
School-Based Interventions to Support Healthy Indoor and Outdoor Environments for Children: A Systematic Review

 , , , ,
, , , , 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Methods
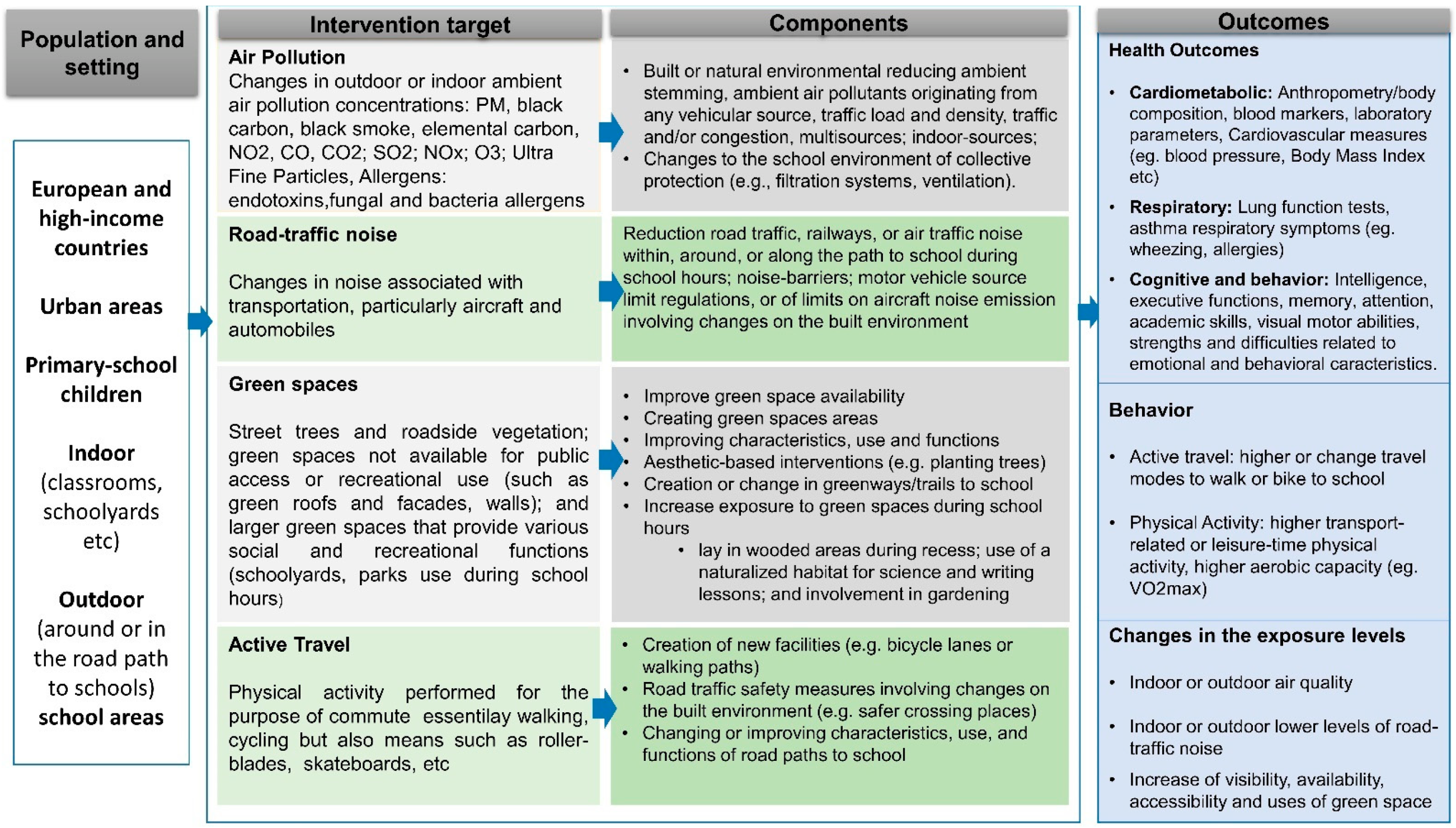
2.1. Scope of the Systematic Review
- Population: primary school-aged children between 5 and 12 years of age enrolled in primary schools from urban areas of Europe and high-level income countries in the rest of the world.
- Intervention: Any intervention which involved changes to the school (indoor or outdoor) built or natural environment to reduce exposures levels to key air pollutants, road traffic or aircraft noise; to increase the visibility, availability, accessibility, or time children spent in green spaces; or to promote active travel to school
- Comparator: Any intervention study was included—the comparison was expected to be no intervention, another intervention, a non-exposed control group or less exposed control groups, standard or currently existing interventions. However, we did not exclude studies based on the comparison.
- Outcomes: Child health outcomes (i.e., respiratory, cardiometabolic, cognitive/behavioral domains), behaviors related to physical activity and active travel, or changes in the exposure levels.
2.2. Search Strategy
2.3. Study Inclusion Criteria

2.4. Data Extraction
2.5. Quality Assessment
3. Results
3.1. Study Selection
3.2. Study Characteristics
3.3. Description and Impact of Interventions
3.4. Air Pollution
3.4.1. Intervention Characteristics
3.4.2. Intervention Effectiveness

3.4.3. Specific Methodological Limitations
3.5. Green Spaces
3.5.1. Intervention Characteristics
3.5.2. Intervention Effectiveness
Increase of Children’s Green Time during School Hours
Greening Schools Indoors
3.5.3. Specific Methodological Limitations
3.6. Active Travel
3.6.1. Interventions Characteristics
3.6.2. Intervention Effectiveness
3.6.3. Specific Methodological Limitations
4. Discussion
4.1. Risk of Bias and Study Quality
4.2. Future Directions
4.3. Policy and Practice Recommendations
4.4. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gascon, M.; Vrijheid, M.; Nieuwenhuijsen, M.J. The Built Environment and Child Health: An Overview of Current Evidence. Curr. Environ. Health Rep. 2016, 3, 250–257. [Google Scholar] [CrossRef] [PubMed]
- Lacagnina, S. The Developmental Origins of Health and Disease (DOHaD). Am. J. Lifestyle Med. 2019, 14, 47–50. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Air Pollution and Child Health: Prescribing Clean Air; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Osborne, S.; Uche, O.; Mitsakou, C.; Exley, K.; Dimitroulopoulou, S. Air Quality around Schools: Part I—A Comprehensive Literature Review across High-Income Countries. Environ. Res. 2021, 196, 110817. [Google Scholar] [CrossRef]
- Vrijheid, M. The Exposome: A New Paradigm to Study the Impact of Environment on Health. Thorax 2014, 69, 876–878. [Google Scholar] [CrossRef]
- Baloch, R.M.; Maesano, C.N.; Christoffersen, J.; Banerjee, S.; Gabriel, M.; Csobod, É.; de Oliveira Fernandes, E.; Annesi-Maesano, I.; Csobod, É.; Szuppinger, P.; et al. Indoor Air Pollution, Physical and Comfort Parameters Related to Schoolchildren’s Health: Data from the European SINPHONIE Study. Sci. Total Environ. 2020, 739, 139870. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization, Regional Office for Europe. Promoting Physical Activity in the Education Sector: Current Status and Success Stories from the European Union Member States of the WHO European Region; World Health Organization, Regional Office for Europe: Geneva, Switzerland, 2018. [Google Scholar]
- De Bont, J.; Casas, M.; Barrera-Gómez, J.; Cirach, M.; Rivas, I.; Valvi, D.; Álvarez, M.; Dadvand, P.; Sunyer, J.; Vrijheid, M. Ambient Air Pollution and Overweight and Obesity in School-Aged Children in Barcelona, Spain. Environ. Int. 2019, 125, 58–64. [Google Scholar] [CrossRef]
- Sunyer, J.; Esnaola, M.; Alvarez-Pedrerol, M.; Forns, J.; Rivas, I.; López-Vicente, M.; Suades-González, E.; Foraster, M.; Garcia-Esteban, R.; Basagaña, X.; et al. Association between Traffic-Related Air Pollution in Schools and Cognitive Development in Primary School Children: A Prospective Cohort Study. PLoS Med. 2015, 12, e1001792. [Google Scholar] [CrossRef]
- Pierangeli, I.; Nieuwenhuijsen, M.J.; Cirach, M.; Rojas-Rueda, D. Health Equity and Burden of Childhood Asthma—Related to Air Pollution in Barcelona. Environ. Res. 2020, 186, 109067. [Google Scholar] [CrossRef]
- Clark, C.; Crombie, R.; Head, J.; van Kamp, I.; van Kempen, E.; Stansfeld, S.A. Does Traffic-Related Air Pollution Explain Associations of Aircraft and Road Traffic Noise Exposure on Children’s Health and Cognition? A Secondary Analysis of the United Kingdom Sample from the RANCH Project. Am. J. Epidemiol. 2012, 176, 327–337. [Google Scholar] [CrossRef]
- Forns, J.; Dadvand, P.; Foraster, M.; Alvarez-Pedrerol, M.; Rivas, I.; López-Vicente, M.; Suades-Gonzalez, E.; Garcia-Esteban, R.; Esnaola, M.; Cirach, M.; et al. Traffic-Related Air Pollution, Noise at School, and Behavioral Problems in Barcelona Schoolchildren: A Cross-Sectional Study. Environ. Health Perspect. 2016, 124, 529–535. [Google Scholar] [CrossRef]
- Stansfeld, S.; Clark, C. Health Effects of Noise Exposure in Children. Curr. Environ. Health Rep. 2015, 2, 171–178. [Google Scholar] [CrossRef]
- European Environment Agency. Environmental Noise in Europe, 2020; Publications Office: Luxembourg, 2020. [Google Scholar]
- Rivas, I.; Querol, X.; Wright, J.; Sunyer, J. How to Protect School Children from the Neurodevelopmental Harms of Air Pollution by Interventions in the School Environment in the Urban Context. Environ. Int. 2018, 121, 199–206. [Google Scholar] [CrossRef]
- Markevych, I.; Schoierer, J.; Hartig, T.; Chudnovsky, A.; Hystad, P.; Dzhambov, A.M.; de Vries, S.; Triguero-Mas, M.; Brauer, M.; Nieuwenhuijsen, M.J.; et al. Exploring Pathways Linking Greenspace to Health: Theoretical and Methodological Guidance. Environ. Res. 2017, 158, 301–317. [Google Scholar] [CrossRef]
- World Health Organization, Regional Office for Europe. Urban Green Spaces and Health; World Health Organization, Regional Office for Europe: Geneva, Switzerland, 2016. [Google Scholar]
- Amoly, E.; Dadvand, P.; Forns, J.; López-Vicente, M.; Basagaña, X.; Julvez, J.; Alvarez-Pedrerol, M.; Nieuwenhuijsen, M.J.; Sunyer, J. Green and Blue Spaces and Behavioral Development in Barcelona Schoolchildren: The BREATHE Project. Environ. Health Perspect. 2014, 122, 1351–1358. [Google Scholar] [CrossRef]
- Dadvand, P.; Nieuwenhuijsen, M.J.; Esnaola, M.; Forns, J.; Basagaña, X.; Alvarez-Pedrerol, M.; Rivas, I.; López-Vicente, M.; De Castro Pascual, M.; Su, J.; et al. Green Spaces and Cognitive Development in Primary Schoolchildren. Proc. Natl. Acad. Sci. USA 2015, 112, 7937–7942. [Google Scholar] [CrossRef]
- Fyfe-Johnson, A.L.; Hazlehurst, M.F.; Perrins, S.P.; Bratman, G.N.; Thomas, R.; Garrett, K.A.; Hafferty, K.R.; Cullaz, T.M.; Marcuse, E.K.; Tandon, P.S. Nature and Children’s Health: A Systematic Review. Pediatrics 2021, 148, e2020049155. [Google Scholar] [CrossRef]
- Gray, T. Outdoor Learning: Not New, Just Newly Important. Curric. Perspect. 2018, 38, 145–149. [Google Scholar] [CrossRef]
- Daniels, K.M.; Schinasi, L.H.; Auchincloss, A.H.; Forrest, C.B.; Diez Roux, A.V. The Built and Social Neighborhood Environment and Child Obesity: A Systematic Review of Longitudinal Studies. Prev. Med. 2021, 153, 106790. [Google Scholar] [CrossRef]
- Ortegon-Sanchez, A.; McEachan, R.R.C.; Albert, A.; Cartwright, C.; Christie, N.; Dhanani, A.; Islam, S.; Ucci, M.; Vaughan, L. Measuring the Built Environment in Studies of Child Health—A Meta-Narrative Review of Associations. Int. J. Environ. Res. Public Health 2021, 18, 10741. [Google Scholar] [CrossRef]
- Warembourg, C.; Nieuwenhuijsen, M.; Ballester, F.; de Castro, M.; Chatzi, L.; Esplugues, A.; Heude, B.; Maitre, L.; McEachan, R.; Robinson, O.; et al. Urban Environment during Early-Life and Blood Pressure in Young Children. Environ. Int. 2021, 146, 106174. [Google Scholar] [CrossRef]
- Audrey, S.; Batista-Ferrer, H. Healthy Urban Environments for Children and Young People: A Systematic Review of Intervention Studies. Health Place 2015, 36, 97–117. [Google Scholar] [CrossRef] [PubMed]
- Julvez, J.; López-Vicente, M.; Warembourg, C.; Maitre, L.; Philippat, C.; Gützkow, K.B.; Guxens, M.; Evandt, J.; Andrusaityte, S.; Burgaleta, M.; et al. Early Life Multiple Exposures and Child Cognitive Function: A Multi-Centric Birth Cohort Study in Six European Countries. Environ. Pollut. 2021, 284, 117404. [Google Scholar] [CrossRef] [PubMed]
- Burns, J.; Boogaard, H.; Polus, S.; Pfadenhauer, L.M.; Rohwer, A.C.; van Erp, A.M.; Turley, R.; Rehfuess, E.A. Interventions to Reduce Ambient Air Pollution and Their Effects on Health: An Abridged Cochrane Systematic Review. Environ. Int. 2020, 135, 105400. [Google Scholar] [CrossRef] [PubMed]
- Ortegon-Sanchez, A.; Vaughan, L.; Christie, N.; McEachan, R.R.C. Shaping Pathways to Child Health: A Systematic Review of Street-Scale Interventions in City Streets. Int. J. Environ. Res. Public Health 2022, 19, 5227. [Google Scholar] [CrossRef] [PubMed]
- Jones, R.A.; Blackburn, N.E.; Woods, C.; Byrne, M.; van Nassau, F.; Tully, M.A. Interventions Promoting Active Transport to School in Children: A Systematic Review and Meta-Analysis. Prev. Med. 2019, 123, 232–241. [Google Scholar] [CrossRef]
- Caiaffa, W.T.; Ferreira, F.R.; Ferreira, A.D.; Oliveira, C.D.L.; Camargos, V.P.; Proietti, F.A. Urban health: “The city is a strange lady, smiling today, devouring you tomorrow”. Cien Saude Colet 2008, 13, 1785–1796. [Google Scholar] [CrossRef]
- Pabayo, R.; Gauvin, L.; Barnett, T.A. Longitudinal Changes in Active Transportation to School in Canadian Youth Aged 6 Through 16 Years. Pediatrics 2011, 128, e404–e413. [Google Scholar] [CrossRef]
- United Nations; Statistics Division, U.S. Statistical Yearbook 2020. In Statistical Yearbook, 63rd ed.; UN: New York, NY, USA, 2020; ISBN 978-92-1-259150-6. [Google Scholar]
- World Bank Country and Lending Groups—World Bank Data Help Desk. Available online: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups (accessed on 20 May 2020).
- Brink, L.A.; Nigg, C.R.; Lampe, S.M.R.; Kingston, B.A.; Mootz, A.L.; van Vliet, W. Influence of Schoolyard Renovations on Children’s Physical Activity: The Learning Landscapes Program. Am. J. Public Health 2010, 100, 1672–1678. [Google Scholar] [CrossRef]
- Reeves, B.C.; Wells, G.A.; Waddington, H. Quasi-Experimental Study Designs Series-Paper 5: A Checklist for Classifying Studies Evaluating the Effects on Health Interventions-a Taxonomy without Labels. J. Clin. Epidemiol. 2017, 89, 30–42. [Google Scholar] [CrossRef]
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M.; et al. Better Reporting of Interventions: Template for Intervention Description and Replication (TIDieR) Checklist and Guide. BMJ 2014, 348, g1687. [Google Scholar] [CrossRef]
- Hunter, R.F.; Cleland, C.; Cleary, A.; Droomers, M.; Wheeler, B.W.; Sinnett, D.; Nieuwenhuijsen, M.J.; Braubach, M. Environmental, Health, Wellbeing, Social and Equity Effects of Urban Green Space Interventions: A Meta-Narrative Evidence Synthesis. Environ. Int. 2019, 130, 104923. [Google Scholar] [CrossRef] [PubMed]
- Hanson, S.; Jones, A. Is There Evidence That Walking Groups Have Health Benefits? A Systematic Review and Meta-Analysis. Br. J. Sport. Med. 2015, 49, 710–715. [Google Scholar] [CrossRef] [PubMed]
- Twohig-Bennett, C.; Jones, A. The Health Benefits of the Great Outdoors: A Systematic Review and Meta-Analysis of Greenspace Exposure and Health Outcomes. Environ. Res. 2018, 166, 628–637. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 Explanation and Elaboration: Updated Guidance and Exemplars for Reporting Systematic Reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef] [PubMed]
- Oh, H.-J.; Nam, I.-S.; Yun, H.; Kim, J.; Yang, J.; Sohn, J.-R. Characterization of Indoor Air Quality and Efficiency of Air Purifier in Childcare Centers, Korea. Build. Environ. 2014, 82, 203–214. [Google Scholar] [CrossRef]
- Pacitto, A.; Amato, F.; Moreno, T.; Pandolfi, M.; Fonseca, A.; Mazaheri, M.; Stabile, L.; Buonanno, G.; Querol, X. Effect of Ventilation Strategies and Air Purifiers on the Children’s Exposure to Airborne Particles and Gaseous Pollutants in School Gyms. Sci. Total Environ. 2020, 712, 135673. [Google Scholar] [CrossRef]
- MacNeill, M.; Dobbin, N.; St-Jean, M.; Wallace, L.; Marro, L.; Shin, T.; You, H.; Kulka, R.; Allen, R.W.; Wheeler, A.J. Can Changing the Timing of Outdoor Air Intake Reduce Indoor Concentrations of Traffic-Related Pollutants in Schools? Indoor Air 2016, 26, 687–701. [Google Scholar] [CrossRef]
- Smedje, G.; Mattsson, M.; Wålinder, R. Comparing Mixing and Displacement Ventilation in Classrooms: Pupils Perception and Health. Indoor Air 2011, 21, 454–461. [Google Scholar] [CrossRef]
- Bakó-Biró, Z.; Clements-Croome, D.J.; Kochhar, N.; Awbi, H.B.; Williams, M.J. Ventilation Rates in Schools and Pupils’ Performance. Build. Environ. 2012, 48, 215–223. [Google Scholar] [CrossRef]
- Trompetter, W.J.; Boulic, M.; Ancelet, T.; Garcia-Ramirez, J.C.; Davy, P.K.; Wang, Y.; Phipps, R. The Effect of Ventilation on Air Particulate Matter in School Classrooms. J. Build. Eng. 2018, 18, 164–171. [Google Scholar] [CrossRef]
- Rosbach, J.T.M.; Vonk, M.; Duijm, F.; van Ginkel, J.T.; Gehring, U.; Brunekreef, B. A Ventilation Intervention Study in Classrooms to Improve Indoor Air Quality: The FRESH Study. Environ. Health A Glob. Access Sci. Source 2013, 12, 110. [Google Scholar] [CrossRef]
- Rosbach, J.; Krop, E.; Vonk, M.; van Ginkel, J.; Meliefste, C.; de Wind, S.; Gehring, U.; Brunekreef, B. Classroom Ventilation and Indoor Air Quality-Results from the FRESH Intervention Study. Indoor Air 2016, 26, 538–545. [Google Scholar] [CrossRef]
- Twardella, D.; Matzen, W.; Lahrz, T.; Burghardt, R.; Spegel, H.; Hendrowarsito, L.; Frenzel, A.C.; Fromme, H. Effect of Classroom Air Quality on Students’ Concentration: Results of a Cluster-Randomized Cross-over Experimental Study. Indoor Air 2012, 22, 378–387. [Google Scholar] [CrossRef]
- Petersen, S.; Jensen, K.L.; Pedersen, A.L.S.; Rasmussen, H.S. The Effect of Increased Classroom Ventilation Rate Indicated by Reduced CO2 Concentration on the Performance of Schoolwork by Children. Indoor Air 2016, 26, 366–379. [Google Scholar] [CrossRef]
- Block, K.; Gibbs, L.; Staiger, P.K.; Gold, L.; Johnson, B.; Macfarlane, S.; Long, C.; Townsend, M. Growing Community: The Impact of the Stephanie Alexander Kitchen Garden Program on the Social and Learning Environment in Primary Schools. Health Educ. Behav. 2012, 39, 419–432. [Google Scholar] [CrossRef]
- Wells, N.M.; Myers, B.M.; Henderson, C.R. School Gardens and Physical Activity: A Randomized Controlled Trial of Low-Income Elementary Schools. Prev. Med. 2014, 69 (Suppl. 1), S27–S33. [Google Scholar] [CrossRef]
- Van Den Berg, A.; Warren, J.L.; McIntosh, A.; Hoelscher, D.; Ory, M.G.; Jovanovic, C.; Lopez, M.; Whittlesey, L.; Kirk, A.; Walton, C.; et al. Impact of a Gardening and Physical Activity Intervention in Title 1 Schools: The TGEG Study. Child. Obes. 2020, 16, S44–S54. [Google Scholar] [CrossRef]
- Rees-Punia, E.; Holloway, A.; Knauft, D.; Schmidt, M.D. Effects of School Gardening Lessons on Elementary School Children’s Physical Activity and Sedentary Time. J. Phys. Act. Health 2017, 14, 959–964. [Google Scholar] [CrossRef]
- Gustafsson, P.E.; Szczepanski, A.; Nelson, N.; Gustafsson, P.A. Effects of an Outdoor Education Intervention on the Mental Health of Schoolchildren. J. Adventure Educ. Outdoor Learn. 2012, 12, 63–79. [Google Scholar] [CrossRef]
- Largo-Wight, E.; Guardino, C.; Wludyka, P.S.; Hall, K.W.; Wight, J.T.; Merten, J.W. Nature Contact at School: The Impact of an Outdoor Classroom on Children’s Well-Being. Int. J. Environ. Health Res. 2018, 28, 653–666. [Google Scholar] [CrossRef]
- Kuo, M.; Browning, M.H.E.M.; Penner, M.L. Do Lessons in Nature Boost Subsequent Classroom Engagement? Refueling Students in Flight. Front. Psychol. 2018, 8, 2253. [Google Scholar] [CrossRef] [PubMed]
- Taylor, A.F.; Butts-Wilmsmeyer, C. Self-Regulation Gains in Kindergarten Related to Frequency of Green Schoolyard Use. J. Environ. Psychol. 2020, 70, 101440. [Google Scholar] [CrossRef]
- Bang, K.-S.; Kim, S.; Song, M.K.; Kang, K.I.; Jeong, Y. The Effects of a Health Promotion Program Using Urban Forests and Nursing Student Mentors on the Perceived and Psychological Health of Elementary School Children in Vulnerable Populations. Int. J. Environ. Res. Public Health 2018, 15, 1977. [Google Scholar] [CrossRef] [PubMed]
- Quibell, T.; Charlton, J.; Law, J. Wilderness Schooling: A Controlled Trial of the Impact of an Outdoor Education Programme on Attainment Outcomes in Primary School Pupils. Br. Educ. Res. J. 2017, 43, 572–587. [Google Scholar] [CrossRef]
- Amicone, G.; Petruccelli, I.; De Dominicis, S.; Gherardini, A.; Costantino, V.; Perucchini, P.; Bonaiuto, M. Green Breaks: The Restorative Effect of the School Environment’s Green Areas on Children’s Cognitive Performance. Front. Psychol. 2018, 9, 1579. [Google Scholar] [CrossRef]
- Barton, J.; Sandercock, G.; Pretty, J.; Wood, C. The Effect of Playground- and Nature-Based Playtime Interventions on Physical Activity and Self-Esteem in UK School Children. Int. J. Environ. Health Res. 2015, 25, 196–206. [Google Scholar] [CrossRef]
- Wood, C.; Gladwell, V.; Barton, J. A Repeated Measures Experiment of School Playing Environment to Increase Physical Activity and Enhance Self-Esteem in UK School Children. PLoS ONE 2014, 9, e108701. [Google Scholar] [CrossRef]
- Raney, M.A.; Hendry, C.F.; Yee, S.A. Physical Activity and Social Behaviors of Urban Children in Green Playgrounds. Am. J. Prev. Med. 2019, 56, 522–529. [Google Scholar] [CrossRef]
- Van Dijk-Wesselius, J.E.; Maas, J.; Hovinga, D.; van Vugt, M.; van den Berg, A.E. The Impact of Greening Schoolyards on the Appreciation, and Physical, Cognitive and Social-Emotional Well-Being of Schoolchildren: A Prospective Intervention Study. Landsc. Urban Plan. 2018, 180, 15–26. [Google Scholar] [CrossRef]
- Van den Berg, A.E.; Wesselius, J.E.; Maas, J.; Tanja-Dijkstra, K. Green Walls for a Restorative Classroom Environment: A Controlled Evaluation Study. Environ. Behav. 2017, 49, 791–813. [Google Scholar] [CrossRef]
- Bernardo, F.; Loupa-Ramos, I.; Matos Silva, C.; Manso, M. The Restorative Effect of the Presence of Greenery on the Classroom in Children’s Cognitive Performance. Sustainability 2021, 13, 3488. [Google Scholar] [CrossRef]
- McDonald, N.C.; Steiner, R.L.; Lee, C.; Smith, T.R.; Zhu, X.; Yang, Y. Impact of the Safe Routes to School Program on Walking and Bicycling. J. Am. Plan. Assoc. 2014, 80, 153–167. [Google Scholar] [CrossRef]
- McDonald, N.; Yang, Y.; Abbott, S.M.; Bullock, A.N. Impact of the Safe Routes to School Program on Walking and Biking: Eugene, Oregon Study. Transp. Policy 2013, 29, 243–248. [Google Scholar] [CrossRef]
- Stewart, O.; Moudon, A.V.; Claybrooke, C. Multistate Evaluation of Safe Routes to School Programs. Am. J. Health Promot. AJHP 2014, 28, S89–S96. [Google Scholar] [CrossRef]
- Hoelscher, D.; Ory, M.; Dowdy, D.; Miao, J.G.; Atteberry, H.; Nichols, D.; Evans, A.; Menendez, T.; Lee, C.; Wang, S.J. Effects of Funding Allocation for Safe Routes to School Programs on Active Commuting to School and Related Behavioral, Knowledge, and Psychosocial Outcomes: Results From the Texas Childhood Obesity Prevention Policy Evaluation (T-COPPE) Study. Environ. Behav. 2016, 48, 210–229. [Google Scholar] [CrossRef]
- Hinckson, E.A.; Garrett, N.; Duncan, S. Active Commuting to School in New Zealand Children (2004–2008): A Quantitative Analysis. Prev. Med. 2011, 52, 332–336. [Google Scholar] [CrossRef]
- Hinckson, E.A.; Badland, H.M. School Travel Plans: Preliminary Evidence for Changing School-Related Travel Patterns in Elementary School Children. Am. J. Health Promot. AJHP 2011, 25, 368–371. [Google Scholar] [CrossRef]
- Ragland, D.R.; Pande, S.; Bigham, J.; Cooper, J.F. Examining Long-Term Impact of California Safe Routes to School Program: Ten Years Later. Transp. Res. Rec. 2014, 2464, 86–92. [Google Scholar] [CrossRef]
- Buliung, R.; Faulkner, G.; Beesley, T.; Kennedy, J. School Travel Planning: Mobilizing School and Community Resources to Encourage Active School Transportation. J. Sch. Health 2011, 81, 704–712. [Google Scholar] [CrossRef]
- Smith, M.; Hawley, G.; Mackay, L.; Hosking, J.; Mackie, H.; Ikeda, E.; Egli, V.; Ellaway, A.; Witten, K. Impact of Changing Road Infrastructure on Children’s Active Travel: A Multi-Methods Study from Auckland, New Zealand. J. Transp. Health 2020, 18, 100868. [Google Scholar] [CrossRef]
- Mammen, G.; Stone, M.R.; Buliung, R.; Faulkner, G. School Travel Planning in Canada: Identifying Child, Family, and School-Level Characteristics Associated with Travel Mode Shift from Driving to Active School Travel. J. Transp. Health 2014, 1, 288–294. [Google Scholar] [CrossRef]
- Mammen, G.; Stone, M.R.; Faulkner, G.; Ramanathan, S.; Buliung, R.; O’Brien, C.; Kennedy, J. Active School Travel: An Evaluation of the Canadian School Travel Planning Intervention. Prev. Med. 2014, 60, 55–59. [Google Scholar] [CrossRef] [PubMed]
- Østergaard, L.; Støckel, J.T.; Andersen, L.B. Effectiveness and Implementation of Interventions to Increase Commuter Cycling to School: A Quasi-Experimental Study. BMC Public Health 2015, 15, 1199. [Google Scholar] [CrossRef] [PubMed]
- Mittleman, M.A.; Mostofsky, E. Exchangeability in the Case-Crossover Design. Int. J. Epidemiol. 2014, 43, 1645–1655. [Google Scholar] [CrossRef] [PubMed]
- Janes, H.; Sheppard, L.; Lumley, T. Case-Crossover Analyses of Air Pollution Exposure Data: Referent Selection Strategies and Their Implications for Bias. Epidemiology 2005, 16, 717–726. [Google Scholar] [CrossRef]
- Dobson, D.; Cook, T.J. Avoiding Type III Error in Program Evaluation: Results from a Field Experiment. Eval. Program Plan. 1980, 3, 269–276. [Google Scholar] [CrossRef]
- Larouche, R.; Mammen, G.; Rowe, D.A.; Faulkner, G. Effectiveness of Active School Transport Interventions: A Systematic Review and Update. BMC Public Health 2018, 18, 206. [Google Scholar] [CrossRef]
- Zare Sakhvidi, M.J.; Knobel, P.; Bauwelinck, M.; de Keijzer, C.; Boll, L.M.; Spano, G.; Ubalde-Lopez, M.; Sanesi, G.; Mehrparvar, A.H.; Jacquemin, B.; et al. Greenspace Exposure and Children Behavior: A Systematic Review. Sci. Total. Environ. 2022, 824, 153608. [Google Scholar] [CrossRef]
- De Souza Andrade, A.C.; Mingoti, S.A.; Fernandes, A.P.; de Andrade, R.G.; de Lima Friche, A.A.; Xavier, C.C.; Proietti, F.A.; Diez-Roux, A.V.; Caiaffa, W.T. Neighborhood-Based Physical Activity Differences: Evaluation of the Effect of Health Promotion Program. PLoS ONE 2018, 13, e0192115. [Google Scholar] [CrossRef]
- Foraster, M.; Esnaola, M.; López-Vicente, M.; Rivas, I.; Álvarez-Pedrerol, M.; Persavento, C.; Sebastian-Galles, N.; Pujol, J.; Dadvand, P.; Sunyer, J. Exposure to Road Traffic Noise and Cognitive Development in Schoolchildren in Barcelona, Spain: A Population-Based Cohort Study. PLoS Med. 2022, 19, e1004001. [Google Scholar] [CrossRef]
- Cepeda, M.; Schoufour, J.; Freak-Poli, R.; Koolhaas, C.M.; Dhana, K.; Bramer, W.M.; Franco, O.H. Levels of Ambient Air Pollution According to Mode of Transport: A Systematic Review. Lancet Public Health 2017, 2, e23–e34. [Google Scholar] [CrossRef]
- Pereira, V.R.; Coimbra, V.C.C.; de Souza Cardoso, C.; Oliveira, N.A.; Vieira, A.C.G.; de Oliveira Nobre, M.; Nino, M.E.L. Participatory methodologies in research with children: Creative and innovative approaches. Rev. Gaucha Enferm. 2017, 37, e67908. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernandes, A.; Ubalde-López, M.; Yang, T.C.; McEachan, R.R.C.; Rashid, R.; Maitre, L.; Nieuwenhuijsen, M.J.; Vrijheid, M. School-Based Interventions to Support Healthy Indoor and Outdoor Environments for Children: A Systematic Review. Int. J. Environ. Res. Public Health 2023, 20, 1746. https://doi.org/10.3390/ijerph20031746
Fernandes A, Ubalde-López M, Yang TC, McEachan RRC, Rashid R, Maitre L, Nieuwenhuijsen MJ, Vrijheid M. School-Based Interventions to Support Healthy Indoor and Outdoor Environments for Children: A Systematic Review. International Journal of Environmental Research and Public Health. 2023; 20(3):1746. https://doi.org/10.3390/ijerph20031746
Chicago/Turabian StyleFernandes, Amanda, Mònica Ubalde-López, Tiffany C. Yang, Rosemary R. C. McEachan, Rukhsana Rashid, Léa Maitre, Mark J. Nieuwenhuijsen, and Martine Vrijheid. 2023. "School-Based Interventions to Support Healthy Indoor and Outdoor Environments for Children: A Systematic Review" International Journal of Environmental Research and Public Health 20, no. 3: 1746. https://doi.org/10.3390/ijerph20031746
APA StyleFernandes, A., Ubalde-López, M., Yang, T. C., McEachan, R. R. C., Rashid, R., Maitre, L., Nieuwenhuijsen, M. J., & Vrijheid, M. (2023). School-Based Interventions to Support Healthy Indoor and Outdoor Environments for Children: A Systematic Review. International Journal of Environmental Research and Public Health, 20(3), 1746. https://doi.org/10.3390/ijerph20031746