Addetia, A.; Hannon, W.W.; Choudhary, M.C.; Dingens, A.S.; Li, J.Z.; Bloom, J.D. Prospective mapping of viral mutations that escape antibodies used to treat COVID-19. Science 2021, 371, 850–854. [Google Scholar] [CrossRef]
- France, K.; Hangorsky, U.; Wu, C.W.; Sollecito, T.P.; Stoopler, E.T. Participation in an existing massive open online course in dentistry during the COVID-19 pandemic. J. Dent. Educ. 2021, 85, 78–81. [Google Scholar] [CrossRef]
- Iyer, P.; Aziz, K.; Ojcius, D.M. Impact of COVID-19 on dental education in the United States. J. Dent. Educ. 2020, 84, 718–722. [Google Scholar] [CrossRef]
- Schlenz, M.A.; Schmidt, A.; Wöstmann, B.; Krämer, N.; Schulz-Weidner, N. Students’ and lecturers’ perspective on the implementation of online learning in dental education due to SARS-CoV-2 (COVID-19): A cross-sectional study. BMC Med. Educ. 2020, 20, 354. [Google Scholar] [CrossRef]
- Hattar, S.; AlHadidi, A.; Sawair, F.A.; Alraheam, I.A.; El-Ma’aita, A.; Wahab, F.K. Impact of COVID-19 pandemic on dental education: Online experience and practice expectations among dental students at the University of Jordan. BMC Med. Educ. 2021, 21, 151. [Google Scholar] [CrossRef]
- Varvara, G.; Bernardi, S.; Bianchi, S.; Sinjari, B.; Piattelli, M. Dental Education Challenges during the COVID-19 Pandemic Period in Italy: Undergraduate Student Feedback, Future Perspectives, and the Needs of Teaching Strategies for Professional Development. Healthcare 2021, 9, 454. [Google Scholar] [CrossRef]
- Iurcov, R.; Pop, L.M.; Iorga, M. Impact of COVID-19 Pandemic on Academic Activity and Health Status among Romanian Medical Dentistry Students; A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 6041. [Google Scholar] [CrossRef]
- Goriuc, A.; Sandu, D.; Tatarciuc, M.; Luchian, I. The Impact of the COVID-19 Pandemic on Dentistry and Dental Education: A Narrative Review. Int. J. Environ. Res. Public Health 2022, 19, 2537. [Google Scholar] [CrossRef]
- UMF_Iasi. Serii si Grupe—2020–2021. Available online: https://www.umfiasi.ro/ro/academic/programe-de-studii/licenta/Pagini/Student---Medicin%C4%83-dentar%C4%83.aspx (accessed on 15 February 2022).
- SurveyMonkey. Available online: https://www.surveymonkey.co.uk/mp/margin-of-error-calculator/ (accessed on 28 August 2022).
- Deery, C. The COVID-19 pandemic: Implications for dental education. Evid.-Based Dent. 2020, 21, 46–47. [Google Scholar] [CrossRef]
- Fazio, M.; Lombardo, C.; Marino, G.; Marya, A.; Messina, P.; Scardina, G.A.; Tocco, A.; Torregrossa, F.; Valenti, C. LinguAPP: An m-Health Application for Teledentistry Diagnostics. Int. J. Environ. Res. Public Health 2022, 19, 822. [Google Scholar] [CrossRef]
- Elangovan, S.; Mahrous, A.; Marchini, L. Disruptions during a pandemic: Gaps identified and lessons learned. J. Dent. Educ. 2020, 84, 1270–1274. [Google Scholar] [CrossRef]
- Clemente, M.P.; Moreira, A.; Pinto, J.C.; Amarante, J.M.; Mendes, J. The Challenge of Dental Education After COVID-19 Pandemic—Present and Future Innovation Study Design. Inquiry 2021, 58, 469580211018293. [Google Scholar] [CrossRef]
- Goh, P.; Sandars, J. A vision of the use of technology in medical education after the COVID-19 pandemic [version 1]. MedEdPublish 2020, 9, 49. [Google Scholar] [CrossRef]
- Wu, D.T.; Wu, K.Y.; Nguyen, T.T.; Tran, S.D. The impact of COVID-19 on dental education in North America-Where do we go next? Eur. J. Dent. Educ. 2020, 24, 825–827. [Google Scholar] [CrossRef]
- Coughlan, J.; Timuş, D.; Crnic, T.; Srdoč, D.; Halton, C.; Dragan, I.F. Impact of COVID-19 on dental education in Europe: The students’ perspective. Eur. J. Dent. Educ. 2022, 26, 599–607. [Google Scholar] [CrossRef]
- Quinn, B.; Field, J.; Gorter, R.; Akota, I.; Manzanares, M.C.; Paganelli, C.; Davies, J.; Dixon, J.; Gabor, G.; Amaral Mendes, R.; et al. COVID-19: The immediate response of european academic dental institutions and future implications for dental education. Eur. J. Dent. Educ. 2020, 24, 811–814. [Google Scholar] [CrossRef]
- Hakami, Z.; Khanagar, S.B.; Vishwanathaiah, S.; Hakami, A.; Bokhari, A.M.; Jabali, A.H.; Alasmari, D.; Aldrees, A.M. Psychological impact of the coronavirus disease 2019 (COVID-19) pandemic on dental students: A nationwide study. J. Dent. Educ. 2021, 85, 494–503. [Google Scholar] [CrossRef]
- Saeed, S.G.; Bain, J.; Khoo, E.; Siqueira, W.L. COVID-19: Finding silver linings for dental education. J. Dent. Educ. 2020, 84, 1060–1063. [Google Scholar] [CrossRef] [PubMed]
- UMF_Iasi. Available online: https://www.umfiasi.ro/ro/Pagini/Suport-psihologic-pentru-comunitatea-UMF-Iasi.aspx (accessed on 28 November 2022).
- Bennardo, F.; Buffone, C.; Fortunato, L.; Giudice, A. COVID-19 is a challenge for dental education—A commentary. Eur. J. Dent. Educ. 2020, 24, 822–824. [Google Scholar] [CrossRef]
- Li, B.; Cheng, L.; Wang, H. Challenges and Opportunities for Dental Education from COVID-19. Dent. J. 2022, 10, 188. [Google Scholar] [CrossRef]
- Park, J.C.; Kwon, H.E.; Chung, C.W. Innovative digital tools for new trends in teaching and assessment methods in medical and dental education. J. Educ. Eval. Health Prof. 2021, 18, 13. [Google Scholar] [CrossRef]
- Sharab, L.; Adel, M.; Abualsoud, R.; Hall, B.; Albaree, S.; de Leeuw, R.; Kutkut, A. Perception, awareness, and attitude toward digital dentistry among pre-dental students: An observational survey. Bull. Natl. Res. Cent. 2022, 46, 246. [Google Scholar] [CrossRef]
- Meng, L.; Hua, F.; Bian, Z. Coronavirus Disease 2019 (COVID-19): Emerging and Future Challenges for Dental and Oral Medicine. J. Dent. Res. 2020, 99, 481–487. [Google Scholar] [CrossRef] [PubMed]
- Alharbi, F.; Alwadei, S.H.; Alwadei, A.; Asiri, S.; Alwadei, F.; Alqerban, A.; Almuzian, M. Comparison between two asynchronous teaching methods in an undergraduate dental course: A pilot study. BMC Med. Educ. 2022, 22, 488. [Google Scholar] [CrossRef]
- Kunin, M.; Julliard, K.N.; Rodriguez, T.E. Comparing face-to-face, synchronous, and asynchronous learning: Postgraduate dental resident preferences. J. Dent. Educ. 2014, 78, 856–866. [Google Scholar] [CrossRef] [PubMed]
- Kalludi, S.; Punja, D.; Rao, R.; Dhar, M. Is Video Podcast Supplementation as a Learning Aid Beneficial to Dental Students? J. Clin. Diagn. Res. 2015, 9, Cc04–Cc07. [Google Scholar] [CrossRef] [PubMed]
- Prakash, S.S.; Muthuraman, N.; Anand, R. Short-duration podcasts as a supplementary learning tool: Perceptions of medical students and impact on assessment performance. BMC Med. Educ. 2017, 17, 167. [Google Scholar] [CrossRef]
- Zhang, E.; Trad, N.; Corty, R.; Zohrob, D.; Trivedi, S.; Rodman, A. How podcasts teach: A comprehensive analysis of the didactic methods of the top hundred medical podcasts. Med. Teach. 2022, 44, 1146–1150. [Google Scholar] [CrossRef] [PubMed]
- Huang, T.-K.; Yang, C.-H.; Hsieh, Y.-H.; Wang, J.-C.; Hung, C.-C. Augmented reality (AR) and virtual reality (VR) applied in dentistry. Kaohsiung J. Med. Sci. 2018, 34, 243–248. [Google Scholar] [CrossRef] [PubMed]
- Chaturvedi, S.; Elmahdi, A.E.; Abdelmonem, A.M.; Haralur, S.B.; Alqahtani, N.M.; Suleman, G.; Sharif, R.A.; Gurumurthy, V.; Alfarsi, M.A. Predoctoral dental implant education techniques—Students’ perception and attitude. J. Dent. Educ. 2021, 85, 392–400. [Google Scholar] [CrossRef]
- Bentata, Y. The COVID-19 pandemic and international federation of medical students’ association exchanges: Thousands of students deprived of their clinical and research exchanges. Med. Educ. Online 2020, 25, 1783784. [Google Scholar] [CrossRef]
- Abouzeid, H.; Chaturvedi, S.; Abdelaziz, K.M.; Alzahrani, F.; AlQarni, A.; Alqahtani, N. Role of Robotics and Artificial Intelligence in Oral Health and Preventive Dentistry—Knowledge, Perception and Attitude of Dentists. Oral Health Prev. Dent. 2021, 19, 353–363. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Questions | Answers Rank | ||||
|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | |
| Q1. What do you think about online education? | very bad | bad | neutral | good | very good |
| Q2. How efficient is online education for you? | not at all | a little bit | medium | a lot | very much |
| Q3. Do you enjoy learning online? | not at all | not really | neutral | yes, but with some changes | yes, definitely |
| Q4. To what extent did the relationship with colleagues suffer? | very much | a lot | moderate | a little bit | not at all |
| Q5. To what extent has the relationship with the teaching staff suffered? | very much | a lot | moderate | a little bit | not at all |
| Q6. To what extent do you receive help from teachers during your online study? | very much | a lot | moderate | a little bit | not at all |
| Q7. To what extent have the changes in the last 10 months affected you psychologically? | very much | a lot | moderate | a little bit | not at all |
| Q8. In your opinion, after the end of the pandemic period, should online teaching remain a component of dental education? | no | to littleextent | moderate extent | to a largeextent | yes |
| Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | ||
|---|---|---|---|---|---|---|---|---|---|
| Q1 | χ2 | - | |||||||
| ρ | 1 | ||||||||
| 1-β | - | ||||||||
| Q2 | χ2 | 285.979 | - | ||||||
| ρ | 0.786 ** | 1 | |||||||
| 1-β | 1 | - | |||||||
| Q3 | χ2 | 230.655 | 210.226 | - | |||||
| ρ | 0.635 ** | 0.708 ** | 1 | ||||||
| 1-β | 1 | 1 | - | ||||||
| Q4 | χ2 | 44.846 | 40.859 | 33.992 | - | ||||
| ρ | 0.234 ** | 0.306 ** | 0.229 ** | 1 | |||||
| 1-β | 0.883 | 0.991 | 0.866 | - | |||||
| Q5 | χ2 | 69.652 | 118.120 | 69.142 | 192.041 | - | |||
| ρ | 0.418 ** | 0.490 ** | 0.359 ** | 0.586 ** | 1 | ||||
| 1-β | 1 | 1 | 0.999 | 1 | - | ||||
| Q6 | χ2 | 53.662 | 63.246 | 33.946 | 29.172 | 39.950 | - | ||
| ρ | 0.386 ** | 0.375 ** | 0.236 ** | 0.189 ** | 0.288 ** | 1 | |||
| 1-β | 1 | 1 | 0.889 | 0.677 | 0.981 | - | |||
| Q7 | χ2 | 51.571 | 72.787 | 50.956 | 57.135 | 57.083 | 48.482 | - | |
| ρ | 0.334 ** | 0.421 ** | 0.330 ** | 0.332 ** | 0.358 ** | 0.318 ** | 1 | ||
| 1-β | 0.998 | 1 | 0.997 | 0.997 | 0.999 | 0.995 | - | ||
| Q8 | χ2 | 99.090 | 97.099 | 113.490 | 18.962 | 40.878 | 18.202 | 38.243 | - |
| ρ | 0.493 ** | 0.536 ** | 0.590 ** | 0.168 ** | 0.282 ** | 0.063 | 0.230 ** | 1 | |
| 1-β | 1 | 1 | 1 | 0.547 | 0.976 | 0.059 | 0.869 | - |
| Q13-Do You Consider That the Teaching of Theoretical Notions Should Be Done: | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Answer Options | Hybrid | Online | Onsite | χ2 | df | ϕc | p | Total | |||
| N | N | N | N | % | |||||||
| Q14 | Increasing the amount of asynchronous content | 34 | 50 | 19 | 7, 873 | 2 | 0.17 | <0.020 | 103 | 39.77 | |
| Increasing the amount of synchronous content | 65 | 49 | 42 | 156 | 60.23 | ||||||
| Total | N | 99 | 99 | 61 | 259 | ||||||
| % | 38.22 | 38.22 | 23.55 | 100.00 | |||||||
| Q14 = Do you think that the following should be considered when teaching theoretical notions online | |||||||||||
| Strengths | Limitations | Concerns | Suggestions |
|---|---|---|---|
| Unlike previous years, we managed to attend all the courses. More time to spend in a familiar, safe environment. Reduced costs for transportation and accommodation for students from outside the university center. Increased usage of digital teaching content during the classes. Availability of online teaching materials to be watched at any time. | Lack of practical skills. Dentistry is not a theoretical domain; hands-on practical training is mandatory. We were struggling to keep our concentration and motivation at a high level. Lack of interactivity with the peers and teaching staff. Not all the disciplines allow the courses to be recorded and do not offer online materials. Lack of separation between the work environment and home environment. Distraction by family-related issues in the home environment. Internet connectivity issues. | Because of the lack of practical activity, the information will be superficially assimilated, without a deep understanding. Lack of experience of patient interaction and treatment, with concerns about the future profession. Lack of social interaction and the alteration of the student–professor relationship. Stress and uncertainty related to the new online examination method, irrelevant and altered quality of online examination. Losing the privacy of one’s own home because of the need to turn on the camera and bringing the stress related to the faculty activities to the private environment at home. | In person attendance at the clinical training. The level of interactivity during the online classes should be increased. On-site examination. At least those who had COVID should attend on-site classes. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tanculescu, O.; Apostu, A.-M.; Doloca, A.; Solomon, S.M.; Diaconu-Popa, D.; Ciongradi, C.I.; Vieriu, R.-M.; Aungurencei, O.; Fatu, A.-M.; Ioanid, N.; et al. Perception of Remote Learning by Fixed Prosthodontic Students at a Romanian Faculty of Dentistry. Int. J. Environ. Res. Public Health 2023, 20, 3622. https://doi.org/10.3390/ijerph20043622
Tanculescu O, Apostu A-M, Doloca A, Solomon SM, Diaconu-Popa D, Ciongradi CI, Vieriu R-M, Aungurencei O, Fatu A-M, Ioanid N, et al. Perception of Remote Learning by Fixed Prosthodontic Students at a Romanian Faculty of Dentistry. International Journal of Environmental Research and Public Health. 2023; 20(4):3622. https://doi.org/10.3390/ijerph20043622
Chicago/Turabian StyleTanculescu, Oana, Alina-Mihaela Apostu, Adrian Doloca, Sorina Mihaela Solomon, Diana Diaconu-Popa, Carmen Iulia Ciongradi, Raluca-Maria Vieriu, Ovidiu Aungurencei, Ana-Maria Fatu, Nicoleta Ioanid, and et al. 2023. "Perception of Remote Learning by Fixed Prosthodontic Students at a Romanian Faculty of Dentistry" International Journal of Environmental Research and Public Health 20, no. 4: 3622. https://doi.org/10.3390/ijerph20043622
APA StyleTanculescu, O., Apostu, A.-M., Doloca, A., Solomon, S. M., Diaconu-Popa, D., Ciongradi, C. I., Vieriu, R.-M., Aungurencei, O., Fatu, A.-M., Ioanid, N., Scurtu, M., & Saveanu, C. I. (2023). Perception of Remote Learning by Fixed Prosthodontic Students at a Romanian Faculty of Dentistry. International Journal of Environmental Research and Public Health, 20(4), 3622. https://doi.org/10.3390/ijerph20043622