
Pandemic-Related Stress and Other Emotional Difficulties in a Sample of Men and Women Living in Romantic Relationships during the COVID-19 Pandemic



Abstract
1. Introduction
Research Question and Hypotheses
2. Materials and Methods
2.1. Participants and Procedure
2.2. Tools
2.3. Statistical Analyses
3. Results
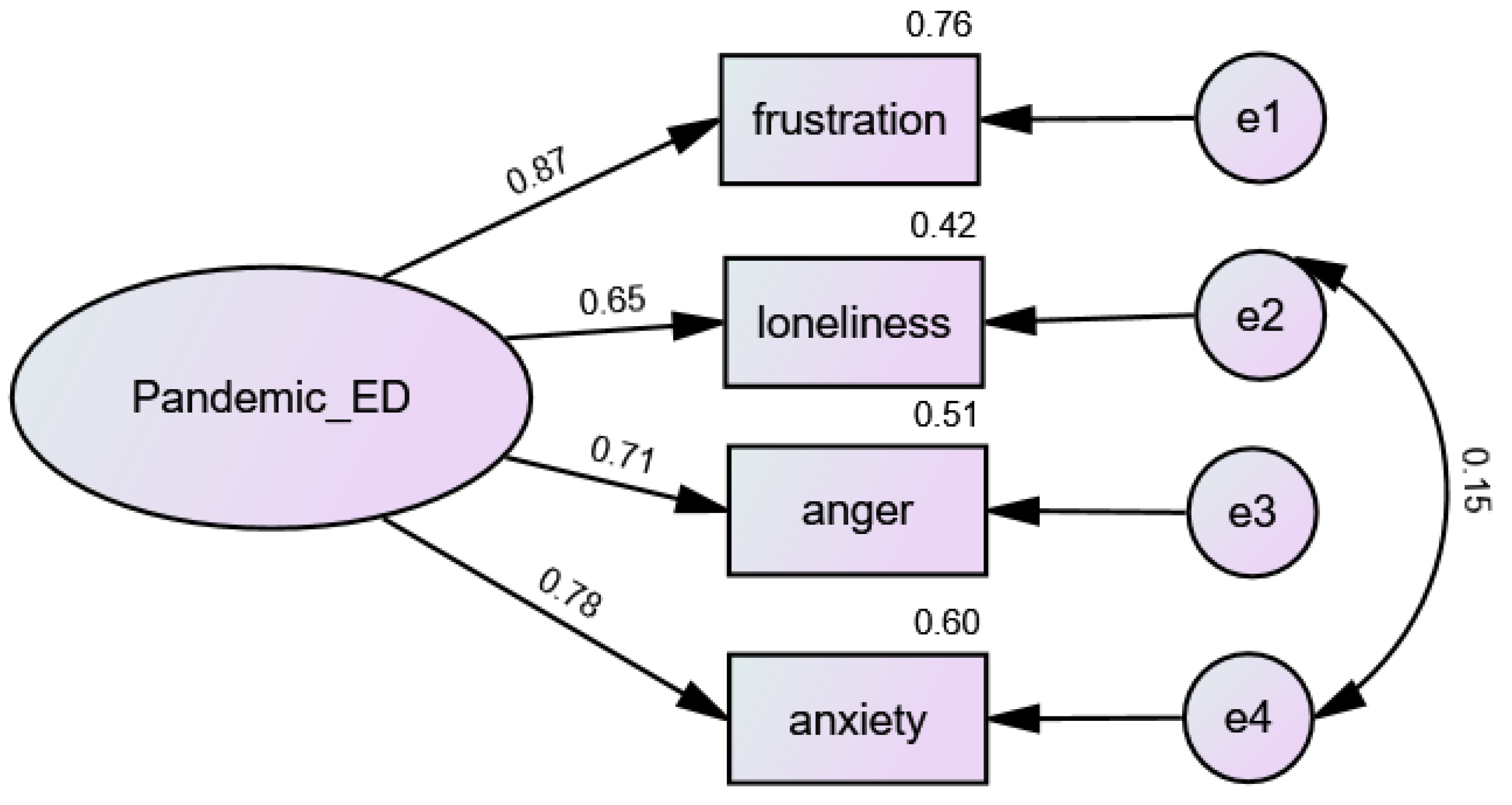
3.1. Pandemic-Related Emotional Difficulties Scale
3.2. Correlational Analyses
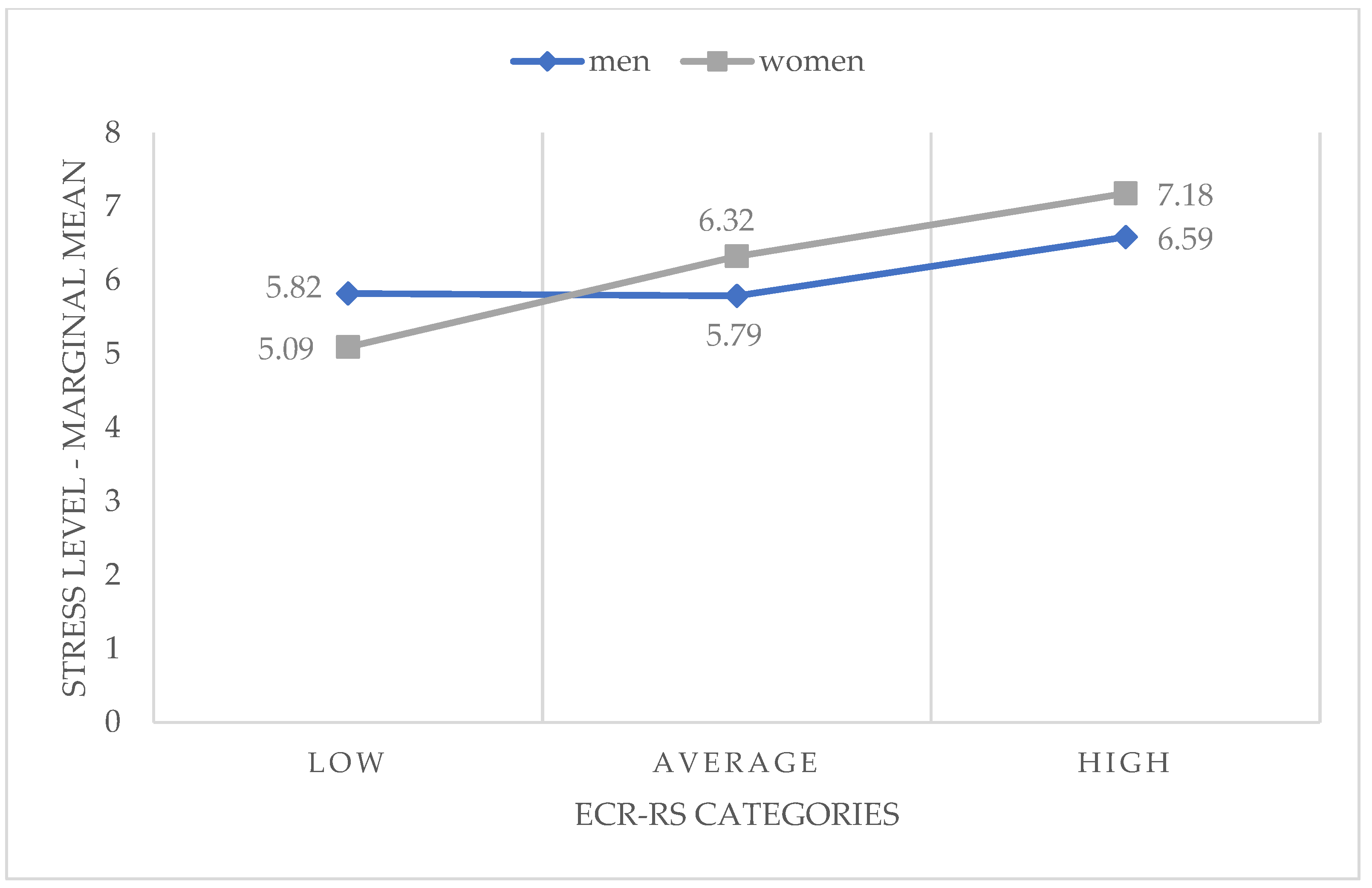
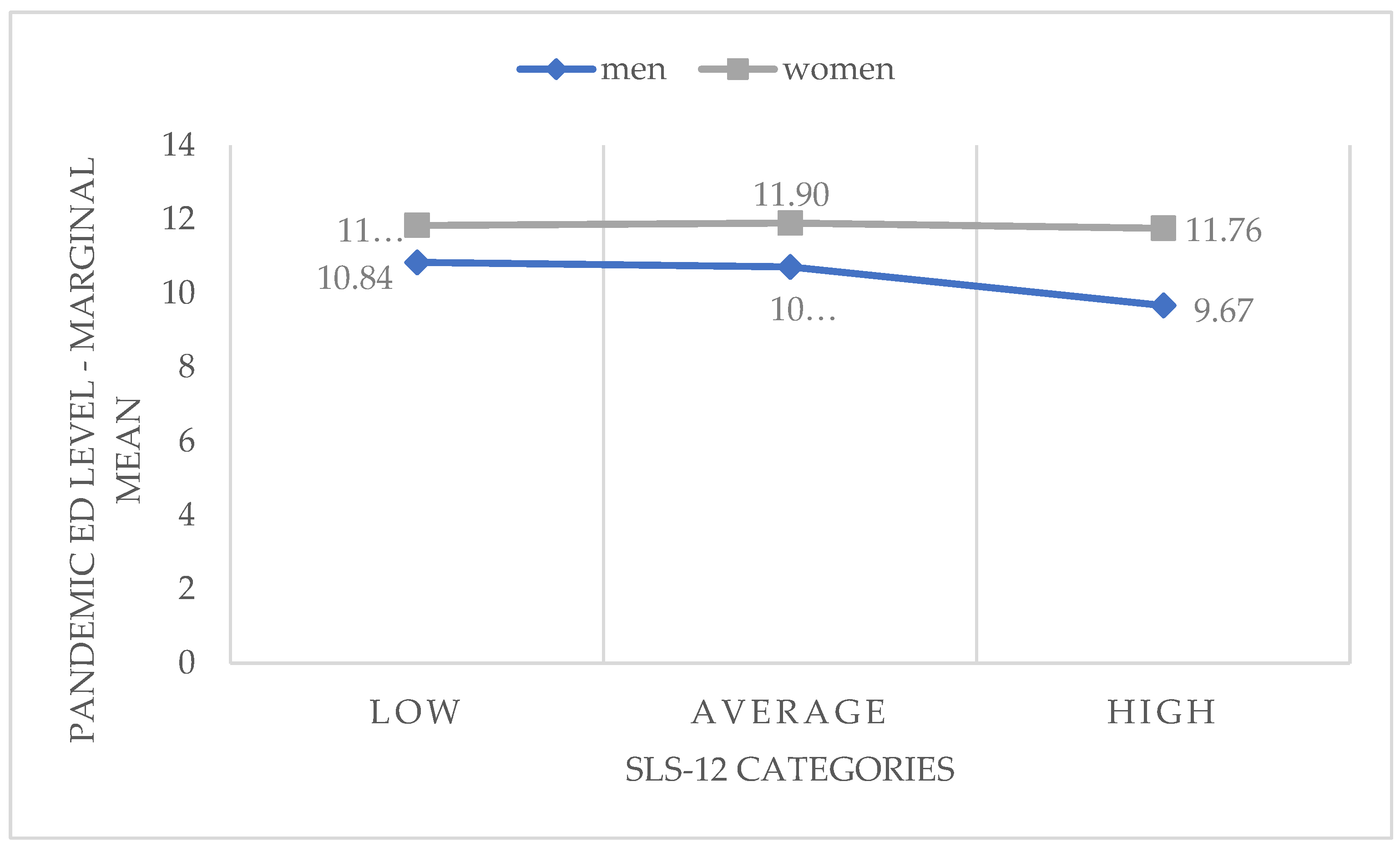
3.3. Differences between Women and Men in Stress and Pandemic-Related Difficulties
3.4. Determinants of Stress and Pandemic-Related Difficulties
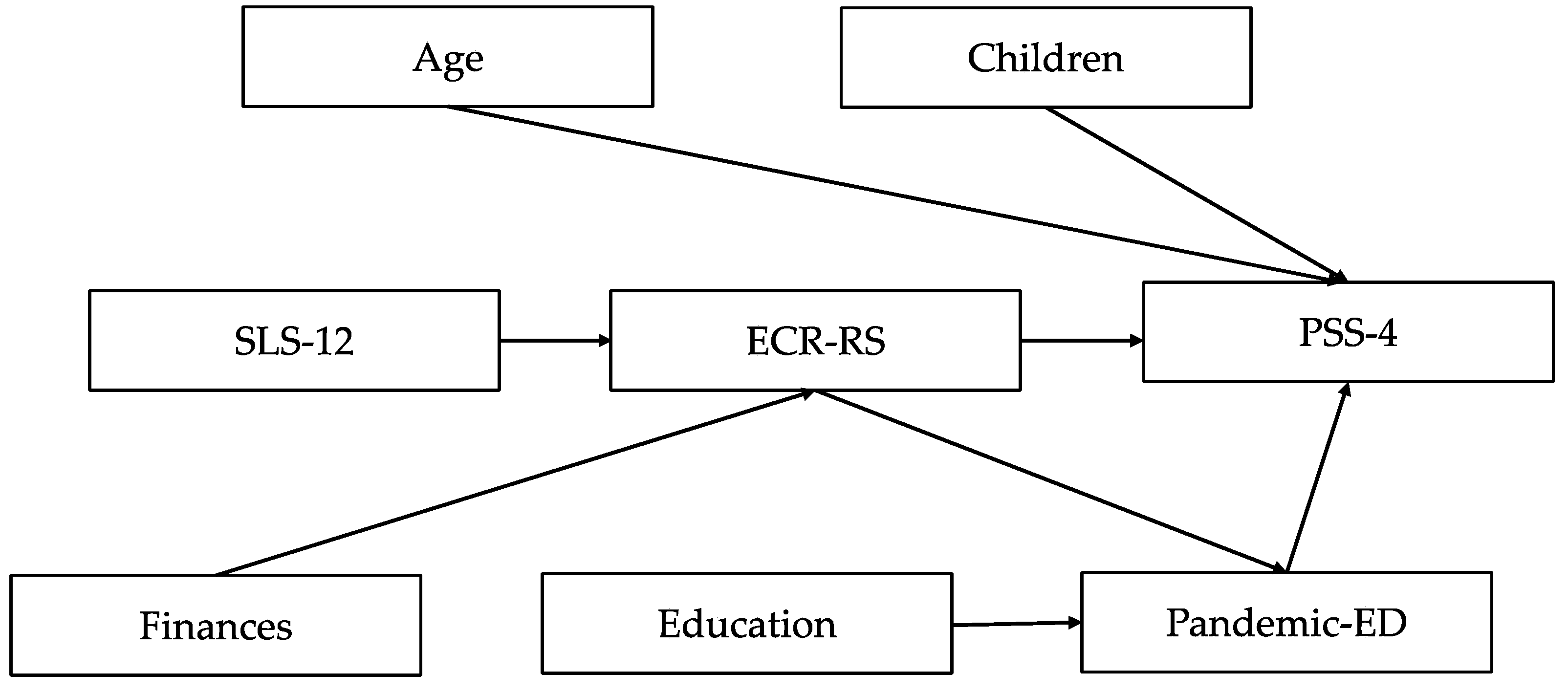
3.5. SEM Models
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

References
- Fiorillo, A.; Frangou, S. European Psychiatry 2020: Moving Forward. Eur. Psychiatry 2020, 63, e1. [Google Scholar] [CrossRef]
- Salari, N.; Hosseinian-Far, A.; Jalali, R.; Vaisi-Raygani, A.; Rasoulpoor, S.; Mohammadi, M.; Rasoulpoor, S.; Khaledi-Paveh, B. Prevalence of Stress, Anxiety, Depression among the General Population during the COVID-19 Pandemic: A Systematic Review and Meta-Analysis. Glob. Health 2020, 16, 57. [Google Scholar] [CrossRef]
- Van Agteren, J.; Bartholomaeus, J.; Fassnacht, D.B.; Iasiello, M.; Ali, K.; Lo, L.; Kyrios, M. Using Internet-Based Psychological Measurement to Capture the Deteriorating Community Mental Health Profile During COVID-19: Observational Study. JMIR Ment. Health 2020, 7, e20696. [Google Scholar] [CrossRef]
- Birditt, K.S.; Nevitt, M.R.; Almeida, D.M. Daily Interpersonal Coping Strategies: Implications for Self-Reported Well-Being and Cortisol. JSPR 2015, 32, 687–706. [Google Scholar] [CrossRef]
- Kujawa, A.; Green, H.; Compas, B.E.; Dickey, L.; Pegg, S. Exposure to COVID-19 Pandemic Stress: Associations with Depression and Anxiety in Emerging Adults in the United States. Depress. Anxiety 2020, 37, 1280–1288. [Google Scholar] [CrossRef]
- Laghi, F.; Di Tata, D.; Bianchi, D.; Lonigro, A.; Pompili, S.; Zammuto, M.; Baiocco, R. Problematic Alcohol Use in Young Adults during the COVID-19 Lockdown in Italy. Psychol. Health Med. 2022, 27, 139–149. [Google Scholar] [CrossRef]
- Zheng, J.; Morstead, T.; Sin, N.; Klaiber, P.; Umberson, D.; Kamble, S.; DeLongis, A. Psychological Distress in North America during COVID-19: The Role of Pandemic-Related Stressors. Soc. Sci. Med. 2021, 270, 113687. [Google Scholar] [CrossRef]
- Juster, R.-P.; McEwen, B.S.; Lupien, S.J. Allostatic Load Biomarkers of Chronic Stress and Impact on Health and Cognition. Neurosci. Biobehav. Rev. 2010, 35, 2–16. [Google Scholar] [CrossRef]
- Thoits, P.A. Stress and Health: Major Findings and Policy Implications. J. Health Soc. Behav. 2010, 51, S41–S53. [Google Scholar] [CrossRef]
- Hajian, S.; Mehrabi, E.; Simbar, M.; Houshyari, M. Coping Strategies and Experiences in Women with a Primary Breast Cancer Diagnosis. APJCP 2017, 18, 215–224. [Google Scholar] [CrossRef]
- Ogueji, A.I.; Okoloba, M.M. Compassion-Focused Therapy (Cft) As An Intervention Against Suicidal Ideation In Newly Diagnosed People Living With Hiv/Aids (Plwha) Attending A Nigerian Maternity Teaching Hospital. Glob. Psychiatry 2020, 3, 104–112. [Google Scholar] [CrossRef]
- Ogueji, I.A.; Okoloba, M.M.; Demoko Ceccaldi, B.M. Coping Strategies of Individuals in the United Kingdom during the COVID-19 Pandemic. Curr. Psychol. 2022, 41, 7493–7499. [Google Scholar] [CrossRef]
- Prati, G.; Pietrantoni, L. Optimism, Social Support, and Coping Strategies As Factors Contributing to Posttraumatic Growth: A Meta-Analysis. J. Loss Trauma 2009, 14, 364–388. [Google Scholar] [CrossRef]
- Babicka-Wirkus, A.; Wirkus, L.; Stasiak, K.; Kozłowski, P. University Students’ Strategies of Coping with Stress during the Coronavirus Pandemic: Data from Poland. PLoS ONE 2021, 16, e0255041. [Google Scholar] [CrossRef]
- Guszkowska, M.; Dąbrowska-Zimakowska, A. Coping with Stress During the Second Wave of the COVID-19 Pandemic by Polish University Students: Strategies, Structure, and Relation to Psychological Well-Being. PRBM 2022, 15, 339–352. [Google Scholar] [CrossRef]
- Cacioppo, J.T.; Cacioppo, S. Social Relationships and Health: The Toxic Effects of Perceived Social Isolation: Social Relationships and Health. Soc. Personal. Psychol. Compass 2014, 8, 58–72. [Google Scholar] [CrossRef]
- Hawkley, L.C.; Cacioppo, J.T. Loneliness Matters: A Theoretical and Empirical Review of Consequences and Mechanisms. Ann. Behav. Med. 2010, 40, 218–227. [Google Scholar] [CrossRef]
- Ong, A.D.; Uchino, B.N.; Wethington, E. Loneliness and Health in Older Adults: A Mini-Review and Synthesis. Gerontology 2016, 62, 443–449. [Google Scholar] [CrossRef]
- Newsom, J.T.; Nishishiba, M.; Morgan, D.L.; Rook, K.S. The Relative Importance of Three Domains of Positive and Negative Social Exchanges: A Longitudinal Model with Comparable Measures. Psychol. Aging 2003, 18, 746–754. [Google Scholar] [CrossRef]
- Rook, K.S. Social Networks in Later Life: Weighing Positive and Negative Effects on Health and Well-Being. Curr. Dir. Psychol. Sci. 2015, 24, 45–51. [Google Scholar] [CrossRef]
- Karandashev, V.A. Cultural Perspective on Romantic Love. Online Readings Psychol. Cult. 2015, 5, 2. [Google Scholar] [CrossRef]
- Graham, J.M. Measuring Love in Romantic Relationships: A Meta-Analysis. JSPR 2011, 28, 748–771. [Google Scholar] [CrossRef]
- Collins, W.A.; Welsh, D.P.; Furman, W. Adolescent Romantic Relationships. Annu. Rev. Psychol. 2009, 60, 631–652. [Google Scholar] [CrossRef]
- Baumeister, R.F.; Leary, M.R. The Need to Belong: Desire for Interpersonal Attachments as a Fundamental Human Motivation. Psychol. Bull. 1995, 117, 497–529. [Google Scholar] [CrossRef]
- Mikulincer, M.; Shaver, P.R.; Simpson, J.A.; Dovidio, J.F. (Eds.) APA Handbook of Personality and Social Psychology; American Psychological Association: Washington, DC, USA; Volume 3, Interpersonal relations. [CrossRef]
- Till, B.; Niederkrotenthaler, T. Romantic Relationships and Mental Health During the COVID-19 Pandemic in Austria: A Population-Based Cross-Sectional Survey. Front. Psychol. 2022, 13, 857329. [Google Scholar] [CrossRef]
- Meier, A.; Allen, G. Intimate Relationship Development during the Transition to Adulthood: Differences by Social Class. New Dir. Child Adolesc. Dev. 2008, 2008, 25–39. [Google Scholar] [CrossRef]
- Montgomery, M.J. Psychosocial Intimacy and Identity: From Early Adolescence to Emerging Adulthood. J. Adolesc. Res. 2005, 20, 346–374. [Google Scholar] [CrossRef]
- Dush, C.M.K.; Amato, P.R. Consequences of Relationship Status and Quality for Subjective Well-Being. JSPR 2005, 22, 607–627. [Google Scholar] [CrossRef]
- Gove, W.R.; Hughes, M.; Style, C.B. Does Marriage Have Positive Effects on the Psychological Well-Being of the Individual? JHSB 1983, 24, 122. [Google Scholar] [CrossRef]
- Holt-Lunstad, J.; Birmingham, W.; Jones, B.Q. Is There Something Unique about Marriage? The Relative Impact of Marital Status, Relationship Quality, and Network Social Support on Ambulatory Blood Pressure and Mental Health. Ann. Behav. Med. 2008, 35, 239–244. [Google Scholar] [CrossRef]
- Kõlves, K.; Ide, N.; De Leo, D. Fluctuations of Suicidality in the Aftermath of a Marital Separation: 6-Month Follow-up Observations. J. Affect. Disord. 2012, 142, 256–263. [Google Scholar] [CrossRef] [PubMed]
- Blanca, M.J.; Ferragut, M.; Ortiz-Tallo, M.; Bendayan, R. Life Satisfaction and Character Strengths in Spanish Early Adolescents. J. Happiness Stud. 2018, 19, 1247–1260. [Google Scholar] [CrossRef]
- Park, N.; Peterson, C.; Seligman, M.E.P. Strengths of Character and Well-Being. J. Soc. Clin. Psychol. 2004, 23, 603–619. [Google Scholar] [CrossRef]
- Su, Z.; Cheshmehzangi, A.; McDonnell, D.; Šegalo, S.; Ahmad, J.; Bennett, B. Gender Inequality and Health Disparity amid COVID-19. Nurs. Outlook 2022, 70, 89–95. [Google Scholar] [CrossRef]
- Bambra, C.; Riordan, R.; Ford, J.; Matthews, F. The COVID-19 Pandemic and Health Inequalities. J. Epidemiol Community Health 2020, 74, 964–968. [Google Scholar] [CrossRef] [PubMed]
- Guerrina, R.; Borisch, B.; Callahan, L.F.; Howick, J.; Reginster, J.-Y.; Mobasheri, A. Health and Gender Inequalities of the COVID-19 Pandemic: Adverse Impacts on Women’s Health, Wealth and Social Welfare. FWH 2021, 2, 670310. [Google Scholar] [CrossRef]
- Jin, J.-M.; Bai, P.; He, W.; Wu, F.; Liu, X.-F.; Han, D.-M.; Liu, S.; Yang, J.-K. Gender Differences in Patients With COVID-19: Focus on Severity and Mortality. Public Health Front. 2020, 8, 152. [Google Scholar] [CrossRef] [PubMed]
- Ausín, B.; González-Sanguino, C.; Castellanos, M.Á.; Muñoz, M. Gender-Related Differences in the Psychological Impact of Confinement as a Consequence of COVID-19 in Spain. J. Gen. Stud. 2021, 30, 29–38. [Google Scholar] [CrossRef]
- Szabo, A.; Ábel, K.; Boros, S. Attitudes toward COVID-19 and Stress Levels in Hungary: Effects of Age, Perceived Health Status, and Gender. Psychol Trauma 2020, 12, 572–575. [Google Scholar] [CrossRef] [PubMed]
- Horesh, D.; Kapel Lev-Ari, R.; Hasson-Ohayon, I. Risk Factors for Psychological Distress during the COVID-19 Pandemic in Israel: Loneliness, Age, Gender, and Health Status Play an Important Role. Br. J. Health Psychol. 2020, 25, 925–933. [Google Scholar] [CrossRef]
- Carlson, D.L.; Petts, R.J.; Pepin, J.R. Changes in US Parents’ Domestic Labor During the Early Days of the COVID-19 Pandemic. Sociol. Inq. 2022, 92, 1217–1244. [Google Scholar] [CrossRef] [PubMed]
- Fisher, A.N.; Ryan, M.K. Gender Inequalities during COVID-19. Group Process. Intergroup Relat. 2021, 24, 237–245. [Google Scholar] [CrossRef]
- Hennekam, S.; Shymko, Y. Coping with the COVID-19 Crisis: Force Majeure and Gender Performativity. Gend. Work Organ. 2020, 27, 788–803. [Google Scholar] [CrossRef]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.H. Review of the psychometric evidence of the perceived stress scale. Asian Nurs. Res. (Korean Soc. Nurs. Sci). 2012, 6, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Fraley, R.C.; Heffernan, M.E.; Vicary, A.M.; Brumbaugh, C.C. The experiences in close relationships—Relationship Structures Questionnaire: A method for assessing attachment orientations across relationships. Psychol. Assess. 2011, 23, 615–625. [Google Scholar] [CrossRef]
- Kozakiewicz, A.; Izdebski, Z.; Mazur, J. The Measurement of Love: Psychometric Properties and Preliminary Findings of the Short Love Scale (SLS-12) in a Polish Sample. Int. J. Environ. Res. Public Health 2022, 19, 13269. [Google Scholar] [CrossRef]
- Perneger, T.V.; Burnand, B. A simple imputation algorithm reduced missing data in SF-12 health surveys. J. Clin. Epidemiol. 2005, 58, 142–149. [Google Scholar] [CrossRef]
- Terwee, C.B.; Bot, S.D.M.; de Boer, M.R.; van der Windt, D.A.W.M.; Knol, D.L.; Dekker, J.; Bouter, L.M.; de Vet, H.C.W. Quality criteria were proposed for measurement properties of health status questionnaires. J. Clin. Epidemiol. 2007, 60, 34–42. [Google Scholar] [CrossRef]
- Cain, M.K.; Zhang, Z.; Yuan, K.-H. Univariate and multivariate skewness and kurtosis for measuring nonnormality: Prevalence, influence and estimation. Behav. Res. Methods 2017, 49, 1716–1735. [Google Scholar] [CrossRef]
- Arbuckle, J.M. IBM® SPSS® AmosTM 25 User’s Guide; IBM: Chumney, FL, USA, 2017. [Google Scholar]
- Finney, S.J.; DiStefano, C. Nonnormal and categorical data in structural equation modeling. In Structural Equation Modeling. A Second Course, 2nd ed.; Hancock, G.R., Mueller, R.O., Eds.; Information Age Publishing: Greenwich, CT, USA, 2013; pp. 439–492. [Google Scholar]
- Hancock, G.R.; Liu, M. Bootstrapping standard errors and data-model fit statistics in structural modeling. In Handbook of Structural Equation Modeling; Hoyle, R.H., Ed.; The Guilford Press: New York, NY, USA, 2012; pp. 296–306. [Google Scholar]
- Hair, J.F. Multivariate Data Analysis; Cengage India: Delhi, India, 2018. [Google Scholar]
- Alpar, R. Application of Multivariate Statistical Methods; Detail Press: Ankara, Turkey, 2013. [Google Scholar]
- McDonald, R.P.; Marsh, H.W. Choosing a multivariate model: Noncentrality and goodness of fit. Psychol. Bull. 1990, 107, 247–255. [Google Scholar] [CrossRef]
- Marsh, H.W.; Hocevar, D. Application of confirmatory factor analysis to the study of self-concept: First- and higher order factor models and their invariance across groups. Psychol. Bull. 1985, 97, 562–582. [Google Scholar] [CrossRef]
- Petrocelli, J.V. Hierarchical multiple regression in counseling research: Common problems and possible remedies. Meas. Eval. Couns. Dev. 2003, 36, 9–22. [Google Scholar] [CrossRef]
- Zhao, X.; Lynch, J.G., Jr.; Chen, Q. Reconsidering Baron and Kenny: Myths and truths about mediation analysis. J. Consum. Res. 2010, 37, 197–206. [Google Scholar] [CrossRef]
- Mehmetoglu, M. Medsem: A Stata package for statistical mediation analysis. Int. J. Comput. Econ. Econom. 2018, 8, 63–78. [Google Scholar]
- Montemurro, N. The Emotional Impact of COVID-19: From Medical Staff to Common People. Brain Behav. Immun. 2020, 87, 23–24. [Google Scholar] [CrossRef]
- Rajkumar, R.P. COVID-19 and Mental Health: A Review of the Existing Literature. Asian J. Psychiatr. 2020, 52, 102066. [Google Scholar] [CrossRef]
- Vindegaard, N.; Benros, M.E. COVID-19 Pandemic and Mental Health Consequences: Systematic Review of the Current Evidence. Brain Behav. Immun. 2020, 89, 531–542. [Google Scholar] [CrossRef]
- Pietromonaco, P.R.; Overall, N.C. Applying Relationship Science to Evaluate How the COVID-19 Pandemic May Impact Couples’ Relationships. Am. Psychol. 2021, 76, 438–450. [Google Scholar] [CrossRef]
- Simpson, J.A.; Rholes, W.S. Chapter Six—Adult Attachment Orientations, Stress, and Romantic Relationships. Adv. Exp. Soc. Psycholy 2012, 45, 279–328. [Google Scholar] [CrossRef]
- Walen, H.R.; Lachman, M.E. Social Support and Strain from Partner, Family, and Friends: Costs and Benefits for Men and Women in Adulthood. J. Soc. Pers. Relatsh. 2000, 17, 5–30. [Google Scholar] [CrossRef]
- Diener, E.; Gohm, C.L.; Suh, E.; Oishi, S. Similarity of the Relations between Marital Status and Subjective Well-Being Across Cultures. J. Cross Cult. Psychol. 2000, 31, 419–436. [Google Scholar] [CrossRef]
- Efklides, A.; Kalaitzidou, M.; Chankin, G. Subjective Quality of Life in Old Age in Greece: The Effect of Demographic Factors, Emotional State, and Adaptation to Aging. Eur. Psychol. 2003, 8, 178–191. [Google Scholar] [CrossRef]
- O’Connor, R.C.; Wetherall, K.; Cleare, S.; McClelland, H.; Melson, A.J.; Niedzwiedz, C.L.; O’Carroll, R.E.; O’Connor, D.B.; Platt, S.; Scowcroft, E.; et al. Mental Health and Well-Being during the COVID-19 Pandemic: Longitudinal Analyses of Adults in the UK COVID-19 Mental Health & Wellbeing Study. Br. J. Psychiatry 2021, 218, 326–333. [Google Scholar] [CrossRef]
- Proto, E.; Quintana-Domeque, C. COVID-19 and Mental Health Deterioration by Ethnicity and Gender in the UK. PLoS ONE 2021, 16, e0244419. [Google Scholar] [CrossRef] [PubMed]
- Etheridge, B.; Spantig, L. The gender gap in mental well-being at the onset of the Covid-19 pandemic: Evidence from the UK. Eur. Econ. Rev. 2022, 145, 104114. [Google Scholar] [CrossRef] [PubMed]
- Kowal, M.; Coll-Martín, T.; Ikizer, G.; Rasmussen, J.; Eichel, K.; Studzińska, A.; Koszałkowska, K.; Karwowski, M.; Najmussaqib, A.; Pankowski, D.; et al. Who is the Most Stressed During the COVID-19 Pandemic? Data From 26 Countries and Areas. Appl. Psychol. Health Well-Being 2020, 12, 946–966. [Google Scholar] [CrossRef]
- Schnell, T.; Krampe, H. Meaning in Life and Self-Control Buffer Stress in Times of COVID-19: Moderating and Mediating Effects with Regard to Mental Distress. Front. Psychiatry 2020, 11, 582352. [Google Scholar] [CrossRef] [PubMed]
- De Oliveira, L.; Carvalho, J. Women’s Sexual Health During the Pandemic of COVID-19: Declines in Sexual Function and Sexual Pleasure. Curr. Sex. Health Rep. 2021, 13, 76–88. [Google Scholar] [CrossRef]
- Schokkenbroek, J.M.; Hardyns, W.; Anrijs, S.; Ponnet, K. Partners in lockdown: Relationship stress in men and women during the COVID-19 pandemic. Couple Fam. Psychol. Res. Pract. 2021, 10, 10–149. [Google Scholar] [CrossRef]
- Brennan, K.A.l; Shaver, P.R. Attachment styles and personality disorders: Their connections to each other and to parental divorce, parental death, and perceptions of parental caregiving. J. Pers. 1998, 66, 835–878. [Google Scholar] [CrossRef] [PubMed]
- Ogolsky, B.G.; Monk, J.K. Maintaining relationships. In The Cambridge Handbook of Personal Relationships; Vangelisti, A., Perlman, D., Eds.; Cambridge University Press: Cambridge, UK, 2018; pp. 523–537. [Google Scholar] [CrossRef]
- Matud, M.P. Gender differences in stress and coping styles. Pers. Indiv. Differ. 2004, 37, 1401–1415. [Google Scholar] [CrossRef]
- Jackson, J.B.; Miller, R.B.; Oka, M.; Henry, R.G. Gender differences in marital satisfaction: A meta-analysis. J. Marriage Fam. 2014, 76, 105–129. [Google Scholar] [CrossRef]
- Rusu, P.P. Dyadic coping in Romanian couples. In Couples Coping with Stress: A Cross-Cultural Perspective; Falconier, M.K., Randall, A.K., Bodenmann, G., Eds.; Routledge/Taylor & Francis Group: New York, NY, USA, 2016; pp. 187–202. [Google Scholar]
- Randall, A.K.; Leon, G.; Basili, E.; Martos, T.; Boiger, M.; Baldi, M.; Hocker, L.; Kline, K.; Masturzi, A.; Aryeetey, R.; et al. Coping with Global Uncertainty: Perceptions of COVID-19 Psychological Distress, Relationship Quality, and Dyadic Coping for Romantic Partners across 27 Countries. JSPR 2022, 39, 3–33. [Google Scholar] [CrossRef]
- Donato, S.; Parise, M.; Pagani, A.F.; Lanz, M.; Regalia, C.; Rosnati, R.; Iafrate, R. Together Against COVID-19 Concerns: The Role of the Dyadic Coping Process for Partners’ Psychological Well-Being During the Pandemic. Front. Psychol. 2021, 11, 578395. [Google Scholar] [CrossRef]
- Ahmed, M.Z.; Ahmed, O.; Aibao, Z.; Hanbin, S.; Siyu, L.; Ahmad, A. Epidemic of COVID-19 in China and Associated Psychological Problems. Asian J. Psychiatr. 2020, 51, 102092. [Google Scholar] [CrossRef]
- Huang, Y.; Zhao, N. Generalized Anxiety Disorder, Depressive Symptoms and Sleep Quality during COVID-19 Outbreak in China: A Web-Based Cross-Sectional Survey. Psychiatry Res. 2020, 288, 112954. [Google Scholar] [CrossRef]
- Cluver, L.; Lachman, J.M.; Sherr, L.; Wessels, I.; Krug, E.; Rakotomalala, S.; Blight, S.; Hillis, S.; Bachman, G.; Green, O.; et al. Parenting in a Time of COVID-19. Lancet 2020, 395, e64. [Google Scholar] [CrossRef]
- Waddell, N.; Overall, N.C.; Chang, V.T.; Hammond, M.D. Gendered division of labor during a nationwide COVID-19 lockdown: Implications for relationship problems and satisfaction. JSPR. 2021, 38, 1759–1781. [Google Scholar] [CrossRef]
- Di Giorgio, E.; Di Riso, D.; Mioni, G.; Cellini, N. The Interplay between Mothers’ and Children Behavioral and Psychological Factors during COVID-19: An Italian Study. Eur. Child Adolesc. Psychiatry 2021, 30, 1401–1412. [Google Scholar] [CrossRef]
- Morelli, M.; Cattelino, E.; Baiocco, R.; Trumello, C.; Babore, A.; Candelori, C.; Chirumbolo, A. Parents and Children During the COVID-19 Lockdown: The Influence of Parenting Distress and Parenting Self-Efficacy on Children’s Emotional Well-Being. Front. Psychol. 2020, 11, 584645. [Google Scholar] [CrossRef]
- Park, C.L.; Russell, B.S.; Fendrich, M.; Finkelstein-Fox, L.; Hutchison, M.; Becker, J. Americans’ COVID-19 Stress, Coping, and Adherence to CDC Guidelines. J. Gen. Intern. Med. 2020, 35, 2296–2303. [Google Scholar] [CrossRef]
- Russell, B.S.; Hutchison, M.; Tambling, R.; Tomkunas, A.J.; Horton, A.L. Initial Challenges of Caregiving During COVID-19: Caregiver Burden, Mental Health, and the Parent–Child Relationship. Child Psychiatry Hum. Dev. 2020, 51, 671–682. [Google Scholar] [CrossRef] [PubMed]
- Fontanesi, L.; Marchetti, D.; Mazza, C.; Di Giandomenico, S.; Roma, P.; Verrocchio, M.C. The effect of the COVID-19 lockdown on parents: A call to adopt urgent measures. Psychol. Trauma Theory Res. Pract. Policy 2020, 12, S79–S81. [Google Scholar] [CrossRef]
- Uthede, S.; Nilsson, I.; Wagman, P.; Håkansson, C.; Farias, L. Occupational balance in parents of pre-school children: Potential differences between mothers and fathers. Scand. J. Occup. Ther. 2022, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Dew, J. The Association Between Consumer Debt and the Likelihood of Divorce. J. Fam. Econ. Iss. 2011, 32, 554–565. [Google Scholar] [CrossRef]
- Kelley, H.H.; LeBaron, A.B.; Hill, E.J. Family Matters: Decade Review from Journal of Family and Economic Issues. J. Fam. Econ. Issues 2021, 42, 20–33. [Google Scholar] [CrossRef] [PubMed]
- APA. Stress in America. American Psychological Association. 2019. Available online: https://www.apa.org/news/press/releases/stress/2019/stress-america-2019.pdf (accessed on 5 January 2023).
- Kelley, H.H.; Lee, Y.; LeBaron-Black, A.; Dollahite, D.C.; James, S.; Marks, L.D.; Hall, T. Change in Financial Stress and Relational Wellbeing During COVID-19: Exacerbating and Alleviating Influences. J. Fam. Econ. Issues 2022, 5841. [Google Scholar] [CrossRef]
- Turliuc, M.N.; Candel, O.S. Not All in the Same Boat. Socioeconomic Differences in Marital Stress and Satisfaction During the Covid-19 Pandemic. Front. Psychol. 2021, 12, 635148. [Google Scholar] [CrossRef]
- Gamonal-Limcaoco, S.; Montero-Mateos, E.; Lozano-López, M.T.; Maciá-Casas, A.; Matías-Fernández, J.; Roncero, C. Perceived stress in different countries at the beginning of the coronavirus pandemic. Int. J. Psychiatry Med. 2022, 57, 309–322. [Google Scholar] [CrossRef]
- Dang, H.-A.H.; Viet Nguyen, C. Gender Inequality during the COVID-19 Pandemic: Income, Expenditure, Savings, and Job Loss. World Dev. 2021, 140, 105296. [Google Scholar] [CrossRef] [PubMed]
- Ogan, M.A.; Monk, J.K.; Kanter, J.B.; Proulx, C.M. Stress, Dyadic Coping, and Relationship Instability During the COVID-19 Pandemic. JSPR 2021, 38, 2944–2964. [Google Scholar] [CrossRef]
- Pollard, A.E.; Rogge, R.D. Love in the Time of COVID-19: A Multi-Wave Study Examining the Salience of Sexual and Relationship Health During the COVID-19 Pandemic. Arch. Sex. Behav. 2022, 51, 247–271. [Google Scholar] [CrossRef]
- Clavél, F.D.; Cutrona, C.E.; Russell, D.W. United and divided by stress: How stressors differentially influence social support in African American couples over time. Pers. Soc. Psychol. Bull. 2017, 43, 1050–1064. [Google Scholar] [CrossRef] [PubMed]
- Diamond, L.M.; Hicks, A.M. “It’s the economy, honey!” Couples’ blame attributions during the 2007-2009 economic crisis. Pers. Relatsh. 2012, 19, 586–600. [Google Scholar] [CrossRef]
- Bodenmann, G.; Randall, A.K.; Falconier, M.K. Coping in couples: The Systemic Transactional Model (STM). In Couples Coping with Stress: A Cross-Cultural Perspective; Falconier, M.K., Randall, A.K., Bodenmann, G., Eds.; Routledge/Taylor & Francis Group: New York, NY, USA, 2016; pp. 5–22. [Google Scholar]
- Huebschmann, N.A.; Sheets, E.S. Don’t Fear Conflict: Relationship Stress Beliefs in Friend, Familial, and Romantic Relationships. Psi Chi J. 2021, 26, 252–261. [Google Scholar] [CrossRef]
- Lorant, V.; Smith, P.; Van den Broeck, K.; Nicaise, P. Psychological Distress Associated with the COVID-19 Pandemic and Suppression Measures during the First Wave in Belgium. BMC Psychiatry 2021, 21, 112. [Google Scholar] [CrossRef]
- Van der Velden, P.G.; Hyland, P.; Contino, C.; von Gaudecker, H.-M.; Muffels, R.; Das, M. Anxiety and Depression Symptoms, the Recovery from Symptoms, and Loneliness before and after the COVID-19 Outbreak among the General Population: Findings from a Dutch Population-Based Longitudinal Study. PLoS ONE 2021, 16, e0245057. [Google Scholar] [CrossRef]
- Koçak, O.; Koçak, Ö.E.; Younis, M.Z. The Psychological Consequences of COVID-19 Fear and the Moderator Effects of Individuals’ Underlying Illness and Witnessing Infected Friends and Family. Int. J. Environ. Res. Public Health 2021, 18, 1836. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Categories | Total N = 1405 | Male N = 709 | Female N = 696 |
|---|---|---|---|---|
| Education | Elementary and vocational | 25.2 | 20.6 | 29.9 |
| High school | 35.2 | 33.9 | 36.6 | |
| University | 39.6 | 45.6 | 34.5 | |
| Place of residence | Large cities | 30.6 | 36.8 | 24.3 |
| Small towns | 31.2 | 33.4 | 29.0 | |
| Rural areas | 38.2 | 29.9 | 46.7 | |
| Relationship status | Formal | 77.5 | 78.7 | 76.3 |
| Informal | 22.5 | 21.3 | 23.7 | |
| Children | Yes | 83.6 | 83.2 | 84.1 |
| No | 16.4 | 16.8 | 15.9 | |
| Financial situation | Worse | 36.2 | 33.9 | 38.6 |
| Same or hard to say | 58.9 | 60.9 | 56.9 | |
| Improved | 4.8 | 5.2 | 4.5 |
| CMIN/DF | RMR | GFI | AGFI | CFI | NFI | RFI | IFI | TLI | RMSEA |
|---|---|---|---|---|---|---|---|---|---|
| 2.432/1 | 0.008 | 0.999 | 0.991 | 0.999 | 0.999 | 0.994 | 0.999 | 0.996 | 0.032 |
| Pandemic-ED Items | M | SD | Skewness | Kurtosis | Floor Effect (%) | Ceiling Effect (%) |
|---|---|---|---|---|---|---|
| frustration | 3.03 | 1.164 | −0.056 | −0.599 | 12.6 | 12.7 |
| loneliness | 2.38 | 1.135 | 0.471 | −0.454 | 27.8 | 5.4 |
| anger | 2.81 | 1.204 | 0.113 | −0.760 | 17.7 | 10.5 |
| anxiety | 2.76 | 1.139 | 0.175 | −0.512 | 16.2 | 9.0 |
| Scale | PSS-4 | Pandemic-ED | ECR-RS Total | SLS-12 | Age in Years |
|---|---|---|---|---|---|
| PSS-4 | 1 | 0.444 ** | 0.370 ** | −0.248 ** | −0.232 ** |
| Pandemic-ED | 0.444 ** | 1 | 0.262 ** | −0.226 ** | −0.084 * |
| ECR-RS-total | 0.370 ** | 0.262 ** | 1 | −0.701 ** | −0.098 ** |
| SLS-12 | −0.248 ** | −0.226 ** | −0.701 ** | 1 | −0.051 |
| Age in years | −0.232 ** | −0.084 * | −0.098 ** | −0.051 | 1 |
| Scale | M (SD) (N = 1405) | Men (N = 709) | Women (N = 696) | U Mann-Whitney | p | Glass’ Delta |
|---|---|---|---|---|---|---|
| PSS-4 | 5.65 (3.17) | 5.15 | 6.16 | −5.741 | <0.001 | 0.331 |
| Pandemic-ED | 10.99 (3.83) | 10.12 | 11.86 | −8.720 | <0.001 | 0.474 |
| ECR-RS_total | 22.52 (11.26) | 21.70 | 23.35 | −1.862 | 0.068 | |
| Anxiety | 7.46 (4.84) | 7.05 | 7.87 | −2.371 | 0.018 | 0.183 |
| Avoidance | 15.06 (8.17) | 16.65 | 15.48 | −0.607 | 0.544 | |
| SLS-12 | 48.46 (10.23) | 49.35 | 47.54 | −2.564 | 0.010 | 0.192 |
| Sexual life | 7.21 (2.38) | 7.27 | 7.16 | −0.618 | 0.537 | |
| Closeness | 7.77 (2.09) | 7.90 | 7.64 | −1.434 | 0.152 | |
| Commitment | 33.47 (6.62) | 34.18 | 32.74 | −3.386 | <0.001 | 0.215 |
| Independent Variable PSS-4 | Model 1 | Model 2 | Model 3 | |||
|---|---|---|---|---|---|---|
| β | p | β | p | β | p | |
| Gender * | 0.094 | <0.001 | 0.099 | <0.001 | 0.027 | 0.262 |
| Age | −0.165 | <0.001 | −0.138 | <0.001 | −0.143 | <0.001 |
| Education * | −0.026 | 0.307 | −0.021 | 0.402 | −0.043 | 0.060 |
| Place of residence * | 0.009 | 0.717 | −0.005 | 0.829 | 0.000 | 0.991 |
| Relationship status * | −0.022 | 0.465 | −0.007 | 0.823 | 0.000 | 0.988 |
| Length of relationship | −0.041 | 0.353 | −0.032 | 0.456 | −0.017 | 0.668 |
| Children * | −0.034 | 0.223 | −0.035 | 0.208 | −0.047 | 0.068 |
| Financial situation * | 0.159 | <0.001 | 0.145 | <0.001 | 0.053 | 0.024 |
| SLS-12 | −0.250 | <0.001 | −0.045 | 0.212 | −0.025 | 0.453 |
| ECR-RS | 0.280 | <0.001 | 0.219 | <0.001 | ||
| Pandemic-ED | 0.358 | <0.001 | ||||
| R-sq | 0.163 | 0.198 | 0.298 | |||
| Independent Variable Pandemic-ED | Model 1 | Model 2 | Model 3 | |||
|---|---|---|---|---|---|---|
| β | p | β | p | β | p | |
| Gender * | 0.199 | <0.001 | 0.202 | <0.001 | 0.166 | <0.001 |
| Age | −0.005 | 0.910 | −0.011 | 0.789 | 0.062 | 0.118 |
| Education * | 0.060 | 0.016 | 0.063 | 0.011 | 0.071 | 0.002 |
| Place of residence * | 0.016 | 0.513 | 0.014 | 0.572 | 0.012 | 0.601 |
| Relationship status * | −0.029 | 0.334 | −0.020 | 0.511 | −0.017 | 0.536 |
| Length of relationship | −0.047 | 0.285 | −0.042 | 0.340 | −0.030 | 0.463 |
| Children * | 0.034 | 0.221 | 0.034 | 0.221 | 0.047 | 0.072 |
| Financial situation * | 0.266 | <0.001 | 0.256 | <0.001 | 0.203 | <0.001 |
| SLS-12 | −0.180 | <0.001 | −0.055 | 0.131 | −0.038 | 0.257 |
| ECR-RS | 0.171 | <0.001 | 0.068 | 0.048 | ||
| PSS_4 | 0.367 | <0.001 | ||||
| R-sq | 0.159 | 0.172 | 0.280 | |||
| Total (N = 1405) | Men (N = 709) | Women (N = 696) | ||||
|---|---|---|---|---|---|---|
| Path | Estimate | p | Estimate | p | Estimate | p |
| SLS-12 -> ECR-RS | −0.724 | <0.001 | −0.701 | <0.001 | −0.739 | <0.001 |
| Finances -> ECR-RS | 0.056 | 0.002 | 0.051 | 0.053 | 0.061 | 0.015 |
| ECR-RS -> Pandemic-ED | 0.228 | <0.001 | 0.279 | <0.001 | 0.170 | <0.001 |
| Education -> Pandemic-ED | 0.038 | 0.123 | 0.057 | 0.103 | 0.067 | 0.061 |
| ECR-RS -> PSS-4 | 0.241 | <0.001 | 0.219 | <0.001 | 0.266 | <0.001 |
| Pandemic-ED -> PSS-4 | 0.378 | <0.001 | 0.371 | <0.001 | 0.360 | <0.001 |
| Children -> PSS-4 | 0.049 | 0.042 | 0.016 | 0.650 | 0.094 | 0.005 |
| Age -> PSS-4 | −0.163 | <0.001 | −0.114 | 0.002 | −0.196 | <0.001 |
| Total (N = 1405) | Men (N = 709) | Women (N = 696) | ||||
|---|---|---|---|---|---|---|
| Path | Indirect Effect (95%CI) | p | Indirect Effect (95%CI) | p | Indirect Effect (95%CI) | p |
| Finances -> Pandemic-ED | 0.013 (0.006–0.021) | 0.002 | 0.014 (0.002–0.028) | 0.064 | 0.010 (0.003–0.020) | 0.010 |
| Finances -> PSS-4 | 0.018 (0.008–0.029) | 0.002 | 0.016 (0.002–0.032) | 0.068 | 0.020 (0.006–0.035) | 0.013 |
| SLS-12 -> Pandemic-ED | −0.165 (−0.198–−0.131) | <0.001 | −0.196 (−0.240–−0.151) | <0.001 | −0.126 (−0.172–−0.078) | <0.001 |
| SLS-12 -> PSS-4 | −0.236 (−0.270–−0.204) | <0.001 | −0.226 (−0.268–−0.183) | <0.001 | −0.242 (−0.292–−0.193) | <0.001 |
| Education -> PSS-4 | 0.015 (0.000–0.030) | 0.111 | 0.021 (0.000–0.042) | 0.096 | 0.024 (0.003–0.046) | 0.055 |
| ECR-RS -> PSS-4 | 0.086 (0.068–0.105) | <0.001 | 0.103 (0.078–0.135) | <0.001 | 0.061 (0.039–0.085) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kozakiewicz, A.; Izdebski, Z.; Białorudzki, M.; Mazur, J. Pandemic-Related Stress and Other Emotional Difficulties in a Sample of Men and Women Living in Romantic Relationships during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2023, 20, 2988. https://doi.org/10.3390/ijerph20042988
Kozakiewicz A, Izdebski Z, Białorudzki M, Mazur J. Pandemic-Related Stress and Other Emotional Difficulties in a Sample of Men and Women Living in Romantic Relationships during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2023; 20(4):2988. https://doi.org/10.3390/ijerph20042988
Chicago/Turabian StyleKozakiewicz, Alicja, Zbigniew Izdebski, Maciej Białorudzki, and Joanna Mazur. 2023. "Pandemic-Related Stress and Other Emotional Difficulties in a Sample of Men and Women Living in Romantic Relationships during the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 20, no. 4: 2988. https://doi.org/10.3390/ijerph20042988
APA StyleKozakiewicz, A., Izdebski, Z., Białorudzki, M., & Mazur, J. (2023). Pandemic-Related Stress and Other Emotional Difficulties in a Sample of Men and Women Living in Romantic Relationships during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health, 20(4), 2988. https://doi.org/10.3390/ijerph20042988