
A Scoping Review of the Serious Game-Based Rehabilitation of People with Cerebral Palsy


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Search Strategy
2.3. Study Selection
2.4. Searching Process
2.5. Data Extraction and Quality Assessments
3. Results
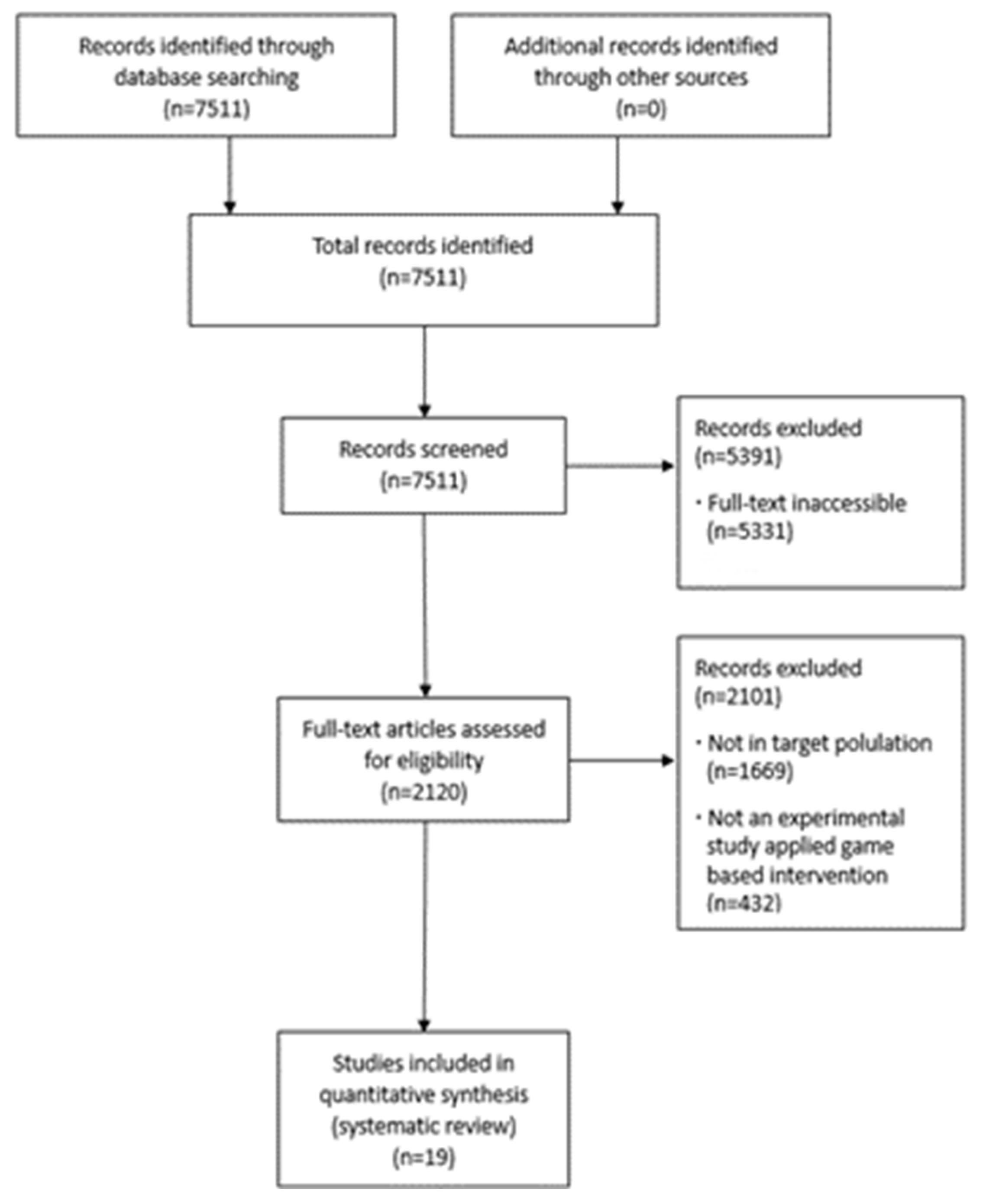
3.1. Search Results
3.2. Methodological Quality of Studies
3.3. Population
3.4. Interventions
3.5. Outcome Measurements
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Evidence of Interventions in Games Used in Serious Contexts for Persons with Cerebral Palsy

{kind=link}
| Author | Level of Evidence/Participants/Age Groups | Intervention | Outcome Measurements | Outcome | ||
|---|---|---|---|---|---|---|
| Group | Session/Time | |||||
| Sajan, John, Grace, Sabu, and Tharion [29] | Level I N = 20 Children with CP Age groups: achool-age child, adolescent | Intervention: interactive video gaming with Nintendo Wii Control: conventional therapy | 40 min, 6 days per week, 3 weeks |
| Interactive video gaming with Nintendo Wii may be offered as an effective supplement to conventional therapy in the rehabilitation of children with CP | |
| Szturm et al. [40] | Level I N = 20 Children with CP Age groups: preschooler, school-age child | Intervention: novel game-based dual-task balance exercise program Control: Conventional physical therapy balance program | 45 min, 3 days per week, 12 weeks |
| The study demonstrates feasible trial procedures and acceptable dual-task-oriented training with a high compliance rate and positive outcomes | |
| Velasco et al. [31] | Level I N = 10 User with CP Age groups: chool-age child | Intervention: cervical and trunk control based on serious videogames and physical exercise Control: Nnon-intervention phase | 25–30 min, 10 sessions |
| Physical therapy, which combines serious games with traditional rehabilitation, can help children with CP achieve better trunk and cervical functions | |
| Wade and Porter [15] | Level I (randomized cross-over trial) N = 13 Young people with cerebral palsy Age groups: school-age child, adolescent | Intervention: a seat “cushion” containing a platform was based on a modified games controller Control: traditional physical and occupational therapy | 3 months |
| The study provides evidence that meaningful and engaging therapeutic activities using computer games controlled by upper body tilt can help to improve sitting skills in children with neuromotor dysfunctions | |
| Zoccolillo et al. [28] | Level I (randomized cross-over trial) N = 22 Children with CP Age groups: preschooler, school-age child, adolescent | Intervention: video-game-based therapy using Xbox with Kinect device Control: conventional therapy | 1 h, twice a week, 8 weeks |
| Video-game-based therapy using Xbox with Kinect device was effective in improving the motor functions of upper limb extremities in children with CP | |
| Amengual Alcover, Jaume-i-Capó, and Moyà-Alcover [13] | Level III N = 9 Spastic hemiplegia and diplegia with CP Age groups: adult | Intervention: PROGame | 20 min, 24 weeks |
| These findings show significant improvements in gait and balance functions, indicators of greater independence in participating adults | |
| Camara Machado et al. [4] | Level III N = 28 Children with CP Age groups: school-age child | Intervention: Xbox 360 Kinect games used in the rehabilitation program | 40 min, twice a week, 2 months |
| The intervention led to important motor function enhancements | |
| Jaume-i-Capó, Martínez-Bueso, Moyà-Alcover, and Varona [36] | Level III N = 9 Adults diagnosed with CP Age groups: adults | Intervention: serious games for balance rehabilitation therapy | 20 min, one session per week, 24 weeks |
| Serious games for balance rehabilitation showed significant increases in balance and gait function scores, increasing the independence of participating adults | |
| Keller and Van Hedel [37] | Level III N = 11 Children and adolescents with CP Age groups: school-age child, adolescent | Intervention: Armeo® Spring the exergame Moorhuhn | 70 min, 3 days, 2 weeks |
| Motor learning performed to train children with CP on affected arm with weight support in a playful, virtual environment | |
| Luna-Oliva et al. [38] | Level III N = 11 Spastic hemiplegia and diplegia with CP Age groups: school-age child | Intervention: Xbox 360 Kinect at school | 30 min, 2 days a week, 2 months |
| Our Kinect Xbox 360 protocol showed improvements in balance and activities of daily living in CP participants in a school setting | |
| Sandlund, Lindh Waterworth, and Häger [42] | Level III N = 14 Children with CP Age groups: school-age child | Intervention: home-based intervention using the EyeToy for PlayStation2 | 4 weeks |
| Motion interactive games in a home rehabilitation setting is highly feasible to use for children with CP | |
| Do, Yoo, Jung, and Park [32] | Level IV N = 3 Spastic hemiplegia with CP Age groups: preschooler, school-age child | Intervention: bilateral arm training using Nintendo Wii game | 30 min, 12 sessions, 10 weeks |
| Bilateral coordination ability and upper limb motor skills on the affected side improved more than during the baseline period | |
| MacIntosh, Desailly, Vignais, Vigneron, and Biddiss [30] | Level IV N = 19 Young people with CP Age groups: school-age child, adolescent | Intervention: biofeedback-enhanced therapeutic exercise video game intervention at home | 60 min, once per week, 4 weeks |
| Combining SFC-style coaching using high-quality biofeedback can complement traditional therapies by positively training adolescents in a home rehabilitation setting | |
| Peper, Van Loon, Van de Rijt, Salverda, and van Kuijk [39] | Level IV N = 6 Spastic hemiplegia with CP Age groups: school-age child | Intervention: Lissajous-based training on bimanual performance | 9 h for more than 6 weeks |
| Our results evaluate the relationship between the specificity of the AHA and the expected benefits of combining the proposed training with a dedicated ambidextrous functional training program | |
| Barton, Hawken, Foster, Holmes, and Butler [14] | Level V N = 1 Spastic diplegia with CP Age groups: school-age child | Intervention: Goblin Post Office game on the CAREN virtual rehabilitation system | 30 min, twice a week, 6 weeks |
| Co-contractions causing increased coupling are expected to reduce over longer exposure times to training | |
| Burdea et al. [41] | Level V N = 3 Children with CP Age groups: school-age child | Intervention: playing two custom virtual reality games | 3 times per week, 12 weeks |
| Game technology is suitable for the age group and is accepted by the participants, supporting the hypothesis that the game-based robotic training of the ankle is beneficial for walking in children with CP | |
| Moldovan, Ghircău, Podar, Rîză, and Moldovan [33] | Level V N = 1 Spastic hemiplegia with CP Age groups: school-age child | Intervention: MIRA exergames with Kinect Xbox® sensor | 30 min, 3 sessions a week, 14 months |
| Long-term virtual occupational therapy associated with the conventional rehabilitation program improved motor function and performance in a child with cerebral palsy and hemiparesis | |
| Reifenberg et al. [34] | Level V N = 1 Spastic hemiplegia with CP Age groups: preschooler | Intervention: game-based neurorehabilitation using telehealth technologies | 7 h for 8 weeks |
| It is feasible to administer game-based neurorehabilitation to a child with cerebral palsy | |
| Sanjay, Kanitkar, Szturm, Gaonkar, and Ankolekar [35] | Level V N = 1 Left spastic hemiplegia with CP Age groups: preschooler | Intervention: computer game-assisted repetitive task practice-based upper extremity therapy program | 40–60 min, 2~3 days per week, 16 weeks |
| The feasibility and acceptability of the G-RTP program demonstrated for use by children with UE motor impairments | |
References
- Digiacomo, F.; Tamburin, S.; Tebaldi, S.; Pezzani, M.; Tagliafierro, M.; Casale, R.; Bartolo, M. Improvement of motor performance in children with cerebral palsy treated with exoskeleton robotic training: A retrospective explorative analysis. Restor. Neurol. Neurosci. 2019, 37, 239–244. [Google Scholar] [CrossRef] [PubMed]
- Elnaggar, R.K.; Alqahtani, B.A.; Elbanna, M.F. Functional outcomes of botulinum neurotoxin-A injection followed by reciprocal electrical stimulation in children with cerebral palsy: A randomized controlled trial. Restor. Neurol. Neurosci. 2020, 38, 431–441. [Google Scholar] [CrossRef] [PubMed]
- Eunson, P. Aetiology and epidemiology of cerebral palsy. J. Paediatr. Child. Health 2012, 22, 361–366. [Google Scholar] [CrossRef]
- Camara Machado, F.R.; Antunes, P.P.; Souza, J.D.M.; Santos, A.C.D.; Levandowski, D.C.; Oliveira, A.A.D. Motor improvement using motion sensing game devices for cerebral palsy rehabilitation. J. Mot. Behav. 2017, 49, 273–280. [Google Scholar] [CrossRef]
- Taub, E.; Ramey, S.L.; DeLuca, S.; Echols, K. Efficacy of constraint-induced movement therapy for children with cerebral palsy with asymmetric motor impairment. Pediatrics 2004, 113, 305–312. [Google Scholar] [CrossRef]
- Imam, M.H.A.; Jahan, I.; Das, M.C.; Muhit, M.; Smithers-Sheedy, H.; McIntyre, S.; Badawi, N.; Khandaker, G. Rehabilitation status of children with cerebral palsy in Bangladesh: Findings from the Bangladesh Cerebral Palsy Register. PLoS ONE 2021, 16, e0250640. [Google Scholar] [CrossRef]
- Weightman, A.; Preston, N.; Levesley, M.; Holt, R.; Mon-Williams, M.; Clarke, M.; Cozens, A.J.; Bhakta, B. Home-Based computer-assisted upper limb exercise for young children with cerebral palsy: A feasibility study investigating impact on motor and functional outcome. J. Rehabil. Med. 2011, 43, 359–363. [Google Scholar] [CrossRef]
- Karni, A.; Meyer, G.; Jezzard, P.; Adams, M.M.; Turner, R.; Ungerleider, L.G. Functional MRI evidence for adult motor cortex plasticity during motor skill learning. Nature 2000, 377, 155–158. [Google Scholar] [CrossRef]
- Liepert, J.; Bauder, H.; Miltner, W.H.; Taub, E.; Weiller, C. Treatment-induced cortical reorganization after stroke in humans. Stroke 2000, 31, 1210–1216. [Google Scholar] [CrossRef]
- Bilde, P.; Kliim-Due, M.; Rasmussen, B.; Petersen, L.; Petersen, T.; Nielsen, J. Individualized, home-based interactive training of cerebral palsy children delivered through the internet. BMC Med. 2011, 11, 32. [Google Scholar] [CrossRef]
- Christman, E.; McAllister, K.; Claar, K.; Kaufman, S.; Page, S.J. Occupational therapists’ opinions of two pediatric constraint-induced movement therapy protocols. Am. J. Occup. Ther. 2015, 69, 6906180020p1–6906180020p7. [Google Scholar] [CrossRef]
- Eugster-Buesch, F.; de Bruin, E.D.; Boltshauser, E.; Steinlin, M.; Küenzle, C.; Müller, E.; Capone, A.; Pfann, R.; Meyer-Heim, A. Forced-use therapy for children with cerebral palsy in the community setting: A single-blinded randomized controlled pilot trial. J. Pediatr. Rehabil. Med. 2012, 5, 65–74. [Google Scholar] [CrossRef]
- Amengual Alcover, E.; Jaume-i-Capó, A.; Moyà-Alcover, B. PROGame: A process framework for serious game development for motor rehabilitation therapy. PLoS ONE 2018, 13, e0197383. [Google Scholar] [CrossRef] [PubMed]
- Barton, G.J.; Hawken, M.B.; Foster, R.J.; Holmes, G.; Butler, P.B. The effects of virtual reality game training on trunk to pelvis coupling in a child with cerebral palsy. J. Neuroeng. Rehabil. 2013, 10, 15. [Google Scholar] [CrossRef]
- Wade, W.; Porter, D. Sitting playfully: Does the use of a centre of gravity computer game controller influence the sitting ability of young people with cerebral palsy? Disabil. Rehabil. Assist. Technol. 2012, 7, 122–129. [Google Scholar] [CrossRef]
- Lopes, S.; Magalhães, P.; Pereira, A.; Martins, J.; Magalhães, C.; Chaleta, E.; Rosário, P. Games used with serious purposes: A systematic review of interventions in patients with cerebral palsy. Front. Psychol. 2018, 9, 1712. [Google Scholar] [CrossRef] [PubMed]
- Salem, Y.; Godwin, E.M. Effects of task-oriented training on mobility function in children with cerebral palsy. NeuroRehabilitation 2009, 24, 307–313. [Google Scholar] [CrossRef]
- Maclean, N.; Pound, P.; Wolfe, C.; Rudd, A. The concept of patient motivation: A qualitative analysis of stroke professionals’ attitudes. Stroke 2002, 33, 444–448. [Google Scholar] [CrossRef]
- Bryanton, C.; Bosse, J.; Brien, M.; Mclean, J.; McCormick, A.; Sveistrup, H. Feasibility, motivation, and selective motor control: Virtual reality compared to conventional home exercise in children with cerebral palsy. Cyberpsychol. Behav. 2006, 9, 123–128. [Google Scholar] [CrossRef] [PubMed]
- Bonnechere, B.; Jansen, B.; Omelina, L.; Degelaen, M.; Wermenbol, V.; Rooze, M.; Jan, S.V.S. Can serious games be incorporated with conventional treatment of children with cerebral palsy? a review. Res. Dev. Disabil. 2014, 35, 1899–1913. [Google Scholar] [CrossRef]
- Ravi, D.K.; Kumar, N.; Singhi, P. Effectiveness of virtual reality rehabilitation for children and adolescents with cerebral palsy: An updated evidence-based systematic review. Physiotherapy 2017, 103, 245–258. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- World Health Organization. Towards a Common Language for Functioning, Disability and Health: ICF; World Health Organization: Geneva, Switzerland, 2002. [Google Scholar]
- Arbesman, M.; Scheer, J.; Lieberman, D. Using AOTA’s critically appraised topic (CAT) and critically appraised paper (CAP) series to link evidence to practice. OT Pract. 2008, 13, 18–22. [Google Scholar]
- Ahn, S.N. A Systematic Review of Interventions Related to Body Awareness in Childhood. Int. J. Environ. Res. Public Health 2022, 19, 8900. [Google Scholar] [CrossRef]
- Law, M.; Stewart, D.; Letts, L.; Pollock, N.; Bosch, J.; Westmorland, M. Critical Review Form–Quantitative Studies; McMaster University: Hamilton, ON, Canada, 1998. [Google Scholar]
- Barclay, L.; McDonald, R.; Lentin, P. Social and community participation following spinal cord injury: A critical review. Int. J. Rehabil. Res. 2015, 38, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Zoccolillo, L.; Morelli, D.; Cincotti, F.; Muzzioli, L.; Gobbetti, T.; Paolucci, S.; Iosa, M. Video-game based therapy performed by children with cerebral palsy: A cross-over randomized controlled trial and a cross-sectional quantitative measure of physical activity. Eur. J. Phys. Rehabil. Med. 2015, 51, 669–676. [Google Scholar]
- Sajan, J.E.; John, J.A.; Grace, P.; Sabu, S.S.; Tharion, G. Wii-based interactive video games as a supplement to conventional therapy for rehabilitation of children with cerebral palsy: A pilot, randomized controlled trial. Dev. Neurorehabil. 2017, 20, 361–367. [Google Scholar] [CrossRef]
- MacIntosh, A.; Desailly, E.; Vignais, N.; Vigneron, V.; Biddiss, E. A biofeedback-enhanced therapeutic exercise video game intervention for young people with cerebral palsy: A randomized single-case experimental design feasibility study. PLoS ONE 2020, 15, e0234767. [Google Scholar] [CrossRef]
- Velasco, M.A.; Raya, R.; Muzzioli, L.; Morelli, D.; Otero, A.; Iosa, M.; Cincotti, F.; Rocon, E. Evaluation of cervical posture improvement of children with cerebral palsy after physical therapy based on head movements and serious games. Biomed. Eng. Online 2017, 16, 74. [Google Scholar] [CrossRef]
- Do, J.H.; Yoo, E.Y.; Jung, M.Y.; Park, H.Y. The effects of virtual reality-based bilateral arm training on hemiplegic children’s upper limb motor skills. NeuroRehabilitation 2016, 38, 115–127. [Google Scholar] [CrossRef] [PubMed]
- Moldovan, I.; Ghircău, O.; Podar, A.; Rîză, O.; Moldovan, R. Virtual occupational therapy in a child with cerebral palsy. Palestrica Third Millenn. Civiliz. Sport 2017, 18, 38–41. [Google Scholar]
- Reifenberg, G.; Gabrosek, G.; Tanner, K.; Harpster, K.; Proffitt, R.; Persch, A. Feasibility of pediatric game-based neurorehabilitation using telehealth technologies: A case report. Am. J. Occup. Ther. 2017, 71, 7103190040p1–7103190040p8. [Google Scholar] [CrossRef]
- Sanjay, P.; Kanitkar, A.; Szturm, T.; Gaonkar, N.; Ankolekar, B. A Computer Game-Assisted Repetitive Task Practice based Upper Extremity Therapy Program for Children with Spastic Unilateral Cerebral Palsy: A Single Case Study. Indian. J. Physiother. Occup. Ther. 2020, 14, 160–166. [Google Scholar]
- Jaume-i-Capó, A.; Martínez-Bueso, P.; Moyà-Alcover, B.; Varona, J. Interactive rehabilitation system for improvement of balance therapies in people with cerebral palsy. IEEE Trans. Neural Syst. Rehabil. Eng. 2013, 22, 419–427. [Google Scholar] [CrossRef]
- Keller, J.W.; Van Hedel, H.J. Weight-supported training of the upper extremity in children with cerebral palsy: A motor learning study. J. Neuroeng. Rehabil. 2017, 14, 87. [Google Scholar] [CrossRef] [PubMed]
- Luna-Oliva, L.; Ortiz-Gutiérrez, R.M.; Cano-de la Cuerda, R.; Piédrola, R.M.; Alguacil-Diego, I.M.; Sánchez-Camarero, C.; Martínez Culebras, M.D.C. Kinect Xbox 360 as a therapeutic modality for children with cerebral palsy in a school environment: A preliminary study. NeuroRehabilitation 2013, 33, 513–521. [Google Scholar] [CrossRef] [PubMed]
- Peper, C.L.E.; Van Loon, E.C.; Van de Rijt, A.; Salverda, A.; van Kuijk, A.A. Bimanual training for children with cerebral palsy: Exploring the effects of Lissajous-based computer gaming. Dev. Neurorehabil. 2013, 16, 255–265. [Google Scholar] [CrossRef]
- Szturm, T.; Parmar, S.T.; Mehta, K.; Shetty, D.R.; Kanitkar, A.; Eskicioglu, R.; Gaonkar, N. Game-Based Dual-Task Exercise Program for Children with Cerebral Palsy: Blending Balance, Visuomotor and Cognitive Training: Feasibility Randomized Control Trial. Sensors 2022, 22, 761. [Google Scholar] [CrossRef]
- Burdea, G.C.; Cioi, D.; Kale, A.; Janes, W.E.; Ross, S.A.; Engsberg, J.R. Robotics and gaming to improve ankle strength, motor control, and function in children with cerebral palsy—A case study series. IEEE Trans. Neural Syst. Rehabil. Eng. 2012, 21, 165–173. [Google Scholar] [CrossRef]
- Sandlund, M.; Lindh Waterworth, E.; Häger, C. Using motion interactive games to promote physical activity and enhance motor performance in children with cerebral palsy. Dev. Neurorehabil. 2011, 14, 15–21. [Google Scholar] [CrossRef]
- Ketelaar, M.; Vermeer, A.; Hart, H.T.; van Petegem-van Beek, E.; Helders, P.J. Effects of a functional therapy program on motor abilities of children with cerebral palsy. Phys. Ther. 2001, 81, 1534–1545. [Google Scholar] [CrossRef]
- Wilson, B.A.; McLellan, D.L. Rehabilitation Studies Handbook; Cambridge University Press: Cambridge, UK, 1997. [Google Scholar]
- Chang, Y.J.; Chen, S.F.; Huang, J.D. The Kinect based system is physical rehabilitation: A pilot study for young adults with motor disabilities. Res. Dev. Disabil. 2011, 32, 2566–2570. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.J.; Han, W.Y.; Tsai, Y.C. A Kinect-based upper limb rehabilitation system to assist people with cerebral palsy. Res. Dev. Disabil. 2013, 34, 3654–3659. [Google Scholar] [CrossRef] [PubMed]
- Whyte, E.M.; Smyth, J.M.; Scherf, K.S. Designing serious game interventions for individuals with autism. J. Autism Dev. Disord. 2015, 45, 3820–3831. [Google Scholar] [CrossRef] [PubMed]

| Levels of Quality | Definition | Frequency (%) |
|---|---|---|
| I | Randomized controlled trials | 5 (26.3) |
| II | Non-randomized two-group studies | 0 (0.0) |
| III | Non-randomized one-group studies | 6 (31.6) |
| IV | Single experimental studies | 3 (15.8) |
| V | Case reports | 5 (26.3) |
| Total | 19 (100.0) |
| Author (Year) | Study Purpose | Literature | Design | Sample | Outcomes | Interventions | Results | Conclusions | Sum |
|---|---|---|---|---|---|---|---|---|---|
| Amengual Alcover, Jaume-i-Capó, and Moyà-Alcover [13] | 1(1) | 1(1) | 1(1) | 1(2) | 2(2) | 2(3) | 2(4) | 1(1) | 11(15) |
| Barton, Hawken, Foster, Holmes, and Butler [14] | 1(1) | 1(1) | 1(1) | 1(2) | 2(2) | 2(3) | 3(4) | 1(1) | 12(15) |
| Burdea et al. [41] | 1(1) | 1(1) | 1(1) | 1(2) | 1(2) | 2(3) | 2(4) | 1(1) | 10(15) |
| Camara Machado et al. [4] | 1(1) | 1(1) | 1(1) | 1(2) | 2(2) | 2(3) | 3(4) | 1(1) | 12(15) |
| Do, Yoo, Jung, and Park [32] | 1(1) | 1(1) | 1(1) | 1(2) | 2(2) | 2(3) | 2(4) | 1(1) | 11(15) |
| Jaume-i-Capó, Martínez-Bueso, Moyà-Alcover, and Varona [36] | 1(1) | 1(1) | 1(1) | 1(2) | 2(2) | 2(3) | 3(4) | 1(1) | 12(15) |
| Keller and Van Hedel [37] | 1(1) | 1(1) | 1(1) | 1(2) | 2(2) | 2(3) | 3(4) | 1(1) | 12(15) |
| Luna-Oliva et al. [38] | 1(1) | 1(1) | 1(1) | 1(2) | 2(2) | 2(3) | 3(4) | 1(1) | 12(15) |
| MacIntosh, Desailly, Vignais, Vigneron, and Biddiss [30] | 1(1) | 1(1) | 1(1) | 2(2) | 2(2) | 2(3) | 3(4) | 1(1) | 13(15) |
| Moldovan, Ghircău, Podar, Rîză, and Moldovan [33] | 1(1) | 1(1) | 1(1) | 1(2) | 2(2) | 2(3) | 2(4) | 1(1) | 11(15) |
| Peper, Van Loon, Van de Rijt, Salverda, and van Kuijk [39] | 1(1) | 1(1) | 1(1) | 1(2) | 2(2) | 2(3) | 3(4) | 1(1) | 12(15) |
| Reifenberg et al. [34] | 1(1) | 1(1) | 1(1) | 1(2) | 2(2) | 2(3) | 2(4) | 1(1) | 11(15) |
| Sajan, John, Grace, Sabu, and Tharion [29] | 1(1) | 1(1) | 1(1) | 2(2) | 2(2) | 3(3) | 4(4) | 1(1) | 15(15) |
| Sandlund, Lindh Waterworth, and Häger [42] | 1(1) | 1(1) | 1(1) | 1(2) | 2(2) | 1(3) | 3(4) | 1(1) | 11(15) |
| Sanjay, Kanitkar, Szturm, Gaonkar, and Ankolekar [35] | 1(1) | 1(1) | 1(1) | 1(2) | 2(2) | 2(3) | 2(4) | 1(1) | 11(15) |
| Szturm et al. [40] | 1(1) | 1(1) | 1(1) | 1(2) | 2(2) | 2(3) | 3(4) | 1(1) | 12(15) |
| Velasco et al. [31] | 1(1) | 1(1) | 1(1) | 1(2) | 2(2) | 3(3) | 3(4) | 1(1) | 13(15) |
| Wade and Porter [15] | 1(1) | 1(1) | 1(1) | 1(2) | 2(2) | 3(3) | 3(4) | 1(1) | 13(15) |
| Zoccolillo et al. [28] | 1(1) | 1(1) | 1(1) | 1(2) | 2(2) | 1(3) | 4(4) | 1(1) | 12(15) |
| Body Functions | Activities and Participation |
|---|---|
Level I
| Level III
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahn, S.N. A Scoping Review of the Serious Game-Based Rehabilitation of People with Cerebral Palsy. Int. J. Environ. Res. Public Health 2023, 20, 7006. https://doi.org/10.3390/ijerph20217006
Ahn SN. A Scoping Review of the Serious Game-Based Rehabilitation of People with Cerebral Palsy. International Journal of Environmental Research and Public Health. 2023; 20(21):7006. https://doi.org/10.3390/ijerph20217006
Chicago/Turabian StyleAhn, Si Nae. 2023. "A Scoping Review of the Serious Game-Based Rehabilitation of People with Cerebral Palsy" International Journal of Environmental Research and Public Health 20, no. 21: 7006. https://doi.org/10.3390/ijerph20217006
APA StyleAhn, S. N. (2023). A Scoping Review of the Serious Game-Based Rehabilitation of People with Cerebral Palsy. International Journal of Environmental Research and Public Health, 20(21), 7006. https://doi.org/10.3390/ijerph20217006