






Encouraging and Reinforcing Safe Breastfeeding Practices during the COVID-19 Pandemic

Abstract
1. Introduction
2. Materials and Methods
- (i)
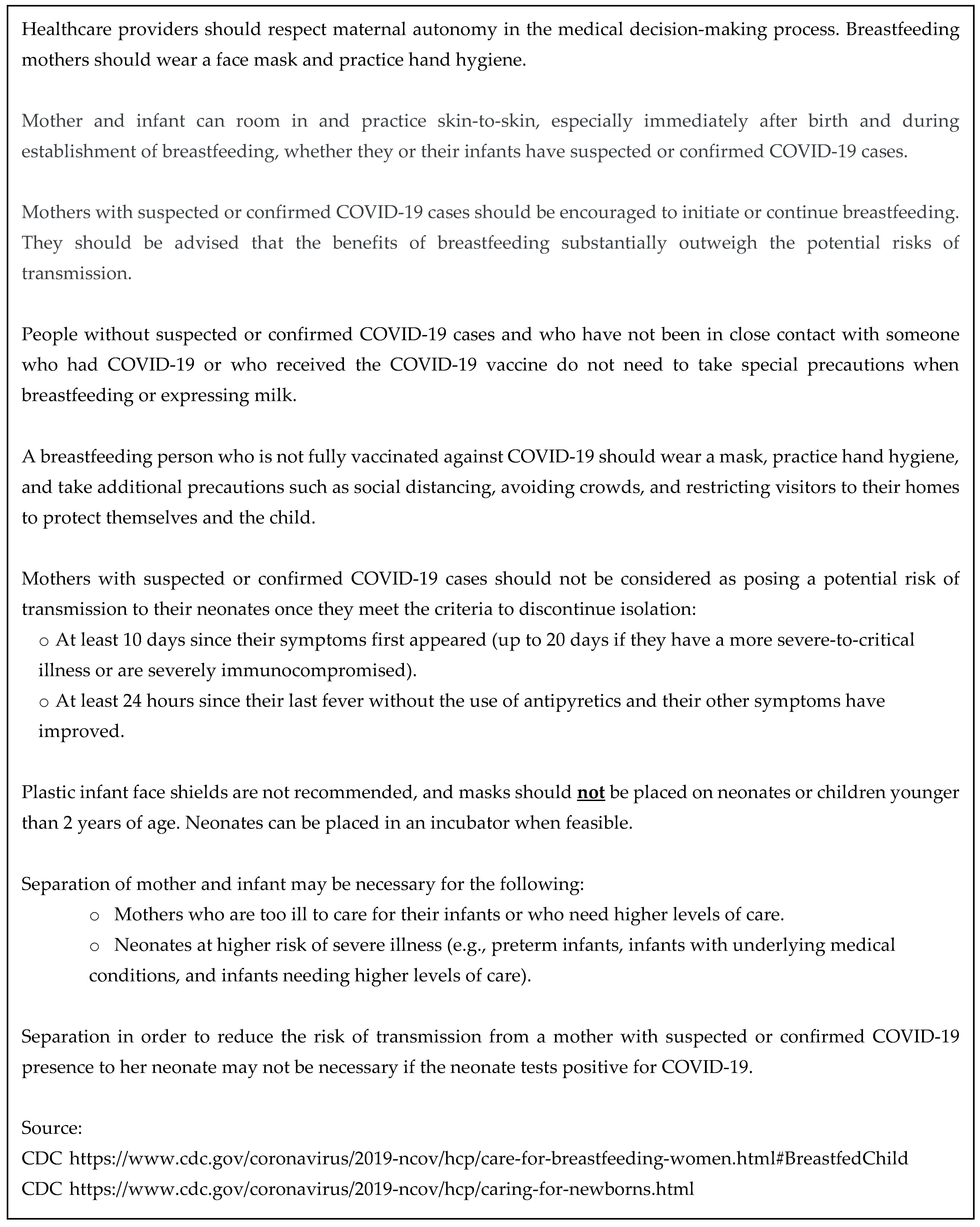
- Participants received a six-panel breastfeeding brochure with a two-panel COVID-19 safe breastfeeding insert (Supplementary Materials).
- (ii)
- Participants were advised to discuss breastfeeding during the pandemic with their obstetrician and to request referral to a certified lactation counselor for breastfeeding evaluation and training.
- (iii)
- Participants were encouraged to call the program educator or PI for breastfeeding support as needed.
- (i)
- Group I: Mothers recruited from December 2019 to June 2020 (early pandemic period).
- (ii)
- Group II: Pregnant Women recruited from July 2020 to August 2021 (later pandemic period).
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lau, H.; Khosrawipour, V.; Kocbach, P.; Mikolajczyk, A.; Schubert, J.; Bania, J.; Khosrawipour, T. The positive impact of lockdown in Wuhan on containing the COVID-19 outbreak in China. J. Travel Med. 2020, 27, taaa037. [Google Scholar] [CrossRef] [PubMed]
- Iacobucci, G. COVID-19: UK lockdown is “crucial” to saving lives, say doctors and scientists. Br. Med. J. 2020, 368, m1204. [Google Scholar] [CrossRef] [PubMed]
- Habibzadeh, F.; Lang, T. The Coronavirus Pandemic: “The Show Must NOT Go On”. Int. J. Occup. Environ. Med. 2020, 11, 63–64. [Google Scholar] [CrossRef] [PubMed]
- Tennessee Government: Stay Home as Much as Possible. Available online: https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/prevention.html (accessed on 19 October 2020).
- CDC. Coronavirus Disease (COVID-19) and Breastfeeding. Division of Nutrition, Physical Activity, and Obesity, National Center for Chronic Disease Prevention and Health Promotion. Available online: https://www.cdc.gov/breastfeeding/breastfeeding-special-circumstances/maternal-or-infant-illnesses/covid-19-and-breastfeeding.html (accessed on 25 March 2020).
- World Health Organization. WHO Guidelines. Pandemic and Epidemic Diseases. Infection Prevention and Control of Epidemic- and Pandemic-Prone Acute Respiratory Infections in Health Care. Guideline I; World Health Organization: Geneva, Switzerland, 2014; ISBN 978-92-4-150713-4. Available online: http://apps.who.int/iris/bitstream/10665/112656/1/9789241507134_eng.pdf (accessed on 26 March 2020).
- Dooling, K. COVID-19 Vaccine Recommendations; CDC Publication: New York, NY, USA, 6 January 2020. Available online: https://www2.cdc.gov/vaccines/ed/ciinc/archives/covid/downloads/1_6/COVID_19_ACIPrecommendations.pdf (accessed on 5 June 2020).
- FDA; U.S. Food & Drug Administration. FDA Approves First COVID-19 Vaccine. Approval Signifies Key Achievement for Public Health. News Release. 23 August 2021. Available online: https://www.fda.gov/news-events/press-announcements/fda-approves-first-covid-19-vaccine (accessed on 1 October 2021).
- Centers for Disease Control and Prevention. Interim Guidelines for Collecting, Handling, and Testing Clinical Specimens from Persons for Coronavirus Disease 2019 (COVID-19). Available online: https://www.cdc.gov/coronavirus/2019-nCoV/lab/guidelines-clinical-specimens.html (accessed on 5 December 2021).
- Nekhlyudov, L.; Mollica, M.; Jacobsen, P.; Mayer, D.; Shulman, L.; Geiger, A. Developing a Quality of Cancer Survivorship Care Framework: Implications for Clinical Care, Research, and Policy. J. Natl. Cancer Inst. 2019, 111, 1120–1130. [Google Scholar] [CrossRef] [PubMed]
- McLeroy, K.R.; Bibeau, D.; Steckler, A.; Glanz, K. An Ecological Perspective on Health Promotion Programs. Health Educ. Q. 1988, 15, 351–377. [Google Scholar] [CrossRef]
- CDC. Risk for COVID-19 Infection, Hospitalization, and Death by Race/Ethnicity. 2 June 2022. National Center for Immunization and Respiratory Diseases (NCIRD), Division of Viral Diseases. Available online: https://www.cdc.gov/coronavirus/2019-ncov/covid-data/investigations-discovery/hospitalization-death-by-race-ethnicity.html (accessed on 11 November 2022).
- Castetbon, K.; Boudet-Berquier, J.; Salanave, B. Combining breastfeeding and work: Findings from the Epifane population-based birth cohort. BMC Pregnancy Childbirth 2020, 20, 110. [Google Scholar] [CrossRef]
- Al-Kuwari, M.G.; Al-Nuaimi, A.A.; Abdulmajeed, J.; Semaan, S.; Al-Romaihi, H.E.; Kandy, M.C. COVID-19 infection across workplace settings in Qatar: A comparison of COVID-19 positivity rates of screened workers from March 1st until July 31st, 2020. J. Occup. Med. Toxicol. 2021, 16, 21. [Google Scholar] [CrossRef]
- Cummings, K.J.; Beckman, J.; Frederick, M.; Harrison, R.; Nguyen, A.; Snyder, R.; Chan, E.; Gibb, K.; Rodriguez, A.; Wong, J.; et al. Disparities in COVID-19 fatalities among working Californians. PLoS ONE 2022, 17, e0266058. [Google Scholar] [CrossRef]
- Burdorf, A.; Porru, F.; Rugulies, R. The COVID-19 pandemic: One year later–An occupational perspective. Scand. J. Work. Environ. Health 2021, 47, 245–247. [Google Scholar] [CrossRef]
- Gholami, M.; Fawad, I.; Shadan, S.; Rowaiee, R.; Ghanem, H.; Khamis, A.H.; Ho, S.B. COVID-19 and healthcare workers: A systematic review and meta-analysis. Int. J. Infect. Dis. 2021, 104, 335–346. [Google Scholar] [CrossRef]
- Lauer, E.A.; Armenti, K.; Henning, M.; Sirois, L. Identifying Barriers and Supports to Breastfeeding in the Workplace Experienced by Mothers in the New Hampshire Special Supplemental Nutrition Program for Women, Infants, and Children Utilizing the Total Worker Health Framework. Int. J. Environ. Res. Public Health 2019, 16, 529. [Google Scholar] [CrossRef] [PubMed]
- Al-Imari, L.; Hum, S.; Krueger, P.; Dunn, S. Breastfeeding during Family Medicine Residency. Fam. Med. 2019, 51, 587–592. [Google Scholar] [CrossRef] [PubMed]
- Morain, S.; Schoen, L.; Marty, M.; Schwarz, E.B. Parental Leave, Lactation, and Childcare Policies at Top US Schools of Public Health. Am. J. Public Health. 2019, 109, 722–728. [Google Scholar] [CrossRef] [PubMed]
- Rimes, K.A.; Oliveira, M.I.C.; Boccolini, C.S. Maternity leave and exclusive breastfeeding. Rev. Saude Publica 2019, 53, 10. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Shin, J.C.; Donovan, S.M. Effectiveness of Workplace Lactation Interventions on Breastfeeding Outcomes in the United States: An Updated Systematic Review. J. Hum. Lact. 2019, 35, 100–113. [Google Scholar] [CrossRef] [PubMed]
- Le Huërou-Luron, I.; Blat, S.; Boudry, G.B.V. Formula-feeding: Impacts on the digestive tract and immediate and long-term health effects. Nutr. Res. Rev. 2010, 23, 23–36. [Google Scholar] [CrossRef] [PubMed]
- van den Bogaard, C.; van den Hoogen, H.J.; Huygen, F.J.; van Weel, C. The relationship between breast-feeding and early childhood morbidity in a general population. Fam. Med. 1991, 23, 510–515. [Google Scholar]
- Hanson, L.A.; Hahn-Zoric, M.; Berndes, M.; Ashraf, R.; Herias, V.; Jalil, F.; Bhutta, T.I.; Laeeq, A.; Mattsby-Baltzer, I. Breast feeding: Overview and breast milk immunology. Acta Paediatr Jpn. 1994, 36, 557–561. [Google Scholar] [CrossRef] [PubMed]
- Deubel, T.F.; Miller, E.M.; Hernandez, I.; Boyer, M.; Louis-Jacques, A. Perceptions and Practices of Infant Feeding among African American Women. Ecol. Food Nutr. 2019, 58, 301–316. [Google Scholar] [CrossRef]
- Hofvander, Y. Breastfeeding and the Baby Friendly Hospitals Initiative: Organization, response and outcome in Sweden and other countries. Acta Paediatr. 2005, 94, 1012–1016. [Google Scholar] [CrossRef]
- Gross, T.T.; Powell, R.; Anderson, A.K.; Hall, J.; Davis, M.; Hilyard, K. WIC peer counselors’ perceptions of breastfeeding in African American women with lower incomes. J. Hum. Lact. 2015, 31, 99–110. [Google Scholar] [CrossRef]
- Labbok, M.H. Global baby-friendly hospital initiative monitoring data: Update and discussion. Breastfeed Med. 2012, 7, 210–222. [Google Scholar] [CrossRef] [PubMed]
- Brodribb, W.; Kruske, S.; Miller, Y.D. Baby-friendly hospital accreditation, in-hospital care practices, and breastfeeding. Pediatrics 2013, 131, 685–692. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, S.S.; Stern, A.D.; Baum, C.F.; Gillman, M.W. Evaluating the impact of the Baby-Friendly Hospital Initiative on breast-feeding rates: A multi-state analysis. Public Health Nutr. 2015, 18, 189–197. [Google Scholar] [CrossRef]
- Pérez-Escamilla, R.; Martinez, J.L.; Segura-Pérez, S. Impact of the Baby-friendly Hospital Initiative on breastfeeding and child health outcomes: A systematic review. Matern. Child Nutr. 2016, 12, 402–417. [Google Scholar] [CrossRef] [PubMed]
- Apple, R.D. The medicalization of infant feeding in the United States and New Zealand: Two countries, one experience. J. Hum. Lact. 1994, 1091, 31–37. [Google Scholar] [CrossRef]
- Wright, A.L. The rise of breastfeeding in the U.S. Pediatr. Clin. N. Am. 2001, 48, 1–12. [Google Scholar] [CrossRef]
- Gartner, L.M.; Morton, J.; Lawrence, R.A.; Naylor, A.J.; O’Hare, D.; Schanler, R.J.; Eidelman, A.I.; American Academy of Pediatrics Section on Breastfeeding. For the Academy of Pediatrics Section on Breastfeeding. Breastfeeding and human milk. Pediatrics 2005, 115, 496–506. [Google Scholar]
- WHO; UNICEF; Swedish International Development Agency. Innocenti Declaration on the Protection, Promotion and Support of Breastfeeding; UNICEF: New York, NY, USA, 1990. [Google Scholar]
- The AAFP Breastfeeding, Family Physicians Supporting (Position Paper). Available online: http://www.aafp.org/online/en/home/policy/policies/b/breastfeedingpositionpaper.html (accessed on 2 September 2021).
- The AAFP Breastfeeding (Policy Statement). Available online: http://www.aafp.org/online/en/home/policy/policies/b/breastfeedingpolicy.html (accessed on 2 September 2021).
- The AAFP Maternal/Child Care: Hospital Use of Infant Formula in Breastfeeding Infants. Available online: http://www.aafp.org/online/en/home/policy/policies/h/hospuseinfantformulabreastfeeding.html (accessed on 2 September 2021).
- U.S. Prev. Services Task Force. Primary care interventions to promote breastfeeding: U.S. Preventive Services Task Force recommendation statement. Ann. Int. Med. 2008, 149, 560–565. [Google Scholar] [CrossRef]
- CDC. Questionnaires: Breastfeeding and Infant feeding Practices. Content Source: Division of Nutrition, Physical Activity, and Obesity, National Center for Chronic Disease Prevention and Health Promotion Page Last Reviewed: 10 August 2021. Available online: https://www.cdc.gov/breastfeeding/data/ifps/questionnaires.htm (accessed on 29 July 2021).
- The CDC Breastfeeding Report Card Was First Released in 2007 and Is Updated Annually. Indicator Data Sources and National Immunization Survey Statistical Information. Available online: www.cdc.gov/breastfeeding/data/ (accessed on 14 July 2021).
- Vassilopoulou, E.; Feketea, G.; Koumbi, L.; Mesiari, C.; Berghea, E.C.; Konstantinou, G.N. Breastfeeding and COVID-19: From Nutrition to Immunity. Front. Immunol. 2021, 12, 661806. [Google Scholar] [CrossRef]
- del C, N.; Contreras-Carreto, N.A.; Rojas-Bernabé, A.; Mancilla-Ramíre, J. Breastfeeding and COVID-19. Gac. Med. Mex. 2021, 157, 194–200. [Google Scholar] [CrossRef]
- Lubbe, W.; Botha, E.; Niela-Vilen, H.; Reimers, P. Breastfeeding during the COVID-19 pandemic-A literature review for clinical practice. Int. Breastfeed J. 2020, 15, 82. [Google Scholar] [CrossRef] [PubMed]
- Green, L.W.; Kreuter, M.W.; Deeds, S.G.; Partridge, K.D. Health Education Planning: A Diagnostic Approach; Mountain View: Mayfield, CA, USA, 1980. [Google Scholar]
- Green, L.W.; Kreuter, M.W. Health Education Planning: An Educational and Ecological Approach; Mountain View: Mayfield, CA, USA, 1991. [Google Scholar]
- Glanz, K.; Rimer, B.K.; Lewis, F.M. Health Behavior and Health Education: Theory, Research, and Practice, 3rd ed.; Jossey-Bass: San Francisco, CA, USA, 2002; pp. 462–484. [Google Scholar]
- Kothari, A.R.; Birch, S. Multilevel health promotion research: Conceptual and analytical considerations. Can. J. Nurs. Res. 2004, 36, 56–75. [Google Scholar]
- Joosten, Y.A.; Israel, T.L.; Williams, N.A.; Boone, L.R.; Schlundt, D.G.; Mouton, C.P.; Dittus, R.S.; Bernard, G.R.; Wilkins, C.H. Community Engagement Studios: A structured approach to obtaining meaningful input from stakeholders to inform research. Acad. Med. 2015, 90, 1646–1650. [Google Scholar] [CrossRef] [PubMed]
- WHO. Questionnaire for Breastfeeding Mothers. Baby-Friendly Hospital Initiative: Revised Updated and Expanded for Integrated Care; World Health Organization: Geneva, Switzerland, 2009; pp. 72–75. ISBN 978-92-4-159495-0. Available online: https://www.ncbi.nlm.nih.gov/books/NBK153471/ (accessed on 19 February 2022).
- Chambers, D.A. Considering the intersection between implementation science and COVID-19. Implement Res Pract. 2020, 1, 1. [Google Scholar] [CrossRef]
- Ward, E.; Jemal, A.; Cokkinides, V.; Singh, G.K.; Cardinez, C.; Ghafoor, A.; Thun, M. Cancer disparities by race/ethnicity and socioeconomic status. CA Cancer J. Clin. 2004, 54, 78–93. [Google Scholar] [CrossRef]
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; Bacon, S.; Bates, C.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Inglesby, P.; et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature 2020, 584, 430–436. [Google Scholar] [CrossRef]
- Calil, V.M.L.T.; Krebs, V.L.J.; de Carvalho, W.B. Guidance on breastfeeding during the COVID-19 pandemic. Rev. Assoc. Med. Bras. 2020, 66, 541–546. [Google Scholar] [CrossRef]
- Fernández-Carrasco, F.J.; Vázquez-Lara, J.M.; González-Mey, U.; Gómez-Salgado, J.; Parrón-Carreño, T.; Rodríguez-Díaz, L. Coronavirus COVID-19 infection and breastfeeding: An exploratory review. Rev. Esp. Salud. Publica 2020, 94, e202005055. (In Spanish) [Google Scholar]
- Pereira, A.; Cruz-Melguizo, S.; Adrien, M.; Fuentes, L.; Marin, E.; Forti, A.; Perez-Medina, T. Breastfeeding mothers with COVID-19 infection: A case series. Int. Breastfeed J. 2020, 15, 69. [Google Scholar] [CrossRef]
- Brown, A.; Shenker, N. Experiences of breastfeeding during COVID-19: Lessons for future practical and emotional support. Matern. Child Nutr. 2021, 17, e13088. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, H. Should COVID-19 Mother Breastfeed her Newborn Child? A Literature Review on the Safety of Breastfeeding for Pregnant Women with COVID-19. Curr. Nutr. Rep. 2021, 10, 71–75. [Google Scholar] [CrossRef]
- Palacios, R.; Patiño, E.G.; Piorelli, R.D.O.; Conde, M.T.R.P.; Batista, A.P.; Zeng, G.; Xin, Q.; Kallas, E.G.; Flores, J.; Ockenhouse, C.F.; et al. Double-Blind, Randomized, Placebo-Controlled Phase III Clinical Trial to Evaluate the Efficacy and Safety of treating Healthcare Professionals with the Adsorbed COVID-19 (Inactivated) Vaccine Manufactured by Sinovac-PROFISCOV: A structured summary of a study protocol for a randomised controlled trial. Trials 2020, 21, 853. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Martins, I.; Louwen, F.; Ayres-de-Campos, D.; Mahmood, T. EBCOG position statement on COVID-19 vaccination for pregnant and breastfeeding women. Eur. J. Obstet. Gynecol. Reprod. Biol. 2021, 262, 256–258. [Google Scholar] [CrossRef]
- Mayo, S.; Monfort, S. Letter to the Editor: Breastfeeding and COVID-19 Vaccine: Yes We Can. J. Hum. Lact. 2021, 37, 275–276. [Google Scholar] [CrossRef]
- McLaurin-Jiang, S.; Garner, C.; Krutsch, K.; Hale, T. Maternal and Child Symptoms Following COVID-19 Vaccination among Breastfeeding Mothers. Breastfeed Med. 2021, 16, 702–709. [Google Scholar] [CrossRef] [PubMed]
- Perl, S.H.; Uzan-Yulzari, A.; Klainer, H.; Asiskovich, L.; Youngster, M.; Rinott, E.; Youngster, I. SARS-CoV-2-Specific Antibodies in Breast Milk After COVID-19 Vaccination of Breastfeeding Women. J. Am. Med. Assoc. 2021, 325, 2013–2014. [Google Scholar] [CrossRef] [PubMed]
- Hall, S. COVID vaccines and breastfeeding: What the data say. Nature 2021, 594, 492–494. [Google Scholar] [CrossRef]
- Sutton, D.; D’Alton, M.; Zhang, Y.; Kahe, K.; Cepin, A.; Goffman, D.; Staniczenko, A.; Yates, H.; Burgansky, A.; Coletta, J.; et al. COVID-19 vaccine acceptance among pregnant, breastfeeding, and nonpregnant reproductive-aged women. Am. J. Obstet. Gynecol. MFM 2021, 3, 100403. [Google Scholar] [CrossRef]
- Hannula, L.; Kaunonen, M.; Tarkka, M.T. A systematic review of professional support interventions for breastfeeding. J. Clin. Nurs. 2008, 17, 1132–1143. [Google Scholar] [CrossRef]
- Jones, S.R.; Stoppard, M. Baby friendly hospitals: Are we failing mothers who formula feed their babies? J. Fam. Health Care 2011, 21, 12–14. [Google Scholar]
- Abul-Fadl, A.M.; Shawky, M.; El-Taweel, A.; Cadwell, K.; Turner-Maffei, C. Evaluation of mothers’ knowledge, attitudes, and practice towards the ten steps to successful breastfeeding in Egypt. Breastfeed Med. 2012, 7, 173–178. [Google Scholar] [CrossRef]
- Attanasio, L.; Kozhimannil, K.B.; McGovern, P.; Gjerdingen, D.; Johnson, P.J. The impact of prenatal employment on breastfeeding intentions and breastfeeding status at 1 week postpartum. J. Hum. Lact. 2013, 29, 620–628. [Google Scholar] [CrossRef] [PubMed]
- Declercq, E.R.; Sakala, C.; Corry, M.P.; Applebaum, S.; Herrlich, A. Major Survey Findings of Listening to Mothers (SM) III: New Mothers Speak Out: Report of National Surveys of Women’s Childbearing Experiences Conducted October-December 2012 and January–April 2013. J. Perinat. Educ. 2014, 23, 17–24. [Google Scholar] [CrossRef]
- Neifert, M.; Lawrence, R.; Seacat, J. Nipple confusion: Toward a formal definition. J. Pediatr. 1995, 126, S125–S129. [Google Scholar] [CrossRef] [PubMed]
- Zimmerman, E.; Thompson, K. Clarifying nipple confusion. J. Perinatol. 2015, 35, 895–899. [Google Scholar] [CrossRef] [PubMed]
- Fabiyi, C.; Peacock, N.; Hebert-Beirne, J.; Handler, A. A Qualitative Study to Understand Nativity Differences in Breastfeeding Behaviors Among Middle-Class African American and African-Born Women. Matern. Child Health J. 2016, 20, 2100–2111. [Google Scholar] [CrossRef] [PubMed]
- Olaiya, O.; Dee, D.L.; Sharma, A.J.; Smith, R.A. Maternity Care Practices and Breastfeeding Among Adolescent Mothers Aged 12–19 Years--United States, 2009–2011. MMWR. Morb. Mortal. Wkly. 2016, 65, 17–22. [Google Scholar] [CrossRef]
- Hawkins, S.S.; Stern, A.D.; Baum, C.F.; Gillman, M.W. Compliance with the Baby-Friendly Hospital Initiative and impact on breastfeeding rates. Arch. Dis. Child. Fetal Neonatal Ed. 2014, 99, F138–F143. [Google Scholar] [CrossRef]
- Reddin, E.; Pincombe, J.; Darbyshire, P. Passive resistance: Early experiences of midwifery students/ graduates and the Baby Friendly Health Initiative 10 steps to successful breastfeeding. Women Birth. 2007, 20, 71–76. [Google Scholar] [CrossRef]
- Kakrani, V.A.; Rathod Waghela, H.K.; Mammulwar, M.S.; Bhawalkar, J.S. Awareness about “Ten Steps for Successful Breastfeeding” among Medical and Nursing Students. Int. J. Prev. Med. 2015, 6, 40. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Study Population | Total | ||
|---|---|---|---|---|
| Group I § Early Pandemic | Group II §§ Later Pandemic | No. | % | |
| Age in years * | ||||
| <21 | 4 (10.3) | 14 (14.4) | 18 | 13.2 |
| 21–34 | 25 (64.1) | 74 (76.3) | 99 | 72.8 |
| >34 | 10 (25.6) | 9 (9.3) | 19 | 14.0 |
| Education | ||||
| High School | 21 (53.9) | 52 (53.6) | 73 | 53.7 |
| Some College | 5 (12.8) | 22 (22.7) | 27 | 19.8 |
| College Degree | 13 (33.3) | 23 (23.7) | 36 | 26.5 |
| Marital Status * | ||||
| Single | 26 (66.7) | 80 (82.5) | 106 | 77.9 |
| Married | 13 (33.3) | 17 (17.5) | 30 | 22.1 |
| Employment | ||||
| Unemployed | 14 (35.9) | 24 (24.7) | 38 | 27.9 |
| Part-Time | 5 (12.8) | 29 (29.9) | 34 | 25.0 |
| Full-Time | 20 (51.3) | 44 (45.4) | 64 | 47.1 |
| Income ** | ||||
| <USD 25,000 | 16 (41.0) | 33 (34.0) | 49 | 36.0 |
| USD 25,000–49,999 | 14 (35.9) | 19 (19.6) | 33 | 24.3 |
| >USD 50,000 | 8 (20.5) | 13 (13.4) | 21 | 15.4 |
| Not Stated | 1 (2.6) | 32 (33.0) | 33 | 24.3 |
| Nutrition assistance * | ||||
| WIC # and SNAP ## | 19 (48.7) | 26 (26.8) | 45 | 33.1 |
| WIC or SNAP | 12 (30.8) | 37 (38.1) | 49 | 36.0 |
| None | 8 (20.5) | 24 (35.1) | 42 | 30.5 |
| Work Return Plan | ||||
| <4 Weeks | 4 (10.3) | 7 (7.2) | 11 | 8.1 |
| 4–7 Weeks | 8 (20.5) | 27 (27.8) | 35 | 25.7 |
| 8–12 Weeks | 9 (23.1) | 32 (33.0) | 41 | 30.1 |
| ≥13 Weeks | 5 (12.8) | 8 (8.2) | 13 | 9.6 |
| Not Working | 13 (33.3) | 23 (23.7) | 36 | 26.5 |
| Daycare Use Plan *** | ||||
| Yes | 4 (10.3) | 29 (29.9) | 33 | 24.3 |
| No | 35 (89.7) | 44 (45.4) | 79 | 58.1 |
| Undecided | 0 (0.00) | 24 (24.7) | 24 | 17.6 |
| Characteristics | Study Population | Total | ||
|---|---|---|---|---|
| Group I Early Pandemic | Group II Later Pandemic | No. | % | |
| Privacy at work to breastfeed | ||||
| Among working mothers * | 10 (41.7) | 47 (64.4) | 57 | 58.2 |
| Breastfeeding experience | ||||
| Was breastfed | 13 (33.3) | 28 (28.9) | 41 | 30.1 |
| Witnessed mother | 9 (23.1) | 17 (17.5) | 26 | 19.1 |
| Witnessed mother or relatives | 12 (30.8) | 37 (38.1) | 49 | 36.0 |
| Witnessed friend | 16 (41.0) | 32 (33.0) | 48 | 35.3 |
| Witnessed anybody | 24 (61.5) | 69 (71.1) | 93 | 68.4 |
| Breastfed previous baby | ||||
| <1 month | 9 (23.1) | 24 (24.7) | 33 | 24.3 |
| 1–5 months | 9 (23.1) | 21 (21.6) | 30 | 22.1 |
| ≥6 months | 9 (23.1) | 12 (12.4) | 21 | 15.4 |
| No previous baby | 12 (30.8) | 40 (41.2) | 52 | 38.2 |
| Referral | ||||
| WIC | 26 (74.3) | 22 (57.9) | 48 | 65.8 |
| CLC | 19 (54.3) | 15 (39.5) | 34 | 46.6 |
| COVID-19 breastfeeding | 12 (34.3) | 10 (26.3) | 22 | 30.1 |
| Breastfeeding goal | ||||
| None or undecided | 19 (48.7) | 50 (51.5) | 69 | 50.7 |
| 3–5 months | 9 (23.1) | 21 (21.7) | 30 | 22.1 |
| ≥6 months | 11 (28.2) | 26 (26.8) | 37 | 27.2 |
| Formula plan | ||||
| At birth or undecided | 19 (48.7) | 65 (67.0) | 84 | 61.8 |
| Before 6 months | 10 (25.7) | 12 (12.3) | 22 | 16.2 |
| ≥6 months | 5 (12.8) | 6 (6.2) | 11 | 8.1 |
| No formula | 5 (12.8) | 14 (14.4) | 19 | 14.0 |
| # COVID-19 BF knowledge. | ||||
| Fair or correct | 19 (48.7) | 59 (60.8) | 78 | 57.4 |
| Incorrect or do not know | 20 (51.3) | 38 (39.2) | 58 | 42.6 |
| Information source ** | ||||
| Media, self, friend, or family | 20 (51.3 | 57 (58.8) | 77 | 56.6 |
| Doctor, nurse, or CLC | 4 (10.3) | 17 (17.5) | 21 | 15.4 |
| Not recorded | 15 (38.5) | 23 (23.7) | 38 | 27.9 |
| Characteristics | Study Population | Total | ||
|---|---|---|---|---|
| Group I Early Pandemic | Group II Later Pandemic | No. | % | |
| Facemask at home | ||||
| Never | 29 (74.4) | 85 (87.6) | 114 | 83.8 |
| Guests visiting | 6 (15.4) | 8 (8.2) | 14 | 10.3 |
| Holding baby | 3 (7.7) | 1 (1.0) | 4 | 2.9 |
| Almost always | 1 (2.6) | 3 (3.1) | 4 | 2.9 |
| Face mask shopping ** | ||||
| Never or sometimes | 7 (18.0) | 8 (8.3) | 15 | 11.0 |
| Most always | 32 (82.1) | 89 (91.7) | 121 | 89.0 |
| COVID-19 safety action | ||||
| Mother outings limited | 17 (43.6) | 49 (50.5) | 66 | 48.5 |
| Hands washed or sanitized | 17 (43.6) | 45 (46.4) | 62 | 45.6 |
| Visitors restricted | 11 (28.2) | 33 (34.0) | 44 | 32.4 |
| Baby outings avoided | 6 (15.4) | 21 (21.6) | 27 | 19.9 |
| Vaccinated | 0 (0.0) | 8 (8.2) | 8 | 5.9 |
| COVID-19 testing | ||||
| Not testing | 14 (35.9) | 57 (58.8) | 71 | 52.2 |
| Negative test | 21 (53.8) | 36 (37.1) | 57 | 41.2 |
| Positive with no symptoms | 0 (0.0) | 1 (1.0) | 1 | 0.7 |
| Positive with symptoms | 4 (13.0) | 3 (3.1) | 7 | 5.1 |
| Breastfeeding Knowledge Topic | Study Population | Total | ||
|---|---|---|---|---|
| Group I 2019–2020 | Group II 2020–2021 | No. | % | |
| Health contraindications *** | ||||
| Yes | 24 (61.5) | 33 (34.0) | 57 | 41.5 |
| No | 15 (38.5) | 28 (28.9) | 43 | 31.6 |
| Do not know | 0 (0.0) | 36 (37.1) | 36 | 26.5 |
| Drug contraindications ** | ||||
| Yes | 28 (71.8) | 53 (54.6) | 81 | 59.6 |
| No | 11 (28.2) | 26 (26.8) | 37 | 27.2 |
| Do not know | 0 (0.0) | 18 (18.6) | 18 | 13.2 |
| Specific health contraindication | ||||
| HIV ** | 14 (35.9) | 12 (12.4) | 26 | 19.1 |
| Breast cancer | 7 (17.9) | 16 (16.5) | 23 | 16.9 |
| COVID-19 with symptoms *** | 11 (28.2) | 5 (5.2) | 16 | 11.8 |
| COVID-19 with no symptoms ** | 6 (15.4) | 3 (3.1) | 9 | 6.6 |
| Mental illness (severe) ** | 6 (15.4) | 2 (2.1) | 8 | 5.9 |
| Specific drug contraindication | ||||
| Cocaine * | 21 (53.8) | 36 (37.1) | 57 | 41.9 |
| Heroin | 17 (43.6) | 33 (34.0) | 50 | 36.8 |
| Marijuana | 11 (28.2) | 23 (23.7) | 34 | 25.0 |
| Opioid or oxycodone * | 13 (33.3) | 16 (16.5) | 29 | 21.3 |
| Chemotherapy *** | 9 (23.1) | 3 (3.1) | 12 | 8.8 |
| Exclusive Breastfeeding *** | ||||
| Some or correct idea | 29 (74.4) | 35 (36.1) | 64 | 47.0 |
| Wrong idea or do not know | 10 (25.6) | 62 (63.9) | 72 | 52.9 |
| Breastfeeding Patterns | Group I Early Pandemic | Group II Later Pandemic | Totals § | |
|---|---|---|---|---|
| No. | % | |||
| 1 month postpartum | n = 31 | n = 39 | n = 70 | |
| Breastmilk provided * | 21 (67.7) | 22 (56.4) | 43 | 61.4 |
| Exclusive breastfeeding ** | 13 (41.9) | 5 (12.8) | 18 | 25.7 |
| Nursing at the breast * | 19 (61.3) | 15 (38.5) | 34 | 48.6 |
| 3 months postpartum | n = 27 | n = 22 | n = 49 | |
| Breastmilk provided * | 15 (55.6) | 7 (31.8) | 22 | 44.9 |
| Exclusive breastfeeding ** | 9 (33.3) | 1 (4.5) | 10 | 20.4 |
| Nursing at the breast | 13 (48.1) | 5 (22.7) | 18 | 36.7 |
| 6 Months postpartum | n = 15 | n = 12 | n = 27 | |
| Breastmilk provided | 7 (46.7) | 4 (33.3) | 11 | 40.7 |
| Exclusive breastfeeding | 3 (20.0) | 0 (0.0) | 3 | 11.1 |
| Nursing at the breast | 6 (40.0) | 4 (33.3) | 10 | 37.0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ukoli, F.; Leavell, J.; Mayo, A.; Moore, J.; Nchami, N.; Britt, A. Encouraging and Reinforcing Safe Breastfeeding Practices during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2023, 20, 1756. https://doi.org/10.3390/ijerph20031756
Ukoli F, Leavell J, Mayo A, Moore J, Nchami N, Britt A. Encouraging and Reinforcing Safe Breastfeeding Practices during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2023; 20(3):1756. https://doi.org/10.3390/ijerph20031756
Chicago/Turabian StyleUkoli, Flora, Jacinta Leavell, Amasyah Mayo, Jayla Moore, Nia Nchami, and Allysceaeioun Britt. 2023. "Encouraging and Reinforcing Safe Breastfeeding Practices during the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 20, no. 3: 1756. https://doi.org/10.3390/ijerph20031756
APA StyleUkoli, F., Leavell, J., Mayo, A., Moore, J., Nchami, N., & Britt, A. (2023). Encouraging and Reinforcing Safe Breastfeeding Practices during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health, 20(3), 1756. https://doi.org/10.3390/ijerph20031756