
Effectiveness of a Participatory Program for Improving the Cardiovascular and Cerebrovascular Health of Older Farmers in Rural Korea



Abstract
1. Introduction
2. Materials and Methods
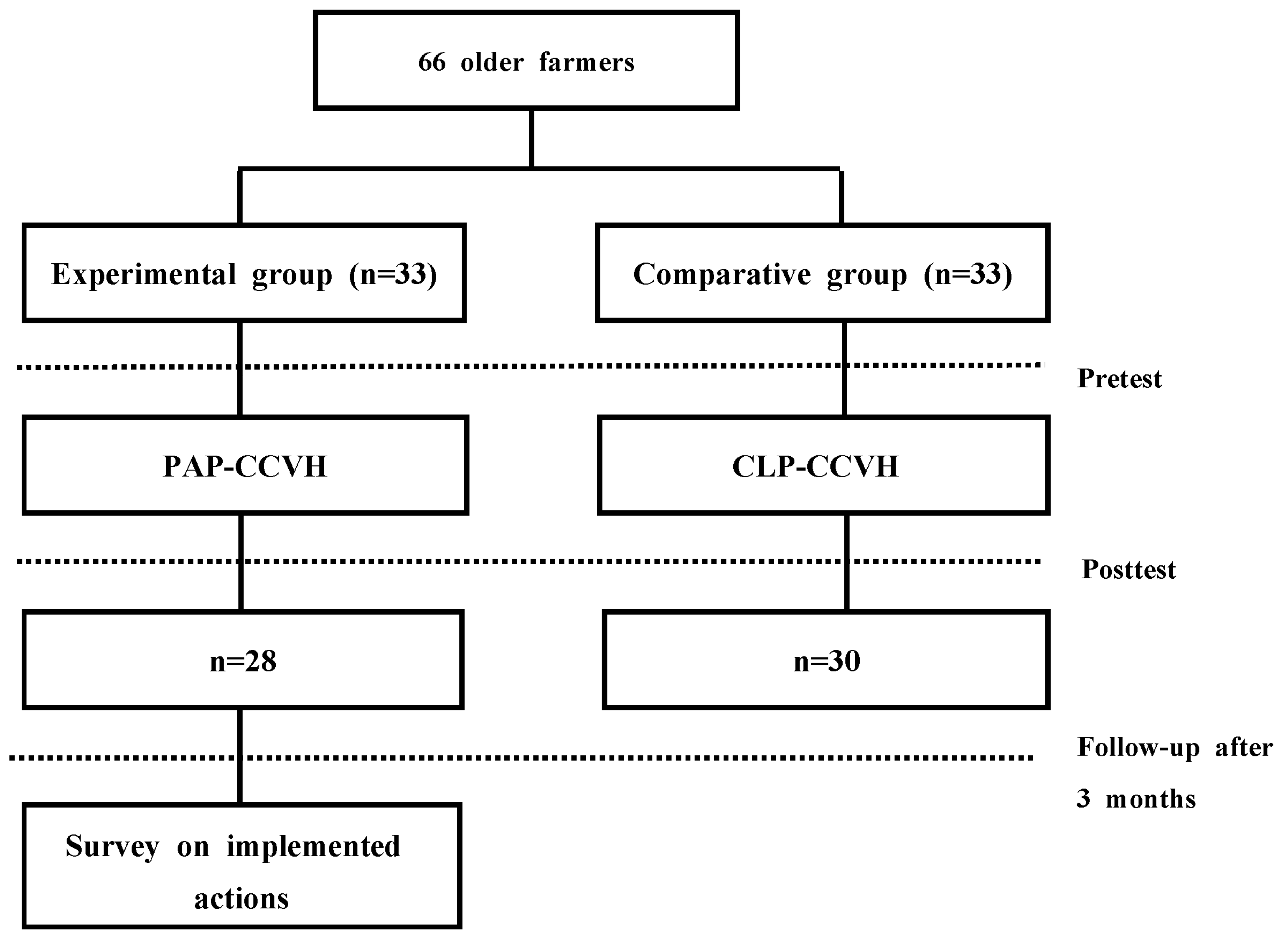
2.1. Participants and Procedures
2.2. Development of a Participatory Program for Cardiovascular and Cerebrovascular Health (PAP-CCVH)
2.2.1. Develop an Action Checklist (Organizational Level)
2.2.2. Train Facilitators (Organizational and Leader Level)
2.2.3. Conduct Group Work (Group, Individual Level)
2.3. Development of a Conventional Lecture Program for Cardiovascular and Cerebrovascular Health (CLP-CCVH)
2.4. Measurements
2.5. Data Analysis
2.6. Data Collection
3. Results
3.1. Homogeneity Test of General Characteristics and Outcome Variables
3.2. Comparison of Health Empowerment among Groups
3.3. Comparison of Self-Efficacy in Managing CCV Health among Groups
3.4. Proposed and Implemented Action Plans
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Korean Statistical Information Service. Agriculture, Forestry, and Fishery Survey in 2021. 2022. Available online: http://kostat.go.kr/portal/korea/kor_nw/1/8/6/index.board (accessed on 20 August 2022).
- Statistics Korea. 2018 Statistics on the Aged. Available online: http://kostat.go.kr/portal/eng/pressReleases/11/3/index.board (accessed on 14 June 2019).
- Rautiainen, R.H.; Ohsfeldt, R.; Sprince, N.L.; Donham, K.J.; Burmeister, L.F.; Reynolds, S.J.; Saarimaki, P.; Zwerling, C. Cost of compensated injuries and occupational diseases in agriculture in Finland. J. Agromed. 2005, 10, 21–29. [Google Scholar] [CrossRef]
- National Center for Health Statistics. Summary health statistics for U.S. adults: National Health Interview Survey, 2009. Vital Health Stat 10(249). 2010; DHHS publication No. (PHS) 2011–1577. Available online: http://www.cdc.gov/nchs/data/series/sr_10/sr10_249.pdf. (accessed on 12 September 2011).
- Record, N.B.; Onion, D.K.; Prior, R.E.; Dixon, D.C.; Record, S.S.; Fowler, F.L.; Cayer, G.R.; Amos, C.I.; Pearson, T.A. Community-wide cardiovascular disease prevention programs and health outcomes in a rural county, 1970-2010. JAMA 2015, 313, 147–155. [Google Scholar] [CrossRef]
- Artinian, N.T.; Fletcher, G.F.; Mozaffarian, D.; Kris-Etherton, P.; Van Horn, L.; Lichtenstein, A.H.; Kumanyika, S.; Kraus, W.E.; Fleg, J.L.; Redeker, N.S.; et al. Interventions to promote physical activity and dietary lifestyle changes for cardiovascular risk factor reduction in adults: A scientific statement from the American Heart Association. Circulation 2010, 122, 406–441. [Google Scholar] [CrossRef] [PubMed]
- Stirrat, C.; Mann, S. Perceptions of cardiovascular risk factors among cardiology outpatients. Heart Lung Circ. 2008, 17, s22–s23. [Google Scholar] [CrossRef]
- Eckel, R.H.; Jakicic, J.M.; Ard, J.D.; de Jesus, J.M.; Miller, N.H.; Hubbard, V.S.; Lee, I.; Lichtenstein, A.H.; Loria, C.M.; Millen, B.E.; et al. 2013 AHA/ACC guideline on lifestyle management to reduce cardiovascular risk. Circulation 2014, 129, s76–s99. [Google Scholar] [CrossRef]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA guideline on the primary prevention of cardiovascular disease: A report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines. Circulation 2019, 140, e596–e646. [Google Scholar] [CrossRef] [PubMed]
- Vongpatanasin, W. Cardiovascular morbidity and mortality in high-risk populations: Epidemiology and opportunities for risk reduction. J. Clin. Hypertens. 2007, 9, 11–15. [Google Scholar] [CrossRef]
- Pearson, T.A.; Blair, S.N.; Daniels, S.R.; Eckel, R.H.; Fair, J.M.; Fortmann, S.P.; Franklin, B.A.; Goldstein, L.B.; Greenland, P.; Grundy, S.M.; et al. AHA guidelines for primary prevention of cardiovascular disease and stroke: 2002 update: Consensus panel guide to comprehensive risk reduction for adult patients without coronary or other atherosclerotic vascular diseases. Circulation 2002, 106, 288–391. [Google Scholar] [CrossRef]
- Ju, K.; So, H. Effects of the nutrition education program on self-efficacy, diet behavior pattern and cardiovascular risk factors for the patients with cardiovascular disease. J. Korean Acad. Nurs. 2008, 38, 64–73. [Google Scholar] [CrossRef]
- Ham, O.K.; Kim, B.J. Evaluation of a cardiovascular health promotion programme offered to low-income women in Korea. J. Clin. Nurs. 2011, 20, 1245–1254. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, K.; Stage, M.; Abildgaard, J.S.; Brauer, C.V. Participatory intervention from an organizational perspective: Employees as active agents in creating a healthy work environment. In Salutogenic Organizations and Chang; Bauer, G., Jenny, G., Eds.; Springer: Dordrecht, The Netherlands, 2013; pp. 327–350. [Google Scholar] [CrossRef]
- Bandura, A. Exercise of personal and collective efficacy in changing societies. In Self-Efficacy in Changing Societies; Bandura, A., Ed.; Cambridge University Press: New York, NY, USA, 1995; pp. 1–45. [Google Scholar]
- Kärner Köhler, A.; Tingström, P.; Jaarsma, T.; Nilsson, S. Patient empowerment and general self-efficacy in patients with coronary heart disease: A cross-sectional study. BMC Fam. Pract. 2018, 19, 76. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.H.; Yoshikawa, E.; Yoshikawa, T.; Kogi, K.; Jung, M.H. Utility of action checklists as a consensus building tool. Ind. Health 2015, 53, 85–94. [Google Scholar] [CrossRef]
- Warner, G.; Packer, T.; Villeneuve, M.; Audulv, A.; Versnel, J. A systematic review of the effectiveness of stroke self-management programs for improving function and participation outcomes: Self-management programs for stroke survivors. Disabil. Rehabil. 2015, 37, 2141–2163. [Google Scholar] [CrossRef]
- Augustine, H.; Roberts, J.; Packer, T. Everyday participation: Important outcomes for people with chronic conditions. Occup. Ther. Now 2011, 13, 8–10. [Google Scholar]
- Sung, K.; Park, J.H.; Park, M.K. Influences of social support, self-esteem and hope on health conservation of the vulnerable elderly with diabetes. J. Korean Acad. Community Health Nurs. 2017, 28, 386–396. [Google Scholar] [CrossRef]
- Yoon, S.Y.; Kam, S.; Kim, J.S.; Jo, S.Y.; Kwon, Y.J.; Song, I.W.; Woo, K.H. The effect of participatory approach program for cardiovascular disease prevention in the workplace. Korean J. Occup. Environ. Med. 2012, 24, 133–144. [Google Scholar] [CrossRef]
- Hwang, S.Y.; Shim, J.L.; Kang, D.Y.; Choi, J. Poor oral health predicts higher 10-year cardiovascular risk: A propensity score matching analysis. J. Cardiovasc. Nurs. 2018, 33, 429–436. [Google Scholar] [CrossRef] [PubMed]
- Park, C.; Park, Y.H. Validity and reliability of Korean version of health empowerment scale (K-HES) for older adults. Asian Nurs. Res. 2013, 7, 142–148. [Google Scholar] [CrossRef]
- Anderson, R.M.; Fitzgerald, J.T.; Gruppen, L.D.; Funnell, M.M.; Oh, M.S. The diabetes empowerment scale-short form (DES-SF). Diabetes Care 2003, 26, 1641–1642. [Google Scholar] [CrossRef]
- Park, M.K.; Kim, J.H. Effects of a comprehensive lifestyle improvement program for middle-aged women with cardio-cerebrovascular disease-related risk factors. J. Korean Acad. Community Health Nurs. 2013, 24, 111–122. [Google Scholar] [CrossRef]
- Maddux, J.E.; Sherer, M.; Rogers, R.W. Self-efficacy expectancy and outcome expectancy: Their relationship and their effects on behavioral intentions. Cogn. Ther. Res. 1982, 6, 207–211. [Google Scholar] [CrossRef]
- Becker, D.M.; Levine, D.M. Risk perception, knowledge, and lifestyles in siblings of people with premature coronary disease. Am. J. Prev. Med. 1987, 3, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Eliasson, A.; Kashani, M.; Vernalis, M. Results of a prospective cardiovascular disease prevention program. Prev. Med. Rep. 2021, 22, 101344. [Google Scholar] [CrossRef]
- Raemdonck, E.; Lambotte, D.; De Witte, N.; Gorus, E. Giving voice to informal caregivers of community-dwelling older adults: A systematic review of empowerment interventions. Health Soc. Care Community 2022, 30, e3354–e3368. [Google Scholar] [CrossRef] [PubMed]
- Shin, D.S.; Kim, C.J.; Choi, Y.J. Effects of an empowerment program for self-management among rural older adults with hypertension in South Korea. Aust. J. Rural. Health 2016, 24, 213–219. [Google Scholar] [CrossRef]
- Chang, A.K.; Fritschi, C.; Kim, M.J. Nurse-led empowerment strategies for hypertensive patients with metabolic syndrome. Contemp. Nurse 2012, 42, 118–128. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.H.; Yoon, S.Y. Effects of a worksite-based self-management program in traditional retail market workers: Longitudinal associations with metabolic parameters. Int. J. Environ. Res. Public Health 2022, 19, 2854. [Google Scholar] [CrossRef]
- de Boer, A.G.; Burdorf, A.; van Duivenbooden, C.; Frings-Dresen, M.H. The effect of individual counselling and education on work ability and disability pension: A prospective intervention study in the construction industry. Occup. Environ. Med. 2007, 64, 792–797. [Google Scholar] [CrossRef]


{kind=link}
| Checklist Items | |
|---|---|
| Hypertension management | |
| 1. | Take antihypertensive medication as prescribed by a doctor. |
| 2. | Measure blood pressure at least 3 times a week and record the results (stay below 130/80 mmHg). |
| 3. | Receive regular urine tests, kidney function tests, and electrocardiograms (ECGs). |
| Diabetes management | |
| 4. | Take diabetes medications as prescribed by a doctor. |
| 5. | Know the normal blood sugar levels, such as fasting blood sugar (70–130 mg/dL), 2-h postprandial blood sugar (90–180 mg/dL), hemoglobin A1C (≤6.5%), and strictly manage your blood sugar with the goal of maintaining normal levels. |
| 6. | Receive regular screening for diabetes complications: (HbA1C test every 3 months), fundus (retina) test every year, kidney function test (microalbuminuria test) every year, peripheral sensory test, and carotid artery ultrasonogram. |
| Dyslipidemia management | |
| 7. | Take cholesterol-lowering medications as prescribed by a doctor. |
| 8. | Receive regular hyperlipidemia (dyslipidemia) tests. |
| 9. | Know the normal lipid levels, such as total cholesterol (<200 mg/dL), triglyceride (<150 mg/dL), LDL cholesterol (<100 mg/dL), and HDL cholesterol (≥60 mg/dL), and manage the levels. |
| Diet management | |
| 10. | Do not eat soups made with salty foods, such as soybean paste stew and kimchi stew. Eat bland foods as much as possible. |
| 11. | Drink more than 1.5 L of water per day. |
| 12. | Regularly eat food with a low glycemic index: multigrain rice, beans, vegetables, seaweed, and raw fruits with low sugar content. |
| 13. | Try to avoid foods high in saturated or trans fats, such as animal fats, fried foods, and fried pancakes. |
| 14. | To build stronger muscles, exercise (for example, walking up the stairs and doing sit-ups) and eat protein-rich foods: chicken breasts, egg whites, fish, and lean cuts of beef or pork. |
| 15. | Eat a variety of foods in even proportions, such as rice, other grains, vegetables, fruits, milk, dairy products, meat, fish, eggs, and beans (all rich in iron, zinc, calcium, and vitamins). |
| 16. | Chew slowly many times when eating. |
| Exercise management | |
| 17. | Avoid working in the same posture for a long time. Use a timer to stretch your body every hour, consciously stretching the chest and back muscles to improve blood circulation. |
| 18. | Do aerobic exercise regularly, at least 3 times a week for at least 30 min (a total of 150 min or more per week) and move around as much as possible. Walking dilates blood vessels, which improves blood circulation, enhances immunity, promotes removal of accumulated substances from the body, and suppresses aging. |
| 19. | Do strength training (free gymnastics, yoga, dumbbells, sit-ups) consistently for several minutes. |
| 20. | Maintain a correct posture while sitting or walking, and consciously stretch your chest and back muscles. A correct posture improves blood circulation by 25%, increases calorie consumption, and improves work efficiency. |
| Stress and sleep management | |
| 21. | Have conversations with others, empathize with them, and praise others as you listen to their stories. Talking openly is the best way to relieve built-up stress. |
| 22. | Do abdominal breathing at least 3 times a day. |
| 23. | Laugh for more than 10 s, 3 times a day. Laughing loudly through exhalation releases good hormones, removes waste products from the body, relaxes blood vessels, and helps improve immunity. |
| 24. | Regulate overall health with a regular soaking bath. It has been reported that the average life expectancy of those who bathe regularly was 20 years longer than that of those without a bath/sauna culture. |
| 25. | Try to sleep at least 6–8 h. |
| Oral management | |
| 26. | Brush teeth immediately after eating. |
| 27. | For the purposes of prevention and treatment, visit the dentist regularly for care. |
| Drinking habit management | |
| 28. | Do not drink alcohol every day. If drinking, then drink below your personal limits. Excessive drinking increases fatigue, so take breaks of 2–3 days with no alcohol. Alcohol and its byproduct acetaldehyde are class 1 carcinogens. Therefore, excessive drinking increases the risk of cancer. |
| 29. | Drink slowly and drink water from time to time. Alcohol is detoxified and excreted in water. |
| Smoking habit management | |
| 30. | Let people around you know if you are trying to quit smoking. |
| 31. | Exercise (strolling, walking) or engage in hobbies to reduce the desire to smoke. |
| Session | Theme | Program Content | Pedagogical Strategy | Time (minutes) |
|---|---|---|---|---|
| Participatory program for cardiovascular and cerebrovascular health (PAP-CCVH) | ||||
| 1. | Opening presentations | ∙Symptoms, emergency actions, and treatment of CCV disease | Lecture | 30 |
| Self-management | ∙Learn to measure blood pressure, blood sugar, and lipid levels | Facilitator support | 30 | |
| 2. | Learning by doing | ∙Practice action checklist ∙Identify positive CCV health behaviors and risky behaviors that need to be improved | Training tool Facilitator support | 60 |
| 3. | Encourage exchange of experiences | ∙Exchange good experiences related to implementing the CCV disease prevention actions | Group discussion Facilitator support | 30 |
| Promote individual involvement | ∙Plan improvement actions | Individual mapping Facilitator support | 30 | |
| Conventional lecture program for cardiovascular and cerebrovascular health (CLP-CCVH) | ||||
| 1. | Opening presentations Self-management | ∙Symptoms, emergency actions, and treatment of CCV disease ∙Learn to measure blood pressure, blood sugar, and lipid levels | Expert lecture | 60 |
| 2. | CCV health management Self-management | ∙Management of diet, exercise, stress, sleep, oral hygiene, alcohol intake, and smoking ∙Learn to measure blood pressure, blood sugar, and lipid levels | Expert lecture | 60 |
| 3. | CCV health management | ∙Management of diet, exercise, stress, sleep, oral hygiene, alcohol intake, and smoking | Expert lecture | 60 |
| Characteristics | Categories | n (%), Mean ± SD | Χ2/t | p | |
|---|---|---|---|---|---|
| Exp. (n = 28) | Comp. (n = 30) | ||||
| Gender | Male | 4 (14.3) | 4 (13.3) | 0.11 | 0.916 |
| Female | 24 (85.7) | 26 (86.7) | |||
| Age (years) | 60–69 | 13 (48.1) | 10 (33.3) | 1.29 | 0.255 |
| 70–80 | 14 (51.9) | 20 (66.7) | |||
| Education | ≤Elementary school | 7 (22.3) | 10 (33.3) | 2.20 | 0.332 |
| Middle school | 10 (37.0) | 6 (20.0) | |||
| ≥High school | 11 (40.7) | 14 (46.7) | |||
| Spouse | Yes | 19 (67.9) | 22 (73.3) | 0.21 | 0.647 |
| No | 9 (32.1) | 8 (26.7) | |||
| Perceived health status | Excellent | 1 (3.6) | 0 (0) | 1.48 + | 0.891 |
| Good | 4 (14.3) | 4 (13.3) | |||
| Moderate | 16 (57.1) | 20 (66.7) | |||
| Bad | 7 (25.0) | 6 (20.0) | |||
| Very bad | 0 (0) | 0 (0) | |||
| Smoking | Yes | 0 (0) | 2 (6.7) | 1.93 | 0.164 |
| No | 28 (100) | 28 (93.3) | |||
| Alcohol | Yes | 8 (28.6) | 14 (46.7) | 2.01 | 0.156 |
| No | 20 (71.4) | 16 (53.3) | |||
| Health empowerment | 3.49 ± 0.69 | 3.42 ± 0.45 | 5.20 | 0.653 | |
| Self-efficacy in managing CCV health | 3.90 ± 0.43 | 3.68 ± 0.42 | 0.05 | 0.052 | |
| Characteristics | Categories | M ± SE | Z(p) + | Sources | Χ2(p) ++ | |
|---|---|---|---|---|---|---|
| Pretest | Posttest | |||||
| Health empowerment | Exp. | 3.49 ± 0.11 | 3.99 ± 0.12 | −3.51 (<0.001) | Group | 2.80 (0.094) |
| Comp. | 3.42 ± 0.10 | 3.57 ± 0.11 | −2.28 (0.023) | Time | 28.70 (<0.001) | |
| G × T | 7.92 (0.005) | |||||
| Self-efficacy in | Exp. | 3.90 ± 0.08 | 4.30 ± 0.08 | −3.75 (<0.001) | Group | 10.37 (0.001) |
| managing CCV health | Comp. | 3.68 ± 0.07 | 3.85 ± 0.08 | −3.41 (0.001) | Time | 37.53 (<0.001) |
| G × T | 5.94 (0.015) | |||||
| Type of Action Plan | Proposed Action Plans (n) | Implemented Action Plans (n) | Rate of Implemented Improvements (%) |
|---|---|---|---|
| Hypertension management | 47 | 41 | 89.1 |
| Diabetes management | 37 | 31 | 86.2 |
| Dyslipidemia management | 31 | 26 | 84.1 |
| Diet management | 78 | 71 | 92.2 |
| Exercise management | 47 | 41 | 89.1 |
| Stress and sleep management | 80 | 73 | 92.2 |
| Oral hygiene management | 30 | 30 | 100.0 |
| Drinking habit management | 2 | 0 | 0 |
| Smoking habit management | 0 | 0 | 0 |
| Total | 352 | 313 | 88.9 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, K.-Y.; Jin, J.; Kim, Y.-H. Effectiveness of a Participatory Program for Improving the Cardiovascular and Cerebrovascular Health of Older Farmers in Rural Korea. Int. J. Environ. Res. Public Health 2023, 20, 3210. https://doi.org/10.3390/ijerph20043210
Kim K-Y, Jin J, Kim Y-H. Effectiveness of a Participatory Program for Improving the Cardiovascular and Cerebrovascular Health of Older Farmers in Rural Korea. International Journal of Environmental Research and Public Health. 2023; 20(4):3210. https://doi.org/10.3390/ijerph20043210
Chicago/Turabian StyleKim, Ki-Youn, Juhye Jin, and Yeon-Ha Kim. 2023. "Effectiveness of a Participatory Program for Improving the Cardiovascular and Cerebrovascular Health of Older Farmers in Rural Korea" International Journal of Environmental Research and Public Health 20, no. 4: 3210. https://doi.org/10.3390/ijerph20043210
APA StyleKim, K.-Y., Jin, J., & Kim, Y.-H. (2023). Effectiveness of a Participatory Program for Improving the Cardiovascular and Cerebrovascular Health of Older Farmers in Rural Korea. International Journal of Environmental Research and Public Health, 20(4), 3210. https://doi.org/10.3390/ijerph20043210