
Epidemiological Profile among Greek CrossFit Practitioners

 ,
,  ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Population
2.3. Sample Calculation
2.4. Measurement Instrument
2.5. Statistical Analysis
3. Results
4. Discussion
4.1. Musculoskeletal Injury Analysis
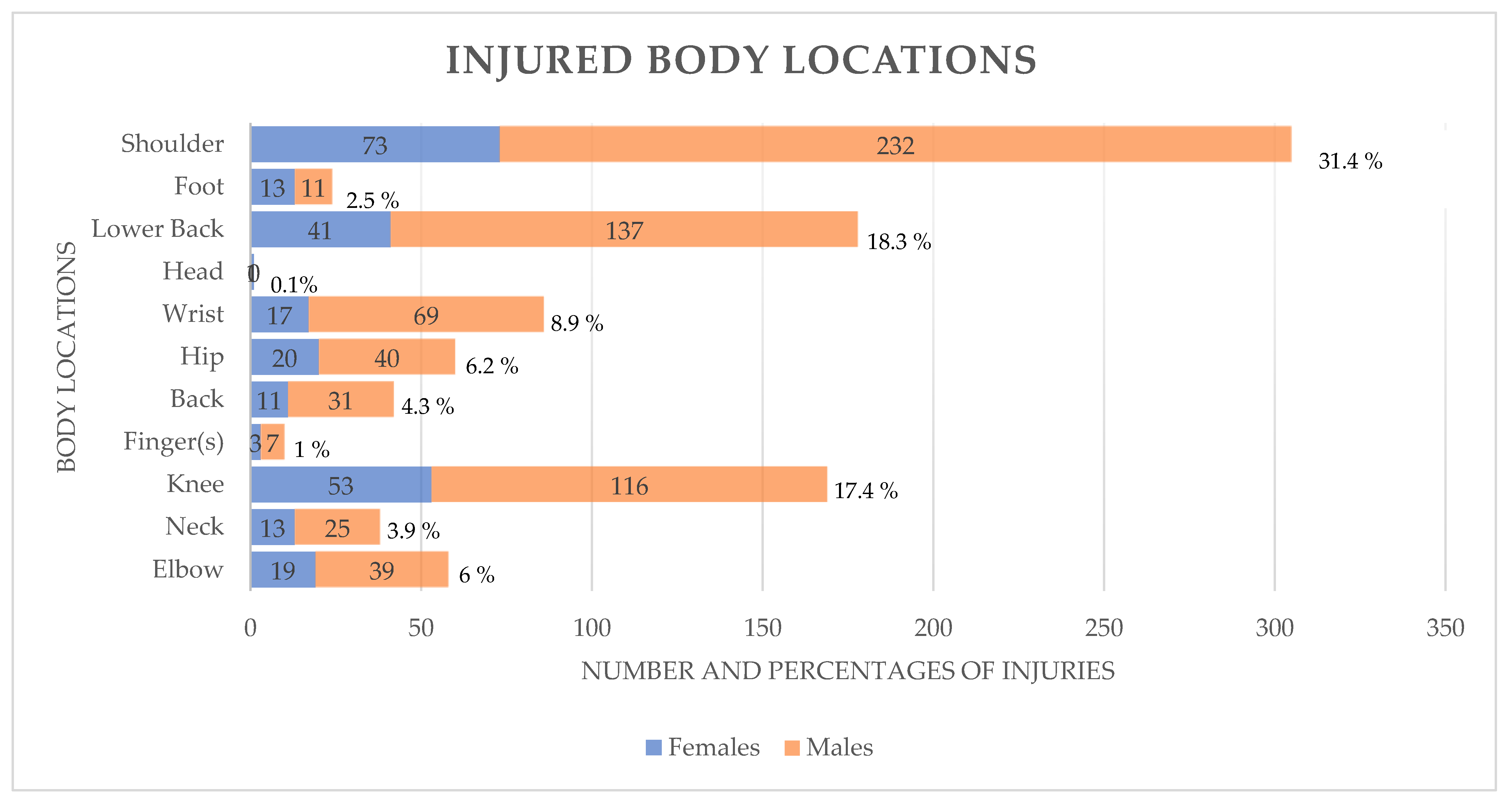
4.1.1. Type and Body Location of Injuries
4.1.2. Treatment and Nutrition in CF Participants
4.2. Risk Factors
4.2.1. Participation in CF Competitions
4.2.2. Rest Days per Week
4.2.3. CF Training Duration
4.2.4. Weekly CF Training Frequency
4.2.5. Prior to CF Training Level
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lavallee, M.E.; Balam, T. An Overview of Strength Training Injuries: Acute and Chronic. Curr. Sports Med. Rep. 2010, 9, 307–313. [Google Scholar] [CrossRef] [PubMed]
- Alekseyev, K.; John, A.; Malek, A.; Lakdawala, M.; Verma, N.; Southall, C.; Nikolaidis, A.; Akella, S.; Erosa, S.; Islam, R.; et al. Identifying the Most Common CrossFit Injuries in a Variety of Athletes. Rehabil. Process Outcome 2020, 9, 117957271989706. [Google Scholar] [CrossRef]
- Minghelli, B.; Vicente, P. Musculoskeletal Injuries in Portuguese CrossFit Practitioners. J. Sports Med. Phys. Fit. 2019, 59, 1213–1220. [Google Scholar] [CrossRef] [PubMed]
- Weisenthal, B.M.; Beck, C.A.; Maloney, M.D.; DeHaven, K.E.; Giordano, B.D. Injury Rate and Patterns among Crossfit Athletes. Orthop. J. Sports Med. 2014, 2, 2325967114531177. [Google Scholar] [CrossRef] [PubMed]
- Gerhart, H.D. A Comparison of Crossfit Training to Traditional Anaerobic Resistance Training in Terms of Selected Fitness Domains Representative of Overall Athletic Performance. Master’s Thesis, Indiana University of Pennsylvania, Indiana, PA, USA, 2013. Volume 9. p. 85. [Google Scholar]
- Sprey, J.W.C.; Ferreira, T.; de Lima, M.V.; Duarte, A.; Jorge, P.B.; Santili, C. An Epidemiological Profile of CrossFit Athletes in Brazil. Orthop. J. Sports Med. 2016, 4, 232596711666370. [Google Scholar] [CrossRef] [PubMed]
- Montalvo, A.M.; Shaefer, H.; Rodriguez, B.; Li, T.; Epnere, K.; Myer, G.D. Retrospective Injury Epidemiology and Risk Factors for Injury in CrossFit. J. Sports Sci. Med. 2017, 16, 53–59. [Google Scholar] [PubMed]
- Moran, S.; Booker, H.; Staines, J.; Williams, S. Rates and Risk Factors of Injury in CrossFitTM: A Prospective Cohort Study. J. Sports Med. Phys. Fit. 2017, 57, 1147–1153. [Google Scholar] [CrossRef]
- Gianzina, E.A.; Kassotaki, O.A. The Benefits and Risks of the High-Intensity CrossFit Training. Sport Sci. Health 2019, 15, 21–33. [Google Scholar] [CrossRef]
- CrossFit. CrossFit about Affiliation. Available online: https://www.crossfit.com/affiliate (accessed on 4 March 2021).
- CrossFit Inc. CrossFit Map. Available online: https://map.crossfit.com/ (accessed on 4 March 2021).
- CrossFit—About CrossFit Affiliates. Available online: https://www.crossfit.com/about-crossfit-affiliates (accessed on 4 March 2021).
- Meyer, J.; Morrison, J.; Zuniga, J. The Benefits and Risks of CrossFit: A Systematic Review. Workplace Health Saf. 2017, 65, 612–618. [Google Scholar] [CrossRef]
- Glassman, G. Understanding CrossFit. CrossFit J. 2007, 56, 1–2. [Google Scholar]
- Drum, S.N.; Bellovary, B.N.; Jensen, R.L.; Moore, M.T.; Donath, L. Perceived Demands and Postexercise Physical Dysfunction in CrossFit® Compared to an ACSM Based Training Session. J. Sports Med. Phys. Fit. 2017, 57, 604–609. [Google Scholar] [CrossRef] [PubMed]
- Tafuri, S.; Salatino, G.; Napoletano, P.L.; Monno, A.; Notarnicola, A. The Risk of Injuries among CrossFit Athletes: An Italian Observational Retrospective Survey. J. Sports Med. Phys. Fit. 2019, 59, 1544–1550. [Google Scholar] [CrossRef] [PubMed]
- da Costa, T.S.; Louzada, C.T.N.; Miyashita, G.K.; da Silva, P.H.J.; Sungaila, H.Y.F.; Lara, P.H.S.; de Castro Pochini, A.; Ejnisman, B.; Cohen, M.; Arliani, G.G. Crossfit®: Injury Prevalence and Main Risk Factors. Clinics 2019, 74, e1402. [Google Scholar] [CrossRef]
- de Almeida Xavier, A.; da Costa Lopes, A.M. Lesões Musculoesqueléticas Em Praticantes de Crossfit. Rev. Interdiscip. Cienc. Med. 2017, 1, 11–27. [Google Scholar]
- Szeles, P.R.D.Q.; Costa, T.S.D.; Cunha, R.A.D.; Hespanhol, L.; Pochini, A.D.C.; Ramos, L.A.; Cohen, M. CrossFit and the Epidemiology of Musculoskeletal Injuries: A Prospective 12-Week Cohort Study. Orthop. J. Sports Med. 2020, 8, 2325967120908884. [Google Scholar] [CrossRef] [PubMed]
- Mehrab, M.; de Vos, R.-J.; Kraan, G.A.; Mathijssen, N.M.C. Injury Incidence and Patterns Among Dutch CrossFit Athletes. Orthop. J. Sports Med. 2017, 5, 232596711774526. [Google Scholar] [CrossRef] [PubMed]
- Gile, M.; Petit, J.; Gremeaux, V. Évaluation du Taux de Blessures Chez les Pratiquants de CrossFit en France. J. Traumatol. Sport 2020, 37, 2–9. [Google Scholar] [CrossRef]
- Feito, Y.; Burrows, E.K.; Tabb, L.P. A 4-Year Analysis of the Incidence of Injuries Among CrossFit-Trained Participants. Orthop. J. Sports Med. 2018, 6, 232596711880310. [Google Scholar] [CrossRef]
- Summitt, R.J.; Cotton, R.A.; Kays, A.C.; Slaven, E.J. Shoulder Injuries in Individuals Who Participate in CrossFit Training. Sports Health 2016, 8, 541–546. [Google Scholar] [CrossRef]
- Silva, C. A Profile of Injuries Among Participants at the 2013 CrossFit Games in Durban. Master’s Thesis, Chiropractic Durban University of Technology, Berea, South Africa, 2013. [Google Scholar]
- Escalante, G.; Gentry, C.R.; Kern, B.D.; Waryasz, G.R. Injury Patterns and Rates of Costa Rican CrossFit® Participants-a Retrospective Study. J. Rom. Sports Med. Soc. 2017, XIII, 2927–2934. [Google Scholar]
- Elliott, M.N.; Haviland, A.M. Use of a Web-Based Convenience Sample to Supplement a Probability Sample. Surv. Methodol. 2007, 33, 211–215. [Google Scholar]
- Byrne, M. Sampling for Qualitative Research. AORN J. 2001, 73, 522–526. [Google Scholar] [CrossRef] [PubMed]
- Hak, P.T.; Hodzovic, E.; Hickey, B. The Nature and Prevalence of Injury during CrossFit Training. J. Strength Cond. Res. 2013. [Google Scholar] [CrossRef] [PubMed]
- Grier, T.; Canham-Chervak, M.; McNulty, V.; Jones, B.H. Extreme Conditioning Programs and Injury Risk in a US Army Brigade Combat Team. US Army Med. Dep. J. 2013, 11, 36–47. [Google Scholar]
- Everhart, J.S.; Poland, S.; Vajapey, S.P.; Kirven, J.C.; France, T.J.; Vasileff, W.K. CrossFit-Related Hip and Groin Injuries: A Case Series. J. Hip Preserv. Surg. 2020, 7, 109–115. [Google Scholar] [CrossRef]
- Larsen, R.T.; Hessner, A.L.; Ishøi, L.; Langberg, H.; Christensen, J. Injuries in Novice Participants during an Eight-Week Start up CrossFit Program—A Prospective Cohort Study. Sports 2020, 8, 21. [Google Scholar] [CrossRef]
- Hopkins, B.S.; Cloney, M.B.; Kesavabhotla, K.; Yamaguchi, J.; Smith, Z.A.; Koski, T.R.; Hsu, W.K.; Dahdaleh, N.S. Impact of CrossFit-Related Spinal Injuries. Clin. J. Sport Med. 2019, 29, 482–485. [Google Scholar] [CrossRef] [PubMed]
- Keogh, J.W.L.; Winwood, P.W. The Epidemiology of Injuries Across the Weight-Training Sports. Sports Med. 2017, 47, 479–501. [Google Scholar] [CrossRef] [PubMed]
- Keogh, J.; Hume, P.A.; Pearson, S. Retrospective Injury Epidemiology of One Hundred One Competitive Oceania Power Lifters: The Effects of Age, Body Mass, Competitive Standard, and Gender. J. Strength Cond. Res. 2006, 20, 672–681. [Google Scholar] [CrossRef] [PubMed]
- Thomas, D.T.; Erdman, K.A.; Burke, L.M. Position of the Academy of Nutrition and Dietetics, Dietitians of Canada, and the American College of Sports Medicine: Nutrition and Athletic Performance. J. Acad. Nutr. Diet. 2016, 116, 501–528. [Google Scholar] [CrossRef] [PubMed]
- Crossfit, Inc. CrossFit Certifications. Available online: https://www.crossfit.com/certifications. (accessed on 4 March 2021).
- Nestle, M. Paleolithic Diets: A Sceptical View. Nutr. Bull. 2000, 25, 43–47. [Google Scholar] [CrossRef]
- Maxwell, C.; Ruth, K.; Friesen, C. Sports Nutrition Knowledge, Perceptions, Resources, and Advice given by Certified Crossfit Trainers. Sports 2017, 5, 21. [Google Scholar] [CrossRef]
- dos Santos Quaresma, M.V.L.; Guazzelli Marques, C.; Nakamoto, F.P. Effects of Diet Interventions, Dietary Supplements, and Performance-Enhancing Substances on the Performance of CrossFit-Trained Individuals: A Systematic Review of Clinical Studies. Nutrition 2021, 82, 110994. [Google Scholar] [CrossRef]
- Kerksick, C.M.; Wilborn, C.D.; Roberts, M.D.; Smith-Ryan, A.; Kleiner, S.M.; Jäger, R.; Collins, R.; Cooke, M.; Davis, J.N.; Galvan, E.; et al. ISSN Exercise & Sports Nutrition Review Update: Research & Recommendations. J. Int. Soc. Sports Nutr. 2018, 15, 38. [Google Scholar] [CrossRef]
- Gogojewicz, A.; Śliwicka, E.; Durkalec-Michalski, K. Assessment of Dietary Intake and Nutritional Status in Crossfit-Trained Individuals: A Descriptive Study. Int. J. Environ. Res. Public Health 2020, 17, 4772. [Google Scholar] [CrossRef]
- Teixeira, R.V.; Dantas, M.; Motas, D.G.D.; Gantois, P.; Aidar, F.J.; Dantas, P.M.S.; Queiros, V.S.D.; Cesário, T.D.M.; De Araújo Tinôco Cabral, B.G. Retrospective Study of Risk Factors and the Prevalence of Injuries in HIFT. Int. J. Sports Med. 2020, 41, 168–174. [Google Scholar] [CrossRef] [PubMed]
- Feito, Y.; Burrows, E.; Tabb, L.; Ciesielka, K.A. Breaking the Myths of Competition: A Cross-Sectional Analysis of Injuries among CrossFit Trained Participants. BMJ Open Sport Exerc. Med. 2020, 6, e000750. [Google Scholar] [CrossRef] [PubMed]
- Chachula, L.A.; Cameron, K.L.; Svoboda, S.J. Association of Prior Injury With the Report of New Injuries Sustained During CrossFit Training. Athl. Train. Sports Health Care 2016, 8, 28–34. [Google Scholar] [CrossRef]
- Lima, P.O.; Souza, M.B.; Sampaio, T.V.; Almeida, G.P.; Oliveira, R.R. Epidemiology and Associated Factors for Crossfit-Related Musculoskeletal Injuries: A Cross-Sectional Study. J. Sports Med. Phys. Fit. 2020, 60, 889–894. [Google Scholar] [CrossRef]
- Sugimoto, D.; Zwicker, R.L.; Quinn, B.J.; Myer, G.D.; Stracciolini, A. Part II: Comparison of Crossfit-Related Injury Presenting to Sports Medicine Clinic by Sex and Age. Clin. J. Sport Med. 2020, 30, 251–256. [Google Scholar] [CrossRef]
- Smith, M.F.; Hillman, R. A Retrospective Service Audit of a Mobile Physiotherapy Unit on the PGA European Golf Tour. Phys. Ther. Sport 2012, 13, 41–44. [Google Scholar] [CrossRef] [PubMed]
- Kellmann, M. Preventing Overtraining in Athletes in High-Intensity Sports and Stress/Recovery Monitoring. Scand. J. Med. Sci. Sports 2010, 20, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Lund, S.S.; Myklebust, G. High Injury Incidence in TeamGym Competition: A Prospective Cohort Study. Scand. J. Med. Sci. Sports 2011, 21, e439–e444. [Google Scholar] [CrossRef] [PubMed]
- Maffulli, N.; Longo, U.G.; Gougoulias, N.; Caine, D.; Denaro, V. Sport Injuries: A Review of Outcomes. Br. Med. Bull. 2011, 97, 47–80. [Google Scholar] [CrossRef] [PubMed]
- Winwood, P.W.; Hume, P.A.; Cronin, J.B.; Keogh, J.W.L. Retrospective Injury Epidemiology of Strongman Athletes. J. Strength Cond. Res. 2014, 28, 28–42. [Google Scholar] [CrossRef]
- Soares, M.R.A.D.R. An Epidemiological Profile of Crossfit Participants in Portugal. Master’s Thesis, Universidade Lusófona de Humanidades e Tecnologias, Lisbon, Portugal, 2017. [Google Scholar]
- Pescatello, L.S.; Arena, R.; Riebe, D.; Thompson, P.D. ACSM’s Guidelines for Exercise Testing and Prescription 9th Ed. 2014. J. Can. Chiropr. Assoc. 2013, 9, 456. [Google Scholar]
- Post, E.G.; Trigsted, S.M.; Riekena, J.W.; Hetzel, S.; McGuine, T.A.; Brooks, M.A.; Bell, D.R. The Association of Sport Specialization and Training Volume With Injury History in Youth Athletes. Am. J. Sports Med. 2017, 45, 1405–1412. [Google Scholar] [CrossRef]
- Moustakidis, S.; Siouras, A.; Vassis, K.; Misiris, I.; Papageorgiou, E.; Tsaopoulos, D. Prediction of Injuries in CrossFit Training: A Machine Learning Perspective. Algorithms 2022, 15, 77. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Sex | n (%) |
|---|---|
| Female | 443 (36) |
| Male | 781 (64) |
| Age group | |
| <18 | 0 (0) |
| 18–29 | 598 (49) |
| 30–39 | 448 (37) |
| 40–49 | 162 (13) |
| ≥50 | 16 (1) |
| Mean ± SD | 30.76 ± 7.58 |
| Height | |
| Mean ± SD | 175.40 ± 8.78 |
| Weight | |
| Mean ± SD | 75.89 ± 13.24 |
| BMI, kg/m2 | |
| Mean ± SD | 24.5 ± 2.72 |
| Type of physical effort that work involve | |
| Sedentary | 501 (41) |
| Many hours of standing and walking without weight transfer | 404 (33) |
| Many hours of standing and walking as well as lifting and transferring weights | 287 (23.4) |
| Lifting heavy objects | 32 (2.6) |
| Any Sports Participation before Starting CrossFit? | |
|---|---|
| No | 155 (12.7) |
| Yes | 1069 (87) |
| Type of sport practiced * | |
| Soccer | 145 (11.8) |
| Basketball | 80 (6.5) |
| Volleyball | 26 (2.1) |
| Running | 64 (5.2) |
| Cycling | 15 (1.2) |
| Swimming | 57 (4.7) |
| Weight training | 430 (35.1) |
| Bodybuilding | 5 (0.4) |
| Tennis | 14 (1.1) |
| Group training programs | 93(7.6) |
| Functional training | 30 (2.5) |
| Martial arts | 97 (7.9) |
| Track and field sports | 80 (6.5) |
| Other | 83 (6.8) |
| Level of sport practiced | |
| Low | 216 (17.6) |
| Medium | 598 (48.9) |
| High | 410 (33.5) |
| Athlete Characteristics | n (%) |
|---|---|
| CF Experience, n (%) | |
| 0–6 mo | 126 (10.3) |
| 6–12 mo | 143 (11.7) |
| 12–24 mo | 361 (29.5) |
| ≥24 mo | 594 (48.5) |
| Reasons for starting participating CF * | |
| Fitness | 835 (68) |
| Curiosity | 321 (26) |
| Recommendation from a professional | 263 (22) |
| Practice frequency | |
| 1–2 times/wk | 69 (6) |
| 3–4 times/wk | 592 (48) |
| >4 times/wk | 563 (46) |
| Mean | 4.27 ± 1.14 |
| Median (range) | 4 (1–7) |
| Workout Duration, n (%) | |
| <1 h | 98 (8) |
| ≥1 h | 1126 (92) |
| Presence of Injury | ||||
|---|---|---|---|---|
| Variable | Yes | No | Total Responses | p |
| Sex | n (%) | n (%) | N | 0.001 * |
| Female | 143 (32.3) | 300 (67.7) | 443 | |
| Male | 391 (50.1) | 390 (49.9) | 781 | |
| Age | 0.000 * | |||
| Mean (±SD) | 31.79 ± 7.52 | 29.96 ± 7.53 | 30.76 ± 7.58 | |
| Height | 0.899 | |||
| Mean (±SD) | 175.43 ± 8.56 | 175.37 ± 8.95 | 175.40 ± 8.78 | |
| BMI | 0.000 * | |||
| Mean (±SD) | 24.96 ± 2.71 | 24.14 ± 2.67 | 24.50 ± 2.72 | |
| Experienced in CrossFit training, y | 0.000 * | |||
| <1 | 67 (24.9) | 202 (75.1) | 269 | |
| 1–2 | 107 (29.6) | 254 (70.4) | 361 | |
| >2 | 360 (60.6) | 234 (39.4) | 594 | |
| training time, min/wk | 0.001 * | |||
| <30 min | 4 (44.4) | 5 (55.5) | 9 | |
| 30–60 min | 234 (38.6) | 372 (61.4) | 606 | |
| 61–90 min | 175 (39.9) | 264 (60.1) | 439 | |
| 91–120 min | 46 (64.8) | 25 (35.2) | 71 | |
| ≥121 min | 75 (75.7) | 24 (24.2) | 99 | |
| Weekly participation, d/wk | 0.000 * | |||
| <3 | 24 (34.8) | 45 (65.2) | 69 | |
| 3–5 | 419 (41.6) | 589 (58.4) | 1008 | |
| >5 | 91 (61.9) | 56 (38.1) | 147 | |
| Participation in competitions | 0.001 * | |||
| yes | 189 (68.5) | 87 (31.5) | 276 | |
| no | 345 (36.4) | 603 (63.6) | 948 | |
| Rest day | 0.001 * | |||
| ≤3 times/wk | 488 (45.2) | 592 (54.8) | 1080 | |
| >3 times/wk | 46 (31.9) | 98 (68) | 144 | |
| Level of athletic activity-fitness before starting CF | 0.001 * | |||
| Low | 100 (46.3) | 116 (53.7) | 216 | |
| Medium | 210 (35.1) | 388 (64.9) | 598 | |
| High | 224 (54.6) | 186 (45.4) | 410 | |
| Mentioning medical history to CF coach before started training | 0.000 * | |||
| yes | 406 (40.2) | 603 (59.8) | 1009 | |
| no | 128 (59.5) | 87 (40.5) | 215 | |
| Coach monitoring | 0.001 * | |||
| yes | 478 (41.4) | 675 (58.5) | 1153 | |
| no | 55 (77.5) | 16 (22.5) | 71 | |
| Monitoring by a health professional on a regular basis | 0.000 * | |||
| yes | 212 (54.4) | 178 (45.6) | 390 | |
| no | 322 (38.6) | 512 (61.4) | 834 | |
| Passive recovery | 0.001 * | |||
| yes | 159 (63.6) | 91 (36.4) | 250 | |
| no | 375 (38.5) | 599 (61.5) | 974 | |
| Nutrition program | 0.001 * | |||
| yes | 139 (54.5) | 116 (45.5) | 255 | |
| no | 395 (40.8) | 574 (59.2) | 969 | |
| Dietary supplement | 0.001 * | |||
| yes | 326 (51.1) | 312 (48.9) | 638 | |
| no | 208 (35.5) | 378 (64.5) | 586 | |
| Types of dietary supplement ** | 0.094 | |||
| Vitamins | 190 (54.3) | 160 (45.7) | 350 | |
| Amino acids | 140 (54.1) | 119 (45.9) | 259 | |
| Protein | 138 (40.6) | 202 (59.4) | 340 | |
| Other | 50 (68.5) | 23 (31.5) | 73 | |
| Variable | Injured Participants |
|---|---|
| Report to coach about pain, discomfort or inability to execute the program | |
| Yes (I mentioned it and stopped) | 455 (85.2) |
| No (I did not mentioned it and continued) | 75 (14) |
| Injury to the same body location in the past | |
| Yes | 224 (41.9) |
| No | 310 (58.1) |
| Type of injury * | |
| Muscle Pain | 274 (51.3) |
| Tendon Pain | 265 (49.6) |
| Joint Pain | 142 (26.6) |
| Neuropathic Pain | 73 (13.7) |
| I do not know the type of injury I had | 41 (7.7) |
| Abstinence from training (days) | |
| 1 to 7 days | 111 (20.8) |
| 7 to 14 days | 58 (10.9) |
| 14 to 28 days | 55 (10.3) |
| 28 to 60 days | 40 (7.5) |
| More than 60 days | 44 (8.2) |
| Treat injury by a health care professional-rehabilitation specialist | |
| Yes | 419 (78.5) |
| No | 115 (21.5) |
| Type of health care professional * | |
| Doctor | 265 (49.6) |
| Physiotherapist | 280 (52.4) |
| Other | 9 (1.7) |
| Treatment followed * | |
| Physiotherapy | 298 (55.8) |
| Rest | 385 (72.1) |
| Medication | 147 (27.5) |
| Injections | 63 (11.8) |
| Surgery | 22 (4.1) |
| Risk Factors | B | S.E. | df | Sig. | Odds Ratio (95% CI) |
|---|---|---|---|---|---|
| Participation in competitions (yes/no) | 1.085 | 0.18 | 1 | 0.00 * | 2.959 (2.49–3.58) |
| Training Level prior to CF (Low/Medium/High) | −0.072 | 0.09 | 1 | 0.43 * | 0.931 (0.88–0.98) |
| Rest/week (days/week) | 0.253 | 0.095 | 1 | 0.01 * | 1.288 (1.12–1.44) |
| Training Duration (minutes per session) | −0.156 | 0.052 | 1 | 0.00 * | 0.856 (0.76–0.93) |
| Frequency of training (Days/week) | 0.187 | 0.08 | 1 | 0.02 * | 1.206 (1.14–1.27) |
| Constant | −1.286 | 0.587 | 1 | 0.03 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vassis, K.; Siouras, A.; Kourkoulis, N.; Poulis, I.A.; Meletiou, G.; Iliopoulou, A.-M.; Misiris, I. Epidemiological Profile among Greek CrossFit Practitioners. Int. J. Environ. Res. Public Health 2023, 20, 2538. https://doi.org/10.3390/ijerph20032538
Vassis K, Siouras A, Kourkoulis N, Poulis IA, Meletiou G, Iliopoulou A-M, Misiris I. Epidemiological Profile among Greek CrossFit Practitioners. International Journal of Environmental Research and Public Health. 2023; 20(3):2538. https://doi.org/10.3390/ijerph20032538
Chicago/Turabian StyleVassis, Konstantinos, Athanasios Siouras, Nikolaos Kourkoulis, Ioannis A. Poulis, Georgios Meletiou, Anna-Maria Iliopoulou, and Ioannis Misiris. 2023. "Epidemiological Profile among Greek CrossFit Practitioners" International Journal of Environmental Research and Public Health 20, no. 3: 2538. https://doi.org/10.3390/ijerph20032538
APA StyleVassis, K., Siouras, A., Kourkoulis, N., Poulis, I. A., Meletiou, G., Iliopoulou, A.-M., & Misiris, I. (2023). Epidemiological Profile among Greek CrossFit Practitioners. International Journal of Environmental Research and Public Health, 20(3), 2538. https://doi.org/10.3390/ijerph20032538