Muscle Activity and Co-Activation of Gait Cycle during Walking in Water and on Land in People with Spastic Cerebral Palsy


Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Experimental Procedure
2.2.1. EMG Assessment
2.2.2. Muscle Co-Activation
2.2.3. Spatiotemporal Data
2.3. Statistical Analysis
3. Results
3.1. Participant Characteristics
3.2. Spatiotemporal Parameters
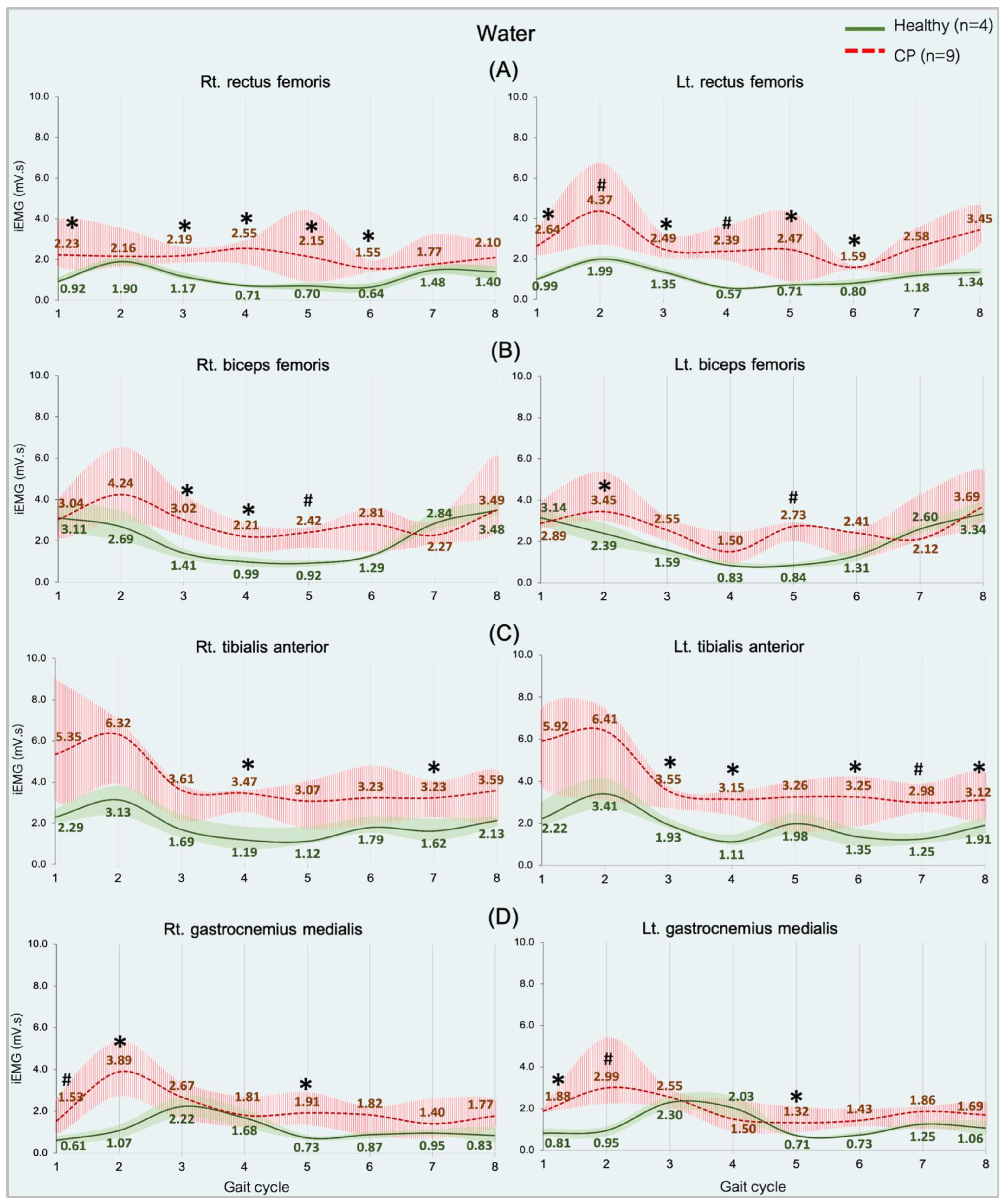
3.3. EMG Activities during Gait Cycle
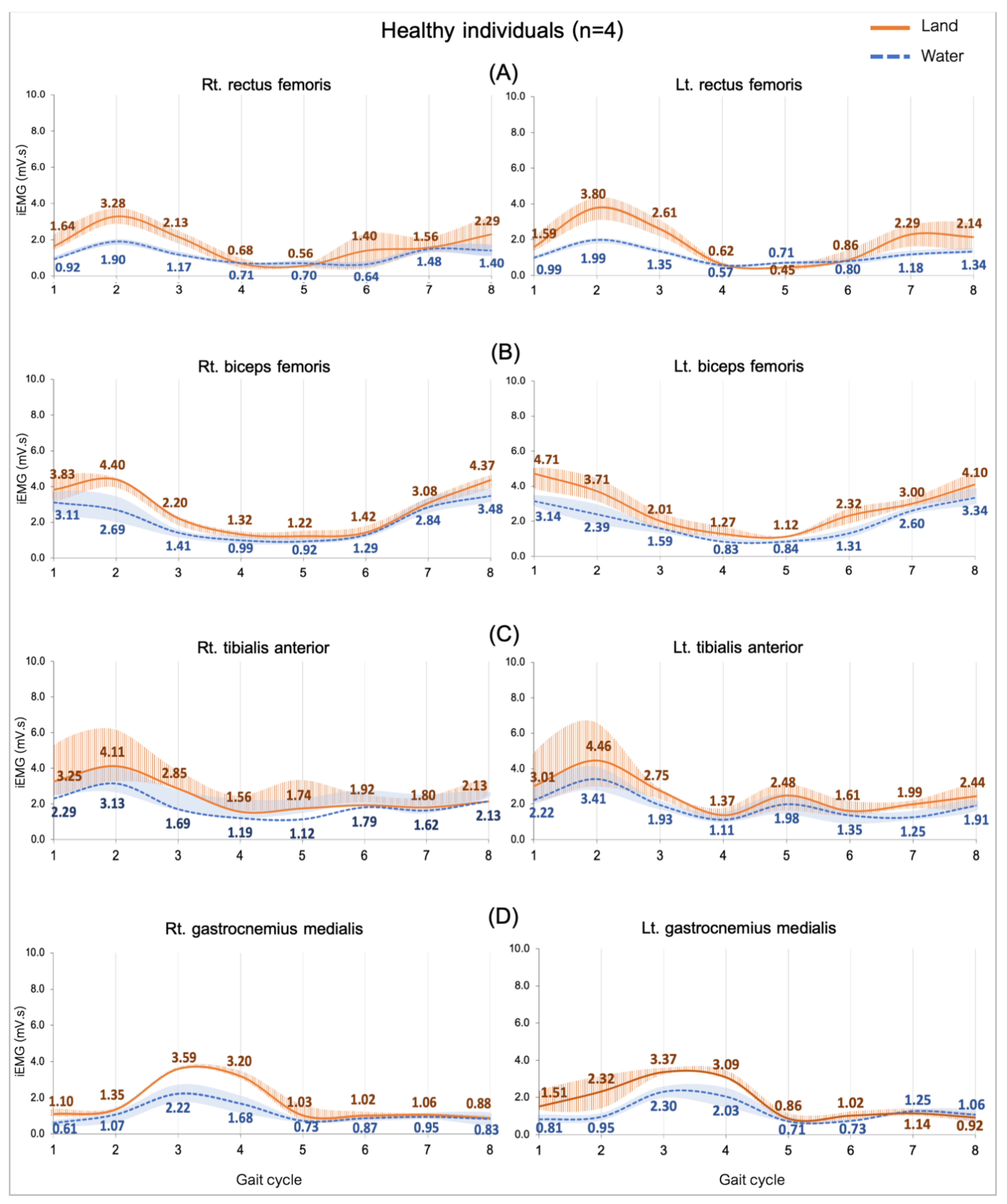
3.3.1. Comparing in Water and on Land in Healthy Subjects
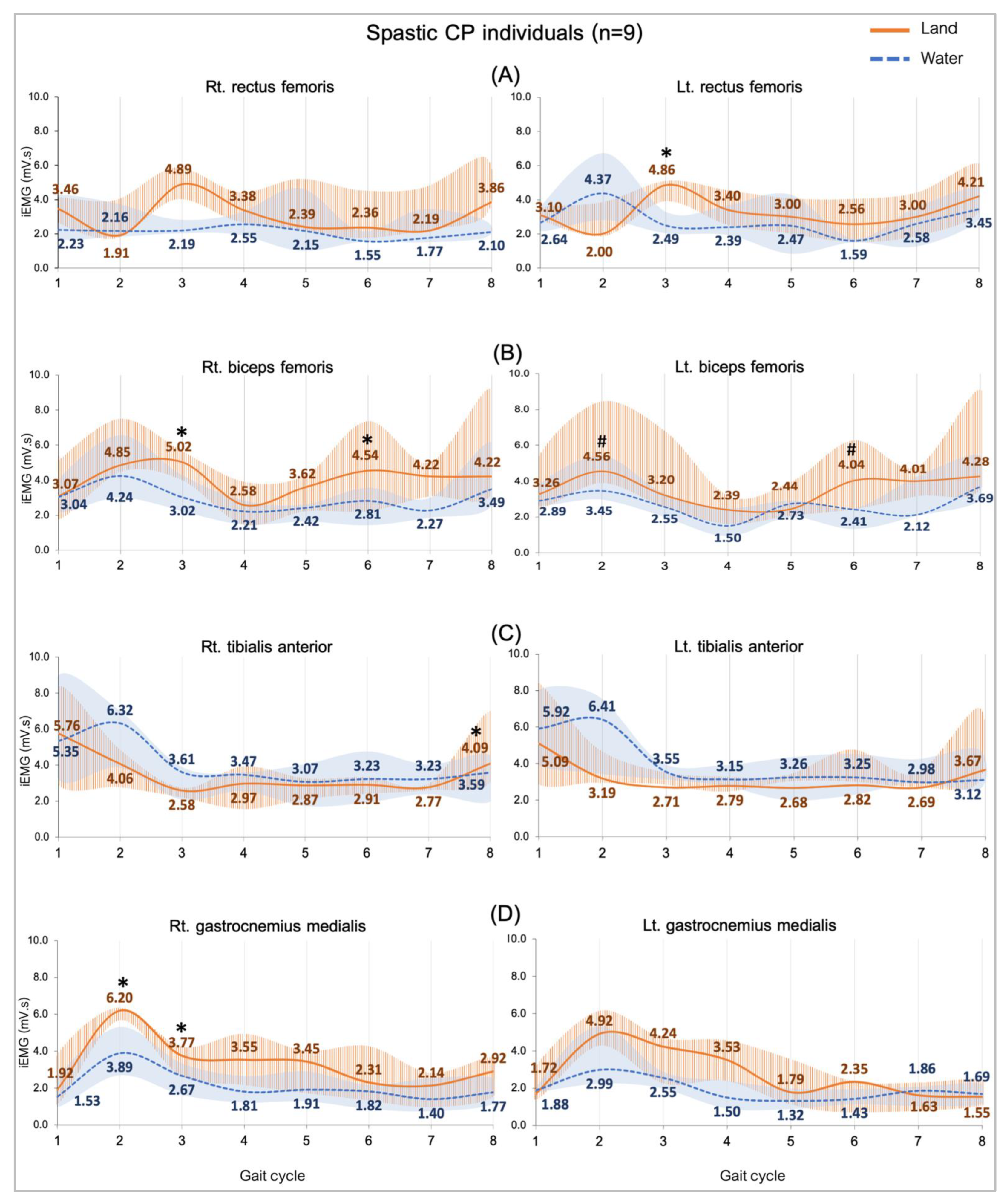
3.3.2. Comparing Subjects with CP in Water and on Land
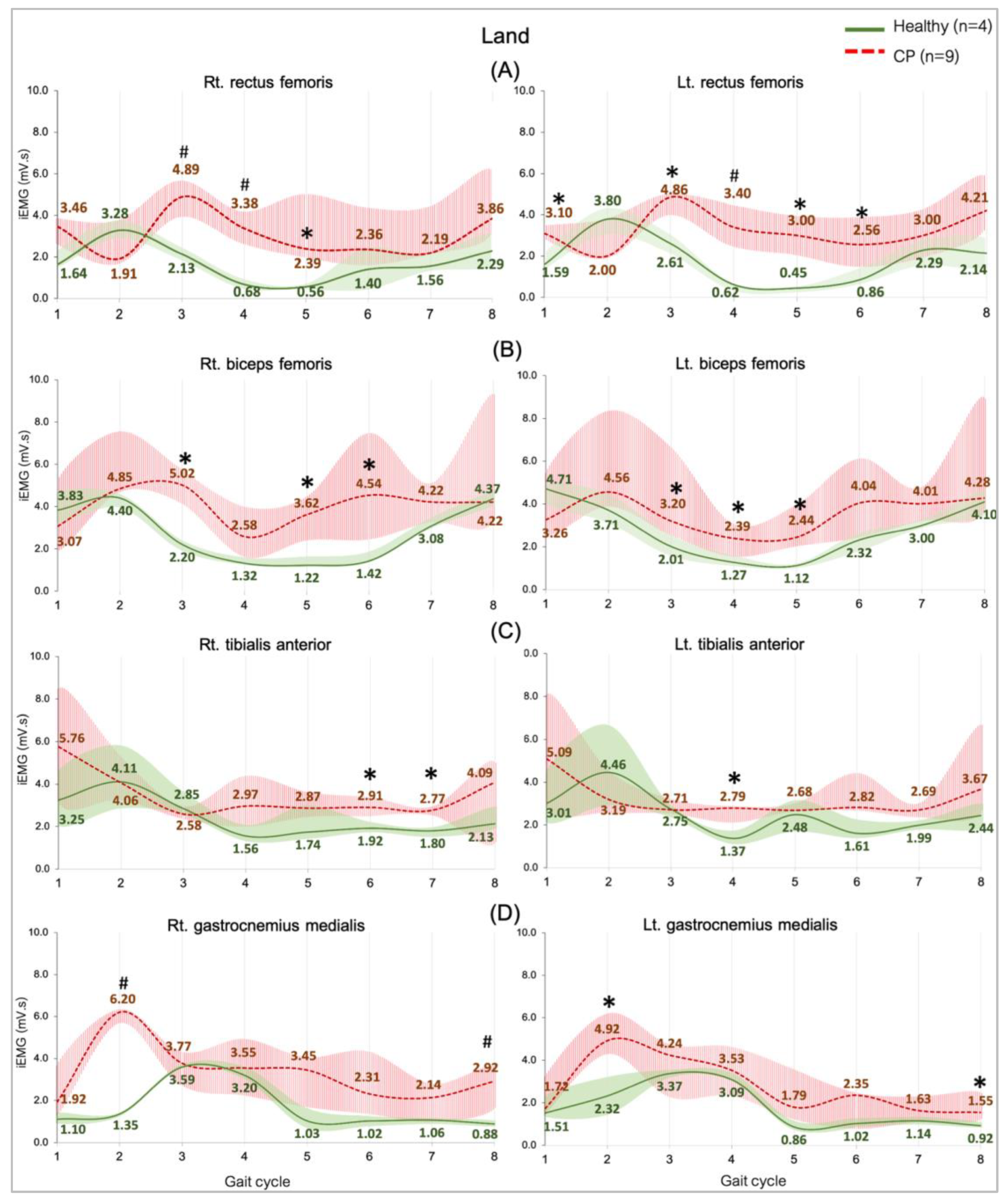
3.3.3. Comparing between Groups on Land
3.3.4. Comparing between Groups in Water
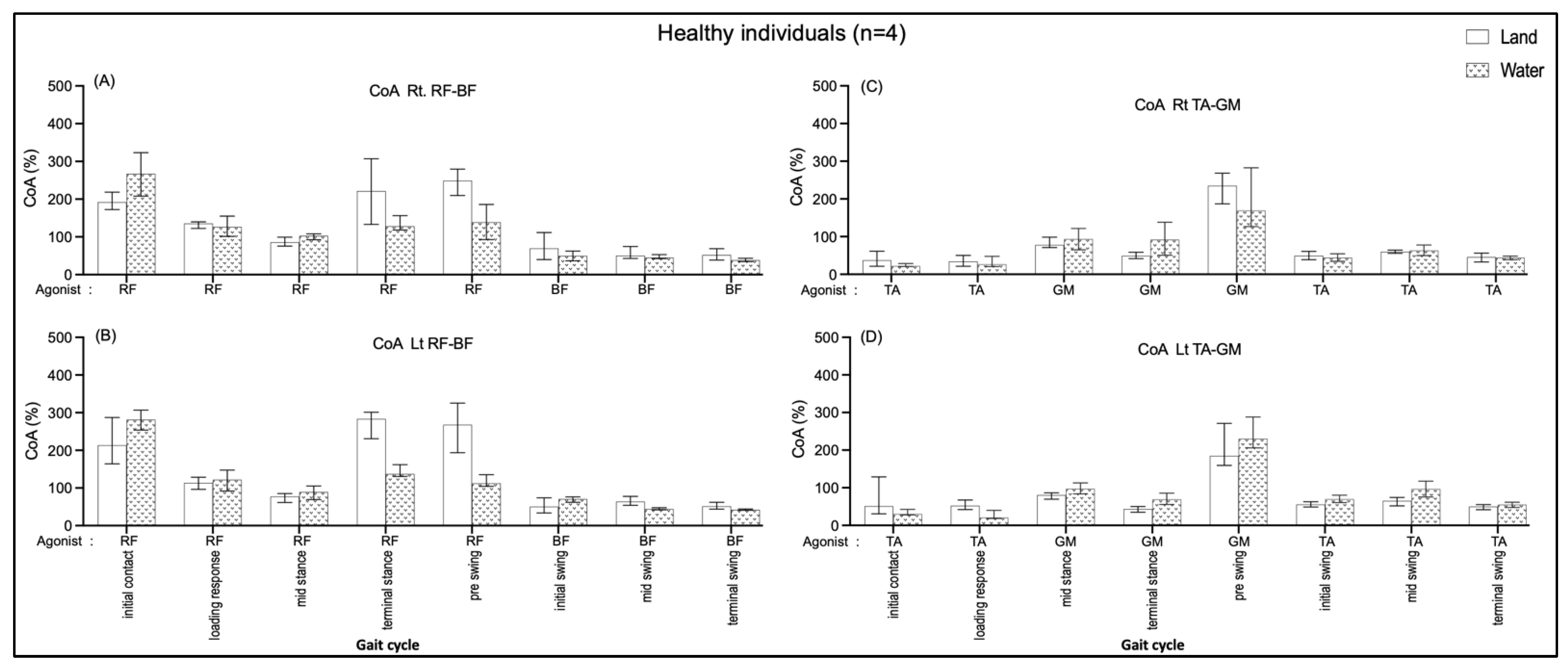
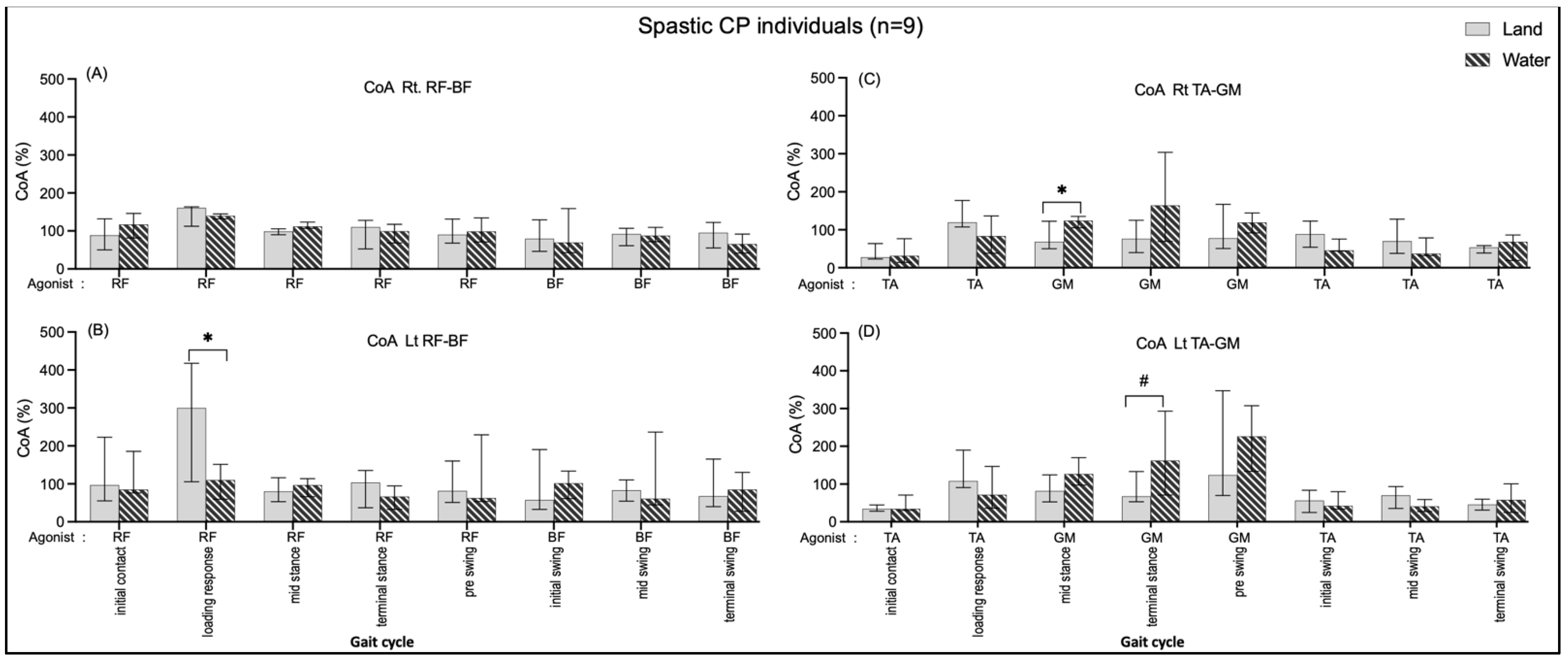
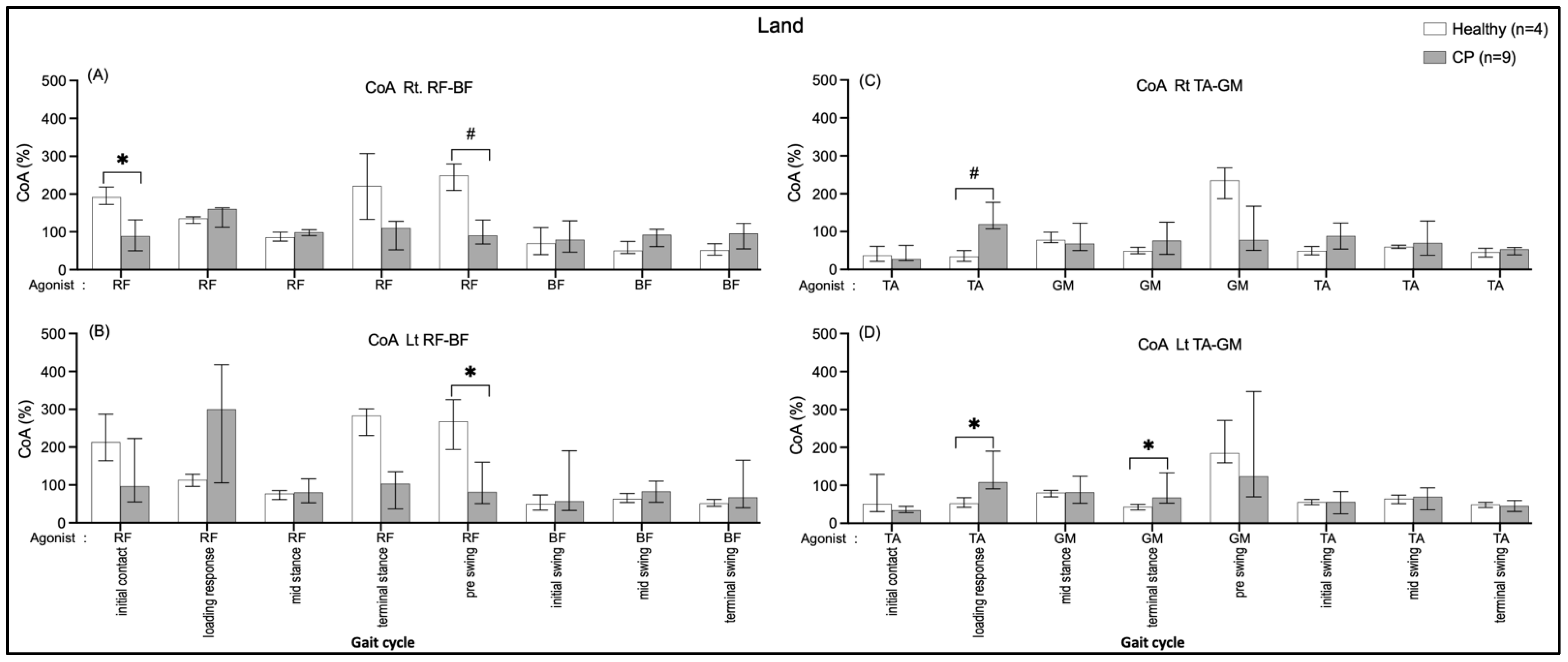
3.4. Muscle Co-Activation during Gait Cycle
3.4.1. Comparing in Water and on Land in Healthy Subjects
3.4.2. Comparing in Water and on Land in Subjects with Cerebral Palsy
3.4.3. Comparing between Groups on Land
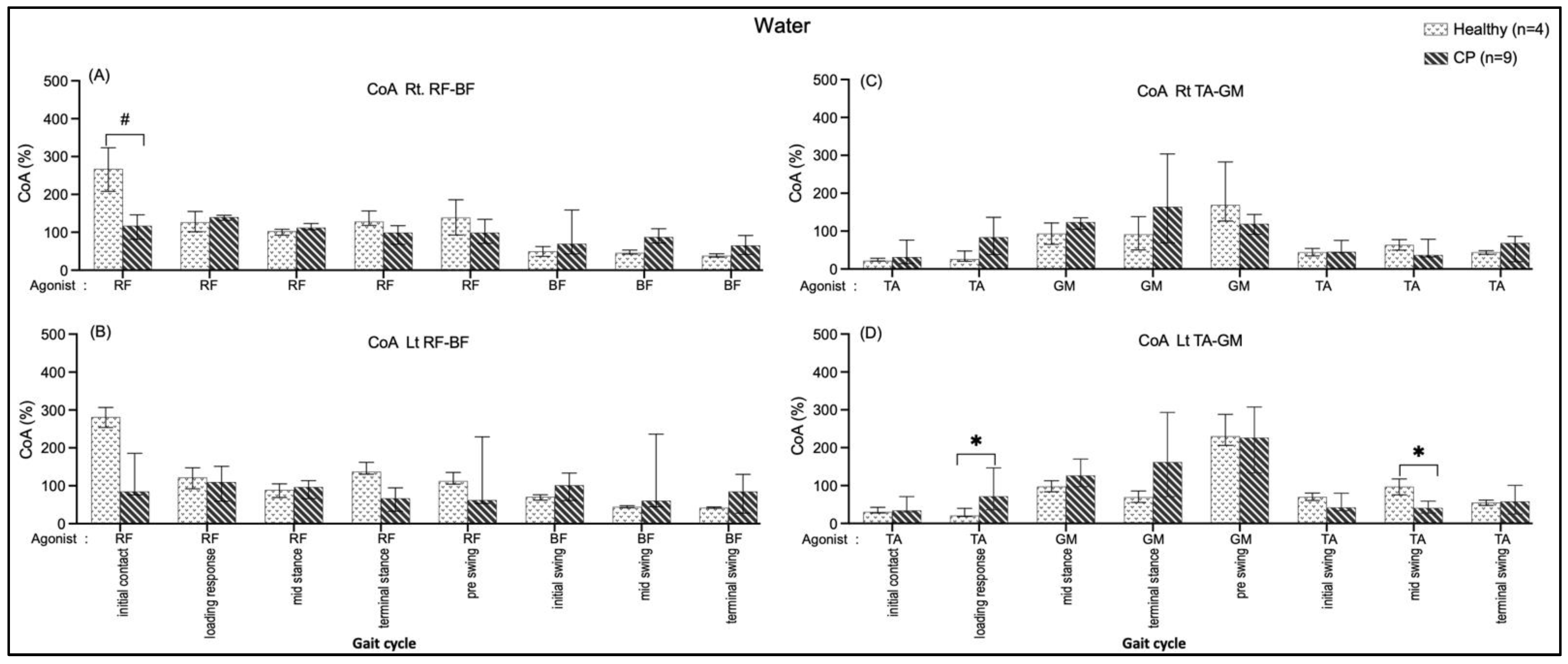
3.4.4. Comparing between Groups in Water
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rosenbaum, P. The Definition and Classification of Cerebral Palsy. Neoreviews 2006, 7, e569–e574. [Google Scholar] [CrossRef]
- Bojanic, D.M.; Petrovacki-Balj, B.D.; Jorgovanovic, N.D.; Ilic, V.R. Quantification of Dynamic EMG Patterns during Gait in Children with Cerebral Palsy. J. Neurosci. Methods 2011, 198, 325–331. [Google Scholar] [CrossRef] [PubMed]
- Colborne, G.R.; Wright, F.V.; Naumann, S. Feedback of Triceps Surae EMG in Gait of Children with Cerebral Palsy: A Controlled Study. Arch. Phys. Med. Rehabil. 1994, 75, 40–45. [Google Scholar] [CrossRef] [PubMed]
- Gagnat, Y.; Brændvik, S.M.; Roeleveld, K. Surface Electromyography Normalization Affects the Interpretation of Muscle Activity and Coactivation in Children with Cerebral Palsy during Walking. Front. Neurol. 2020, 11, 202. [Google Scholar] [CrossRef] [PubMed]
- Unnithan, V.B.; Dowling, J.J.; Frost, G.; Volpe Ayub, B.; Bar-Or, O. Cocontraction and Phasic Activity during GAIT in Children with Cerebral Palsy. Electromyogr. Clin. Neurophysiol. 1996, 36, 487–494. [Google Scholar]
- Oliveira, L.C.; Trócoli, T.O.; Kanashiro, M.S.; Braga, D.; Cyrillo, F.N. Electromyographic Analysis of Rectus Femoris Activity during Seated to Standing Position and Walking in Water and on Dry Land in Healthy Children and Children with Cerebral Palsy. J. Electromyogr. Kinesiol. 2014, 24, 855–859. [Google Scholar] [CrossRef]
- Van Der Krogt, M.M.; Doorenbosch, C.A.M.; Becher, J.G.; Harlaar, J. Dynamic Spasticity of Plantar Flexor Muscles in Cerebral Palsy Gait. J. Rehabil. Med. 2010, 42, 656–663. [Google Scholar] [CrossRef]
- Sutthibuta, U. Systematic Review of Aquatic Exercise Programming for Children and Adolescents with Cerebral Palsy. Int. J. Child Dev. Ment. Health 2014, 2, 49–66. [Google Scholar]
- He, M.X.; Lei, C.J.; Zhong, D.L.; Liu, Q.C.; Zhang, H.; Huang, Y.J.; Li, Y.X.; Liu, X.B.; Li, J.; Jin, R.J.; et al. The Effectiveness and Safety of Electromyography Biofeedback Therapy for Motor Dysfunction of Children with Cerebral Palsy: A Protocol for Systematic Review and Meta-Analysis. Medicine 2019, 98, e16786. [Google Scholar] [CrossRef]
- Hermens, H.J.; Freriks, B.; Disselhorst-Klug, C.; Rau, G. Development of Recommendations for SEMG Sensors and Sensor Placement Procedures. J. Electromyogr. Kinesiol. 2000, 10, 361–374. [Google Scholar] [CrossRef]
- Koury, J.M. Aquatic Therapy Programming: Guidelines for Orthopedic Rehabilitation; Human Kinetics: Champaign, IL, USA, 1996. [Google Scholar]
- Gage, J.R. An Overview of Normal Walking. Instr. Course Lect. 1990, 39, 291–303. [Google Scholar]
- Ervilha, U.F.; Graven-Nielsen, T.; Duarte, M. A Simple Test of Muscle Coactivation Estimation Using Electromyography. Braz. J. Med. Biol. Res. 2012, 45, 977–981. [Google Scholar] [CrossRef] [PubMed]
- Stöckel, T.; Jacksteit, R.; Behrens, M.; Skripitz, R.; Bader, R.; Mau-Moeller, A. The Mental Representation of the Human Gait in Young and Older Adults. Front. Psychol. 2015, 6, 943. [Google Scholar] [CrossRef]
- Masumoto, K.; Takasugi, S.-I.; Hotta, N.; Fujishima, K.; Iwamoto, Y. Electromyographic Analysis of Walking in Water in Healthy Humans. J. Physiol. Anthropol. Appl. Hum. Sci. 2004, 23, 119–127. [Google Scholar] [CrossRef] [PubMed]
- Dietz, V.; Colombo, G. Effects of Body Immersion on Postural Adjustments to Voluntary Arm Movements in Humans: Role of Load Receptor Input. J. Physiol. 1996, 497, 849–856. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, J.; Thorstensson, A.; Halbertsma, J. Changes in Leg Movements and Muscle Activity with Speed of Locomotion and Mode of Progression in Humans. Acta Physiol. Scand. 1985, 123, 457–475. [Google Scholar] [CrossRef]
- Shono, T.; Masumoto, K.; Fujishima, K.; Hotta, N.; Ogaki, T.; Adachi, T. Gait Patterns and Muscle Activity in the Lower Extremities of Elderly Women during Underwater Treadmill Walking against Water Flow. J. Physiol. Anthropol. 2007, 26, 579–586. [Google Scholar] [CrossRef]
- Lorencová, K.; Pavlů, D.; Pánek, D. EMG Analysis of the Influence of a Water Environment on the Rehabilitation of Patients with Parkinson’s Disease. Auc Kinanthropologica 2018, 54, 118–128. [Google Scholar] [CrossRef]
- Jung, T.; Kim, Y.; Lim, H.; Vrongistinos, K. The Influence of Water Depth on Kinematic and Spatiotemporal Gait Parameters during Aquatic Treadmill Walking. Sports Biomech. 2019, 18, 297–307. [Google Scholar] [CrossRef]
- Avela, J.; Santos, P.M.; Kyröläinen, H.; Komi, P.V. Effects of Different Simulated Gravity Conditions on Neuromuscular Control in Drop Jump Exercises. Aviat. Space Environ. Med. 1994, 65, 301–308. [Google Scholar]
- Newman, D.J.; Alexander, H.L.; Webbon, B.W. Energetics and Mechanics for Partial Gravity Locomotion. Aviat. Space Environ. Med. 1994, 65, 815–823. [Google Scholar] [PubMed]
- Barela, A.M.F.; Stolf, S.F.; Duarte, M. Biomechanical Characteristics of Adults Walking in Shallow Water and on Land. J. Electromyogr. Kinesiol. 2006, 16, 250–256. [Google Scholar] [CrossRef]
- Barela, A.M.F.; Duarte, M. Biomechanical Characteristics of Elderly Individuals Walking on Land and in Water. J. Electromyogr. Kinesiol. 2008, 18, 446–454. [Google Scholar] [CrossRef] [PubMed]
- Orselli, M.I.; Duarte, M. Joint Forces and Torques When Walking in Shallow Water. J. Biomech. 2011, 44, 1170–1175. [Google Scholar] [CrossRef] [PubMed]
- Boudarham, J.; Hameau, S.; Zory, R.; Hardy, A.; Bensmail, D.; Roche, N. Coactivation of Lower Limb Muscles during Gait in Patients with Multiple Sclerosis. PLoS ONE 2016, 11, e0158267. [Google Scholar] [CrossRef]
- Kelleher, K.J.; Spence, W.; Solomonidis, S.; Apatsidis, D. The Characterisation of Gait Patterns of People with Multiple Sclerosis. Disabil. Rehabil. 2010, 32, 1242–1250. [Google Scholar] [CrossRef]
- Piitulainen, H.; Kulmala, J.; Mäenpää, H.; Rantalainen, T. The Gait Is Less Stable in Children with Cerebral Palsy in Normal and Dual- Task Gait Compared to Typically Developed Peers. J. Biomech. 2021, 117, 110244. [Google Scholar] [CrossRef]
- Akl, A.R.; Gonçalves, P.; Fonseca, P.; Hassan, A.; Vilas-Boas, J.P.; Conceição, F. Muscle Co-Activation around the Knee during Different Walking Speeds in Healthy Females. Sensors 2021, 21, 677. [Google Scholar] [CrossRef]
- Gross, R.; Leboeuf, F.; Hardouin, J.B.; Perrouin-Verbe, B.; Brochard, S.; Rémy-Néris, O. Does Muscle Coactivation Influence Joint Excursions during Gait in Children with and without Hemiplegic Cerebral Palsy? Relationship between Muscle Coactivation and Joint Kinematics. Clin. Biomech. 2015, 30, 1088–1093. [Google Scholar] [CrossRef]
- Pierce, S.R.; Barbe, M.F.; Barr, A.E.; Shewokis, P.A.; Lauer, R.T. Roles of Reflex Activity and Co-Contraction during Assessments of Spasticity of the Knee Flexor and Knee Extensor Muscles in Children with Cerebral Palsy and Different Functional Levels. Phys. Ther. 2008, 88, 1124–1134. [Google Scholar] [CrossRef]
- Engsberg, J.R.; Ross, S.A.; Olree, K.S.; Park, T.S. Ankle Spasticity and Strength in Children with Spastic Diplegic Cerebral Palsy. Dev. Med. Child Neurol. 2000, 42, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Mari, S.; Serrao, M.; Casali, C.; Conte, C.; Martino, G.; Ranavolo, A.; Coppola, G.; Draicchio, F.; Padua, L.; Sandrini, G.; et al. Lower Limb Antagonist Muscle Co-Activation and Its Relationship with Gait Parameters in Cerebellar Ataxia. Cerebellum 2014, 13, 226–236. [Google Scholar] [CrossRef] [PubMed]
- Lamontagne, A.; Richards, C.L.; Malouin, F. Coactivation during Gait as an Adaptive Behavior after Stroke. J. Electromyogr. Kinesiol. 2000, 10, 407–415. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.H.; Shin, H.K. The Effects of Water-Based Exercise on Postural Control in Children with Spastic Cerebral Palsy. Phys. Ther. Rehabil. Sci. 2017, 6, 77–82. [Google Scholar] [CrossRef]
- Hesse, S.; Werner, C.; Paul, T.; Bardeleben, A.; Chaler, J. Influence of Walking Speed on Lower Limb Muscle Activity and Energy Consumption during Treadmill Walking of Hemiparetic Patients. Arch. Phys. Med. Rehabil. 2001, 82, 1547–1550. [Google Scholar] [CrossRef]
- Ikeda, A.J.; Abel, M.F.; Granata, K.P.; Damiano, D.L. Quantification of Cocontraction in Spastic Cerebral Palsy. Electromyogr. Clin. Neurophysiol. 1998, 38, 497–504. [Google Scholar] [CrossRef]
- Lin, C.J.; Guo, L.Y.; Su, F.C.; Chou, Y.L.; Cherng, R.J. Common Abnormal Kinetic Patterns of the Knee in Gait in Spastic Diplegia of Cerebral Palsy. Gait Posture 2000, 11, 224–232. [Google Scholar] [CrossRef]
- Sutherland, D.H.; Cooper, L. The Pathomechanics of Progressive Crouch Gait in Spastic Diplegia. Orthop. Clin. N. Am. 1978, 9, 143–154. [Google Scholar] [CrossRef]
- Fung, J.; Barbeau, H. A Dynamic EMG Profile Index to Quantify Muscular Activation Disorder in Spastic Paretic Gait. Electroencephalogr. Clin. Neurophysiol. 1989, 73, 233–244. [Google Scholar] [CrossRef]
- Damiano, D.L.; Martellotta, T.L.; Sullivan, D.J.; Granata, K.P.; Abel, M.F. Muscle Force Production and Functional Performance in Spastic Cerebral Palsy: Relationship of Cocontraction. Arch. Phys. Med. Rehabil. 2000, 81, 895–900. [Google Scholar] [CrossRef]
- Den Otter, A.R.; Geurts, A.C.H.; Mulder, T.; Duysens, J. Speed Related Changes in Muscle Activity from Normal to Very Slow Walking Speeds. Gait Posture 2004, 19, 270–278. [Google Scholar] [CrossRef] [PubMed]
- Dietz, V.; Zijlstra, W.; Prokop, T.; Berger, W. Leg Muscle Activation during Gait in Parkinson’s Disease: Adaptation and Interlimb Coordination. Electroencephalogr. Clin. Neurophysiol. Electromyogr. 1995, 97, 408–415. [Google Scholar] [CrossRef] [PubMed]
- Cadenas-Sanchez, C.; Arellano, R.; Vanrenterghem, J.; López-Contreras, G. Kinematic Adaptations of Forward and Backward Walking on Land and in Water. J. Hum. Kinet. 2015, 49, 15–24. [Google Scholar] [CrossRef] [PubMed]
- Chevutschi, A.; Lensel, G.; Vaast, D.; Thevenon, A. An Electromyographic Study of Human Gait Both in Water and on Dry Ground. J. Physiol. Anthropol. 2007, 26, 467–473. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Age | Sex | Height (m) | Weight (Kg) | BMI (Kg/m2) | GMFCs | |
|---|---|---|---|---|---|---|---|
| Healthy | 1 | 16 | M | 1.23 | 25.60 | 16.92 | - |
| 2 | 15 | F | 1.53 | 38.00 | 16.23 | - | |
| 3 | 13 | M | 1.60 | 41.00 | 16.02 | - | |
| 4 | 12 | M | 1.61 | 55.00 | 21.22 | - | |
| Median | 14.00 | 3M,1F | 1.57 | 39.50 | 16.58 | ||
| Q1, Q3 | 12.75, 15.25 | 1.46, 1.60 | 34.90, 44.50 | 16.16, 18.00 | |||
| CP | 1 | 16 | M | 1.55 | 44.68 | 18.60 | I |
| 2 | 15 | M | 1.36 | 25.00 | 13.52 | I | |
| 3 | 13 | M | 1.34 | 32.00 | 17.82 | I | |
| 4 | 12 | M | 1.29 | 21.50 | 12.92 | I | |
| 5 | 16 | M | 1.45 | 26.70 | 12.70 | I | |
| 6 | 15 | M | 1.42 | 37.12 | 18.41 | I | |
| 7 | 16 | M | 1.50 | 36.70 | 16.31 | I | |
| 8 | 17 | F | 1.53 | 45.00 | 19.22 | II | |
| 9 | 13 | M | 1.38 | 41.00 | 21.53 | II | |
| Median | 15.00 | 8M,1F | 1.42 | 36.7 | 17.82 | ||
| Q1, Q3 | 13.00, 16.00 | 1.36, 1.50 | 26.7, 40.00 | 13.52, 18.60 |
| Healthy (n = 4) | CP (n = 9) | Between Gr. p-Value | |
|---|---|---|---|
| Walking speed (m/s) | |||
| • Land | 1.15 [1.04,1.27] | 0.83 [0.69,0.91] | 0.02 * |
| • Water | 1.07 [0.96,1.15] | 0.61 [0.49,0.74] | 0.009 # |
| Within-gr. p-value | 0.07 | 0.008 # | |
| Rt. Cadence (step/s) | |||
| • Land | 1.82 [1.65,2.06] | 1.98 [1.70,2.09] | 1.00 |
| • Water | 2.17 [1.99,2.30] | 1.86 [1.59,2.15] | 0.28 |
| Within-gr. p-value | 0.27 | 0.59 | |
| Lt. Cadence (step/s) | |||
| • Land | 1.79 [1.60,1.92] | 1.92 [1.56,1.99] | 0.54 |
| • Water | 2.09 [2.02,2.15] | 1.88 [1.70,2.03] | 0.22 |
| Within-gr. p-value | 0.07 | 0.59 | |
| Rt. Gait cycle time (s) | |||
| • Land | 1.00 [0.97,1.04] | 1.06 [1.05,1.10] | 0.36 |
| • Water | 1.60 [1.48,1.74] | 1.55 [1.30,1.57] | 0.28 |
| Within-gr. p-value | 0.07 | 0.008 * | |
| Lt. Gait cycle time (s) | |||
| • Land | 1.06 [1.00,1.09] | 1.18 [1.11,1.21] | 0.44 |
| • Water | 1.59 [1.52,1.69] | 1.55 [1.30,1.57] | 0.22 |
| Within-gr. p-value | 0.07 | 0.015 * | |
| Rt. % Stance phase | |||
| • Land | 64.33 [63.35,65.23] | 67.70 [67.42,69.45] | 0.03 * |
| • Water | 62.25 [61.25,62.91] | 65.33 [62.42,67.45] | 0.12 |
| Within-gr. p-value | 0.07 | 0.03 * | |
| Lt. % Stance phase | |||
| • Land | 63.38 [62.44,64.26] | 67.90 [66.73,68.35] | 0.02 * |
| • Water | 62.88 [62.54,63.33] | 65.34 [63.09,65.71] | 0.19 |
| Within-gr. p-value | 1.00 | 0.011 * | |
| Rt. % Swing phase | |||
| • Land | 35.67 [34.77,36.66] | 32.30 [30.55,32.58] | 0.03 * |
| • Water | 37.81 [37.09,38.75] | 34.67 [32.55,37.58] | 0.12 |
| Within-gr. p-value | 0.07 | 0.03 * | |
| Lt. % Swing phase | |||
| • Land | 36.63 [35.74,37.56] | 32.10 [31.66,33.27] | 0.02 * |
| • Water | 37.12 [36.67,37.46] | 34.66 [34.29,36.91] | 0.19 |
| Within-gr. p-value | 0.46 | 0.011 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Phothirook, P.; Amatachaya, S.; Peungsuwan, P. Muscle Activity and Co-Activation of Gait Cycle during Walking in Water and on Land in People with Spastic Cerebral Palsy. Int. J. Environ. Res. Public Health 2023, 20, 1854. https://doi.org/10.3390/ijerph20031854
Phothirook P, Amatachaya S, Peungsuwan P. Muscle Activity and Co-Activation of Gait Cycle during Walking in Water and on Land in People with Spastic Cerebral Palsy. International Journal of Environmental Research and Public Health. 2023; 20(3):1854. https://doi.org/10.3390/ijerph20031854
Chicago/Turabian StylePhothirook, Pariyaporn, Sugalya Amatachaya, and Punnee Peungsuwan. 2023. "Muscle Activity and Co-Activation of Gait Cycle during Walking in Water and on Land in People with Spastic Cerebral Palsy" International Journal of Environmental Research and Public Health 20, no. 3: 1854. https://doi.org/10.3390/ijerph20031854
APA StylePhothirook, P., Amatachaya, S., & Peungsuwan, P. (2023). Muscle Activity and Co-Activation of Gait Cycle during Walking in Water and on Land in People with Spastic Cerebral Palsy. International Journal of Environmental Research and Public Health, 20(3), 1854. https://doi.org/10.3390/ijerph20031854