
Which Specific Exercise Models Are Most Effective on Global Cognition in Patients with Cognitive Impairment? A Network Meta-Analysis
Abstract
1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria and Study Selection
2.2. Search Strategy
2.3. Data Extraction
2.4. Risk of Bias of Individual Studies
2.5. Data Analysis
3. Results
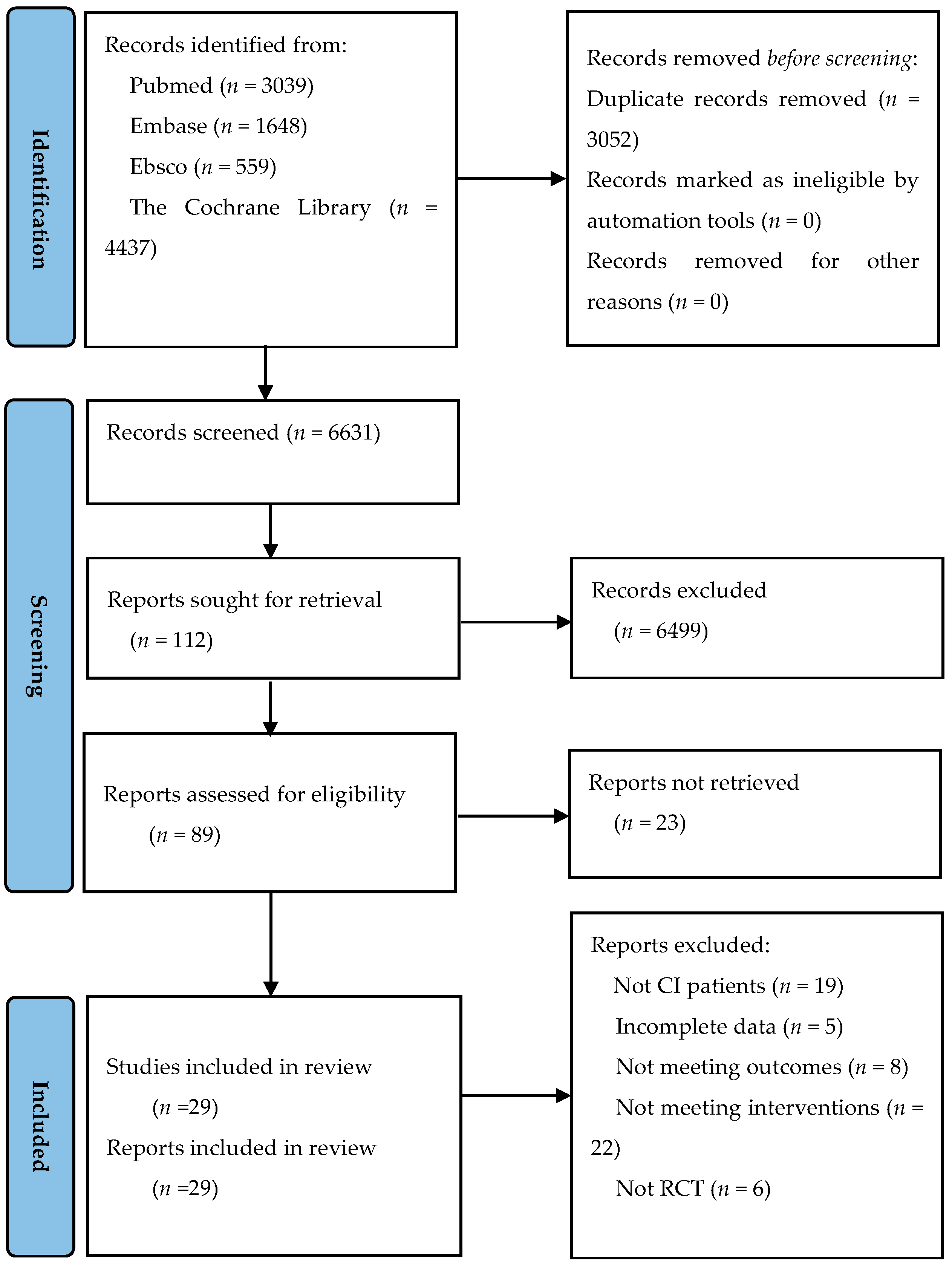
3.1. Literature Selection
3.2. Characteristics of the Included RCTs
3.3. Network Meta-Analysis
3.3.1. Exercise Type
3.3.2. Exercise Time
3.3.3. Exercise Intensity
3.3.4. Exercise Frequency
3.4. Publication Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gauthier, S.; Reisberg, B.; Zaudig, M.; Petersen, R.C.; Ritchie, K.; Broich, K.; Belleville, S.; Brodaty, H.; Bennett, D.; Chertkow, H.; et al. Mild cognitive impairment. Lancet 2006, 367, 1262–1270. [Google Scholar] [CrossRef]
- Keefe, R.S. Should cognitive impairment be included in the diagnostic criteria for schizophrenia? World Psychiatry 2008, 7, 22–28. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Risk Reduction of Cognitive Decline and Dementia; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Ballard, C.; Gauthier, S.; Corbett, A.; Brayne, C.; Aarsland, D.; Jones, E. Alzheimer’s disease. Lancet 2011, 377, 1019–1031. [Google Scholar] [PubMed]
- Petersen, R.C. Mild Cognitive Impairment. N. Engl. J. Med. 2011, 364, 2227–2234. [Google Scholar] [CrossRef] [PubMed]
- Petersen, R.C.; Lopez, O.; Armstrong, M.J.; Getchius, T.S.D.; Ganguli, M.; Gloss, D.; Gronseth, G.S.; Marson, D.; Pringsheim, T.; Day, G.S.; et al. Practice guideline update summary: Mild cognitive impairment: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology. Neurology 2018, 90, 126–135. [Google Scholar] [CrossRef] [PubMed]
- Manly, J.J.; Tang, M.X.; Schupf, N.; Stern, Y.; Vonsattel, J.P.; Mayeux, R. Frequency and course of mild cognitive impairment in a multiethnic community. Ann. Neurol. 2008, 63, 494–506. [Google Scholar]
- Battle, C.E.; Abdul-Rahim, A.H.; Shenkin, S.D.; Hewitt, J.; Quinn, T.J. Cholinesterase inhibitors for vascular dementia and other vascular cognitive impairments: A network meta-analysis. Cochrane Database Syst. Rev. 2021, 2, Cd013306. [Google Scholar] [CrossRef]
- Birks, J.S.; Harvey, R.J. Donepezil for dementia due to Alzheimer’s disease. Cochrane Database Syst. Rev. 2018, 6, Cd001190. [Google Scholar] [PubMed]
- Young, J.; Angevaren, M.; Rusted, J.; Tabet, N. Aerobic exercise to improve cognitive function in older people without known cognitive impairment (Review). Cochrane Collab. 2015, 22, CD005381. [Google Scholar] [CrossRef]
- Panza, G.A.; Taylor, B.A.; MacDonald, H.V.; Johnson, B.T.; Zaleski, A.L.; Livingston, J.; Thompson, P.D.; Pescatello, L.S. Can exercise improve cognitive symptoms of Alzheimer’s Disease? J. Am. Geriatr. Soc. 2018, 66, 487–495. [Google Scholar] [CrossRef] [PubMed]
- Northey, J.M.; Cherbuin, N.; Pumpa, K.L.; Smee, D.J.; Rattray, B. Exercise interventions for cognitive function in adults older than 50: A systematic review with meta-analysis. Br. J. Sport Med. 2018, 52, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Yin, H.; Wang, X.; Jia, Y.; Wang, C.; Wang, L.; Chen, L. Efficacy of different types of exercises on global cognition in adults with mild cognitive impairment: A network meta-analysis. Aging Clin. Exp. Res. 2019, 31, 1391–1400. [Google Scholar] [CrossRef]
- Hutton, B.; Salanti, G.; Caldwell, D.M.; Chaimani, A.; Schmid, C.H.; Cameron, C.; Ioannidis, J.P.; Straus, S.; Thorlund, K.; Jansen, J.P.; et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: Checklist and explanations. Ann. Intern. Med. 2015, 162, 777–784. [Google Scholar] [CrossRef]
- de Sire, A.; Moggio, L.; Demeco, A.; Fortunato, F.; Spano, R.; Aiello, V.; Marotta, N.; Ammendolia, A. Efficacy of rehabilitative techniques in reducing hemiplegic shoulder pain in stroke: Systematic review and meta-analysis. Ann. Phys. Rehabil. Med. 2022, 65, 101602. [Google Scholar] [CrossRef]
- Marotta, N.; Demeco, A.; Indino, A.; de Scorpio, G.; Moggio, L.; Ammendolia, A. Nintendo Wii(TM) versus Xbox Kinect(TM) for functional locomotion in people with Parkinson’s disease: A systematic review and network meta-analysis. Disabil. Rehabil. 2022, 44, 331–336. [Google Scholar] [CrossRef]
- Lam, L.C.; Chau, R.C.; Wong, B.M.; Fung, A.W.; Tam, C.W.; Leung, G.T.; Kwok, T.C.; Leung, T.Y.; Ng, S.P.; Chan, W.M. A 1-year randomized controlled trial comparing mind body exercise (Tai Chi) with stretching and toning exercise on cognitive function in older Chinese adults at risk of cognitive decline. J. Am. Med. Dir. Assoc. 2012, 13, 568.e15–568.e20. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, T.; Shimada, H.; Makizako, H.; Doi, T.; Yoshida, D.; Ito, K.; Shimokata, H.; Washimi, Y.; Endo, H.; Kato, T. A randomized controlled trial of multicomponent exercise in older adults with mild cognitive impairment. PLoS ONE 2013, 8, e61483. [Google Scholar] [CrossRef] [PubMed]
- Yu, F.; Vock, D.M.; Zhang, L.; Salisbury, D.; Nelson, N.W.; Chow, L.S.; Smith, G.; Barclay, T.R.; Dysken, M.; Wyman, J.F. Cognitive effects of aerobic exercise in alzheimer’s disease: A pilot randomized controlled trial. J. Alzheimer’s Dis. JAD 2021, 80, 233–244. [Google Scholar] [CrossRef]
- Bisbe, M.; Fuente-Vidal, A.; Lopez, E.; Moreno, M.; Naya, M.; de Benetti, C.; Mila, R.; Bruna, O.; Boada, M.; Alegret, M. Comparative cognitive effects of choreographed exercise and multimodal physical therapy in older adults with amnestic mild cognitive impairment: Randomized clinical trial. J. Alzheimer’s Dis. JAD 2020, 73, 769–783. [Google Scholar] [CrossRef] [PubMed]
- Lamb, S.E.; Sheehan, B.; Atherton, N.; Nichols, V.; Collins, H.; Mistry, D.; Dosanjh, S.; Slowther, A.M.; Khan, I.; Petrou, S.; et al. Dementia And Physical Activity (DAPA) trial of moderate to high intensity exercise training for people with dementia: Randomised controlled trial. BMJ 2018, 361, k1675. [Google Scholar] [CrossRef] [PubMed]
- Yoon, D.H.; Kang, D.; Kim, H.J.; Kim, J.S.; Song, H.S.; Song, W. Effect of elastic band-based high-speed power training on cognitive function, physical performance and muscle strength in older women with mild cognitive impairment. Geriatr. Gerontol. Int. 2017, 17, 765–772. [Google Scholar] [CrossRef]
- Langoni, C.D.S.; Resende, T.L.; Barcellos, A.B.; Cecchele, B.; Knob, M.S.; Silva, T.D.N.; da Rosa, J.N.; Diogo, T.S.; Filho, I.; Schwanke, C.H.A. Effect of exercise on cognition, conditioning, muscle endurance, and balance in older adults with mild cognitive impairment: A randomized controlled trial. J. Geriatr. Phys. Ther. 2019, 42, E15–E22. [Google Scholar] [CrossRef]
- Wei, X.H.; Ji, L.L. Effect of handball training on cognitive ability in elderly with mild cognitive impairment. Neurosci. Lett. 2014, 566, 98–101. [Google Scholar] [CrossRef]
- Hong, S.G.; Kim, J.H.; Jun, T.W. Effects of 12-week resistance exercise on electroencephalogram patterns and cognitive function in the elderly with mild cognitive impairment: A randomized controlled trial. Clin. J. Sport Med. Off. J. Can. Acad. Sport Med. 2018, 28, 500–508. [Google Scholar] [CrossRef]
- Cancela, J.M.; Ayan, C.; Varela, S.; Seijo, M. Effects of a long-term aerobic exercise intervention on institutionalized patients with dementia. J. Sci. Med. Sport 2016, 19, 293–298. [Google Scholar] [CrossRef] [PubMed]
- Song, D.; Yu, D.S.F. Effects of a moderate-intensity aerobic exercise programme on the cognitive function and quality of life of community-dwelling elderly people with mild cognitive impairment: A randomised controlled trial. Int. J. Nurs. Stud. 2019, 93, 97–105. [Google Scholar] [CrossRef]
- Huang, N.; Li, W.; Rong, X.; Champ, M.; Wei, L.; Li, M.; Mu, H.; Hu, Y.; Ma, Z.; Lyu, J. Effects of a Modified Tai Chi Program on Older People with Mild Dementia: A Randomized Controlled Trial. J. Alzheimer’s Dis. JAD 2019, 72, 947–956. [Google Scholar] [CrossRef] [PubMed]
- Kemoun, G.; Thibaud, M.; Roumagne, N.; Carette, P.; Albinet, C.; Toussaint, L.; Paccalin, M.; Dugue, B. Effects of a physical training programme on cognitive function and walking efficiency in elderly persons with dementia. Dement. Geriatr. Cogn. Disord. 2010, 29, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Jurakic, G.Z.; Krizanic, V.; Sarabon, N.; Markovic, G. Effects of feedback-based balance and core resistance training vs. Pilates training on cognitive functions in older women with mild cognitive impairment: A pilot randomized controlled trial. Aging Clin. Exp. Res. 2017, 29, 1295–1298. [Google Scholar] [CrossRef]
- Law, L.L.F.; Mok, V.C.T.; Yau, M.M.K. Effects of functional tasks exercise on cognitive functions of older adults with mild cognitive impairment: A randomized controlled pilot trial. Alzheimer’s Res. Ther. 2019, 11, 98. [Google Scholar] [CrossRef] [PubMed]
- Shimada, H.; Lee, S.; Akishita, M.; Kozaki, K.; Iijima, K.; Nagai, K.; Ishii, S.; Tanaka, M.; Koshiba, H.; Tanaka, T.; et al. Effects of golf training on cognition in older adults: A randomised controlled trial. J. Epidemiol. Community Health 2018, 72, 944–950. [Google Scholar] [CrossRef]
- Bademli, K.; Lok, N.; Canbaz, M.; Lok, S. Effects of Physical Activity Program on cognitive function and sleep quality in elderly with mild cognitive impairment: A randomized controlled trial. Perspect. Psychiatr. Care 2019, 55, 401–408. [Google Scholar] [CrossRef]
- Holthoff, V.A.; Marschner, K.; Scharf, M.; Steding, J.; Meyer, S.; Koch, R.; Donix, M. Effects of physical activity training in patients with Alzheimer’s dementia: Results of a pilot RCT study. PLoS ONE 2015, 10, e0121478. [Google Scholar] [CrossRef]
- Varela, S.; Ayan, C.; Cancela, J.M.; Martin, V. Effects of two different intensities of aerobic exercise on elderly people with mild cognitive impairment: A randomized pilot study. Clin. Rehabil. 2012, 26, 442–450. [Google Scholar] [CrossRef]
- Lazarou, I.; Parastatidis, T.; Tsolaki, A.; Gkioka, M.; Karakostas, A.; Douka, S.; Tsolaki, M. International Ballroom Dancing Against Neurodegeneration: A Randomized Controlled Trial in Greek community-dwelling elders with mild cognitive impairment. Am. J. Alzheimer’s Dis. Other Dement. 2017, 32, 489–499. [Google Scholar] [CrossRef]
- Mavros, Y.; Gates, N.; Wilson, G.C.; Jain, N.; Meiklejohn, J.; Brodaty, H.; Wen, W.; Singh, N.; Baune, B.T.; Suo, C.; et al. Mediation of cognitive function improvements by strength gains after resistance training in older adults with mild cognitive impairment: Outcomes of the study of mental and resistance training. J. Am. Geriatr. Soc. 2017, 65, 550–559. [Google Scholar] [CrossRef]
- Hoffmann, K.; Sobol, N.A.; Frederiksen, K.S.; Beyer, N.; Vogel, A.; Vestergaard, K.; Braendgaard, H.; Gottrup, H.; Lolk, A.; Wermuth, L.; et al. Moderate-to-High Intensity Physical Exercise in Patients with Alzheimer’s Disease: A randomized controlled trial. J. Alzheimer’s Dis. JAD 2016, 50, 443–453. [Google Scholar] [CrossRef]
- Li, L.; Liu, M.; Zeng, H.; Pan, L. Multi-component exercise training improves the physical and cognitive function of the elderly with mild cognitive impairment: A six-month randomized controlled trial. Ann. Palliat. Med. 2021, 10, 8919–8929. [Google Scholar] [CrossRef]
- Tomoto, T.; Liu, J.; Tseng, B.Y.; Pasha, E.P.; Cardim, D.; Tarumi, T.; Hynan, L.S.; Munro Cullum, C.; Zhang, R. One-Year Aerobic Exercise reduced carotid arterial stiffness and increased cerebral blood flow in amnestic mild cognitive impairment. J. Alzheimer’s Dis. JAD 2021, 80, 841–853. [Google Scholar] [CrossRef]
- Aguiar, P.; Monteiro, L.; Feres, A.; Gomes, I.; Melo, A. Rivastigmine transdermal patch and physical exercises for alzheimer’s disease: A randomized clinical trial. Curr. Alzheimer Res. 2014, 11, 532–537. [Google Scholar] [CrossRef]
- Venturelli, M.; Scarsini, R.; Schena, F. Six-month walking program changes cognitive and ADL performance in patients with Alzheimer. Am. J. Alzheimer’s Dis. Other Dement. 2011, 26, 381–388. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.-Y.; Shan, C.-L.; Qing, H.; Wang, W.; Zhu, Y.; Yin, M.-M.; Machado, S.; Yuan, T.-F.; Wu, T. The effects of aerobic exercise on cognitive function of Alzheimer’s diseasepatients. CNS Neurol. Disord. Drug Targets 2015, 14, 1292–1297. [Google Scholar] [CrossRef]
- Silva, D.O.F.; Ferreira, J.V.; Placido, J.; Sant’Anna, P.; Araujo, J.; Marinho, V.; Laks, J.; Camaz Deslandes, A. Three months of multimodal training contributes to mobility and executive function in elderly individuals with mild cognitive impairment, but not in those with Alzheimer’s disease: A randomized controlled trial. Maturitas 2019, 126, 28–33. [Google Scholar] [CrossRef]
- Arcoverde, C.; Deslandes, A.; Moraes, H.; Almeida, C.; Araujo, N.B.; Vasques, P.E.; Silveira, H.; Laks, J. Treadmill training as an augmentation treatment for Alzheimer’s disease: A pilot randomized controlled study. Arq. Neuropsiquiatr. 2014, 72, 190–196. [Google Scholar] [CrossRef]
- Cruz, L.C.D.; Teixeira-Araujo, A.A.; Passos Andrade, K.T.; Rocha, T.; Puga, G.M.; Moreira, S.R. Low-intensity resistance exercise reduces hyperglycemia and enhances glucose control over a 24-hour period in women with type 2 Diabetes. J. Strength Cond. Res. 2019, 33, 2826–2835. [Google Scholar] [CrossRef]
- ACSM. Physical Activity Guidelines for Americans, 2nd ed.; American College of Sports Medicine: Indianapolis, IN, USA, 2018. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Serial Number | Content |
|---|---|
| #1 | Cognitive Dysfunction [Mesh Terms] OR Dementia [Mesh Terms] OR Alzheimer Disease [Mesh Terms] |
| #2 | Mild Cognitive Impairment [Title/Abstract] OR Mild Cognitive Disorder [Title/Abstract] OR Mild Cognitive Dysfunction [Title/Abstract] OR Mild Cognitive Decline [Title/Abstract] OR Mild Neurocognitive Disorder [Title/Abstract] |
| #3 | #1 OR #2 |
| #4 | Sports [Mesh Terms] OR Exercise [Mesh Terms] OR Exercise Movement Techniques [Mesh Terms] OR Resistance Training [Mesh Terms] OR Yoga [Mesh Terms] OR Dance Therapy [Mesh Terms] OR Virtual Reality Exposure Therapy [Mesh Terms] OR Breathing Exercises [Mesh Terms] OR Walking [Mesh Terms] OR High-Intensity Interval Training [Mesh Terms] OR Muscle Stretching Exercises [Mesh Terms] OR Tai Ji [Mesh Terms] |
| #5 | Core Stability [Title/Abstract] OR Whole Body Vibration Exercise [Title/Abstract] OR Body-Mind Exercise [Title/Abstract] OR Health Qigong [Title/Abstract] OR Yijinjing [Title/Abstract] OR Wuqinxi [Title/Abstract] OR Liuzijue [Title/Abstract] OR Baduanjin [Title/Abstract] OR Multicomponent Exercise [Title/Abstract] |
| #6 | #4 OR #5 |
| #7 | #3 AND #6 |
| Study | Age (T/C) | Sample (T/C) | Intervention/Comparator | Exercise Moderators | Outcome | |||
|---|---|---|---|---|---|---|---|---|
| Intensity | Time (Min) | Frequency (Days/Week) | Duration (Weeks) | |||||
| Lam 2012 [17] | 77.20 ± 6.30/78.30 ± 6.60 | 93/169 | Tai chi/stretching | moderate | 30 | ≥3 | 48 | ①③ |
| Suzuki 2013 [18] | 74.80 ± 7.40/75.80 ± 6.10 | 47/45 | multicomponent exercise/education | moderate | 90 | 2 | 24 | ①③ |
| Yu 2021 [19] | 77.4 ± 6.6/77.5 ± 7.1 | 64/32 | cycling/stretching | moderate | 40–60 | 3 | 24 | ① |
| Bisbe 2019 [20] | 72.88 ± 5.60/77.29 ± 5.16 | 17/14 | aerobic dances/multicomponent exercise | Moderate/moderate | 60 | NR | 12 | ③ |
| Lamb 2018 [21] | ≥65 | 278/137 | aerobic dances/usual care | NR | 60–90 | 12 | ① | |
| Yoon 2016 [22] | NR | 23/7 | strength training/stretching | vigorous/moderate | 60 | 2 | 12 | ③ |
| Langoni 2018 [23] | 72.60 ± 7.80/71.90 ± 7.90 | 26/26 | multicomponent exercise/no exercise | moderate | 60 | 2 | 24 | ③ |
| Wei 2014 [24] | 66.73 ± 5.48/65.27 ± 4.63 | 30/30 | handball/recreational activities | moderate | 30 | 5 | 24 | ③ |
| Hong 2017 [25] | 75.92 ± 4.81/77.89 ± 3.40 | 10/12 | resistance exercise/maintain current lifestyle | moderate | 60 | 2 | 12 | ④ |
| Cancela 2016 [26] | 80.63 ± 8.32/82.90 ± 7.42 | 73/113 | aerobic exercise/recreational activities | moderate | 15 | 4 | 12 | ③ |
| Song 2019 [27] | 76.22 ± 5.76/75.33 ± 6.78 | 60/60 | aerobic exercise/education | moderate | 60 | 2 | 16 | ③ |
| Huang 2019 [28] | 81.90 ± 6.00/81.90 ± 6.10 | 36/38 | Tai Chi/usual care | moderate | 20 | 3 | 40 | ④ |
| Kemoun 2010 [29] | 81.80 ± 5.30 | 16/15 | multicomponent exercise/recreational activities | moderate | 60 | 3 | 15 | ② |
| Jurakic 2017 [30] | 70.40 ± 3.93 | 14/14 | resistance exercise/Pilates | moderate/moderate | 30–60 | 3 | 8 | ④ |
| Law 2019 [31] | 77.94 ± 6.11/75.14 ± 8.53 | 16/14 | multicomponent exercise/maintain current lifestyle | moderate | 60 | 2 | 8 | ⑤ |
| Shimada 2018 [32] | 70.10 ± 4.00/70.70 ± 4.70 | 53/47 | golf/education | moderate | 90–120 | 1 | 12 | ③ |
| Bademli 2019 [33] | 72.24 ± 7.16/70.67 ± 8.34 | 30/30 | multicomponent exercise/maintain current lifestyle | moderate | 80 | 3 | 20 | ③ |
| Holthoff 2015 [34] | 72.40 ± 4.34/70.67 ± 5.41 | 13/12 | resistance exercise/maintain current lifestyle | moderate | 30 | 3 | 24 | ③ |
| Varela 2011 [35] | 77.88 ± 10.75/79.40 ± 6.72 | 33/15 | cycling/recreational activities | low | 30 | 3 | 12 | ③ |
| Lazarou 2017 [36] | 67.92 ± 9.47/65.89 ± 10.76 | 66/63 | international ballroom dancing/no exercise | moderate | 60 | 2 | 40 | ③④ |
| Mavros 2017 [37] | NR | 27/23 | resistance exercise/stretching | moderate | 75 | 2 | 24 | ① |
| Hoffmann 2016 [38] | 69.80 ± 7.40/71.30 ± 7.30 | 102/88 | aerobic exercise/maintain current lifestyle | vigorous | 60 | 3 | 16 | ③ |
| Li 2021 [39] | ≥60 | 42/42 | multicomponent exercise/stretching | NR | 30 | 5 | 24 | ③④ |
| Tomoto 2021 [40] | 55–80 | 17/20 | multicomponent exercise/stretching | vigorous | 30–40 | 3–4 | 48 | ③ |
| Aguiar 2014 [41] | 74.70 ± 7.40/78.60 ± 8.40 | 17/17 | multicomponent exercise/usual care | moderate | 40 | 2 | 24 | ③ |
| Venturelli 2011 [42] | 83 ± 6/85 ± 5 | 11/10 | walking program/usual care | moderate | 30 | 3 | 24 | ③ |
| Yang 2015 [43] | 72.00 ± 6.69/71.92 ± 7.28 | 25/25 | aerobic exercise/education | vigorous | 40 | 3 | 12 | ① |
| Silva 2019 [44] | 71.85 ± 5.69/78.20 ± 5.26 | 12/7 | multicomponent exercise/maintain current lifestyle | moderate | 60 | 2 | 12 | ③ |
| Arcoverde 2014 [45] | 78.5 (64–81.2)/79 (74.7–82.2) | 10/10 | aerobic exercise/education | vigorous | 30 | 2 | 16 | ③ |
| Moderators | Effect Size | ||||
|---|---|---|---|---|---|
| exercise type | multicomponent exercise | −0.05 (−1.68, 1.59) | - | - | −0.85 (−1.41, −0.28) |
| 0.11 (−0.53, 0.75) | aerobic exercise | 0.82 (−0.84, 2.48) | - | −0.72 (−1.55, 0.12) | |
| 0.03 (−0.89, 0.96) | −0.08 (−0.94, 0.79) | resistance training | - | −0.48 (−1.55, 0.59) | |
| 0.50 (−0.55, 1.55) | 0.39 (−0.61, 1.40) | 0.47 (−0.57, 1.50) | mind-body exercise | −0.72 (−1.17, −0.28) | |
| 0.84 (0.31, 1.36) | 0.73 (0.31, 1.15) | 0.80 (0.05, 1.56) | 0.34 (−0.58, 1.25) | control | |
| exercise time (min) | short | - | - | - | |
| 0.03 (−0.42, 0.47) | medium | - | - | ||
| 0.27 (−0.29, 0.83) | 0.24 (−0.33, 0.82) | long | - | ||
| 0.83 (0.53, 1.13) | 0.80 (0.48, 1.13) | 0.56 (0.09, 1.04) | control | ||
| exercise intensity | vigorous | - | - | - | |
| 0.04 (−0.60, 0.69) | moderate | - | - | ||
| 0.35 (−0.96, 1.65) | 0.30 (−0.87, 1.47) | light | - | ||
| 0.77 (0.18, 1.36) | 0.72 (0.43, 1.02) | 0.42 (−0.75, 1.59) | control | ||
| exercise frequency (days/week) | high | - | - | - | |
| 0.47 (−0.51, 1.46) | medium | - | - | ||
| 0.69 (−0.29, 1.67) | 0.22 (−0.44, 0.87) | low | - | ||
| 1.28 (0.41, 2.14) | 0.80 (0.33, 1.27) | 0.59 (0.14, 1.04) | control | ||
| Moderators | Sample Size (Number of Studies) | SMD (95% CI) | p Value | Rank (SUCRA) | |
|---|---|---|---|---|---|
| exercise type | multicomponent exercise | 483 (9) | 0.84 (0.31, 1.36) | 0.002 | 1 (74.3) |
| resistance training | 87 (5) | 0.80 (0.05, 1.56) | 0.037 | 3 (61.0) | |
| mind-body exercise | 143 (3) | 0.34 (−0.58, 1.25) | 0.471 | 4 (44.4) | |
| aerobic exercise | 559 (14) | 0.73 (0.31, 1.15) | 0.001 | 2 (63.9) | |
| exercise time (min) | short (≤45) | 400 (12) | 0.83 (0.18, 1.19) | <0.001 | 1 (77.3) |
| medium (>45–≤60) | 378 (10) | 0.68 (0.48, 1.13) | 0.008 | 2 (62.9) | |
| long (>60) | 435 (5) | 0.65 (−0.04, 1.34) | 0.067 | 3 (58.5) | |
| exercise intensity | light | 17 (1) | 0.42 (−0.75, 1.59) | 0.478 | 3 (45.9) |
| moderate | 681 (20) | 0.72 (0.43, 1.02) | <0.001 | 2 (71.8) | |
| vigorous | 93 (5) | 0.77 (0.18, 1.36) | 0.011 | 1 (74.4) | |
| exercise frequency (days/week) | low (≤2) | 629 (12) | 0.59 (0.14, 1.04) | 0.011 | 3 (44.5) |
| medium (3–4) | 437 (12) | 0.80 (0.33, 1.27) | 0.001 | 2 (64.0) | |
| high (5–7) | 145 (3) | 1.28 (0.41, 2.14) | 0.004 | 1 (91.3) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, J.; Dong, Y.; Yan, S.; Yi, L.; Qiu, J. Which Specific Exercise Models Are Most Effective on Global Cognition in Patients with Cognitive Impairment? A Network Meta-Analysis. Int. J. Environ. Res. Public Health 2023, 20, 2790. https://doi.org/10.3390/ijerph20042790
Yang J, Dong Y, Yan S, Yi L, Qiu J. Which Specific Exercise Models Are Most Effective on Global Cognition in Patients with Cognitive Impairment? A Network Meta-Analysis. International Journal of Environmental Research and Public Health. 2023; 20(4):2790. https://doi.org/10.3390/ijerph20042790
Chicago/Turabian StyleYang, Junchao, Yunfeng Dong, Shuting Yan, Longyan Yi, and Junqiang Qiu. 2023. "Which Specific Exercise Models Are Most Effective on Global Cognition in Patients with Cognitive Impairment? A Network Meta-Analysis" International Journal of Environmental Research and Public Health 20, no. 4: 2790. https://doi.org/10.3390/ijerph20042790
APA StyleYang, J., Dong, Y., Yan, S., Yi, L., & Qiu, J. (2023). Which Specific Exercise Models Are Most Effective on Global Cognition in Patients with Cognitive Impairment? A Network Meta-Analysis. International Journal of Environmental Research and Public Health, 20(4), 2790. https://doi.org/10.3390/ijerph20042790