
Health Professionals’ Motivational Strategies to Enhance Adherence in the Rehabilitation of People with Lower Limb Fractures: Scoping Review

 ,
,  , ,
, ,  , ,
, ,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Stage 1: Identifying Research Questions
2.2. Stage 2: Identifying Relevant Studies
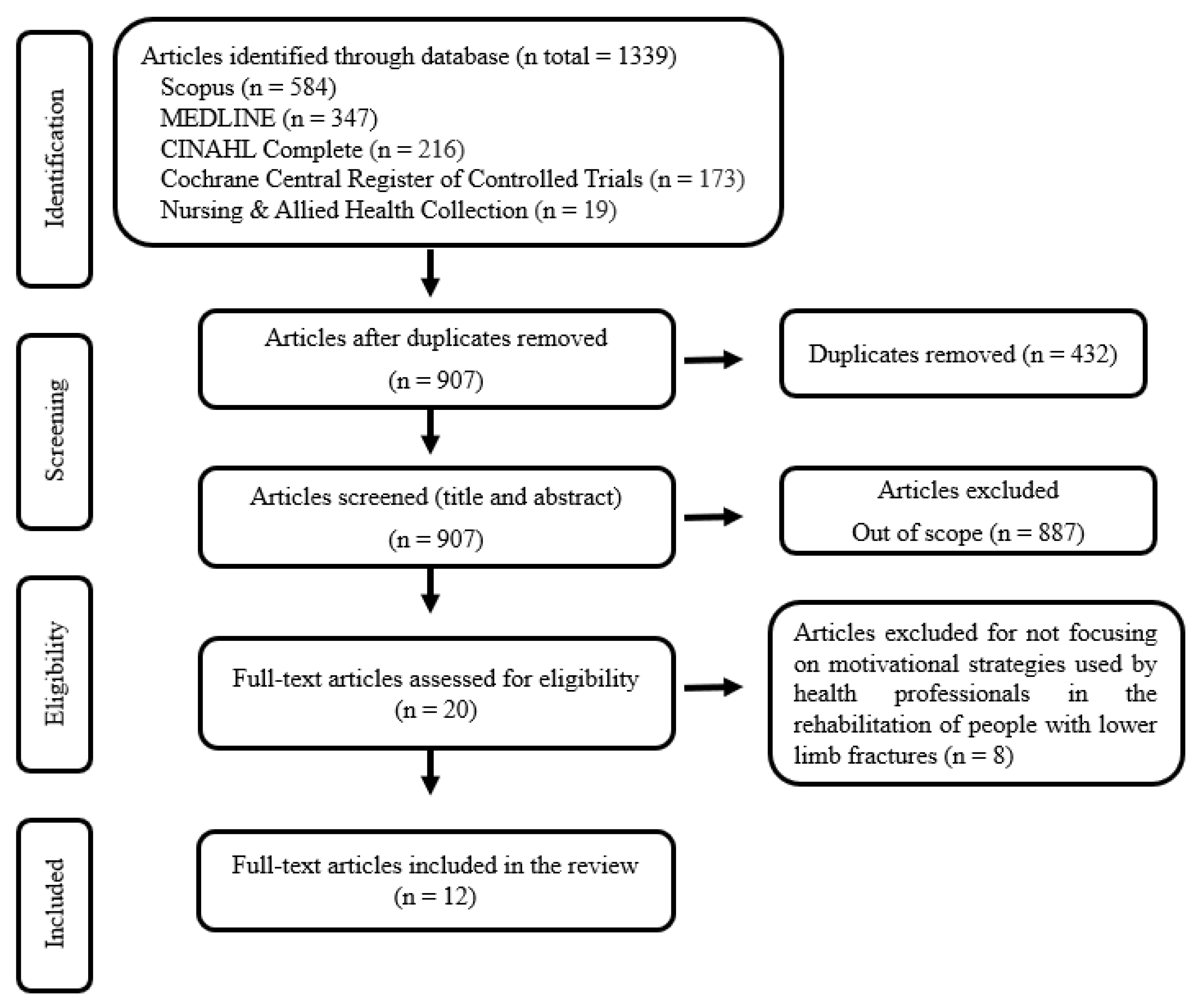
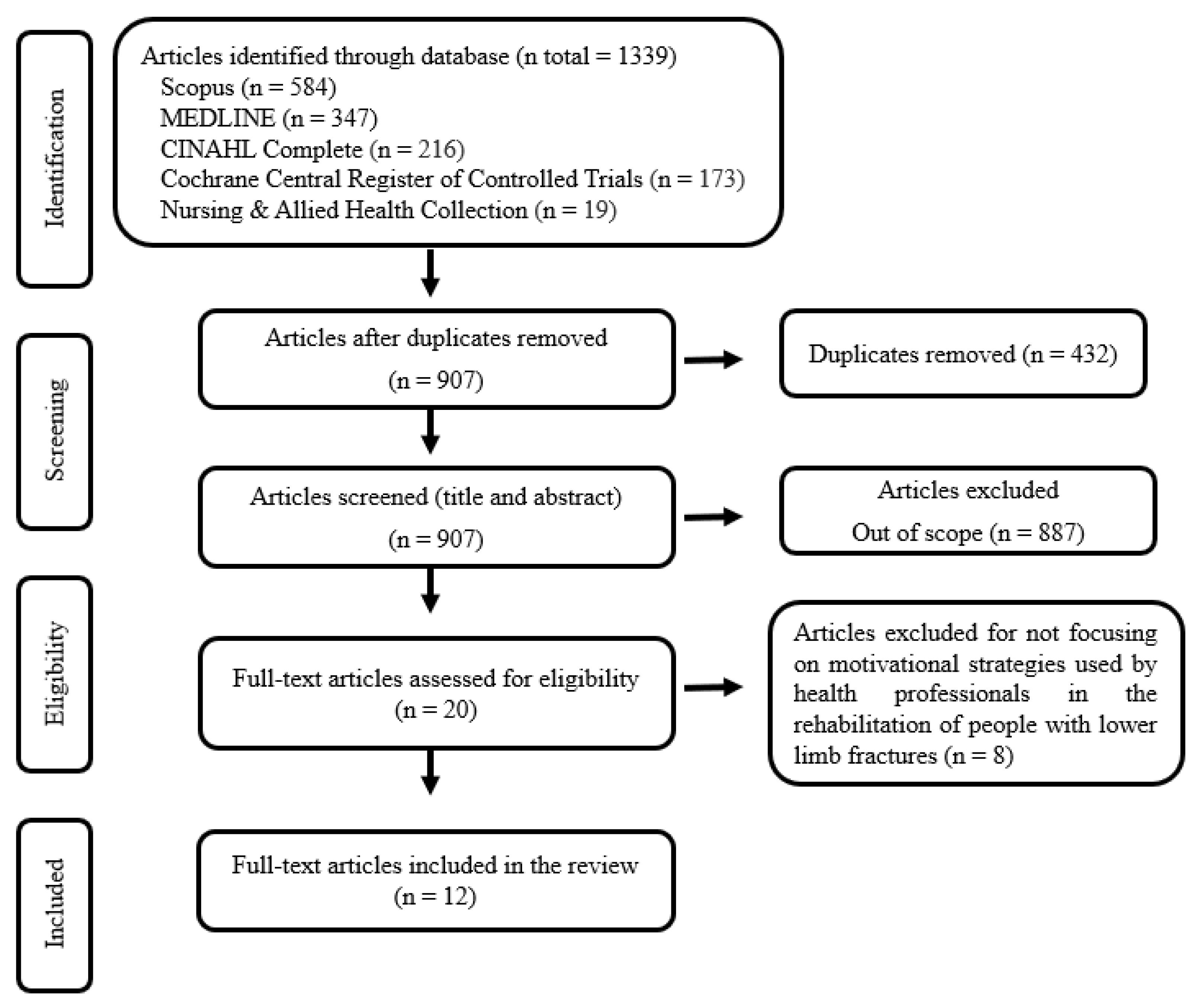
2.3. Stage 3: Study Selection
2.4. Stage 4: Charting the Data
2.5. Stage 5: Collating, Summarizing, and Reporting the Results
3. Results

{kind=link}
| Author/Year/Title/Country | Study Design/Aim | Interventions |
|---|---|---|
| Olsson et al., 2007 [32] Effects of nursing interventions within an integrated care pathway for patients with hip fracture Sweden | Quasi-experimental prospective study. To evaluate the contribution of nursing care within an integrated care pathway for patients with hip fractures. |
|
| Resnick et al., 2007 [35] Testing the effectiveness of the exercise plus program in older women post-hip fracture United States of America | Randomized controlled trial. To test the impact of a self-efficacy-based intervention, the Exercise Plus Program, and the different components of the intervention on self-efficacy, outcome expectations, and exercise behavior among older women post-hip fracture. |
|
| Casado et al., 2009 [34] Social support for exercise by experts in older women post-hip fracture United States of America | Secondary data analysis from a randomized controlled trial. To examine how social support for exercise by experts affected the self-efficacy, outcome expectations, and exercise behavior among older women following a hip fracture. |
|
| Sipilä et al., 2011 [30] Promoting mobility after hip fracture (ProMo): study protocol and selected baseline results of a year-long randomized controlled trial among community-dwelling older people Finland | Randomized controlled trial. To describe the design, intervention, and demographic baseline results of a study investigating the effects of a rehabilitation program aiming to restore mobility and functional capacity among community-dwelling participants after hip fracture. |
|
| Harmelink et al., 2017 [33] The effectiveness of the use of a digital activity coaching system in addition to a two-week home-based exercise program in patients after total knee arthroplasty: study protocol for a randomized controlled trial the Netherlands | Randomized controlled trial. To determine the effectiveness of an activity coaching system in addition to a home-based exercise program after a TKA compared to only the home-based exercise program with physical functioning as the outcome. |
|
| Room et al., 2020 [28] Development of a functional rehabilitation intervention for post-knee arthroplasty patients: Community based Rehabilitation post-Knee Arthroplasty (CORKA) trial United Kingdom | Study protocol for a randomized controlled trial. To develop a functional rehabilitation intervention for the CORKA trial. |
|
| Vestøl et al., 2020 [31] The importance of a good therapeutic alliance in promoting exercise motivation in a group of older Norwegians in the subacute phase of hip fracture; a qualitative study Norway | Qualitative descriptive study. To explore how older people who had participated in an evidence-based exercise intervention describe their relationship with their therapists and how this relationship might contribute to their motivation for exercise. |
|
| Barker et al., 2021 [27] Home-based rehabilitation programme compared with traditional physiotherapy for patients at risk of poor outcome after knee arthroplasty: the CORKA randomised controlled trial United Kingdom | Randomized controlled trial. To evaluate whether a home-based rehabilitation program for people at risk of a poor outcome after knee arthroplasty offers superior outcomes to traditional outpatient physiotherapy. |
|
| Meng et al., 2022 [37] Effectiveness of self-efficacy-enhancing interventions on rehabilitation following total hip replacement: a randomized controlled trial with six-month follow-up China | Randomized controlled trial. To explore the effect of a self-efficacy-enhancing intervention program following hip replacement on patients’ rehabilitation outcomes (self-efficacy, functional exercise compliance, hip function, activity and social participation, anxiety and depression, and quality of life). |
|
| Bieler et al., 2022 [29] Effectiveness of promotion and support for physical activity maintenance post total hip arthroplasty-study protocol for a pragmatic, assessor-blinded, randomized controlled trial Denmark | Randomized controlled trial. To investigate whether the promotion and support of physical activity initiated 3 months after total hip arthroplasty complementary to usual rehabilitation care can increase objective measured physical activity 6 months post-surgery. |
|
| Deng et al., 2022 [36] A self-efficacy-enhancing intervention for Chinese patients after total hip arthroplasty: study protocol for a randomized controlled trial with 6-month follow-up China | Study protocol for a randomized controlled trial. To develop and assess the feasibility of a self-efficacy-enhancing intervention to improve exercise adherence in patients undergoing total hip arthroplasty. |
|
| Lee and Lee, 2022 [38] Effectiveness of Multicomponent Home-Based Rehabilitation in Elderly Patients after Hip Fracture Surgery: A Randomized Controlled Trial South Korea | Randomized controlled trial. To assess the clinical effectiveness of an 8-week personalized multicomponent home-based rehabilitation program by comparing it with a home exercise program after discharge. |
|
3.1. Mastery Experiences
3.2. Vicarious Experience
3.3. Verbal Persuasion
3.4. Physiological and Affective States
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bigham-Sadegh, A.; Oryan, A. Basic concepts regarding fracture healing and the current options and future directions in managing bone fractures. Int. Wound J. 2015, 12, 238–247. [Google Scholar] [CrossRef] [PubMed]
- Bergh, C.; Wennergren, D.; Moller, M.; Brisby, H. Fracture incidence in adults in relation to age and gender: A study of 27,169 fractures in the Swedish Fracture Register in a well-defined catchment area. PLoS ONE 2020, 15, e0244291. [Google Scholar] [CrossRef] [PubMed]
- Collaborators, G.B.D.F. Global, regional, and national burden of bone fractures in 204 countries and territories, 1990–2019: A systematic analysis from the Global Burden of Disease Study 2019. Lancet Healthy Longev. 2021, 2, e580–e592. [Google Scholar] [CrossRef]
- Polinder, S.; Haagsma, J.; Panneman, M.; Scholten, A.; Brugmans, M.; Van Beeck, E. The economic burden of injury: Health care and productivity costs of injuries in the Netherlands. Accid. Anal. Prev. 2016, 93, 92–100. [Google Scholar] [CrossRef]
- Perry, S.B.; Downey, P.A. Fracture risk and prevention: A multidimensional approach. Phys. Ther. 2012, 92, 164–178. [Google Scholar] [CrossRef]
- Luan, X.; Tian, X.; Zhang, H.; Huang, R.; Li, N.; Chen, P.; Wang, R. Exercise as a prescription for patients with various diseases. J. Sport Health Sci. 2019, 8, 422–441. [Google Scholar] [CrossRef]
- Peek, K.; Sanson-Fisher, R.; Mackenzie, L.; Carey, M. Interventions to aid patient adherence to physiotherapist prescribed self-management strategies: A systematic review. Physiotherapy 2016, 102, 127–135. [Google Scholar] [CrossRef]
- England, P.H. Health Matters: Physical Activity—Prevention and Management of Long-Term Conditions. Available online: https://www.gov.uk/government/publications/health-matters-physical-activity/health-matters-physical-activity-prevention-and-management-of-long-term-conditions (accessed on 8 February 2023).
- Room, J.; Boulton, M.; Dawes, H.; Archer, K.; Barker, K. Physiotherapists’ perceptions of how patient adherence and non-adherence to recommended exercise for musculoskeletal conditions affects their practice: A qualitative study. Physiotherapy 2021, 113, 107–115. [Google Scholar] [CrossRef]
- Jack, K.; McLean, S.M.; Moffett, J.K.; Gardiner, E. Barriers to treatment adherence in physiotherapy outpatient clinics: A systematic review. Man. Ther. 2010, 15, 220–228. [Google Scholar] [CrossRef]
- Gesar, B.; Hommel, A.; Hedin, H.; Baath, C. Older patients’ perception of their own capacity to regain pre-fracture function after hip fracture surgery—An explorative qualitative study. Int. J. Orthop. Trauma Nurs. 2017, 24, 50–58. [Google Scholar] [CrossRef]
- Griffiths, F.; Mason, V.; Boardman, F.; Dennick, K.; Haywood, K.; Achten, J.; Parsons, N.; Griffin, X.; Costa, M. Evaluating recovery following hip fracture: A qualitative interview study of what is important to patients. BMJ Open 2015, 5, e005406. [Google Scholar] [CrossRef] [PubMed]
- Hagsten, B.; Svensson, O.; Gardulf, A. Early individualized postoperative occupational therapy training in 100 patients improves ADL after hip fracture: A randomized trial. Acta Orthop. Scand. 2004, 75, 177–183. [Google Scholar] [CrossRef] [PubMed]
- Fu, W.; Li, Y.; Liu, Y.; Li, D.; Wang, G.; Liu, Y.; Zhang, T.; Zheng, Y. The influence of different physical exercise amounts on learning burnout in adolescents: The mediating effect of self-efficacy. Front. Psychol. 2023, 14, 1089570. [Google Scholar] [CrossRef]
- Isa, T.; Ueda, Y.; Nakamura, R.; Misu, S.; Ono, R. Relationship between the intention-behavior gap and self-efficacy for physical activity during childhood. J. Child Health Care Prof. Work. Child. Hosp. Community 2019, 23, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, M.M.; Zebis, M.K.; Langberg, H.; Poulsen, O.M.; Mortensen, O.S.; Jensen, J.N.; Sjogaard, G.; Bredahl, T.; Andersen, L.L. Influence of self-efficacy on compliance to workplace exercise. Int. J. Behav. Med. 2013, 20, 365–370. [Google Scholar] [CrossRef] [PubMed]
- Pekmezi, D.; Jennings, E.; Marcus, B.H. Evaluating and Enhancing Self-Efficacy for Physical Activity. ACSM’s Health Fit. J. 2009, 13, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A.; Freeman, W.H.; Lightsey, R. Self-Efficacy: The Exercise of Control. J. Cogn. Psychother. 1999, 13, 158–166. [Google Scholar] [CrossRef]
- Bandura, A. Self-Efficacy: The Exercise of Control; Freeman: New York, NY, USA, 1997. [Google Scholar]
- Pudkasam, S.; Feehan, J.; Talevski, J.; Vingrys, K.; Polman, R.; Chinlumprasert, N.; Stojanovska, L.; Apostolopoulos, V. Motivational strategies to improve adherence to physical activity in breast cancer survivors: A systematic review and meta-analysis. Maturitas 2021, 152, 32–47. [Google Scholar] [CrossRef]
- Argent, R.; Daly, A.; Caulfield, B. Patient Involvement With Home-Based Exercise Programs: Can Connected Health Interventions Influence Adherence? JMIR mHealth uHealth 2018, 6, e47. [Google Scholar] [CrossRef]
- McGrane, N.; Galvin, R.; Cusack, T.; Stokes, E. Addition of motivational interventions to exercise and traditional physiotherapy: A review and meta-analysis. Physiotherapy 2015, 101, 1–12. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Aromataris, E.; Munn, Z. JBI Manual for Evidence Synthesis; JBI: Eagan, MN, USA, 2020. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V.; Hayfield, N.; Terry, G. Handbook of Research Methods in Health Social Sciences; Liamputtong P.: Singapore, 2019. [Google Scholar]
- Barker, K.L.; Room, J.; Knight, R.; Dutton, S.; Toye, F.; Leal, J.; Kenealy, N.; Maia Schlussel, M.; Collins, G.; Beard, D.; et al. Home-based rehabilitation programme compared with traditional physiotherapy for patients at risk of poor outcome after knee arthroplasty: The CORKA randomised controlled trial. BMJ Open 2021, 11, e052598. [Google Scholar] [CrossRef] [PubMed]
- Room, J.; Batting, M.; Barker, K.L. Development of a functional rehabilitation intervention for post knee arthroplasty patients: COmmunity based Rehabilitation post Knee Arthroplasty (CORKA) trial. Physiotherapy 2020, 106, 52–64. [Google Scholar] [CrossRef]
- Bieler, T.; Magnusson, S.P.; Siersma, V.; Rinaldo, M.; Schmiegelow, M.T.; Beck, T.; Krifa, A.M.; Kjaer, B.H.; Palm, H.; Midtgaard, J. Effectiveness of promotion and support for physical activity maintenance post total hip arthroplasty-study protocol for a pragmatic, assessor-blinded, randomized controlled trial (the PANORAMA trial). Trials 2022, 23, 647. [Google Scholar] [CrossRef] [PubMed]
- Sipila, S.; Salpakoski, A.; Edgren, J.; Heinonen, A.; Kauppinen, M.A.; Arkela-Kautiainen, M.; Sihvonen, S.E.; Pesola, M.; Rantanen, T.; Kallinen, M. Promoting mobility after hip fracture (ProMo): Study protocol and selected baseline results of a year-long randomized controlled trial among community-dwelling older people. BMC Musculoskelet. Disord. 2011, 12, 277. [Google Scholar] [CrossRef]
- Vestol, I.; Debesay, J.; Pajalic, Z.; Bergland, A. The importance of a good therapeutic alliance in promoting exercise motivation in a group of older Norwegians in the subacute phase of hip fracture; a qualitative study. BMC Geriatr. 2020, 20, 118. [Google Scholar] [CrossRef]
- Olsson, L.E.; Karlsson, J.; Ekman, I. Effects of nursing interventions within an integrated care pathway for patients with hip fracture. J. Adv. Nurs. 2007, 58, 116–125. [Google Scholar] [CrossRef]
- Harmelink, K.E.M.; Zeegers, A.; Tonis, T.M.; Hullegie, W.; Nijhuis-van der Sanden, M.W.G.; Staal, J.B. The effectiveness of the use of a digital activity coaching system in addition to a two-week home-based exercise program in patients after total knee arthroplasty: Study protocol for a randomized controlled trial. BMC Musculoskelet. Disord. 2017, 18, 290. [Google Scholar] [CrossRef]
- Casado, B.L.; Resnick, B.; Zimmerman, S.; Nahm, E.S.; Orwig, D.; Macmillan, K.; Magaziner, J. Social support for exercise by experts in older women post-hip fracture. J. Women Aging 2009, 21, 48–62. [Google Scholar] [CrossRef]
- Resnick, B.; Orwig, D.; Yu-Yahiro, J.; Hawkes, W.; Shardell, M.; Hebel, J.R.; Zimmerman, S.; Golden, J.; Werner, M.; Magaziner, J. Testing the effectiveness of the exercise plus program in older women post-hip fracture. Ann. Behav. Med. Publ. Soc. Behav. Med. 2007, 34, 67–76. [Google Scholar] [CrossRef] [PubMed]
- Deng, B.; Chen, Y.; Meng, Y.; Zhang, Y.; Tan, X.; Zhou, X.; Zhang, M. A self-efficacy-enhancing intervention for Chinese patients after total hip arthroplasty: Study protocol for a randomized controlled trial with 6-month follow-up. J. Orthop. Surg. Res. 2022, 17, 1. [Google Scholar] [CrossRef] [PubMed]
- Meng, Y.; Deng, B.; Liang, X.; Li, J.; Li, L.; Ou, J.; Yu, S.; Tan, X.; Chen, Y.; Zhang, M. Effectiveness of self-efficacy-enhancing interventions on rehabilitation following total hip replacement: A randomized controlled trial with six-month follow-up. J. Orthop. Surg. Res. 2022, 17, 225. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Lee, S.H. Effectiveness of Multicomponent Home-Based Rehabilitation in Elderly Patients after Hip Fracture Surgery: A Randomized Controlled Trial. J. Pers. Med. 2022, 12, 649. [Google Scholar] [CrossRef]
- Ardito, R.B.; Rabellino, D. Therapeutic alliance and outcome of psychotherapy: Historical excursus, measurements, and prospects for research. Front. Psychol. 2011, 2, 270. [Google Scholar] [CrossRef]
- Kornhaber, R.; Walsh, K.; Duff, J.; Walker, K. Enhancing adult therapeutic interpersonal relationships in the acute health care setting: An integrative review. J. Multidiscip. Healthc. 2016, 9, 537–546. [Google Scholar] [CrossRef]
- Dambi, J.M.; Mavhu, W.; Beji-Chauke, R.; Kaiyo-Utete, M.; Mills, R.; Shumba, R.; Muchemwa, S.; Musesengwa, R.; Verhey, R.; Abas, M.; et al. The impact of working alliance in managing youth anxiety and depression: A scoping review. npj Mental Health Res. 2023, 2. [Google Scholar] [CrossRef]
- Barbisan, G.K.; de Pieri, L.Z.; Goncalves, L.; Reboucas, C.D.V.; da Rocha, N.S. Positive Association Between Therapeutic Alliance and Quality of Life in Psychodynamic Psychotherapy, Cognitive Behavior Therapy, and Interpersonal Therapy: The Patient’s Perspective. Front. Psychiatry 2021, 12, 613627. [Google Scholar] [CrossRef]
- Allen, M.L.; Cook, B.L.; Carson, N.; Interian, A.; La Roche, M.; Alegria, M. Patient-Provider Therapeutic Alliance Contributes to Patient Activation in Community Mental Health Clinics. Adm. Policy Ment. Health 2017, 44, 431–440. [Google Scholar] [CrossRef]
- Comer, A.; Fettig, L.; Torke, A.M. Identifying Goals of Care. Med. Clin. N. Am. 2020, 104, 767–775. [Google Scholar] [CrossRef]
- Schellinger, S.E.; Anderson, E.W.; Frazer, M.S.; Cain, C.L. Patient Self-Defined Goals: Essentials of Person-Centered Care for Serious Illness. Am. J. Hosp. Palliat. Care 2018, 35, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Punga, A.R.; Westerberg, E.; Asenlof, P. Implementation of tailored exercise programs for MG patients in a gym setting: A pragmatic feasibility case study. Neuromuscul. Disord. NMD 2023, 33, 334–338. [Google Scholar] [CrossRef] [PubMed]
- Tavares, E.; Coelho, J.; Rogado, P.; Correia, R.; Castro, C.; Fernandes, J.B. Barriers to Gait Training among Stroke Survivors: An Integrative Review. J. Funct. Morphol. Kinesiol. 2022, 7, 85. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, J.B.; Fernandes, S.B.; Almeida, A.S.; Vareta, D.A.; Miller, C.A. Older Adults’ Perceived Barriers to Participation in a Falls Prevention Strategy. J. Pers. Med. 2021, 11, 450. [Google Scholar] [CrossRef] [PubMed]
- Jansen, F.; Eerenstein, S.E.J.; Cnossen, I.C.; Lissenberg-Witte, B.I.; de Bree, R.; Doornaert, P.; Halmos, G.B.; Hardillo, J.A.U.; van Hinte, G.; Honings, J.; et al. Effectiveness of a guided self-help exercise program tailored to patients treated with total laryngectomy: Results of a multi-center randomized controlled trial. Oral Oncol. 2020, 103, 104586. [Google Scholar] [CrossRef] [PubMed]
- Lee, F.I.; Lee, T.D.; So, W.K. Effects of a tailor-made exercise program on exercise adherence and health outcomes in patients with knee osteoarthritis: A mixed-methods pilot study. Clin. Interv. Aging 2016, 11, 1391–1402. [Google Scholar] [CrossRef] [PubMed]
- Shao, J.H.; Yu, K.H.; Chen, S.H. Effectiveness of a self-management program for joint protection and physical activity in patients with rheumatoid arthritis: A randomized controlled trial. Int. J. Nurs. Stud. 2021, 116, 103752. [Google Scholar] [CrossRef]
- Hiraga, Y.; Hisano, S.; Nomiyama, K.; Hirakawa, Y. Effects of using activity diary for goal setting in occupational therapy on reducing pain and improving psychological and physical performance in patients after total knee arthroplasty: A non-randomised controlled study. Hong Kong J. Occup. Ther. HKJOT 2019, 32, 53–61. [Google Scholar] [CrossRef]
- Belogianni, K.; Baldwin, C. Types of Interventions Targeting Dietary, Physical Activity, and Weight-Related Outcomes among University Students: A Systematic Review of Systematic Reviews. Adv. Nutr. 2019, 10, 848–863. [Google Scholar] [CrossRef]
- Foti, F.; Menghini, D.; Alfieri, P.; Costanzo, F.; Mandolesi, L.; Petrosini, L.; Vicari, S. Learning by observation and learning by doing in Down and Williams syndromes. Dev. Sci. 2018, 21, e12642. [Google Scholar] [CrossRef]
- Lockwood, P.L. The anatomy of empathy: Vicarious experience and disorders of social cognition. Behav. Brain Res. 2016, 311, 255–266. [Google Scholar] [CrossRef] [PubMed]
- Bose, S.; Dun, C.; Zhang, G.Q.; Walsh, C.; Makary, M.A.; Hicks, C.W. Medicare Beneficiaries In Disadvantaged Neighborhoods Increased Telemedicine Use During The COVID-19 Pandemic. Health Aff. 2022, 41, 635–642. [Google Scholar] [CrossRef] [PubMed]
- Gordon, B. Why You Should Keep a Close Eye on Telehealth. Available online: https://www.apta.org/article/2020/01/08/why-you-should-keep-a-close-eye-on-telehealth (accessed on 18 June 2023).
- Bombard, Y.; Baker, G.R.; Orlando, E.; Fancott, C.; Bhatia, P.; Casalino, S.; Onate, K.; Denis, J.L.; Pomey, M.P. Engaging patients to improve quality of care: A systematic review. Implement. Sci. IS 2018, 13, 98. [Google Scholar] [CrossRef] [PubMed]
- Nicolson, P.J.A.; Hinman, R.S.; French, S.D.; Lonsdale, C.; Bennell, K.L. Improving Adherence to Exercise: Do People With Knee Osteoarthritis and Physical Therapists Agree on the Behavioral Approaches Likely to Succeed? Arthritis Care Res. 2018, 70, 388–397. [Google Scholar] [CrossRef]
| Parameter | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Population | Patients with lower limb fractures; Adults ≥ 18 years old. | Other health conditions besides lower limb fractures; Participants < 18 years old. |
| Concept | Studies that explore motivational strategies developed by healthcare professionals. | Studies that do not address motivational strategies. |
| Context | Studies conducted in rehabilitation settings (e.g., acute, post-acute, and long-term care). | Studies conducted in non-healthcare or non-rehabilitation settings. |
| Domain | Strategies | Interventions |
|---|---|---|
| Mastery experiences | Therapeutic alliance | A thorough interview on admission. |
| Develop a trusting and motivating relationship. | ||
| Feelings of mutuality and respect in the alliance. | ||
| Face-to-face counseling sessions. | ||
| Health literacy | Educate patients in rehabilitation exercise, complications, disease, and the benefits of exercise. | |
| Provide information leaflets/booklets. | ||
| Cueing with posters describing the exercises. | ||
| Set achievable goals | Identify patients’ abilities and needs. | |
| Confer with patients to develop functional exercise goals at different stages of rehabilitation. | ||
| Physical activity diary. | ||
| Calendar of daily exercise activities. | ||
| Personalize the rehabilitation program | Develop an individually tailored exercise program. | |
| Tailor the instruction and program to make the task understandable. | ||
| Manage unpleasant sensations | Identifying the challenges of postoperative rehabilitation through discussion. | |
| Use prescribed medications or heat/ice treatment to relieve or decrease pain. | ||
| Vicarious experience | Sharing cases | Share previous success stories to build confidence and motivate patients. |
| Problem-solving method | Identify obstacles to participating in the rehabilitation program. | |
| Use the problem-solving method to address perceived obstacles to participation in rehabilitation programs. | ||
| Verbal persuasion | Persuasion | Describe the benefits of physical activities. |
| Behavioral contract. | ||
| Regular contact with patients via phone. | ||
| Encouragement and compliments | Assert that participants can self-manage. | |
| Provide positive verbal feedback on their efforts. | ||
| Give verbal encouragement and compliments. | ||
| Motivation interviewing. | ||
| Reinforce participants’ past and present successes or accomplishments. | ||
| Family involvement. | ||
| Digital activity coaching system. | ||
| Physiological and affective states | Avoid negative emotional stimulation | Assess patients’ expressions of anxiety and depression. |
| Help to seek support | Telephone-assisted counseling. | |
| Identify individual barriers and resources for performing the exercise plan. | ||
| Provide strategies for dealing with the identified barriers and coping in the future. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernandes, J.B.; Ferreira, N.; Domingos, J.; Ferreira, R.; Amador, C.; Pardal, N.; Castro, C.; Simões, A.; Fernandes, S.; Bernardes, C.; et al. Health Professionals’ Motivational Strategies to Enhance Adherence in the Rehabilitation of People with Lower Limb Fractures: Scoping Review. Int. J. Environ. Res. Public Health 2023, 20, 7050. https://doi.org/10.3390/ijerph20227050
Fernandes JB, Ferreira N, Domingos J, Ferreira R, Amador C, Pardal N, Castro C, Simões A, Fernandes S, Bernardes C, et al. Health Professionals’ Motivational Strategies to Enhance Adherence in the Rehabilitation of People with Lower Limb Fractures: Scoping Review. International Journal of Environmental Research and Public Health. 2023; 20(22):7050. https://doi.org/10.3390/ijerph20227050
Chicago/Turabian StyleFernandes, Júlio Belo, Noélia Ferreira, Josefa Domingos, Rui Ferreira, Catarina Amador, Nelson Pardal, Cidália Castro, Aida Simões, Sónia Fernandes, Catarina Bernardes, and et al. 2023. "Health Professionals’ Motivational Strategies to Enhance Adherence in the Rehabilitation of People with Lower Limb Fractures: Scoping Review" International Journal of Environmental Research and Public Health 20, no. 22: 7050. https://doi.org/10.3390/ijerph20227050
APA StyleFernandes, J. B., Ferreira, N., Domingos, J., Ferreira, R., Amador, C., Pardal, N., Castro, C., Simões, A., Fernandes, S., Bernardes, C., Vareta, D. A., Peças, D., Ladislau, D., Sousa, N., Duarte, A., & Godinho, C. (2023). Health Professionals’ Motivational Strategies to Enhance Adherence in the Rehabilitation of People with Lower Limb Fractures: Scoping Review. International Journal of Environmental Research and Public Health, 20(22), 7050. https://doi.org/10.3390/ijerph20227050