
Co-Occurring Conduct Problems and Anxiety: Implications for the Functioning and Treatment of Youth with Oppositional Defiant Disorder
 ,
,
Abstract
1. Introduction
2. Method
2.1. Participants
2.2. Measures
2.2.1. Latent Profile Classification Measures
Parental and Teacher Ratings
Self-Ratings
2.2.2. External Validator Measures
Clinician Ratings
Parental Ratings
Teacher Ratings
Self-Ratings
3. Treatment
4. Statistical Analysis
5. Results
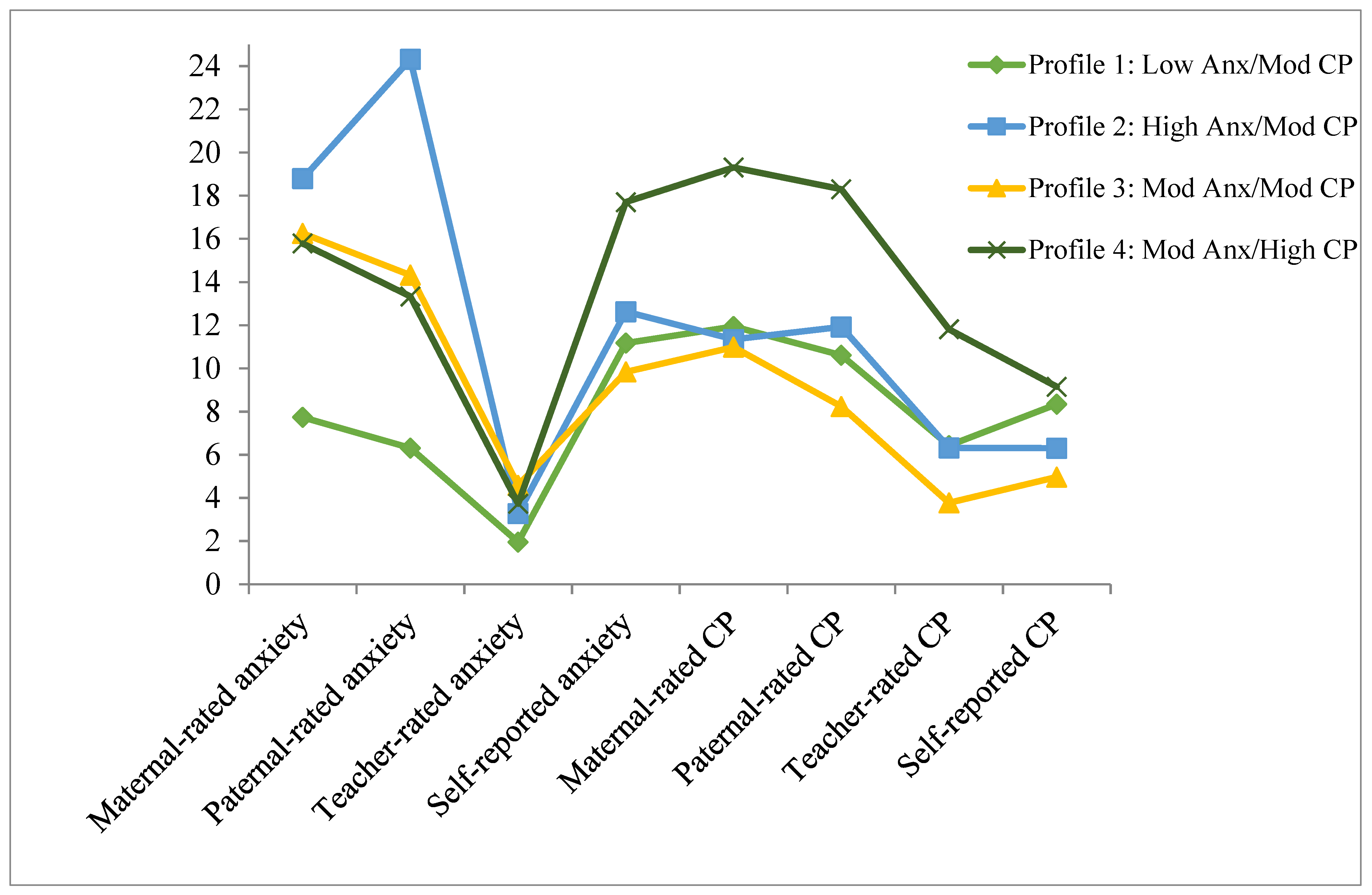
5.1. Latent Profile Classification
5.2. Global Functioning and Treatment Outcomes
5.2.1. Clinician Ratings
5.2.2. Parental Ratings
5.2.3. Teacher Ratings
5.2.4. Self-Ratings
6. Discussion
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Burke, J.D.; Rowe, R.; Boylan, K. Functional Outcomes of Child and Adolescent Oppositional Defiant Disorder Symptoms in Young Adult Men. J. Child Psychol. Psychiatry 2014, 55, 264–272. [Google Scholar] [CrossRef] [PubMed]
- Nock, M.K.; Kazdin, A.E.; Hiripi, E.; Kessler, R.C. Lifetime Prevalence, Correlates, and Persistence of Oppositional Defiant Disorder: Results from the National Comorbidity Survey Replication. J. Child Psychol. Psychiatry 2007, 48, 703–713. [Google Scholar] [CrossRef] [PubMed]
- Kaminski, J.W.; Claussen, A.H. Evidence Base Update for Psychosocial Treatments for Disruptive Behaviors in Children. J. Clin. Child Adolesc. Psychol. 2017, 46, 477–499. [Google Scholar] [CrossRef] [PubMed]
- Hawes, D.J.; Price, M.J.; Dadds, M.R. Callous-Unemotional Traits and the Treatment of Conduct Problems in Childhood and Adolescence: A Comprehensive Review. Clin. Child Fam. Psychol. Rev. 2014, 17, 248–267. [Google Scholar] [CrossRef]
- Foster, E.M.; Jones, D.E.; Conduct Problems Prevention Research Group. The High Costs of Aggression: Public Expenditures Resulting from Conduct Disorder. Am. J. Public Health 2005, 95, 1767–1772. [Google Scholar] [CrossRef]
- Roetman, P.J.; Siebelink, B.M.; Vermeiren, R.R.; Colins, O.F. Classes of Oppositional Defiant Disorder Behavior in Clinic-Referred Children and Adolescents: Concurrent Features and Outcomes: Classification Des Comportements Dans Le Trouble Oppositionnel Avec Provocation Chez Des Enfants et Des Adolescents Aiguillés à Une Clinique: Caractéristiques Co-Occurrentes et Résultats. Can. J. Psychiatry 2021, 66, 657–666. [Google Scholar]
- Racz, S.J.; McMahon, R.J.; Gudmundsen, G.; McCauley, E.; Vander Stoep, A. Latent Classes of Oppositional Defiant Disorder in Adolescence and Prediction to Later Psychopathology. Dev. Psychopathol. 2022, 1–19. [Google Scholar] [CrossRef]
- Lavigne, J.V.; Bryant, F.B.; Hopkins, J.; Gouze, K.R. Dimensions of Oppositional Defiant Disorder in Young Children: Model Comparisons, Gender and Longitudinal Invariance. J. Abnorm. Child Psychol. 2015, 43, 423–439. [Google Scholar] [CrossRef]
- Mikolajewski, A.J.; Taylor, J.; Iacono, W.G. Oppositional Defiant Disorder Dimensions: Genetic Influences and Risk for Later Psychopathology. J. Child Psychol. Psychiatry 2017, 58, 702–710. [Google Scholar] [CrossRef]
- Burke, J.D.; Boylan, K.; Rowe, R.; Duku, E.; Stepp, S.D.; Hipwell, A.E.; Waldman, I.D. Identifying the Irritability Dimension of ODD: Application of a Modified Bifactor Model across Five Large Community Samples of Children. J. Abnorm. Psychol. 2014, 123, 841. [Google Scholar] [CrossRef]
- Waldman, I.D.; Rowe, R.; Boylan, K.; Burke, J.D. External Validation of a Bifactor Model of Oppositional Defiant Disorder. Mol. Psychiatry 2018, 26, 1. [Google Scholar] [CrossRef]
- Boylan, K.; Vaillancourt, T.; Boyle, M.; Szatmari, P. Comorbidity of Internalizing Disorders in Children with Oppositional Defiant Disorder. Eur. Child Adolesc. Psychiatry 2007, 16, 484–494. [Google Scholar] [CrossRef]
- Maughan, B.; Rowe, R.; Messer, J.; Goodman, R.; Meltzer, H. Conduct Disorder and Oppositional Defiant Disorder in a National Sample: Developmental Epidemiology. J. Child Psychol. Psychiatry 2004, 45, 609–621. [Google Scholar] [CrossRef]
- Déry, M.; Lapalme, M.; Jagiellowicz, J.; Poirier, M.; Temcheff, C.; Toupin, J. Predicting Depression and Anxiety from Oppositional Defiant Disorder Symptoms in Elementary School-Age Girls and Boys with Conduct Problems. Child Psychiatry Hum. Dev. 2017, 48, 53–62. [Google Scholar] [CrossRef]
- Cunningham, N.R.; Ollendick, T.H. Comorbidity of Anxiety and Conduct Problems in Children: Implications for Clinical Research and Practice. Clin. Child Fam. Psychol. Rev. 2010, 13, 333–347. [Google Scholar] [CrossRef]
- Boden, J.M.; Fergusson, D.M.; Horwood, L.J. Risk Factors for Conduct Disorder and Oppositional/Defiant Disorder: Evidence from a New Zealand Birth Cohort. J. Am. Acad. Child Adolesc. Psychiatry 2010, 49, 1125–1133. [Google Scholar] [CrossRef]
- Drabick, D.A.G.; Gadow, K.D.; Loney, J. Co-Occurring ODD and GAD Symptom Groups: Source-Specific Syndromes and Cross-Informant Comorbidity. J. Clin. Child Adolesc. Psychol. 2008, 37, 314–326. [Google Scholar] [CrossRef]
- Wesselhoeft, R.; Stringaris, A.; Sibbersen, C.; Kristensen, R.V.; Bojesen, A.B.; Talati, A. Dimensions and Subtypes of Oppositionality and Their Relation to Comorbidity and Psychosocial Characteristics. Eur. Child Adolesc. Psychiatry 2018, 28, 351–365. [Google Scholar] [CrossRef]
- Beauchaine, T.P.; Webster-Stratton, C.; Reid, M.J. Mediators, Moderators, and Predictors of 1-Year Outcomes among Children Treated for Early-Onset Conduct Problems: A Latent Growth Curve Analysis. J. Consult. Clin. Psychol. 2005, 73, 371. [Google Scholar] [CrossRef]
- Franco, X.; Saavedra, L.M.; Silverman, W.K. External Validation of Comorbid Patterns of Anxiety Disorders in Children and Adolescents. J. Anxiety Disord. 2007, 21, 717–729. [Google Scholar] [CrossRef]
- Walker, J.L.; Lahey, B.B.; Russo, M.F.; Frick, P.J.; Christ, M.A.G.; McBurnett, K.; Loeber, R.; Stouthamer-Loeber, M.; Green, S.M. Anxiety, Inhibition, and Conduct Disorder in Children: I. Relations to Social Impairment. J. Am. Acad. Child Adolesc. Psychiatry 1991, 30, 187–191. [Google Scholar] [CrossRef] [PubMed]
- Drabick, D.A.G.; Ollendick, T.H.; Bubier, J.L. Co-occurrence of ODD and Anxiety: Shared Risk Processes and Evidence for a Dual-pathway Model. Clin. Psychol. Sci. Pract. 2010, 17, 307–318. [Google Scholar] [CrossRef] [PubMed]
- Sachser, C.; Keller, F.; Goldbeck, L. Complex PTSD as Proposed for ICD-11: Validation of a New Disorder in Children and Adolescents and Their Response to Trauma-Focused Cognitive Behavioral Therapy. J. Child Psychol. Psychiatry Allied Discip. 2017, 58, 160–168. [Google Scholar] [CrossRef] [PubMed]
- Iampietro, M.; Giovannetti, T.; Drabick, D.A.; Kessler, R.K. Empirically Defined Patterns of Executive Function Deficits in Schizophrenia and Their Relation to Everyday Functioning: A Person-Centered Approach. Clin. Neuropsychol. 2012, 26, 1166–1185. [Google Scholar] [CrossRef] [PubMed]
- Andrade, B.F.; Waschbusch, D.A.; King, S.; Thurston, C.; McNutt, L.; Terrio, B.; Northern Partners in Action for Children and Youth, Nova Scotia. Teacher-Classified Peer Social Status: Preliminary Validation and Associations with Behavior Ratings. J. Psychoeduc. Assess. 2005, 23, 279–290. [Google Scholar] [CrossRef]
- Herzhoff, K.; Tackett, J.L. Subfactors of Oppositional Defiant Disorder: Converging Evidence from Structural and Latent Class Analyses. J. Child Psychol. Psychiatry 2016, 57, 18–29. [Google Scholar] [CrossRef]
- Althoff, R.R.; Kuny-Slock, A.V.; Verhulst, F.C.; Hudziak, J.J.; Ende, J. Classes of Oppositional-defiant Behavior: Concurrent and Predictive Validity. J. Child Psychol. Psychiatry 2014, 55, 1162–1171. [Google Scholar] [CrossRef]
- Aebi, M.; Barra, S.; Bessler, C.; Steinhausen, H.-C.; Walitza, S.; Plattner, B. Oppositional Defiant Disorder Dimensions and Subtypes among Detained Male Adolescent Offenders. J. Child Psychol. Psychiatry 2016, 57, 729–736. [Google Scholar] [CrossRef]
- Ollendick, T.H.; Greene, R.W.; Austin, K.E.; Fraire, M.G.; Halldorsdottir, T.; Allen, K.B.; Jarrett, M.A.; Lewis, K.M.; Whitmore Smith, M.; Cunningham, N.R.; et al. Parent Management Training and Collaborative & Proactive Solutions: A Randomized Control Trial for Oppositional Youth. J. Clin. Child Adolesc. Psychol. 2016, 45, 591–604. [Google Scholar] [CrossRef]
- Bögels, S.M.; Brechman-Toussaint, M.L. Family Issues in Child Anxiety: Attachment, Family Functioning, Parental Rearing and Beliefs. Clin. Psychol. Rev. 2006, 26, 834–856. [Google Scholar] [CrossRef]
- Kusche, C.A.; Cook, E.T.; Greenberg, M.T. Neuropsychological and Cognitive Functioning in Children with Anxiety, Externalizing, and Comorbid Psychopathology. J. Clin. Child Psychol. 1993, 22, 172–195. [Google Scholar] [CrossRef]
- Muris, P.; Ollendick, T.H. The Role of Temperament in the Etiology of Child Psychopathology. Clin. Child Fam. Psychol. Rev. 2005, 8, 271–289. [Google Scholar] [CrossRef]
- Raine, A.; Dodge, K.; Loeber, R.; Gatzke-Kopp, L.; Lynam, D.; Reynolds, C.; Stouthamer-Loeber, M.; Liu, J. The Reactive–Proactive Aggression Questionnaire: Differential Correlates of Reactive and Proactive Aggression in Adolescent Boys. Aggress. Behav. 2006, 32, 159–171. [Google Scholar] [CrossRef]
- Cavanagh, M.; Quinn, D.; Duncan, D.; Graham, T.; Balbuena, L. Oppositional Defiant Disorder Is Better Conceptualized as a Disorder of Emotional Regulation. J. Atten. Disord. 2017, 21, 381–389. [Google Scholar] [CrossRef]
- Suveg, C.; Sood, E.; Comer, J.S.; Kendall, P.C. Changes in Emotion Regulation Following Cognitive-Behavioral Therapy for Anxious Youth. J. Clin. Child Adolesc. Psychol. 2009, 38, 390–401. [Google Scholar] [CrossRef]
- Fraire, M.G.; Ollendick, T.H. Anxiety and Oppositional Defiant Disorder: A Transdiagnostic Conceptualization. Clin. Psychol. Rev. 2013, 33, 229–240. [Google Scholar] [CrossRef]
- Reynolds, C.R. Behavior Assessment System for Children; Wiley Online Library: Hoboken, NJ, USA, 2004. [Google Scholar]
- Pelham, W.E.; Evans, S.W.; Gnagy, E.M.; Greenslade, K.E. Teacher Ratings of DSM-III-R Symptoms for the Disruptive Behavior Disorders: Prevalence, Factor Analyses, and Conditional Probabilities in a Special Education Sample. Sch. Psychol. Rev. 1992, 21, 285–299. [Google Scholar] [CrossRef]
- Beck, J.S. Beck Youth Inventories—Second Edition for Children and Adolescents Manual; Psychological Corporation: San Antonio, TX, USA, 2005. [Google Scholar]
- Silverman, W.K.; Albano, A.M. The Anxiety Disorders Interview Schedule for Children (ADIS-C/P); Psychological Corporation: San Antonio, TX, USA, 1996. [Google Scholar]
- Shaffer, D.; Gould, M.S.; Brasic, J.; Ambrosini, P.; Fisher, P.; Bird, H.; Aluwahlia, S. A Children’s Global Assessment Scale (CGAS). Arch. Gen. Psychiatry 1983, 40, 1228–1231. [Google Scholar] [CrossRef]
- Shields, A.; Cicchetti, D. Emotion Regulation among School-Age Children: The Development and Validation of a New Criterion Q-Sort Scale. Dev. Psychol. 1997, 33, 906. [Google Scholar] [CrossRef]
- Brown, K.; Atkins, M.S.; Osborne, M.L.; Milnamow, M. A Revised Teacher Rating Scale for Reactive and Proactive Aggression. J. Abnorm. Child Psychol. 1996, 24, 473–480. [Google Scholar] [CrossRef]
- Gioia, G.A.; Guy, S.C.; Isquith, P.K.; Kenworthy, L. Behavior Rating Inventory of Executive Function; Psychological Assessment Resources: Lutz, FL, USA, 1996. [Google Scholar]
- Barkley, R.A. Defiant Children: A Clinician’s Manual for Parent Training and Assessment; Psychological Corporation: San Antonio, TX, USA, 1997. [Google Scholar]
- Greene, R.W. The Explosive Child: A New Approach for Understanding and Parenting Easily Frustrated," Chronically Inflexible" Children; HarperCollins Publishers: New York, NY, USA, 1998. [Google Scholar]
- Murrihy, R.C.; Drysdale, S.A.; Dedousis-Wallace, A.; Rémond, L.; McAloon, J.; Ellis, D.M.; Halldorsdottir, T.; Greene, R.W.; Ollendick, T.H. Community-Delivered Collaborative and Proactive Solutions and Parent Management Training for Oppositional Youth: A Randomized Trial. Behav. Ther. 2022. [Google Scholar] [CrossRef]
- Muthén, L.K. Mplus User’s Guide; Muthén & Muthén: Los Angeles, CA, USA, 2010. [Google Scholar]
- Akaike, H. Factor Analysis and AIC. Psychometrika 1987, 52, 317–332. [Google Scholar] [CrossRef]
- Schwarz, G. Estimating the Dimension of a Model. Ann. Stat. 1978, 6, 461–464. [Google Scholar] [CrossRef]
- Sclove, S.L. Application of Model-Selection Criteria to Some Problems in Multivariate Analysis. Psychometrika 1987, 52, 333–343. [Google Scholar] [CrossRef]
- Frick, P.J.; Morris, A.S. Temperament and Developmental Pathways to Conduct Problems. J. Clin. Child Adolesc. Psychol. 2004, 33, 54–68. [Google Scholar] [CrossRef]
- Frick, P.J.; Ellis, M. Callous-Unemotional Traits and Subtypes of Conduct Disorder. Clin. Child Fam. Psychol. Rev. 1999, 2, 149–168. [Google Scholar] [CrossRef]
- Gray, J.A. The Psychology of Fear and Stress; CUP Archive: Cambridge, UK, 1987; Volume 5. [Google Scholar]
- Drabick, D.A.G.; Bubier, J.; Chen, D.; Price, J.; Lanza, H.I. Source-Specific Oppositional Defiant Disorder among Inner-City Children: Prospective Prediction and Moderation. J. Clin. Child Adolesc. Psychol. 2011, 40, 23–35. [Google Scholar] [CrossRef]
- De Los Reyes, A.; Augenstein, T.M.; Wang, M.; Thomas, S.A.; Drabick, D.A.G.; Burgers, D.E.; Rabinowitz, J. The Validity of the Multi-Informant Approach to Assessing Child and Adolescent Mental Health. Psychol. Bull. 2015, 141, 858. [Google Scholar] [CrossRef]
- Anderson, S.R.; Ollendick, T.H. Diagnosing Oppositional Defiant Disorder Using the Anxiety Disorders Interview Schedule for DSM-IV: Parent Version and the Diagnostic Interview Schedule for Children. J. Psychopathol. Behav. Assess. 2012, 34, 467–475. [Google Scholar] [CrossRef]
- Nylund, K.; Bellmore, A.; Nishina, A.; Graham, S. Subtypes, Severity, and Structural Stability of Peer Victimization: What Does Latent Class Analysis Say? Child Dev. 2007, 78, 1706–1722. [Google Scholar] [CrossRef]
- Nylund, K.L.; Asparouhov, T.; Muthén, B.O. Deciding on the Number of Classes in Latent Class Analysis and Growth Mixture Modeling: A Monte Carlo Simulation Study. Struct. Equ. Model. 2007, 14, 535–569. [Google Scholar] [CrossRef]


{kind=link}
| Categorical Variables | N (%) |
|---|---|
| Gender | |
| Female | 49 (36.6) |
| Male | 85 (63.4) |
| Race | |
| White | 112 (83.6) |
| Non-white | 22 (16.4) |
| Comorbid anxiety disorder | |
| Generalized anxiety disorder | 30 (22.39) |
| Separation anxiety disorder | 16 (11.94) |
| Social phobia | 23 (17.16) |
| Specific phobia | 26 (19.40) |
| Comorbid ADHD | 89 (66.4) |
| Continuous Variables | M (SD) |
| Age in years | 9.67 (1.82) |
| ODD CSR | 5.99 (1.05) |
| CGAS | 59.37 (5.89) |
| Maternal-reported CD symptoms | 1.93 (1.74) |
| Paternal-reported CD symptoms | 1.21 (1.44) |
| Number of Classes | Number of Free Parameters | Log Likelihood | AIC | BIC | ABIC | BLRT |
|---|---|---|---|---|---|---|
| 1 | 16 | −2674.35 | 5380.70 | 5427.07 | 5376.46 | - |
| 2 | 25 | −2644.15 | 5338.30 | 5410.74 | 5331.66 | <0.001 |
| 3 | 34 | −2623.92 | 5315.84 | 5414.37 | 5306.82 | <0.001 |
| 4 | 43 | −2608.53 | 5303.06 | 5427.67 | 5291.65 | 0.0128 |
| Profile 1 Low Anx/Mod CP | Profile 2 High Anx/Mod CP | Profile 3 Mod Anx/Mod CP | Profile 4 Mod Anx/High CP | Pairwise | |||||
|---|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | M | SD | Comparisons | |
| Clinician ratings | |||||||||
| ANX CSR pre | 2.82 | 2.68 | 4.05 | 2.51 | 3.22 | 2.67 | 4.35 | 2.43 | - |
| ODD CSR pre | 5.81 | 1.12 | 6.18 | 1.01 | 5.86 | 1.20 | 6.30 | 1.18 | - |
| ODD CSR post | 3.85 | 2.83 | 3.52 | 2.76 | 3.18 | 2.73 | 4.37 | 3.09 | - |
| ODD CSR 6-month | 3.89 | 3.74 | 3.46 | 3.48 | 3.14 | 2.59 | 4.95 | 2.53 | - |
| ODD CSR 1-year | 3.71 | 3.54 | 3.94 | 4.19 | 2.98 | 3.00 | 6.16 | 2.38 | 4 > 1, 2, 3 |
| CGAS pre | 60.10 | 5.64 | 57.80 | 6.31 | 61.50 | 7.14 | 56.60 | 5.01 | 1, 3 > 4; 3 > 2 |
| CGAS post | 67.18 | 10.41 | 67.41 | 8.77 | 68.99 | 11.63 | 63.89 | 8.96 | - |
| CGAS 6-month | 66.44 | 16.82 | 67.73 | 17.61 | 68.66 | 12.45 | 51.56 | 20.81 | - |
| CGAS 1-year | 66.66 | 11.96 | 65.29 | 17.73 | 72.00 | 15.25 | 57.22 | 15.15 | 1, 3 > 4 |
| Maternal Ratings | |||||||||
| ODD symptoms | 5.42 | 2.05 | 5.74 | 2.03 | 5.63 | 2.01 | 6.43 | 2.31 | - |
| CD symptoms | 1.87 | 1.92 | 1.84 | 1.78 | 1.68 | 1.95 | 2.57 | 2.55 | - |
| Externalizing problems | 71.40 | 11.60 | 72.30 | 9.30 | 69.00 | 10.90 | 85.30 | 10.30 | 4 >1, 2, 3 |
| Aggression | 69.79 | 12.76 | 71.01 | 10.99 | 68.47 | 11.62 | 77.56 | 16.15 | - |
| Lability | 35.10 | 6.87 | 38.60 | 6.14 | 36.60 | 6.07 | 40.2 | 6.98 | 2, 4 > 1 |
| Negative emotionality | 10.25 | 2.28 | 11.64 | 1.98 | 11.17 | 2.19 | 11.78 | 3.02 | - |
| Emotional self-control | 8.45 | 3.56 | 10.90 | 3.56 | 9.94 | 3.54 | 12.30 | 3.27 | 2, 4 > 1; 4 > 3 |
| Proactive aggression | 16.23 | 3.86 | 16.60 | 3.27 | 16.45 | 4.07 | 19.06 | 3.14 | - |
| Reactive aggression | 14.45 | 2.26 | 15.55 | 2.09 | 15.26 | 2.02 | 15.79 | 2.09 | - |
| Executive functioning | 67.55 | 10.63 | 71.36 | 9.74 | 69.25 | 8.96 | 73.54 | 11.73 | - |
| Self-regulation | 41.62 | 7.03 | 43.52 | 6.18 | 42.14 | 7.29 | 43.16 | 10.27 | - |
| Paternal Ratings | |||||||||
| ODD symptoms | 3.89 | 2.59 | 5.35 | 2.87 | 3.56 | 2.46 | 5.71 | 3.88 | 2 > 1, 3; 4 > 3 |
| CD symptoms | 1.04 | 1.54 | 1.78 | 2.42 | .72 | 1.35 | 2.41 | 2.45 | 2 > 3; 4 > 3, 1 |
| Externalizing problems | 65.00 | 8.88 | 71.90 | 11.00 | 62.00 | 10.40 | 81.70 | 13.30 | 4 > 2 > 1, 3 |
| Aggression | 63.10 | 9.72 | 68.60 | 12.30 | 61.40 | 9.92 | 73.50 | 17.90 | 2, 4 > 1, 3 |
| Lability | 33.90 | 7.13 | 38.90 | 6.03 | 35.00 | 7.52 | 40.80 | 11.30 | 2, 4 > 1, 3 |
| Negative emotionality | 9.00 | 2.53 | 11.00 | 2.07 | 8.99 | 2.59 | 10.10 | 4.53 | 2 > 1, 3 |
| Emotional self-control | 7.63 | 3.24 | 10.60 | 3.44 | 8.17 | 3.16 | 10.20 | 4.84 | 2 > 1, 3; 4 > 1 |
| Proactive aggression | 15.00 | 3.18 | 15.80 | 3.16 | 15.00 | 4.55 | 19.30 | 4.71 | 4 > 1, 2, 3 |
| Reactive aggression | 13.59 | 2.85 | 14.91 | 2.81 | 14.02 | 3.18 | 16.02 | 3.46 | - |
| Executive functioning | 64.20 | 12.20 | 70.30 | 10.10 | 65.30 | 11.90 | 72.60 | 15.60 | 2, 4 > 1 |
| Self-regulation | 36.30 | 9.78 | 41.50 | 8.95 | 37.10 | 9.23 | 42.90 | 14.50 | 2 > 1, 3 |
| Teacher Ratings | |||||||||
| Externalizing problems | 59.90 | 16.30 | 59.10 | 18.00 | 53.50 | 15.60 | 72.00 | 17.80 | 4 > 1, 2, 3 |
| Aggression | 61.00 | 19.50 | 59.10 | 22.70 | 53.90 | 16.40 | 67.80 | 22.00 | 4 > 3 |
| School problems | 53.10 | 9.72 | 54.70 | 13.50 | 51.60 | 13.80 | 63.60 | 9.64 | 4 > 1, 2, 3 |
| Social skills | 38.20 | 13.40 | 45.40 | 14.20 | 47.20 | 16.00 | 40.50 | 13.70 | 2, 3 > 1 |
| Learning problems | 48.60 | 10.60 | 52.30 | 15.30 | 49.20 | 12.30 | 60.00 | 13.50 | 4 > 1, 3 |
| Study skills | 42.20 | 11.20 | 45.40 | 14.20 | 48.00 | 12.70 | 36.80 | 10.60 | 3 > 1, 4; 2 > 4 |
| Self-Report | |||||||||
| Proactive aggression | 12.60 | 2.72 | 12.10 | 2.53 | 11.60 | 2.21 | 14.7 | 3.49 | 4 > 1, 2, 3 |
| Reactive aggression | 8.85 | 2.27 | 8.92 | 2.41 | 8.29 | 2.40 | 10.7 | 3.05 | 4 > 1, 2, 3 |
| Self-concept | 40.10 | 11.80 | 42.90 | 10.70 | 44.60 | 11.30 | 34.9 | 13.70 | 2, 3 > 4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Halldorsdottir, T.; Fraire, M.G.; Drabick, D.A.G.; Ollendick, T.H. Co-Occurring Conduct Problems and Anxiety: Implications for the Functioning and Treatment of Youth with Oppositional Defiant Disorder. Int. J. Environ. Res. Public Health 2023, 20, 3405. https://doi.org/10.3390/ijerph20043405
Halldorsdottir T, Fraire MG, Drabick DAG, Ollendick TH. Co-Occurring Conduct Problems and Anxiety: Implications for the Functioning and Treatment of Youth with Oppositional Defiant Disorder. International Journal of Environmental Research and Public Health. 2023; 20(4):3405. https://doi.org/10.3390/ijerph20043405
Chicago/Turabian StyleHalldorsdottir, Thorhildur, Maria G Fraire, Deborah A. G. Drabick, and Thomas H. Ollendick. 2023. "Co-Occurring Conduct Problems and Anxiety: Implications for the Functioning and Treatment of Youth with Oppositional Defiant Disorder" International Journal of Environmental Research and Public Health 20, no. 4: 3405. https://doi.org/10.3390/ijerph20043405
APA StyleHalldorsdottir, T., Fraire, M. G., Drabick, D. A. G., & Ollendick, T. H. (2023). Co-Occurring Conduct Problems and Anxiety: Implications for the Functioning and Treatment of Youth with Oppositional Defiant Disorder. International Journal of Environmental Research and Public Health, 20(4), 3405. https://doi.org/10.3390/ijerph20043405