
Retraction of Clinical Trials about the SARS-CoV-2 Infection: An Unaddressed Problem and Its Possible Impact on Coronavirus Disease (COVID)-19 Treatment

 and
and
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
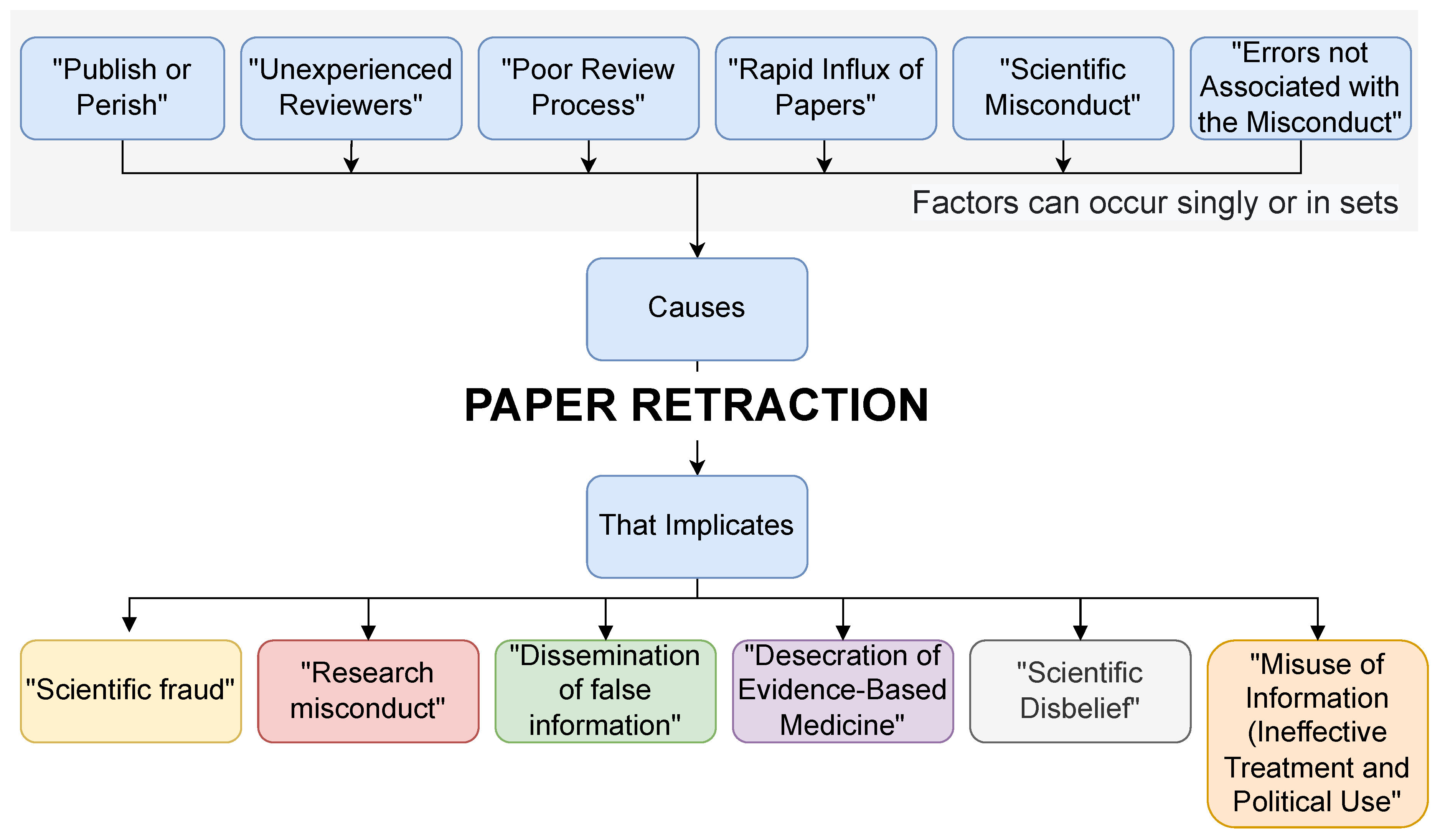
- (1)
- This was due to pressure to publish, which, despite not being demonstrated empirically for any of these articles, is a valid possibility and further studies are to elucidate this possibility.
- (2)
- That retractions are due to insufficient peer review, which implies that skilled reviewers can detect randomization errors, research misconduct, and similar minor errors resulting in work that is not reproducible. It is unclear whether skilled and experienced reviewers would request raw data from the studies or be able to detect some of the issues identified as the cause of retractions upon review.
- (3)
- That the rapid influx of papers causes retractions. In this sense, due to the urgency for new information and possible treatment for a new deadly disease, all researchers turned to COVID-19. This converged in a high number of articles being submitted simultaneously.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Carvalho, T.; Lima, T.; Melani, V.; Mendes, M.; Pereira, L.; Marson, F.A.L. The scientific production during 2009 swine flu pandemic and 2019/2020 COVID-19 pandemic. Pulmonology 2020, 26, 340–345. [Google Scholar] [CrossRef] [PubMed]
- Valencise, F.E.; Boschiero, M.N.; Palamim, C.V.C.; Marson, F.A.L. The COVID-19 impact on the scientific production on the 25 main death causes according to world region. Pulmonology 2022, 28, 1–3. [Google Scholar] [CrossRef]
- Yeo-Teh, N.S.L.; Tang, B.L. An alarming retraction rate for scientific publications on Coronavirus Disease 2019 (COVID-19). Account. Res. 2021, 28, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Anderson, C.; Nugent, K.; Peterson, C. Academic Journal Retractions and the COVID-19 Panemic. J. Prim. Care Community Health 2021, 12, 21501327211015592. [Google Scholar] [CrossRef] [PubMed]
- Fang, F.C.; Casadevall, A. Retracted science and the retraction index. Infect. Immun. 2011, 79, 3855–3859. [Google Scholar] [CrossRef] [PubMed]
- Bar-Ilan, J.; Halevi, G. Temporal characteristics of retracted articles. Scientometrics 2018, 116, 1771–1783. [Google Scholar] [CrossRef]
- Marcus, M.A.; Abritis, A.J.; Oransky, M.I. How to Stop the Unknowing Citation of Retracted Papers. Anesthesiology 2022, 137, 280–282. [Google Scholar] [CrossRef]
- Boschiero, M.N.; Carvalho, T.A.; Marson, F.A.D.L. Retraction in the era of COVID-19 and its influence on evidence-based medicine: Is science in jeopardy? Pulmonology 2021, 27, 97–106. [Google Scholar] [CrossRef] [PubMed]
- Samaha, A.; Mouawia, H.; Fawaz, M.; Hassan, H.; Salami, A.; Bazzal, A.; Saab, H.; Al-Wakeel, M.; Alsaabi, A.; Chouman, M.; et al. Effects of a Single Dose of Ivermectin on Viral and Clinical Outcomes in Asymptomatic SARS-CoV-2 Infected Subjects: A Pilot Clinical Trial in Lebanon. Viruses 2021, 13, 989, Retraction on Viruses 2021, 13, 2154. [Google Scholar] [CrossRef]
- Lakkireddy, M.; Gadiga, S.G.; Malathi, R.D.; Karra, M.L.; Raju, I.S.S.V.P.M.; Ragini; Chinapaka, S.; Baba, K.S.S.S.; Kandakatla, M. Impact of daily high dose oral vitamin D therapy on the inflammatory markers in patients with COVID-19 disease. Sci. Rep. 2021, 11, 10641, Retraction on Sci. Rep. 2022, 12, 6487. [Google Scholar] [CrossRef]
- McCoy, J.; Goren, A.; Cadegiani, F.A.; Vaño-Galván, S.; Kovacevic, M.; Situm, M.; Shapiro, J.; Sinclair, R.; Tosti, A.; Stanimirovic, A.; et al. Proxalutamide Reduces the Rate of Hospitalization for COVID-19 Male Outpatients: A Randomized Double-Blinded Placebo-Controlled Trial. Front. Med. (Lausanne) 2021, 8, 668698, Retraction on Front. Med. (Lausanne) 2022, 9, 964099. [Google Scholar] [CrossRef] [PubMed]
- Dabbous, H.M.; El-Sayed, M.H.; El Assal, G.; Elghazaly, H.; Ebeid, F.F.S.; Sherief, A.F.; Elgaafary, M.; Fawzy, E.; Hassany, S.M.; Riad, A.R.; et al. Safety and efficacy of favipiravir versus Hydroxychloroquine in management of COVID-19: A randomised controlled trial. Sci. Rep. 2021, 11, 7282, Retraction on Sci. Rep. 2021, 11, 18983. [Google Scholar] [CrossRef] [PubMed]
- Dabbous, H.M.; Abd-Elsalam, S.; El-Sayed, M.H.; Sherief, A.F.; Ebeid, F.F.S.; El Ghafar, M.S.A.; Soliman, S.; Elbahnasawy, M.; Badawi, R.; Tageldin, M.A. Efficacy of favipiravir in COVID-19 treatment: A multi-center randomized study. Arch. Virol. 2021, 166, 949–954, Retraction on Arch. Virol. 2022, 167, 277. [Google Scholar] [CrossRef] [PubMed]
- Abd-Elsalam, S.; Ahmed, O.A.; Mansour, N.O.; Abdelaziz, D.H.; Salama, M.; Fouad, M.H.A.; Soliman, S.; Naguib, A.M.; Hantera, M.S.; Ibrahim, I.S.; et al. Remdesivir Efficacy in COVID-19 Treatment: A Randomized Controlled Trial. Am. J. Trop. Med. Hyg. 2021, 106, 886–890, Retraction on Am. J. Trop. Med. Hyg. 2022, 107, 1. Epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Abd-Elsalam, S.; Esmail, E.S.; Khalaf, M.; Abdo, E.F.; Medhat, M.A.; El Ghafar, M.S.A.; Ahmed, O.A.; Soliman, S.; Serangawy, G.N.; Alboraie, M. Hydroxychloroquine in the treatment of COVID-19: A multi-center randomized controlled study. Am. J. Trop. Med. Hyg. 2020, 103, 1635–1639, Retraction on Am. J. Trop. Med. Hyg. 2022, 107, 1. Epub ahead of print. [Google Scholar] [CrossRef]
- El-Bendary, M.; Abd-Elsalam, S.; Elbaz, T.; El-Akel, W.; Cordie, A.; Elhadidy, T.; Elalfy, H.; Farid, K.; Elegezy, M.; El-Badrawy, A.; et al. Efficacy of combined Sofosbuvir and Daclatasvir in the treatment of COVID-19 patients with pneumonia: A multi-center Egyptian study. Expert Rev. Anti Infect. Ther. 2022, 20, 291–295, Retraction on Expert Rev. Anti Infect. Ther. 2022, 20, 1243. [Google Scholar] [CrossRef]
- Bolland, M.J.; Grey, A.; Avenell, A. Citation of retracted publications: A challenging problem. Account. Res. 2022, 29, 18–25. [Google Scholar] [CrossRef]
- Boschiero, M.N.; Palamim, C.V.C.; Ortega, M.M.; Mauch, R.M.; Marson, F.A.L. One Year of Coronavirus Disease 2019 (COVID-19) in Brazil: A Political and Social Overview. Ann. Glob. Health 2021, 87, 44. [Google Scholar] [CrossRef]
- Morshed, T.; Hayden, S. Google Versus PubMed: Comparison of Google and PubMed’s Search Tools for Answering Clinical Questions in the Emergency Department. Ann. Emerg. Med. 2020, 75, 408–415. [Google Scholar] [CrossRef]
- Alessi, J.; Becker, A.S.; Amaral, B.; de Oliveira, G.B.; Franco, D.W.; Knijnik, C.P.; Kobe, G.L.; de Brito, A.; de Carvalho, T.R.; Telo, G.H.; et al. Type 1 diabetes and the challenges of emotional support in crisis situations: Results from a randomized clinical trial of a multidisciplinary teleintervention. Sci. Rep. 2022, 12, 3086, Retraction on Sci. Rep. 2022, 12, 4265. [Google Scholar] [CrossRef]
- Guzman-Prado, Y. Retraction of Studies on Potential Drug Therapies for COVID-19: A Call for Reliability and Scientific Integrity. Am. J. Cardiol. 2020, 132, 173. [Google Scholar] [CrossRef] [PubMed]
- Frampton, G.; Woods, L.; Scott, D.A. Inconsistent and incomplete retraction of published research: A cross-sectional study on Covid-19 retractions and recommendations to mitigate risks for research, policy, and practice. PloS ONE 2021, 16, e0258935. [Google Scholar] [CrossRef] [PubMed]
- Marson, F.; Ortega, M. COVID-19 in Brazil. Pulmonology 2020, 26, 241–244. [Google Scholar] [CrossRef]
- Kataoka, Y.; Banno, M.; Tsujimoto, Y.; Ariie, T.; Taito, S.; Suzuki, T.; Oide, S.; Furukawa, T.A. Retracted randomized controlled trials were cited and not corrected in systematic reviews and clinical practice guidelines. J. Clin. Epidemiol. 2022, 150, 90–97. [Google Scholar] [CrossRef]
- Ambrosino, N.; Pacini, F. Publish or perish? Perish to publish? (Unrequested advices to young researchers). Pulmonology 2022, 28, 327–329. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Study Type by Indexation in PubMed * | Clinical Trials (COVID-19-Related)—8445 Studies (A) | Clinical Trials (non-COVID-19-Related)—202,398 Studies (B) ** | Proportion between the Percentages from (A) and (B) *** |
|---|---|---|---|
| Clinical trial phases | |||
| I | 142 (1.68%) | 4774 (2.36%) | 0.71 |
| II | 250 (2.96%) | 7426 (3.67%) | 0.81 |
| III | 156 (1.85%) | 5445 (2.69%) | 0.69 |
| IV | 17 (0.20%) | 594 (0.29%) | 0.69 |
| Clinical trial protocol | 549 (6.50%) | 7942 (3.92%) | 1.66 |
| Randomized clinical trial | 2086 (24.70%) | 92,111 (45.51%) | 0.54 |
| Retracted clinical trials | 8 (0.11%) | 111 (0.05%) | 1.73 |
| Study | First Author Country | Journal | Impact Factor |
|---|---|---|---|
| Effects of a single dose of Ivermectin on viral and clinical outcomes in asymptomatic SARS-CoV-2 infected subjects: A pilot clinical trial in Lebanon [9] | Lebanon | Viruses | 5.818 |
| Impact of daily high dose oral vitamin D therapy on the inflammatory markers in patients with COVID-19 disease [10] | India | Scientific Reports | 4.996 |
| Proxalutamide reduces the rate of hospitalization for COVID-19 male outpatients: a randomized double-blinded placebo-controlled trial [11] * | United States of America | Frontiers in Medicine | 5.058 |
| Safety and efficacy of Favipiravir versus Hydroxychloroquine in management of COVID-19: A randomized controlled trial [12] | Egypt | Scientific Reports | 4.996 |
| Efficacy of Favipiravir in COVID-19 treatment: a multi-center randomized study [13] | Egypt | Archives of Virology | 2.685 |
| Remdesivir efficacy in COVID-19 treatment: A randomized controlled trial [14] | Egypt | American Journal of Tropical Medicine and Hygiene | 2.345 |
| Hydroxychloroquine in the treatment of COVID-19: A multi-center randomized controlled study [15] | Egypt | American Journal of Tropical Medicine and Hygiene | 2.345 |
| Efficacy of combined Sofosbuvir and Daclatasvir in the treatment of COVID-19 patients with pneumonia: a multi-center Egyptian study [16] | Egypt | Expert Review of Anti-Infective Therapy | 5.091 |
| Study | Objective | Methods (Intervention, Study Design, and Outcomes) | Results and Conclusion | Retraction Notes | Altmetric * | |
|---|---|---|---|---|---|---|
| Clinical Trial | Retraction Note | |||||
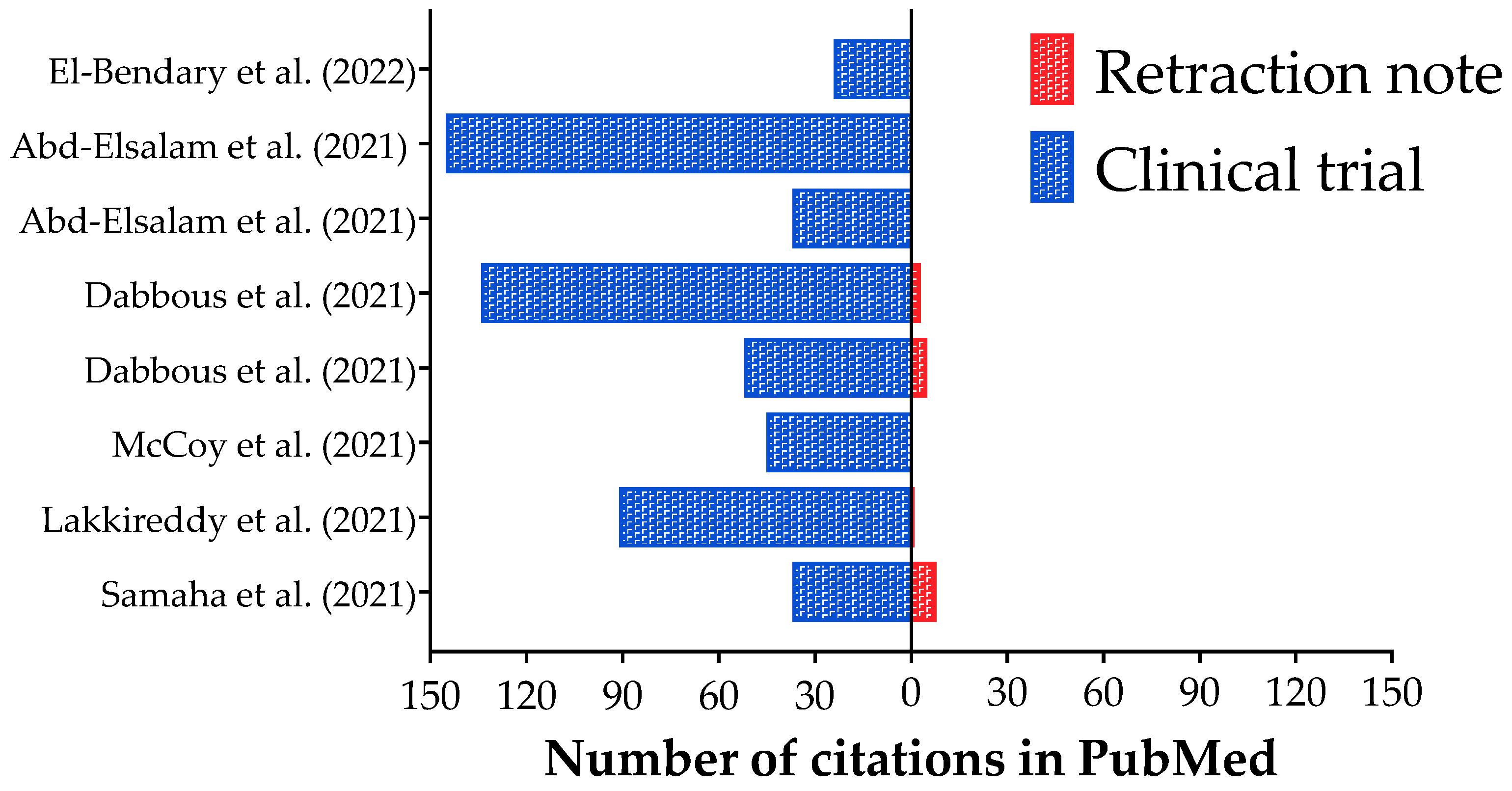
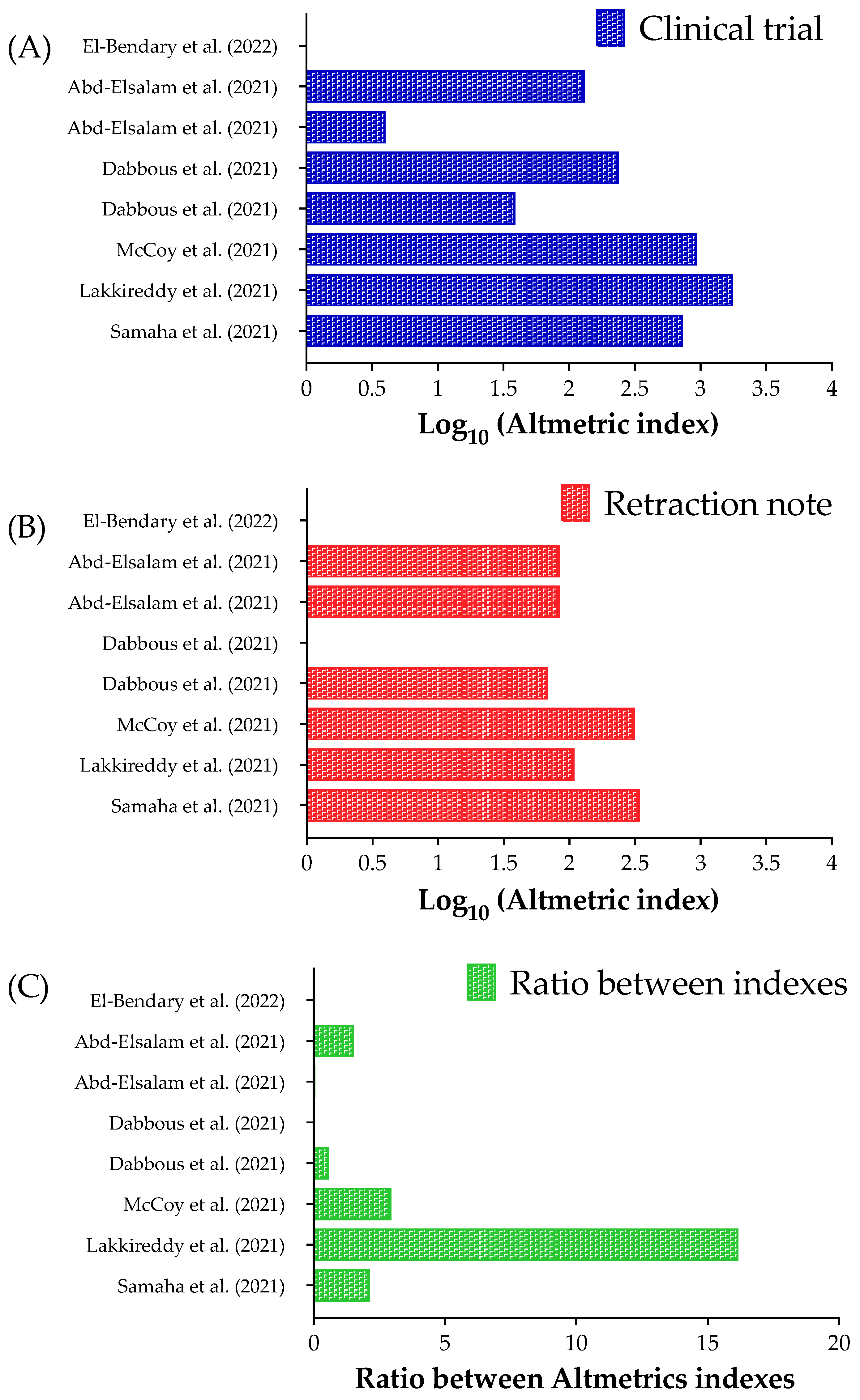
| [9] | Determine the efficacy of Ivermectin, an Food and Drug Administration-approved drug, in producing clinical benefits and decreasing the viral load of SARS-CoV-2 among asymptomatic participants that tested positive for SARS-CoV-2 in Lebanon. | A randomized controlled trial was conducted on 100 asymptomatic Lebanese participants who tested positive for SARS-CoV-2. Fifty patients received standard preventive treatment, mainly supplements. The experimental group received a single dose (according to body weight) of Ivermectin and the same supplements the control group received. | 72 h after the treatment regimen started, the increase in Ct-values was higher in the Ivermectin than in the control group. Moreover, more participants in the control group developed clinical symptoms. Three individuals (6%) from this study group required hospitalization—Ivermectin group (0%). In this context, Ivermectin appears to be efficacious in providing clinical benefits in a randomized treatment of asymptomatic SARS-CoV-2-positive participants, effectively resulting in fewer symptoms, lower viral load, and reduced hospital admissions. | After the publication, the authors contacted the editorial office regarding an error between files used for the statistical analysis. In adhering to the complaints procedure from the journal, an investigation confirmed the error reported by the authors. The Editor approved the retraction. Also, the authors agreed to this retraction. | 736 (37 citations in PubMed) | 344 (eight citations in PubMed) |
| [10] | Investigate the impact of Pulse D therapy in reducing the inflammatory markers of COVID-19. | Consented COVID-19 participants with hypovitaminosis D were evaluated for inflammatory markers [neutrophil/lymphocyte ratio, C-reactive protein, lactate dehydrogenase, Interleukin-6, and Ferritin] along with vitamin D on the first day and 9th/11th days as per their respective body mass index category. Subjects were randomized into vitamin D and non-vitamin D groups. The Vitamin D group received Pulse D therapy (targeted daily supplementation of 60,000 IUs of vitamin D for eight or ten days depending upon their body mass index) in addition to the standard treatment. Non-vitamin D group received standard therapy alone. | Eighty-seven out of one hundred and thirty subjects have completed the study (vitamin D: 44, and non-vitamin D: 43). Vitamin D level has increased from 16 ± 6 ng/mL to 89 ± 32 ng/mL after Pulse D therapy in vitamin D group and was associated with a significant reduction of the measured inflammatory markers; the reduction of these markers in non-vitamin D group was insignificant. The difference in the reduction of markers between the study groups was also significant. | After publication, concerns were raised about several aspects of the study: at baseline, there are significant differences in the parameters measured, indicating that randomization may not have been performed correctly. Post-publication peer review has confirmed that the alternative allocation method was inappropriate for randomized clinical trials. This means that the patients were not precisely randomized; therefore, the differences in outcome between the two arms cannot be attributed to the Pulse D therapy only. | 1763 (91 citations in PubMed) | 109 (one citation in Pubmed) |
| [11] | Determine if Proxalutamide, an androgen receptor antagonist, could be an effective treatment for men with COVID-19 in an outpatient setting. | A randomized, double-blinded, and a placebo-controlled clinical trial was conducted at two outpatient centers (Brasilia, Brazil). Male participants with confirmed COVID-19 but not requiring hospitalization (8-point ordinal scale < 3) were administered Proxalutamide 200 mg/day or placebo for up to seven days. The primary endpoint was the hospitalization rate at 30 days post-randomization. A total of 268 men were randomized in a 1:1 ratio: 134 received Proxalutamide, and 134 received a placebo. The participants were included in the intention-to-treat analysis. | The 30-day hospitalization rate was 2.2% in men taking Proxalutamide when compared to 26% in placebo. The 30-day hospitalization risk ratio was 0.09 (95%CI = 0.03–0.27). Patients in the Proxalutamide arm more frequently reported gastrointestinal adverse events; however, no patient discontinued treatment. In the placebo group, six patients were lost during follow-up, and two participants died from acute respiratory distress syndrome. The study demonstrated that the hospitalization rate in Proxalutamide-treated men was reduced by 91% when compared to usual care. | After publication, the journal received letters of complaint questioning the integrity of the article, following which an Expression of Concern was published. A thorough investigation was conducted following policies and Committee on Publication Ethics guidelines. The investigation found that the methods did not adequately support the claims made in the conclusions. Mainly, the allocation to treatment and control groups was not sufficiently random. | 936 (45 citations in PubMed) | 316 (No citation in PubMed) |
| [12] | Explore the safety and efficacy of Favipiravir in the treatment of COVID-19 mild and moderate cases. | The authors performed a randomized-controlled open-label interventional phase 3 clinical trial. One hundred patients were recruited from 18th April till 18th May. Fifty participants received Favipiravir 3200 mg on day 1, followed by 600 mg twice (day 2-day 10). Fifty participants received Hydroxychloroquine 800 mg on day 1, followed by 200 mg twice (days 2–10) and oral Oseltamivir 75 mg/12 h/day for ten days. Participants were enrolled in Ain Shams University Hospital and Assiut University Hospital. Both arms were comparable as regards demographic characteristics and comorbidities. | The average onset of SARS-CoV-2 PCR (polymerase chain reaction) negativity was 8.1 and 8.3 days in the Hydroxychloroquine-arm and Favipiravir-arm, respectively: 55.1% of those on the Hydroxychloroquine-arm turned PCR negative at/or before the 7th day from diagnosis when compared to 48% on the Favipiravir-arm. Four patients in the Favipiravir arm developed transient transaminitis. On the other hand, heartburn and nausea were reported in about 20 participants in Hydroxychloroquine-arm. Only one patient in Hydroxychloroquine-arm died after developing acute myocarditis, which resulted in acute heart failure. Favipiravir was considered a safe and effective alternative to Hydroxychloroquine in mild or moderate COVID-19-infected patients. | Concerns were brought to the Editors’ attention after publication, and the study’s raw data were requested. The authors provided several versions of their dataset. Post-publication peer review confirmed that none of these versions fully recapitulates the results presented in the cohort background comparisons, casting doubt on the reliability of the data. Additional concerns were raised about the randomization procedure, as the equal distribution of male and female patients is unlikely unless sex is a parameter considered during randomization. However, based on the clarification provided by the authors, sex was not considered during this process. The Editors, therefore, no longer have confidence in the results and conclusions presented. | 39 (52 citations in PubMed) | 68 (Five citations in PubMed) |
| [13] | Evaluate the efficacy of Favipiravir in the treatment of patients with COVID-19. | A multi-center, randomized, interventional phase 2/3 study that included participants with COVID-19 was performed. Ninety-eight participants were eligible to participate. After excluding participants who refused to participate, 96 participants were randomly assigned into two groups. The Chloroquine group included 48 participants who received Chloroquine 600 mg tablets twice daily added to the standard-of-care therapy for ten days. The Favipiravir group included 48 participants who received 1600 mg of Favipiravir twice a day on the first day and 600 mg twice daily from the second to the tenth day, added to the standard-of-care therapy for ten days. Four participants in this group quit after the beginning of the study, and the final number in this group was 44. The four patients who left the study preferred to complete their treatment and be transferred to military hospitals, after which the authors lost contact with them. | Although not statistically significant, the Favipiravir group had a lower mean duration of hospital stay than the Chloroquine group (13.29 ± 5.86 vs. 15.89 ± 4.75 days). None of the participants in the Favipiravir group needed mechanical ventilation or had an oxygen saturation < 90%, but these differences were insignificant when compared to the Chloroquine group. Four patients in the Chloroquine group required mechanical ventilation and received Methylprednisolone after their condition worsened. Two patients (4.2%) in the Chloroquine group and one (2.3%) in the Favipiravir group died; however, no significant differences were observed between the groups regarding side effects. The patient’s age and C-reactive protein level were the only factors significantly associated with mortality, and Favipiravir treatment was not significantly related to COVID-19 mortality. The authors concluded that Favipiravir is a promising drug for the treatment of COVID-19 that might decrease the hospital stay and the need for mechanical ventilation. | After publication, concerns were raised about reporting this clinical trial, and the authors were asked to provide their raw data files. The raw data was examined. First, the reported baseline variables showed that the distribution of one variable was highly statistically different in the two study groups. Second, two variables showed different rounding to significant figures in the two groups. Third, for two variables, there was a different distribution of the variables when moving through the groups. It is unclear how these variations could occur in a correctly performed trial, so severe doubts about the randomization process and data validity arose. These doubts were reinforced by the equal sex distribution even though sex was not stated as an inclusion parameter. | 239 (134 citations in PubMed) | 0 (Three citations in PubMed) |
| [14] | To assess the efficacy of Remdesivir in hospitalized Egyptian patients with COVID-19. | Patients were randomly assigned at a 1:1 ratio to receive either Remdesivir in addition to standard care or standard care alone. Two hundred patients (100 in each group) completed the study and were included in the final analysis. | The Remdesivir group showed a significantly lower median duration of hospital stay than the control group (10 vs. 16 days). Eleven patients in the Remdesivir group needed mechanical ventilation when compared with eight patients in the control group. The mortality rate was comparable between the two groups; however, it was significantly associated with older age, elevated C-reactive protein levels, elevated D-dimer, and the need for mechanical ventilation. Remdesivir positively influenced the length of hospital stay, but it had no mortality benefit. | Data overlap and copying were described. Second, the authors have not provided a reasonable explanation for this significant problem. Third, adequate data error-checking or validation has not been provided to ensure that the results presented in the paper accurately represent the sourced data. The journal lost confidence in the totality of the data. Because of this and insufficient answers to repeated inquiries, the journal retracted the article. | Four (37 citations in PubMed) | 85 (No citation in PubMed) |
| [15] | The authors aimed to evaluate the safety and efficacy of Hydroxychloroquine added to standard care in patients with COVID-19. | A multi-center, randomized controlled trial was conducted at three major university hospitals in Egypt. One hundred ninety-four patients with a confirmed diagnosis of COVID-19 were included. They were equally randomized into two arms: 97 patients administrated Hydroxychloroquine plus standard care, and 97 patients administered only standard care as a control arm. The primary endpoints were recovery within 28 days, need for mechanical ventilation, or death. The two groups were matched for age and sex, and there was no significant difference between them regarding baseline characteristics or laboratory parameters. | Four patients (4.1%) in the Hydroxychloroquine group and five (5.2%) in the control group needed mechanical ventilation. The overall mortality did not differ between the two groups, as six patients (6.2%) died in the Hydroxychloroquine group, and five (5.2%) died in the control group. Univariate logistic regression analysis showed that Hydroxychloroquine treatment was not significantly associated with decreased mortality in patients with COVID-19. So, adding Hydroxychloroquine to standard care did not add significant benefit, did not decrease the need for ventilation, and did not reduce mortality rates. | Data overlap and copying were described. Second, the authors have not provided a reasonable explanation for this significant problem. Third, adequate data error-checking or validation has not been provided to ensure that the results presented in the paper accurately represent the sourced data. The journal lost confidence in the totality of the data. Because of this and insufficient answers to repeated inquiries, the journal retracted the article. | 131 (145 citations in PubMed) | 85 (No citation in PubMed) |
| [16] | The study evaluated the efficacy of generic Sofosbuvir/Daclatasvir in treating patients with COVID-19 who presented with pneumonia. | This multi-center prospective study involved 174 patients with COVID-19. Patients were randomized into two groups. Group A (96 patients) received Sofosbuvir (400 mg)/Daclatasvir (60 mg) for 14 days in combination with conventional therapy. Group B (78 patients) received conventional therapy alone. Clinical, laboratory, and radiological data were collected at baseline and after 7, 14, and 28 days of therapy. The primary endpoint was the rate of clinical/virological cure. | A lower mortality rate was observed in Group A (14 vs. 21%). After one month of therapy, no differences were found in intensive care unit admission rates, oxygen therapy, or ventilation. Additionally, a statistically significant shorter duration of hospital stay (9 vs. 12%) and a faster achievement of PCR negativity at day 14 (84 vs. 47%) were noticed in Group A. | Since publication, concerns were raised about the integrity of the data and reported results. When approached for an explanation, the authors could not address the concerns raised and could not provide sufficient supporting information. As verifying the validity of published work is core to the integrity of the scholarly record, the article was retracted. The corresponding author listed in this publication was informed. The authors disagree with the retraction. | One (24 citations in PubMed) | 0 (No citation PubMed) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Valencise, F.E.; Palamim, C.V.C.; Marson, F.A.L. Retraction of Clinical Trials about the SARS-CoV-2 Infection: An Unaddressed Problem and Its Possible Impact on Coronavirus Disease (COVID)-19 Treatment. Int. J. Environ. Res. Public Health 2023, 20, 1835. https://doi.org/10.3390/ijerph20031835
Valencise FE, Palamim CVC, Marson FAL. Retraction of Clinical Trials about the SARS-CoV-2 Infection: An Unaddressed Problem and Its Possible Impact on Coronavirus Disease (COVID)-19 Treatment. International Journal of Environmental Research and Public Health. 2023; 20(3):1835. https://doi.org/10.3390/ijerph20031835
Chicago/Turabian StyleValencise, Felipe Eduardo, Camila Vantini Capasso Palamim, and Fernando Augusto Lima Marson. 2023. "Retraction of Clinical Trials about the SARS-CoV-2 Infection: An Unaddressed Problem and Its Possible Impact on Coronavirus Disease (COVID)-19 Treatment" International Journal of Environmental Research and Public Health 20, no. 3: 1835. https://doi.org/10.3390/ijerph20031835
APA StyleValencise, F. E., Palamim, C. V. C., & Marson, F. A. L. (2023). Retraction of Clinical Trials about the SARS-CoV-2 Infection: An Unaddressed Problem and Its Possible Impact on Coronavirus Disease (COVID)-19 Treatment. International Journal of Environmental Research and Public Health, 20(3), 1835. https://doi.org/10.3390/ijerph20031835