
Volumetric Assessment of Apical Periodontitis Using Cone-Beam Computed Tomography—A Systematic Review


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Selection Criteria
2.2. Exclusion Criteria
2.3. Search Strategies
2.4. Quality Assessment
3. Results
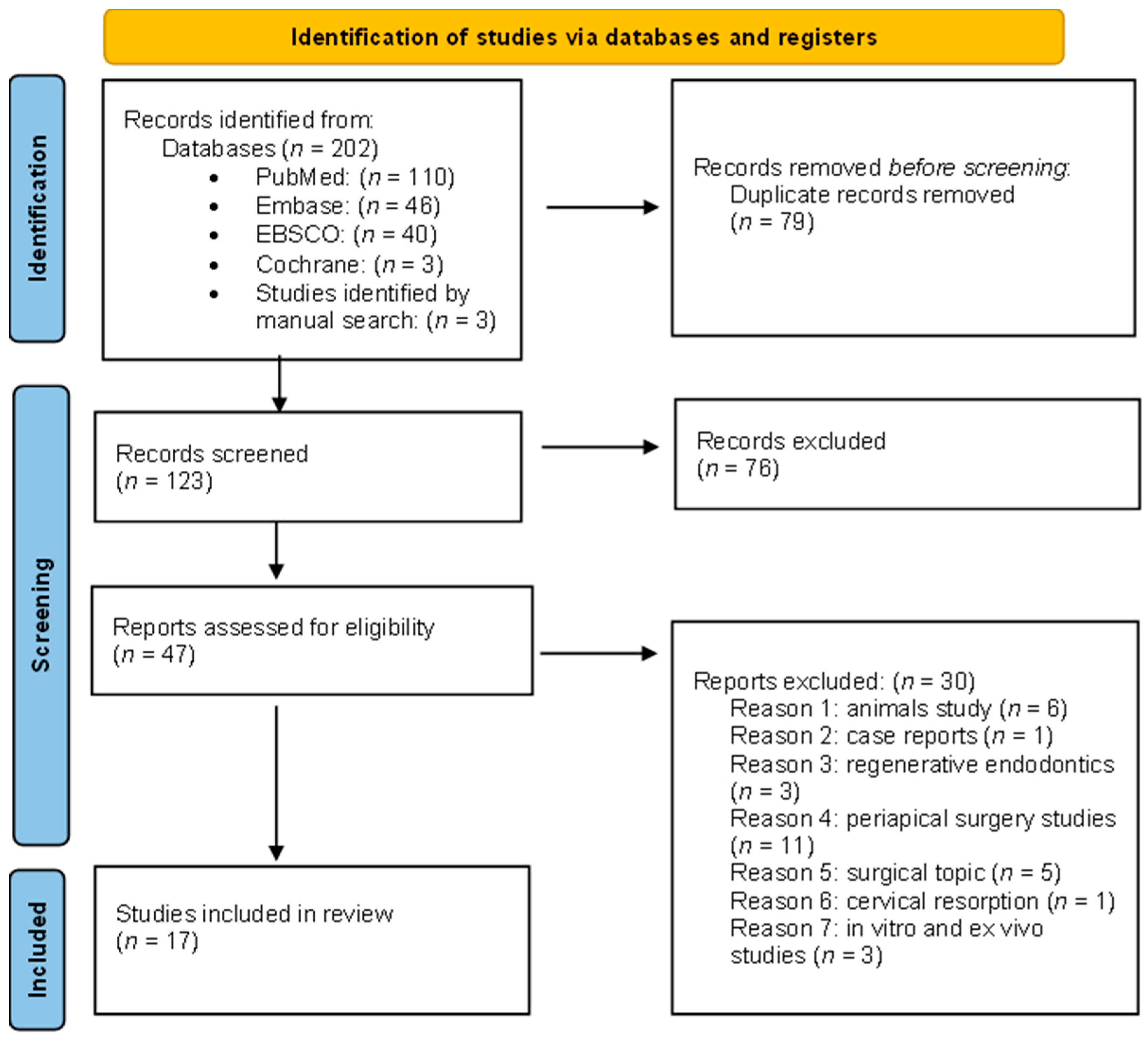
3.1. Study Selection
3.2. Study Characteristics
3.3. CBCT Parameters
3.4. Results of Individual Studies
3.5. Quality Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Graunaite, I.; Lodiene, G.; Maciulskiene, V. Pathogenesis of apical periodontitis: A literature review. J. Oral Maxillofac. Res. 2012, 2, e1. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.; Ha, S.W.; Kim, U.; Kim, S.; Kim, E. A one-year radiographic healing assessment after endodontic microsurgery using cone-beam computed tomographic scans. J. Clin. Med. 2020, 9, 3714. [Google Scholar] [CrossRef]
- Garcia-Font, M.; Abella, F.; Patel, S.; Rodríguez, M.; Sanchez, J.A.G.; Duran-Sindreu, F. Cone-beam computed tomographic analysis to detect the association between primary and secondary endodontic infections and mucosal thickness of maxillary sinus. J. Endod. 2020, 46, 1235–1240. [Google Scholar] [CrossRef]
- Dutra, K.; Haas, L.; Porporatti, A.; Flores-Mir, C.; Santos, J.N.; Mezzomo, L.A.; Corrêa, M.; Canto, G.D.L. Diagnostic accuracy of cone-beam computed tomography and conventional radiography on apical periodontitis: A systematic review and meta-analysis. J. Endod. 2016, 42, 356–364. [Google Scholar] [CrossRef]
- Aminoshariae, A.; Kulild, J.; Syed, A. Cone-beam computed tomography compared with intraoral radiographic lesions in endodontic outcome studies: A systematic review. J. Endod. 2018, 44, 1626–1631. [Google Scholar] [CrossRef]
- Patel, S.; Brown, J.; Pimentel, T.; Kelly, R.D.; Abella, F.; Duracket, C. Cone beam computed tomography in endodontics—A review of the literature. Int. Endod. J. 2019, 52, 1138–1152. [Google Scholar] [CrossRef] [PubMed]
- Antony, D.; Thomas, T.; Nivedhitha, M. Two-dimensional periapical, panoramic radiography versus three-dimensional cone-beam computed tomography in the detection of periapical lesion after endodontic treatment: A systematic review. Cureus 2020, 12, e7736. [Google Scholar] [CrossRef] [PubMed]
- Jakovljevic, A.; Nikolic, N.; Jacimovic, J.; Pavlovic, O.; Milicic, B.; Beljic-Ivanovic, K.; Miletic, M.; Andric, M.; Milasin, J. Prevalence of apical periodontitis and conventional nonsurgical root canal treatment in general adult population: An updated systematic review and meta-analysis of cross-sectional studies published between 2012 and 2020. J. Endod. 2020, 46, 1371–1386. [Google Scholar] [CrossRef]
- Ramis-Alario, A.; Soto-Penaloza, D.; Tarazona-Alvarez, B.; Peñarrocha-Diago, M.; Peñarrocha-Oltra, D. Comparison of the diagnostic efficacy of 2D radiography and cone beam computed tomography in persistent apical periodontal disease: A PRISMA-DTA systematic review and meta-analysis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2021, 132, e153–e168. [Google Scholar] [CrossRef]
- Liang, Y.H.; Jiang, L.M.; Jiang, L.; Chen, X.B.; Liu, Y.Y.; Tian, F.C.; Bao, X.D.; Gao, X.J.; Versluis, M.; Wu, M.K.; et al. Radiographic healing after a root canal treatment performed in single-rooted teeth with and without ultrasonic activation of the irrigant: A randomized controlled trial. J. Endod. 2013, 39, 1218–1225. [Google Scholar] [CrossRef]
- Metska, M.; Parsa, A.; Aartman, I.; Wesselink, P.R.; Ozoket, A.R. Volumetric changes in apical radiolucencies of endodontically treated teeth assessed by cone-beam computed tomography 1 year after orthograde retreatment. J. Endod. 2013, 39, 1504–1509. [Google Scholar] [CrossRef] [PubMed]
- Rizzi-Maia, C.; Maia-Filho, E.; Nelson-Filho, P.; Segato, R.A.; de Queiroz, A.M.; Paula-Silva, F.W.; da Silva Pereira, S.M.; Borges, A.H.; da Silva, L.A.B. Single vs two-session root canal treatment: A preliminary randomized clinical study using cone beam computed tomography. J. Contemp. Dent. Pract. 2016, 17, 515–521. [Google Scholar] [CrossRef]
- Filho, E.; Calisto, A.; Tavares, R.; de Castro Rizzi, C.; Segato, R.A.B.; da Silvaet, L.A.B. Correlation between the periapical index and lesion volume in cone-beam computed tomography images. Iran. Endod. J. 2018, 13, 155–158. [Google Scholar]
- Zhang, M.M.; Fang, G.F.; Chen, X.T.; Liang, Y.H. Four-year outcome of nonsurgical root canal retreatment using cone beam computed tomography: A prospective cohort study. J. Endod. 2021, 47, 382–390. [Google Scholar] [CrossRef]
- Borden, W.G.; Wang, X.; Wu, M.K.; Shemeshet, H. Area and 3-dimensional volumetric changes of periapical lesions after root canal treatments. J. Endod. 2013, 39, 1245–1249. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.M.; Liang, Y.H.; Gao, X.J.; Jiang, L.; van der Sluis, L.; Wu, M.-K. Management of apical periodontitis: Healing of post-treatment periapical lesions present 1 year after endodontic treatment. J. Endod. 2015, 41, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Jalali, P.; Tahmasabi, M.; Augsburger, R.; Khalilkhani, N.K.; Daghighi, K. Dynamics of bone loss in cases with acute or chronic apical abscess. J. Endod. 2019, 45, 1–5. [Google Scholar] [CrossRef]
- Boubaris, M.; Chan, K.L.; Zhao, W.; Cameron, A.; Sun, J.; Love, R.; George, R. A novel volume-based cone beam computed tomographic periapical index. J. Endod. 2021, 47, 1308–1313. [Google Scholar] [CrossRef]
- Boubaris, M.; Cameron, A.; Love, R.; George, R. Sphericity of Periapical Lesion and Its Relation to the Novel CBCT Periapical Volume Index. J. Endod. 2022, 48, 1395–1399. [Google Scholar] [CrossRef]
- Kamburoglu, K.; Yilmaz, F.; Gulsabi, K.; Gulen, O.; Gulsahiet, A. Change in periapical lesion and adjacent mucosal thickening dimensions one year after endodontic treatment: Volumetric cone beam computed tomography assessment. J. Endod. 2017, 43, 218–224. [Google Scholar] [CrossRef]
- Sönmez, G.; Kamburoglu, K.; Yilmaz, F.; Koç, C.; Barış, E.; Tüzüner, A. Versatility of high-resolution ultrasonography in the assessment of granulomas and radicular cysts: A comparative in vivo study. Dentomaxillofac. Radiol. 2019, 48, 20190082. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- The Joanna Briggs Institute. Reviewer’s Manual. 2014. Available online: https://joannabriggs.org/assets/docs/sumari/ReviewersManualMixed-Methods-Review-Methods-2014-ch1.pdf (accessed on 5 May 2018).
- Esposito, S.A.; Huybrechts, B.; Slagmolen, P.; Cotti, E.; Coucke, W.; Pauwels, R.; Lambrechts, P.; Jacobs, R. A novel method to estimate the volume of bone defects using cone-beam computed tomography: An in vitro study. J. Endod. 2013, 39, 1111–1115. [Google Scholar] [CrossRef] [PubMed]
- Ahlowalia, M.S.; Patel, S.; Anwar, H.M.S.; Cama, G.; Austin, R.S.; Wilson, R.; Mannocciet, F. Accuracy of CBCT for volumetric measurement of simulated periapical lesions. Int. Endod. J. 2013, 46, 538–546. [Google Scholar] [CrossRef] [PubMed]
- Zapata, R.O.; Bramante, C.M.; Duarte, M.H.; Ramos Fernandes, L.M.P.S.; Camargo, E.J.; de Moraes, I.G.; Bernardineli, N.; Vivan, R.R.; Capelozza, A.L.A.; Garcia, R.B. The influence of cone-beam computed tomography and periapical radiographic evaluation on the assessment of periapical bone destruction in dog’s teeth. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2011, 112, 272–279. [Google Scholar] [CrossRef]
- Kamburoğlu, K.; Çakmak, E.E.; Eratam, N.; Sönmez, G.; Karahanet, S. In vitro assessment of periapical lesions created in sheep mandibles by using high resolution ultrasonography and cone beam computed tomography. Dentomaxillofac. Radiol. 2021, 50, 20210048. [Google Scholar] [CrossRef]
- López, F.U.; Kopper, P.M.P.; Cucco, C.; Bona, A.D.; de Figueiredo, J.A.P.; Vier-Pelisseret, F.V. Accuracy of cone-beam computed tomography and periapical radiography in apical periodontitis diagnosis. J. Endod. 2014, 40, 2057–2060. [Google Scholar] [CrossRef] [PubMed]
- Paula-Silva, F.W.G.; Hassan, B.; Silva, L.A.B.; Leonardo, M.R.; Wu, M.K. Outcome of root canal treatment in dogs determined by periapical radiography and cone-beam computed tomography scans. J. Endod. 2009, 35, 723–726. [Google Scholar] [CrossRef]
- Villoria, E.M.; Lenzi, A.R.; Soares, R.V.; Souki, B.Q.; Sigurdsson, A.; Marques, A.P.; Fidel, S.R. Post-processing open-source software for the CBCT monitoring of periapical lesions healing following endodontic treatment: Technical report of two cases. Dentomaxillofac. Radiol. 2017, 46, 20160293. [Google Scholar] [CrossRef] [PubMed]
- Kateb, N.M.E.; Fata, M.M. Influence of periapical lesion size on healing outcome following regenerative endodontic procedures: A clinical investigation. Oral Radiol. 2022, 38, 480–489. [Google Scholar] [CrossRef]
- Sahib, A.M.; Al-Adili, S.S. Evaluation of healing process of periapical defect filled by platelet rich fibrin using cone beam computed tomography–comparative clinical study. Indian J. Public Health Res. Dev. 2019, 10, 448–453. [Google Scholar] [CrossRef]
- Cotti, E.; Esposito, S.; Jacobs, R.; Slagmolen, P.; Bakland, L.K. Comprehensive management of a complex traumatic dental injury. Dent. Traumatol. 2014, 30, 400–405. [Google Scholar] [CrossRef] [PubMed]
- Vallaeys, K.; Kacem, A.; Legoux, H.; Tenier, M.L.; Hamitouche, C.; Arbab-Chirani, R. 3D dento-maxillary osteolytic lesion and active contour segmentation pilot study in CBCT: Semi-automatic vs manual methods. Dentomaxillofac. Radiol. 2015, 44, 20150079. [Google Scholar] [CrossRef] [PubMed]
- Schloss, T.; Sonntag, D.; Kohli, M.R.; Setzer, F.C. A comparison of 2- and 3-dimensional healing assessment after endodontic surgery using cone-beam computed tomographic volumes or periapical radiographs. J. Endod. 2017, 43, 1072–1079. [Google Scholar] [CrossRef]
- Karan, N.B.; Aricioğlu, B. Assessment of bone healing after mineral trioxide aggregate and platelet-rich fibrin application in periapical lesions using cone-beam computed tomographic imaging. Clin. Oral Investig. 2020, 24, 1065–1072. [Google Scholar] [CrossRef]
- Pitcher, B.; Alaqla, A.; Noujeim, M.; Wealleans, J.A.; Kotsakis, G.; Chrepa, V. Binary decision trees for preoperative periapical cyst screening using cone-beam computed tomography. J. Endod. 2017, 43, 383–388. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Yang, G.; Ren, B.; Gao, Y.; Peng, X.; Li, M.; Xu, H.H.K.; Han, Q.; Li, J.; Zhou, X.; et al. Effect of antibacterial root canal sealer on persistent apical periodontitis. Antibiotics 2021, 10, 741. [Google Scholar] [CrossRef]
- Dhamija, R.; Tewari, S.; Sangwan, P.; Duhan, J.; Mittal, S. Impact of platelet-rich plasma in the healing of through-and-through periapical lesions using 2-dimensional and 3-dimensional evaluation: A randomized controlled trial. J. Endod. 2020, 46, 1167–1184. [Google Scholar] [CrossRef]
- Kim, D.; Ku, H.; Nam, T.; Yoon, T.C.; Lee, C.Y.; Kim, E. Influence of size and volume of periapical lesions on the outcome of endodontic microsurgery: 3-dimensional analysis using cone-beam computed tomography. J. Endod. 2016, 42, 1196–1201. [Google Scholar] [CrossRef]
- Tanomaru-Filho, M.; Jorge, E.G.; Guerreiro-Tanomaru, J.M.; Reis, J.M.S.; Spin-Neto, R.; Gonçalves, M. Two- and tridimensional analysis of periapical repair after endodontic surgery. Clin. Oral Investig. 2015, 19, 17–25. [Google Scholar] [CrossRef] [PubMed]
- Kauke, M.; Safi, A.F.; Grandoch, A.; Nickenig, H.J.; Zöller, J.; Kreppel, M. Volumetric analysis of keratocystic odontogenic tumors and non-neoplastic jaw cysts—Comparison and its clinical relevance. J. Craniomaxillofac. Surg. 2018, 46, 257–263. [Google Scholar] [CrossRef] [PubMed]
- Ramis-Alario, A.; Tarazona-Álvarez, B.; Peñarrocha-Diago, M.; Soto-Peñaloza, D.; Peñarrocha-Diago, M.; Peñarrocha-Oltra, D. Is periapical surgery follow-up with only two-dimensional radiographs reliable? A retrospective cohort type sensitivity study. Med. Oral Patol. Oral Cir. Bucal. 2021, 26, e711–e718. [Google Scholar] [CrossRef]
- Hung, K.; Hui, L.; Yeung, A.W.K.; Wu, Y.; Hsung, R.T.C.; Bornstein, M.M. Volumetric analysis of mucous retention cysts in the maxillary sinus: A retrospective study using cone-beam computed tomography. Imaging Sci. Dent. 2021, 51, 117–127. [Google Scholar] [CrossRef]
- Tiwari, U.O.; Chandra, R.; Tripathi, S.; Jain, J.; Jaiswal, S.; Tiwari, R.K. Comparative analysis of platelet-rich fibrin, platelet-rich fibrin with hydroxyapatite and platelet-rich fibrin with alendronate in bone regeneration: A cone-beam computed tomography analysis. J. Conserv. Dent. 2020, 23, 348–353. [Google Scholar]
- Parmar, P.D.; Dhamija, R.; Tewari, S.; Sangwan, P.; Gupta, A.; Duhan, J.; Mittal, S. 2D and 3D radiographic outcome assessment of the effect of guided tissue regeneration using resorbable collagen membrane in the healing of through-and-through periapical lesions—A randomized controlled trial. Int. Endod. J. 2019, 52, 935–948. [Google Scholar] [CrossRef]
- Ahmedm, G.M.; Nageh, M.; El-Baz, A.A.; Saif, N. CBCT volumetric evaluation of bone healing after endodontic microsurgery using platelet-rich fibrin (PRF). Endod. Pract. Today 2018, 12, 241–248. [Google Scholar]
- Sureshbabu, N.M.; Ranganath, A.; Jacob, B. Concentrated growth factor—Surgical management of large periapical lesion using a novel platelet concentrate in combination with bone graft. Ann. Maxillofac. Surg. 2020, 10, 246–250. [Google Scholar] [PubMed]
- Matny, L.E.; Ruparel, N.B.; Levin, M.D.; Noujeim, A.; Diogenes, A. A volumetric assessment of external cervical resorption cases and its correlation to classification, treatment planning, and expected prognosis. J. Endod. 2020, 46, 1052–1058. [Google Scholar] [CrossRef] [PubMed]
- Liang, Y.H.; Jiang, L.; Gao, X.J.; Wesselink, M.W. Detection and measurement of artificial periapical lesions by cone-beam computed tomography. Int. Endod. J. 2014, 47, 332–338. [Google Scholar] [CrossRef] [PubMed]
- Komatsu, K.; Abe, Y.; Yoshioka, T.; Ishimura, H.; Ebihara, A.; Suda, H. Differential diagnosis of vertical root fractures using reconstructed three-dimensional models of bone defects. Dentomaxillofac. Radiol. 2014, 43, 20140256. [Google Scholar] [CrossRef]
- Trindade, J.L.; Liedke, G.S.; Tibúrcio-Machado, C.D.S.; Barcelos, R.C.S.; Dotto, G.N.; Bier, C.A.S. Low-dose multidetector computed tomographic and cone-beam computed tomographic protocols for volumetric measurement of simulated periapical lesions. J. Endod. 2021, 47, 1144–1148. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, F.; Ferreira, N.; Martinho, F.; Nascimento, G.G.; Manhães, L.R.C., Jr.; Rocco, M.A.; Carvalho, C.A.T.; Valera, A.C. Correlation between volume of apical periodontitis determined by cone-beam computed tomography analysis and endotoxin levels found in primary root canal infection. J. Endod. 2015, 41, 1015–1019. [Google Scholar] [CrossRef] [PubMed]
- Aoki, E.; Abdala-Junior, R.; Oliveira, J.; Arita, E.S.; Cortes, A.R.G. Reliability and reproducibility of manual and automated volumetric measurements of periapical lesions. J. Endod. 2015, 41, 1–5. [Google Scholar] [CrossRef]
- Machut, K.; Zółtowska, A. Plasma Rich in Growth Factors in the Treatment of Endodontic Periapical Lesions in Adult Patients: 3-Dimensional Analysis Using Cone-Beam Computed Tomography on the Outcomes of Non-Surgical Endodontic Treatment Using A-PRF+ and Calcium Hydroxide: A Retrospective Cohort Study. J. Clin. Med. 2022, 11, 6092. [Google Scholar]
- Toia, C.C.; Khoury, R.D.; Corazza, B.J.M.; Orozco, E.I.F.; Valera, M.C. Effectiveness of 1-Visit and 2-Visit Endodontic Retreatment of Teeth with Persistent/Secondary Endodontic Infection: A Randomized Clinical Trial with 18 Months of Follow-up. J. Endod. 2022, 48, 4–14. [Google Scholar] [CrossRef]
- Lofthag-Hansen, S.; Huumonen, S.; Gröndahl, K.; Gröndahl, H.-G. Limited cone-beam CT and intraoral radiography for the diagnosis of periapical pathology. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2007, 103, 114–119. [Google Scholar] [CrossRef] [PubMed]
- Patel, S. New dimensions in endodontic imaging: Part 2.Cone beam computed tomography. Int. Endod. J. 2009, 42, 463–475. [Google Scholar] [CrossRef] [PubMed]
- Cotton, T.; Geisler, T.M.; Holden, D.T.; Schwartz, S.A.; Schindler, W.G. Endodontic applications of cone-beam volumetric tomography. J. Endod. 2007, 33, 1121–1132. [Google Scholar] [CrossRef]
- Patel, S.; Dawood, A.; Whaites, E.; Ford, T.P. New dimensions in endodontic imaging: Part 1.Conventional and alternative radiographic systems. Int. Endod. J. 2009, 42, 447–462. [Google Scholar] [CrossRef]
- Orstavik, D.; Kerekes, K.; Eriksen, H.M. The periapical index: A scoring system for radiographic assessment of apical periodontitis. Endod. Dent. Traumatol. 1986, 2, 20–34. [Google Scholar] [CrossRef]
- Venskutonis, T.; Plotino, G.; Tocci, L.; Gambarini, G.; Maminskas, J.; Juodzbalys, G. Periapical and endodontic status scale based on periapical bone lesions and endodontic treatment quality evaluation using cone-beam computed tomography. J. Endod. 2015, 41, 190–196. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Database (n) | Search Strategy |
|---|---|
| PubMED (n = 110) | (Cone-Beam Computed Tomography[Mesh] OR cone-beam OR CBCT) AND (Periapical Periodontitis[Mesh] OR periapical) AND volume |
| Embase (n = 46) | (‘tooth periapical disease’/exp OR ‘tooth periapical disease’) AND (‘cone beam computed tomography’/exp OR ‘cone beam computed tomography’) AND (‘volume’/exp OR ‘volume’) |
| EBSCO Dentistry and Oral Sciences Source (n = 40) | periapical lesion AND cone beam computed tomography AND volume |
| Cochrane (n = 3) | ‘‘periapical periodontitis” in Title Abstract Keyword AND “cone beam computed tomography” in Title Abstract Keyword AND “volume” in Title Abstract Keyword-(Word variations have been searched) |
| Authors, Year, Country | Materials | Treatment | Purpose | ||||
|---|---|---|---|---|---|---|---|
| Patricipants | Teeth | Target Condition | |||||
| Amount | Sex | Age (Years) | |||||
| Borden et al. [15] 2013 The Netherlands | 42 | 32 F, 10 M | 21–78 | 50 (9 anterior, 6 premolars, 35 molars) | Preoperative periapical radiolucency on both PA and CBCT scans | Single visit, crown down technique, lateral compaction and later warm vertical compaction techniques | The aim of this study was to measure the changes in lesion size after root canal treatments with PA and CBCT imaging and to assess the outcome based on these parameters. |
| Liang et al. [10] 2013 China | 105 | - | 18–76 | 105 (incisors, canines, premolars) | Periapical lesions with radiographic evidence of bone loss | Single visit, crown down technique and warm vertical compaction filling | The aim of this study was to compare the outcome of a root canal treatment with and without additional ultrasonic activation of the irrigant. |
| Metska et al. [11] 2013 The Netherlands | 37 | 12 F, 10 M | 20–70 | 45 | Apical periodontitis after completed endodontic treatment | Reendodontic treatment and lateral or warm vertical condensation | Assess by CBCT scans the volumetric changes of periapical radiolucencies in endodontically treated teeth 1 year after orthograde retreatment. |
| Cardoso et al. [53] 2015 Brazil | 24 | - | 22–45 | 24 | Teeth with primary endodontic infection, absence of periodontal pockets deeper than 4 mm | - | This clinical study was conducted to correlate the levels of endotoxins and bacterial counts found in primary endodontic infection with the volume of periapical bone destruction determined by CBCT analysis. |
| Zhang et al. [16] 2015 China | 130 | - | - | 162 | Periapical lesions 12 months after RCT | Crown down technique and warm vertical condensation | Assesses second-year volumetric changes in post-treatment periapical radiolucencies detected 1 year after treatment. |
| Aoki et al. [54] 2015 Brazil | 43 | 29 F, 14 M | average age 54.6 ± 8.5 | - | Periapical lesion after endodontic diseases | - | To test the reliability and reproducibility of 2 methods: manual and automated segmentation (using a threshold-based region growing algorithm) for measuring the volume of periapical lesions. |
| Rizzi-Maia et al. [12] 2016 Brazil | 13 | 9 F, 4 M | 18–58 | 26 (21 incisors, 1 canine, 4 premolars) | Teeth with pulp necrosis and visible periapical lesion | Single session: lateral condensationTwo sessions: Ca(OH)2 and then filled with lateral condensation | To compare root canal treatment of teeth with AP in a single or two visits, using CBCT. |
| Kamburoglu et al. [20] 2017Turkey | 21 | 14 F, 7 M | 18–52 | 21 (molars) | Periapical lesions with mucosal thickening more or equally 2 mm | Two sessions with Ca(OH)2 dressing and single cone gutta percha technique | To obtain linear and volumetric measurements of lesion dimensions in maxillary first molars with periapical pathology and to measure maxillary sinus mucosal thickening in the vicinity of periapical lesions before and 1 year after endodontic treatment by using CBCT. |
| Filho et al. [13] 2018 Brazil | 21 | - | average age 36.67 ± 11.21 | 35 (30 incisors, 2 canines, 3 premolars) | Pulp necrosis and radiographically visible chronic apical periodontitis | - | The study aimed to correlate the Periapical Index, obtained by way of periapical radiographs, with the volume of chronic periapical lesion, obtained through CBCT, in the permanent teeth. |
| Jalali et al. [17] 2019 USA | 48 | 22 F, 26 M | older than 18 | 48 | Acute or chronic apical abscesses | - | Evaluate the size and pattern of bone loss in patients with acute apical abscess and chronic apical abscess using CBCT images. |
| Sönmez et al. [21] 2019 Turkey | 33 | 23 F, 10 M | 18–62 | 33 (19 incisors, 1 canine, 10 premolars, 3 molars) | Periapical lesions which had been determined as granulomas or periapical cysts | Two sessions with Ca(OH)2 dressing and single cone gutta percha technique | To evaluate and compare the diagnostic potential of high-resolution ultrasound with periapical radiographs (PR) and CBCT in assessing granulomas and radicular cysts. |
| Garcia-Font et al. [3] 2020 UK | - | - | 18–79 | 131 (16 premolars, 115 molars) | Periapical lesions of primary and secondary endodontic lesions | Primary and secondary endodontic infections | CBCT was used to evaluate the differences in the mucosal thickness of the Schneiderian membrane in primary and secondary endodontic lesions. |
| Zhang et al. [14] 2020 China | 80 | 68 F, 29 M | ≤45 and >45 | 97 (46 anterior, 22 premolars, 29 molars) | Teeth, which had to undergo nonsurgical root treatment | Reendodontic treatment, crown down technique, single visit and vertical warm gutta percha technique | To investigate the 4-year outcome and prognostic factors of nonsurgical root canal retreatment determined by measuring the volumetric change of periapical radiolucencies on CBCT scans. |
| Boubaris et al. [18] 2021 Australia | 91 | 52 F, 39 M | average age 55 ± 5.15 | 273 roots (44 incisors, 19 canines, 62 premolars, 148 molars) | Periapical lesion after endodontic diseases | - | To evaluate the variations in the volume of periapical lesions scored using a cone-beam computed tomographic periapical index (CBCTPAI) and to develop a new volume-based periapical index. |
| Boubaris et al. [19] 2022 Australia | 113 | 66 F, 47 M | mean age 56 | 261 roots (53 incisors, 15 canines, 48 premolars, 145 molars | Teeth with periapical radiolucency. | - | The aim of this study was to assess the sphericity of periapical radiolucent lesions and its relation to the CBCTPAVI. |
| Machut et al. [55] 2022 Poland | 36 (3 patients into both groups) | 10 F, 9 M (study group); 9 F, 10 M (control group) | average age Study group: 33.7 Control group: 30.0 | 40 Study group (11 incisors, 3 canines, 4 premolars, 2 molars). Control group (9 incisors, 2 canines, 6 premolars, 3 molars) | Apical periodontitis | Modified crown-down technique. Application of A-PRF below thecemento-dentinal junction. Final obturation by the thermoplastic method with calibrated gutta-percha cone and AH-plus sealer. | The aim of this study is to compare six-month follow-ups of periapical lesion healing after one-visit RCT with A-PRF+ application vs. two-visit RCT with inter-appointment calcium hydroxide dressings. |
| Toia et al. [56] 2022 Brazil | 40 | 12 F, 28 M | 12–60 | 40 (29 incisors, 2 canines, 9 premolars) | Posttreatment apical periodontitis | One or two visit root canal treatments. Crown down technique in both groups. Two visit treatment: Ca(OH)2 for 14 days. Single cone technique in both groups. | The aim of this study was to compare the endodontic retreatment of root-filled teeth with PTAP performed in 1 visit vs. 2 visits on the reduction of microbial load. |
| Analysis CBCT | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Authors | Apparatus | Apparatus Parameters | Programme | ||||||
| Voltage (kVp) | Current (mA) | Field of View (cm) | Voxel Size (mm3) | Slice Dimensions (pixels) | Thickness of the Cut Layer (mm) | Segmentation Method | |||
| Borden et al. [15] 2013 | Gendex CB-500; KaVo Dental GmbH, Biberach, Germany | 120 | 5 | - | - | - | 0.125–0.2 | Semiautomatic | Amira Software v.5.4.3 |
| Liang et al. [10] 2013 | 3DX-Accuitomo CBCT scanner (J. Morita Mfg Corp, Kyoto, Japan) | 80 | 4 to 5 | 4 × 4 | - | - | - | Semiautomatic | Amira Software v.5.4.3 |
| Metska et al. [11] 2013 | Pre op: NewTom 3G (QR SLR, Verona, Italy) Post op: NewTom 5G | 1. Pre op: 110 2. Post op:110 | 1.Pre op: 3.90–5.6 2. Post op: 3.76–6.43 | 1. Pre op: 9 inch 2. Post op: 8 × 8 | - | - | - | Semiautomatic | AMIRA software v.5.3.4 |
| Cardoso et al. [53] 2015 | I-CAT Next Generation (Imaging Science International, Hatfield, PA, USA) | - | - | 8 × 8 | 0.2 | - | 0.2 | Automatic | NEMOTEC software |
| Zhang et al. [16] 2015 | 3DX-Accuitomo scanner (JMorita Mfg Corp, Kyoto, Japan) | 80 | 4–5 | 4 × 4 | - | - | - | Manual | Amira software v. 5.4.3 |
| Aoki et al. [54] 2015 | I-CAT Classic (Image Sciences International, Hatfield, PA, USA) | 120 | 8 | 16 × 6 | 0.25 | - | - | Manual: 120 s Automatic: 50 s | OsiriX ImplantViewer 3.006 |
| Rizzi-Maia et al. [12] 2016 | I-CAT Next Generation device (Imaging Sciences International, Hatfield, PA, USA) | - | - | 8 × 8 | 0.2 | - | 0.2 | Automatic | Amira software v.5.3.3 |
| Kamburoglu et al. [20] 2017 | Kodak CS 9300 3D (Carestream Health Co, Rochester, NY, USA) | 80 | 8 | - | 0.09 | - | - | Manual | 3D Doctor |
| Filho et al. [13] 2018 | Next Generation I-CAT (Imaging Sciences International, Hatfield, PA, USA) | - | - | 8 × 8 | 0.2 | - | 0.2 | Automatic | Amira software v.5.3.3 |
| Jalali et al. [17] 2019 | CS 9300 device (Carestream Health, Rochester, NY, USA) | 60–90 kV | 2–15 | - | 0.09 | - | - | Automatic | Mimics Innovation Suite Version 19 software |
| Sönmez et al. [21] 2019 | Planmeca Promax 3D max CBCT unit (Planmeca, Helsinki, Finland) | 90 | 7 | 55 × 50 mm | 0.1 | - | - | Manual | 3D- Doctor |
| Garcia-Font et al. [3] 2020 | ProMax 3Ds (Planmeca OY, Helsinki, Finland) | 84 kV | 8.0 | 19–24 micro SV | 0.2 | - | 0.2 | - | Planmeca Romexis Viewer |
| Zhang et al. [14] 2020 | - | - | - | - | - | - | - | Manual | Amira software v. 5.4.3 |
| Boubaris et al. [18] 2021 | - | - | - | - | - | - | - | Semiautomatic | Mimics Research v.21.0.0.406 |
| Boubaris et al. [19] 2022 | Carestream CS9600 CBCT Scanner; Carestream Dental LLC, Atlanta, GA, USA) | - | - | - | - | - | - | Semiautomatic | Mimics Research v.21.0.0.406 |
| Machut et al. [55] 2022 | CS 3D Imaging v3.5.18 Software (Carestream Health Inc., Trophy, Croissy-Beaubourg, France) | - | - | - | - | - | - | - | ITK-SNAP |
| Toia et al. [56] 2022 Brazil | I-cat CBCT (Next Generation; Imaging Science International, Hatfield, PA, USA) | 120 | 36.15 | 16 × 13 | 0.25 | - | - | Semiautomatic | ITK-SNAP v. 3.8.0 software (Cognitica, Philadelphia, PA, USA) |
| Authors | Preoperative Volume (mm3) | Time of Postoperative Volume Measurement | Postoperative Volume (mm3) | Conclusion | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Borden et al. [15] 2013 | 1.0–281.5 | 10–37 months | - | Lesion changes after root canal treatments determined with 3D volumetric CBCT data and two-dimensional PA data were different, and, thus, the outcome determined with PA could be untrue. | ||||||
| Liang et al. [10] 2013 | 1.5–375.4 | 10–19 months | 0.00–176.20 | Root canal treatments with and without additional ultrasonic activation of the irrigant equally contributed to periapical healing and resulted in a high percentage of absence and reduced lesions, which is seen on outcomes of volumetric measurements. | ||||||
| Median volume of the lesion in the ultrasonic group: 26.6 | - | |||||||||
| Median volume of the lesion in the syringe group: 31.8 | - | |||||||||
| Metska et al. [11] 2013 | 2.26–998.58 | 1 year | 0.00–1215.14 | The volumetric measurements revealed a reduction of the size of periapical radiolucencies in more than half of the teeth 1 year after orthograde retreatment. | ||||||
| Aoki et al. [54] 2015 | Lack of precise data | - | - | Automated segmentation with a region growing algorithm is faster and slightly more reliable to calculate the volume of periapical lesions. | ||||||
| Cardoso et al. [53] 2015 | 100 | - | - | Findings revealed that the levels of endotoxins found in root canal infection are related to the volume of periapical bone destruction determined by CBCT analysis. | ||||||
| Zhang et al. [16] 2015 | 2.6–339.7 | 1 year | 0.8–174.6 | The volumes of post-treatment periapical radiolucencies detected 1 year after treatment in 63% of these teeth showed significant decreases in size during the second year, including complete resolution of the radiolucency in 13 teeth (22%). Thus, the healing of apical periodontitis is a dynamic process that takes time. | ||||||
| 2 years | 0.00–248.0 | |||||||||
| Rizzi-Maia et al. [12] 2016 | One session treatment 73.47 (11.119–182.48) | 1 year | 27.73 (1.07–101.16) | Cone beam-computed tomography imaging made 12 months posttreatment did not show complete repair in any of the teeth, based on the volumetric assessment of the lesion, suggesting that this follow-up period is not sufficient for the occurrence of complete lesion regression. | ||||||
| Two session treatment 65.94 (8.27–238.01) | 12.84 (0.11–29.53) | |||||||||
| Kamburoglu et al. [20] 2017 | 74.95 | 1 year | 19.38 | Within the limitations of this study, we found a significant reduction in periapical lesion width, lesion height, surface area, and volume in maxillary molar teeth, along with adjacent sinus mucosal thickening by using CBCT and specific software 1 year after endodontic treatment. | ||||||
| Mucosal thickening: 5.7 mm | 2 mm | |||||||||
| Jalali et al. [17] 2019 | AAA: 109 | - | - | Cortical fenestration is fundamental for the development of CAA. However, periradicular lesions without evident cortical fenestration can still cause AAA and fascial space involvement. | ||||||
| CCA: 233 | ||||||||||
| Sönmez et al. [21] 2019 | Using ultrasound 394.85 | 6 months | 112.22 | Although lesion depth, surface area, and volume are underestimated, in which CBCT is more accurate, lesion width and pathology as well as treatment outcomes are accurately assessed using ultrasound. | ||||||
| Using CBCT 736.32 | not measured | |||||||||
| Garcia-Font et al. [3] 2020 | Primary infection: lesion volume: 0.05 cm3, mucosal thickness: coronal view 5.41 | - | - | Secondary endodontic infections showed a more increased volume than that in primary endodontic infections. Furthermore, a significant association was noted between the volume and membrane thickness, revealing a greater volume increase in the thickness of the membrane in the primary and secondary infections in 2 planes. | ||||||
| Secondary infection: lesion volume 0.12 cm3; mucosal thickness: coronal view 3.4 | - | - | ||||||||
| Zhang et al. [14] 2020 | 0.7–451.5 | 4 years | 0.00–30.6 | The 4-year outcome of endodontic retreatment was predictable, with a significant volumetric reduction in periapical radiolucencies. | ||||||
| Machut et al. [55] 2022 | - | 6 months | - | The results of 3D radiographic healing assessments of RCT using modified criteria were different from those based on CBCT-PAI criteria. In the 6-month follow-up, CBCT scans showed a better healing tendency in patients in the study group than in the control group. The volumes of apical radiolucency were, on average, reduced by 85.93% in the study group and by 72.31% in the control group. | ||||||
| Toia et al. [56] 2022 | One visit treatment: 54 (10–375) Two visits treatment: 60 (30–470) | 18 months | One visit treatment: 10 (0–30) Two visits treatment: 5.5 (1–48) | In conclusion, 18 months after endodontic retreatment of root-filled teeth with PTAP, no significant differences were observed in the reduction of periapical lesion volume between teeth treated in 1 visit and those treated in 2 visits using Ca(OH)2 for 14 days. Even with the remaining content of LPS and LTA bacteria, it was possible to observe a significant reduction in the volume of periapical lesions in both groups after 18 months of treatment. | ||||||
| Volume (mm3) | Total | |||||||||
| PAI 0 | PAI 1 | PAI 2 | PAI 3 | PAI 4 | PAI 5 | PAI 6 | ||||
| Filho et al. [13] 2018 | - | - | 36.42 | 55.83 | 76.1 | 143.78 | - | 70.72 | Radiographic evaluation of periapical lesions must be carried out with caution, as it may not reflect the lesion’s volumetric characteristics. | |
| CBCTPAVI 0 | CBCTPAVI 1 | CBCTPAVI 2 | CBCTPAVI 3 | CBCTPAVI 4 | CBCTPAVI 5 | CBCTPAVI 6 | ||||
| Boubaris et al. [18] 2021 | 0 | 0.01–0.2 | 0.21–0.7 | 0.71–8.00 | 8.01–70.00 | 70.01–100.00 | 100.01+ | - | The method described in this article is a valid option for scientific inquiry, thus the continuing development of existing imaging software will allow for automation of the extraction of volume data from cone-beam images. | |
| Sphericity | ||||||||||
| CBCTPAVI 0 | CBCTPAVI 1 | CBCTPAVI 2 | CBCTPAVI 3 | CBCTPAVI 4 | CBCTPAVI 5 | CBCTPAVI 6 | ||||
| Boubaris et al. [19] 2022 | 85.7% | 85.7% | 89.1% | 80.4% | 77.8% | 77.8% | 59.6% | Periapical lesions of endodontic origin are mostly semi-spherical (51–78%) in their spread, and as CBCTPAVI score increases, sphericity decreases, indicating that larger lesions expand less uniformly compared with smaller lesions. Clinicians should be aware that lesions of increased volume have less sphericity, and are thus elongated or stretched in 1 or more anatomic plane. | ||
| Borden et al. (2013) Netherlands [15] | Liang et al. (2013) China [10] | Metska et al. (2013) Netherlands [11] | Cardoso et al. (2015) Brazil [53] | Zhang et al. (2015) China [16] | Aoki et al. (2015) Brazil [54] | Rizzi-Maia et al. (2016) Brazil [12] | Kamburoglu et al. (2017) Turkey [20] | Filho et al. (2018) Brazil [13] | Jalali et al. (2019) USA [17] | Sönmez et al. (2019) Turkey [21] | Garcia-Font et al. (2020) United Kingdom [3] | Zhang et al. (2020) China [14] | Boubaris et al. (2021) Australia [18] | Boubaris et al. (2022) Australia [19] | Machut et al. (2022) Poland [55] | Toia et al. (2022) Brazil [56] | |
| - | + | - | - | - | - | + | - | - | - | - | - | - | - | - | - | + | Random or pseudorandom sample |
| + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | Clear inclusion criteria |
| - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | Confounding factors |
| + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | Objective criteria |
| + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | Description of comparisons |
| + | + | + | - | + | - | + | - | - | - | - | - | + | - | - | + | + | Follow up in sufficient time |
| - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | Withdrewed patients |
| + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | Outcomes measurments |
| + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | Statistical analysis |
| 6/9 | 7/9 | 6/9 | 5/9 | 6/9 | 5/9 | 7/9 | 5/9 | 5/9 | 5/9 | 5/9 | 5/9 | 6/9 | 5/9 | 5/9 | 6/9 | 7/9 | YES |
| M | L | M | M | M | M | L | M | M | M | M | M | M | M | M | M | L | Risk of bias |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mackiewicz, E.; Bonsmann, T.; Kaczor-Wiankowska, K.; Nowicka, A. Volumetric Assessment of Apical Periodontitis Using Cone-Beam Computed Tomography—A Systematic Review. Int. J. Environ. Res. Public Health 2023, 20, 2940. https://doi.org/10.3390/ijerph20042940
Mackiewicz E, Bonsmann T, Kaczor-Wiankowska K, Nowicka A. Volumetric Assessment of Apical Periodontitis Using Cone-Beam Computed Tomography—A Systematic Review. International Journal of Environmental Research and Public Health. 2023; 20(4):2940. https://doi.org/10.3390/ijerph20042940
Chicago/Turabian StyleMackiewicz, Ewa, Tobias Bonsmann, Kinga Kaczor-Wiankowska, and Alicja Nowicka. 2023. "Volumetric Assessment of Apical Periodontitis Using Cone-Beam Computed Tomography—A Systematic Review" International Journal of Environmental Research and Public Health 20, no. 4: 2940. https://doi.org/10.3390/ijerph20042940
APA StyleMackiewicz, E., Bonsmann, T., Kaczor-Wiankowska, K., & Nowicka, A. (2023). Volumetric Assessment of Apical Periodontitis Using Cone-Beam Computed Tomography—A Systematic Review. International Journal of Environmental Research and Public Health, 20(4), 2940. https://doi.org/10.3390/ijerph20042940