
Similar Cognitive Skill Impairment in Children with Upper Limb Motor Disorders Due to Arthrogryposis Multiplex Congenita and Obstetrical Brachial Plexus Palsy

 ,
,
Abstract
1. Introduction
2. Methods
2.1. Patients and Control Participants
2.2. Assessment of Cognitive Functions and Motor Functions
2.3. Statistical Analysis
3. Results

{kind=link}
{kind=link}
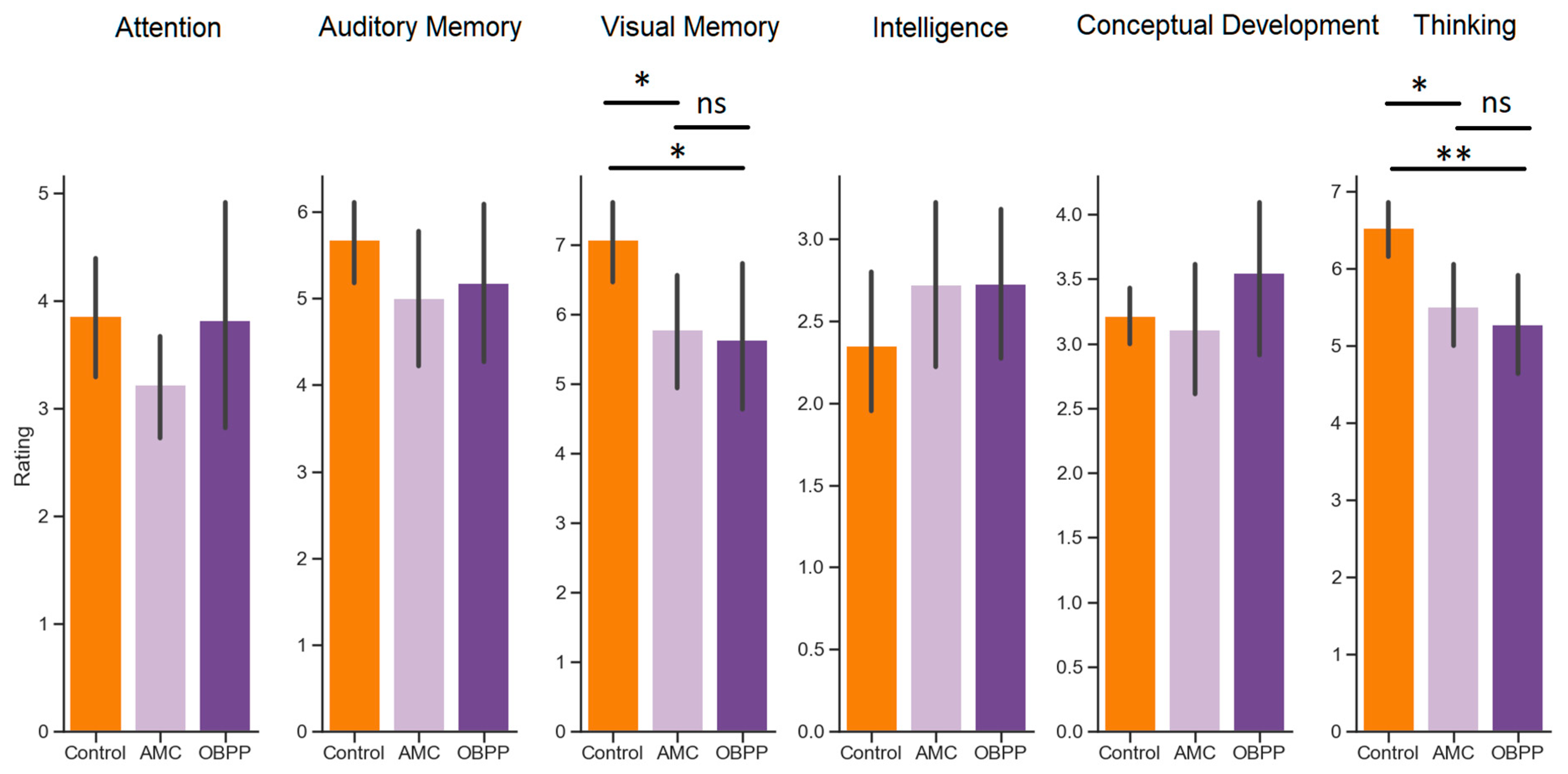
| Task | h | η2approximated | p |
|---|---|---|---|
| Attention | 2.38 | 0.04 | 1.000 |
| Auditory Memory | 1.83 | 0.03 | 1.000 |
| Visual Memory | 9.90 | 0.16 | 0.042 * |
| Intelligence | 1.62 | 0.03 | 1.000 |
| Conceptual Development | 2.65 | 0.05 | 1.000 |
| Thinking | 12.76 | 0.19 | 0.010 * |
4. Discussion
5. Conclusions
- Children with AMC and those with OBPP differ from healthy children in terms of cognitive skills, such as visual memory and thinking.
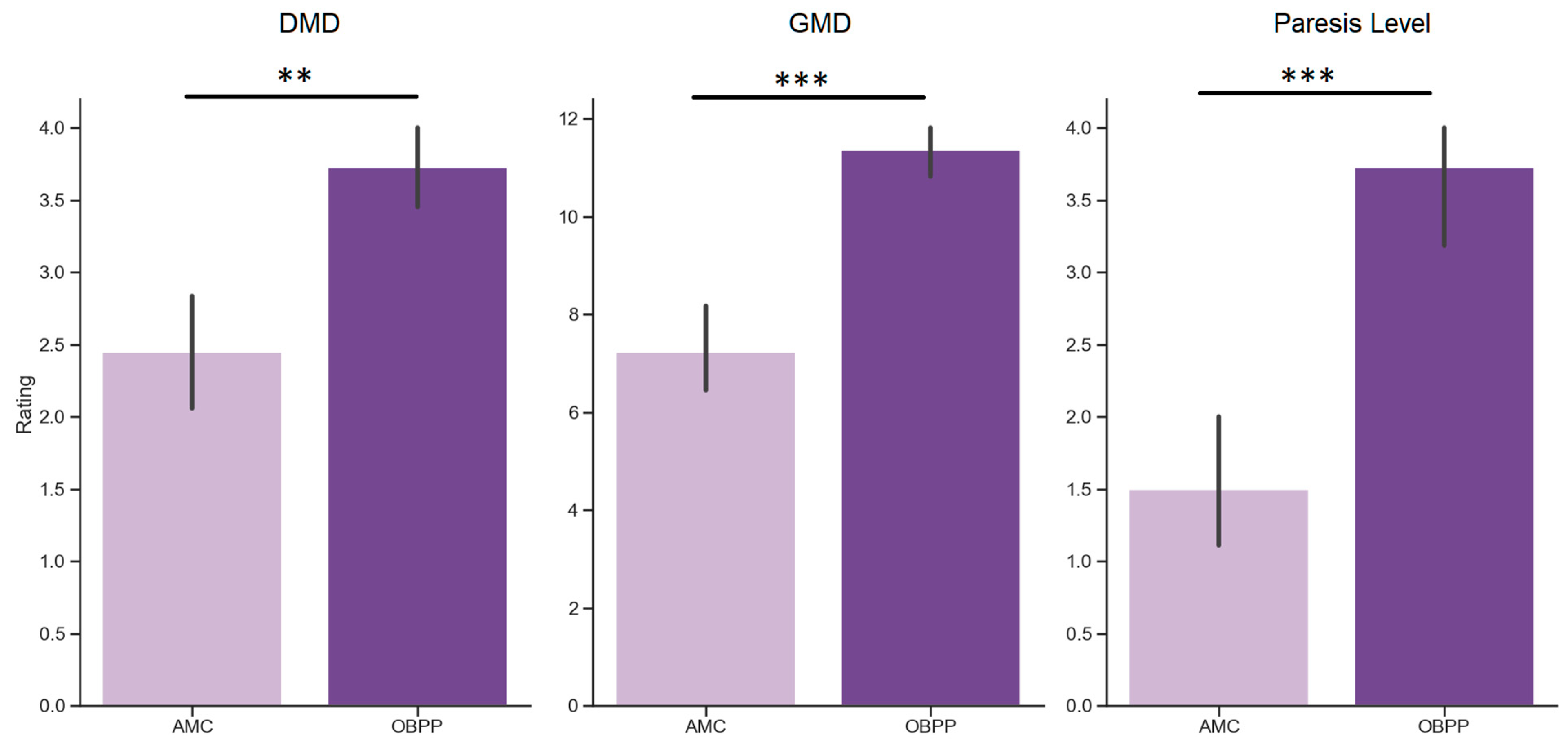
- Children with AMC and those with OBPP differ in terms of motor skills but not in cognitive tests.
- Presumably, the presence of a motor disease may be a more significant factor than its degree of manifestation in explaining cognitive deficits.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Libertus, K.; Hauf, P. Editorial: Motor skills and their foundational role for perceptual, social, and cognitive development. Front. Psychol. 2017, 8, 301. [Google Scholar] [CrossRef] [PubMed]
- Hauert, C.A. The relationship between motor function and cognition in the developmental perspective. Ital. J. Neurol. Sci. 1986, 5, 101–107. [Google Scholar]
- Iverson, J.M. Developing language in a developing body: The relationship between motor development and language development. J. Child Lang. 2010, 37, 229–261. [Google Scholar] [CrossRef] [PubMed]
- van der Fels, I.M.J.; Te Wierike, S.C.M.; Hartman, E.; Elferink-Gemser, M.T.; Smith, J.; Visscher, C. The relationship between motor skills and cognitive skills in 4-16 year old typically developing children: A systematic review. J. Sci. Med. Sport 2015, 18, 697–703. [Google Scholar] [CrossRef] [PubMed]
- Stöckel, T.; Hughes, C.M.L. The relation between measures of cognitive and motor functioning in 5- to 6-year-old children. Psychol. Res. 2016, 80, 543–554. [Google Scholar] [CrossRef]
- Abdelkarim, O.; Ammar, A.; Chtourou, H.; Wagner, M.; Knisel, E.; Hökelmann, A.; Bös, K. Relationship between motor and cognitive learning abilities among primary school-aged children. Alex. J. Med. 2019, 53, 325–331. [Google Scholar] [CrossRef]
- Blagovechtchenski, E.; Pettersson, L.G.; Perfiliev, S.; Krasnochokova, E.; Lundberg, A. Control of digits via C3-C4 propriospinal neurones in cats; recovery after lesions. Neurosci. Res. 2000, 38, 103–107. [Google Scholar] [CrossRef]
- Lemon, R.N. Descending Pathways in Motor Control. Annu. Rev. Neurosci. 2008, 31, 195–218. [Google Scholar] [CrossRef]
- Pettersson, L.G.; Alstermark, B.; Blagovechtchenski, E.; Isa, T.; Sasaski, S. Skilled digit movements in feline and primate-Recovery after selective spinal cord lesions. Proc. Acta Physiol. 2007, 189, 141–154. [Google Scholar] [CrossRef]
- Anderson, V.A.; Anderson, P.; Northam, E.; Jacobs, R.; Catroppa, C. Development of executive functions through late childhood and adolescence in an Australian sample. Dev. Neuropsychol. 2001, 20, 385–406. [Google Scholar] [CrossRef]
- Roebers, C.M.; Kauer, M. Motor and cognitive control in a normative sample of 7-year-olds. Dev. Sci. 2009, 12, 175–181. [Google Scholar] [CrossRef]
- Dahan-Oliel, N.; Cachecho, S.; Barnes, D.; Bedard, T.; Davison, A.M.; Dieterich, K.; Donohoe, M.; Fąfara, A.; Hamdy, R.; Hjartarson, H.T.; et al. International multidisciplinary collaboration toward an annotated definition of arthrogryposis multiplex congenita. Am. J. Med. Genet. C. Semin. Med. Genet. 2019, 181, 288–299. [Google Scholar] [CrossRef]
- Hall, J.G. Arthrogryposis multiplex congenita: Etiology, genetics, classification, diagnostic approach, and general aspects. J. Pediatr. Orthop. B 1997, 6, 159–166. [Google Scholar] [CrossRef]
- Komolkin, I.; Ulrich, E.V.; Agranovich, O.E.; van Bosse, H.J.P. Treatment of Scoliosis Associated With Arthrogryposis Multiplex Congenita. J. Pediatr. Orthop. 2017, 37 (Suppl. S1), S24–S26. [Google Scholar] [CrossRef]
- Trofimova, S.I.; Agranovich, O.E. Restoration of active forearm flexion in children with arthrogryposis:results of transfer of long head of triceps. Pediatr. Traumatol. Orthop. Reconstr. Surg. 2015, 3, 15. [Google Scholar] [CrossRef]
- Koriakina, M.; Agranovich, O.; Petrova, E.; Kadieva, D.; Kopytin, G.; Ermolovich, E.; Moiseenko, O.; Alekseeva, M.; Bredikhin, D.; Bermúdez-Margaretto, B.; et al. Aberrant Auditory and Visual Memory Development of Children with Upper Limb Motor Disorders. Brain Sci. 2021, 11, 1650. [Google Scholar] [CrossRef]
- Lin, Y.J.; Kao, T.W.; Chen, W.L. Relationship between peripheral neuropathy and cognitive performance in the elderly population. Medicine 2021, 100, e26071. [Google Scholar] [CrossRef]
- Piek, J.P.; Dawson, L.; Smith, L.M.; Gasson, N. The role of early fine and gross motor development on later motor and cognitive ability. Hum. Mov. Sci. 2008, 27, 668–681. [Google Scholar] [CrossRef]
- Belopolskaya, N.L. Exclusion of Objects (The Fourth Extra): A Modified Psychodiagnostic Technique: A Manual for Use, 3rd ed.; Stereotyped: Moscow, Russia, 2009. [Google Scholar]
- Murphy, K.R.; Myors, B. Statistical Power Analysis: A Simple and General Model for Traditional and Modern Hypothesis Tests: Second Edition; Routledge: London, UK, 2003; pp. 1–139. [Google Scholar] [CrossRef]
- Higashionna, T.; Iwanaga, R.; Tokunaga, A.; Nakai, A.; Tanaka, K.; Nakane, H.; Tanaka, G. Relationship between motor coordination, cognitive abilities, and academic achievement in Japanese children with neurodevelopmental disorders. Hong Kong J. Occup. Ther. 2017, 30, 49–55. [Google Scholar] [CrossRef]
- Zeng, N.; Ayyub, M.; Sun, H.; Wen, X.; Xiang, P.; Gao, Z. Effects of physical activity on motor skills and cognitive development in early childhood: A systematic review. Biomed Res. Int. 2017, 2017, 2760716. [Google Scholar] [CrossRef]
- Vygotsky, L.; Luria, A. Tool and Symbol in Child Development; Blackwell Publishers: Oxford, UK, 1978. [Google Scholar]
- Jenni, O.G.; Chaouch, A.; Caflisch, J.; Rousson, V. Correlations between motor and intellectual functions in normally developing children between 7 and 18 years. Dev. Neuropsychol. 2013, 38, 98–113. [Google Scholar] [CrossRef] [PubMed]
- Koziol, L.F.; Lutz, J.T. From movement to thought: The development of executive function. Appl. Neuropsychol. Child 2013, 2, 104–115. [Google Scholar] [CrossRef] [PubMed]
- Abd El-Hady, S.S.; Abd El-Azim, F.H.; El-Talawy, H.A.E.A.M. Correlation between cognitive function, gross motor skills and health–Related quality of life in children with Down syndrome. Egypt. J. Med. Hum. Genet. 2018, 19, 97–101. [Google Scholar] [CrossRef]
- Diamond, A. Close interrelation of motor development and cognitive development and of the cerebellum and prefrontal cortex. Child Dev. 2000, 71, 44–56. [Google Scholar] [CrossRef] [PubMed]
- Michel, G.F.; Campbell, J.M.; Marcinowski, E.C.; Nelson, E.L.; Babik, I. Infant Hand Preference and the Development of Cognitive Abilities. Front. Psychol. 2016, 7, 410. [Google Scholar] [CrossRef]
- Morse, A.F.; Benitez, V.L.; Belpaeme, T.; Cangelosi, A.; Smith, L.B. Posture Affects How Robots and Infants Map Words to Objects. PLoS ONE 2015, 10, e0116012. [Google Scholar] [CrossRef]
- Walle, E.A. Infant social development across the transition from crawling to walking. Front. Psychol. 2016, 7, 960. [Google Scholar] [CrossRef]
- Kenny, L.; Hill, E.; Hamilton, A.F. The Relationship between Social and Motor Cognition in Primary School Age-Children. Front. Psychol. 2016, 7, 228. [Google Scholar] [CrossRef]
- Anderson, D.I.; Lohse, K.R.; Lopes, T.C.V.; Williams, A.M. Individual differences in motor skill learning: Past, present and future. Hum. Mov. Sci. 2021, 78, 102818. [Google Scholar] [CrossRef]
- Magallón, S.; Narbona, J.; Crespo-Eguílaz, N. Acquisition of motor and cognitive skills through repetition in typically developing children. PLoS ONE 2016, 11, e0158684. [Google Scholar] [CrossRef]
- Sanders, K.Y. Overprotection and lowered expectations of persons with disabilities: The unforeseen consequences. Work 2006, 27, 181–188. [Google Scholar]
- Gere, M.K.; Villabø, M.A.; Torgersen, S.; Kendall, P.C. Overprotective parenting and child anxiety: The role of co-occurring child behavior problems. J. Anxiety Disord. 2012, 26, 642–649. [Google Scholar] [CrossRef]
- Kiel, E.J.; Maack, D.J. Maternal BIS Sensitivity, Overprotective Parenting, and Children’s Internalizing Behaviors. Pers. Individ. Dif. 2012, 53, 257–262. [Google Scholar] [CrossRef]
- Clarke, K.; Cooper, P.; Creswell, C. The parental overprotection scale: Associations with child and parental anxiety. J. Affect. Disord. 2013, 151, 618–624. [Google Scholar] [CrossRef]
- Nakamura, C.Y. The relationship between children’s expression of hostility and methods of discipline exercised by dominant overprotective parents. Child Dev. 1959, 30, 109–117. [Google Scholar] [CrossRef]
- Blagovechtchenski, E.; Agranovich, O.; Kononova, Y.; Nazarova, M.; Nikulin, V.V. Perspectives for the Use of Neurotechnologies in Conjunction With Muscle Autotransplantation in Children. Front. Neurosci. 2019, 13, 99. [Google Scholar] [CrossRef]
- Blagoveschenskiy, E.D.; Agranovich, O.E.; Kononova, E.L.; Baindurashvili, A.G.; Nazarova, M.A.; Shestokova, A.N.; Gabbasova, E.L.; Nikulin, V.V. Characteristics of electrophysiological activity of the cerebral cortex in children with arthrogryposis. Nervn. Bolezn. 2018, 8, 25–32. [Google Scholar] [CrossRef]
- Golosheykin, S.A.; Blagoveschenskiy, E.D.; Agranovich, O.E.; Nazarova, M.A.; Nikulin, V.V.; Moiseenko, O.E.; Chan, R.W.; Shestakova, A.N. Feasibility and Challenges of Performing Magnetoencephalography Experiments in Children With Arthrogryposis Multiplex Congenita. Front. Pediatr. 2021, 9, 626734. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Blagovechtchenski, E.; Koriakina, M.; Bredikhin, D.; Agranovich, O.; Kadieva, D.; Ermolovich, E.; Jääskeläinen, I.P.; Shestakova, A.N. Similar Cognitive Skill Impairment in Children with Upper Limb Motor Disorders Due to Arthrogryposis Multiplex Congenita and Obstetrical Brachial Plexus Palsy. Int. J. Environ. Res. Public Health 2023, 20, 1841. https://doi.org/10.3390/ijerph20031841
Blagovechtchenski E, Koriakina M, Bredikhin D, Agranovich O, Kadieva D, Ermolovich E, Jääskeläinen IP, Shestakova AN. Similar Cognitive Skill Impairment in Children with Upper Limb Motor Disorders Due to Arthrogryposis Multiplex Congenita and Obstetrical Brachial Plexus Palsy. International Journal of Environmental Research and Public Health. 2023; 20(3):1841. https://doi.org/10.3390/ijerph20031841
Chicago/Turabian StyleBlagovechtchenski, Evgeny, Maria Koriakina, Dimitri Bredikhin, Olga Agranovich, Dzerassa Kadieva, Evgenia Ermolovich, Iiro P. Jääskeläinen, and Anna N. Shestakova. 2023. "Similar Cognitive Skill Impairment in Children with Upper Limb Motor Disorders Due to Arthrogryposis Multiplex Congenita and Obstetrical Brachial Plexus Palsy" International Journal of Environmental Research and Public Health 20, no. 3: 1841. https://doi.org/10.3390/ijerph20031841
APA StyleBlagovechtchenski, E., Koriakina, M., Bredikhin, D., Agranovich, O., Kadieva, D., Ermolovich, E., Jääskeläinen, I. P., & Shestakova, A. N. (2023). Similar Cognitive Skill Impairment in Children with Upper Limb Motor Disorders Due to Arthrogryposis Multiplex Congenita and Obstetrical Brachial Plexus Palsy. International Journal of Environmental Research and Public Health, 20(3), 1841. https://doi.org/10.3390/ijerph20031841