
Predictors of Unmet Needs in Chilean Older People with Dependency: A Cross-Sectional Study

 and
and
Abstract
:1. Introduction
2. Materials and Methods
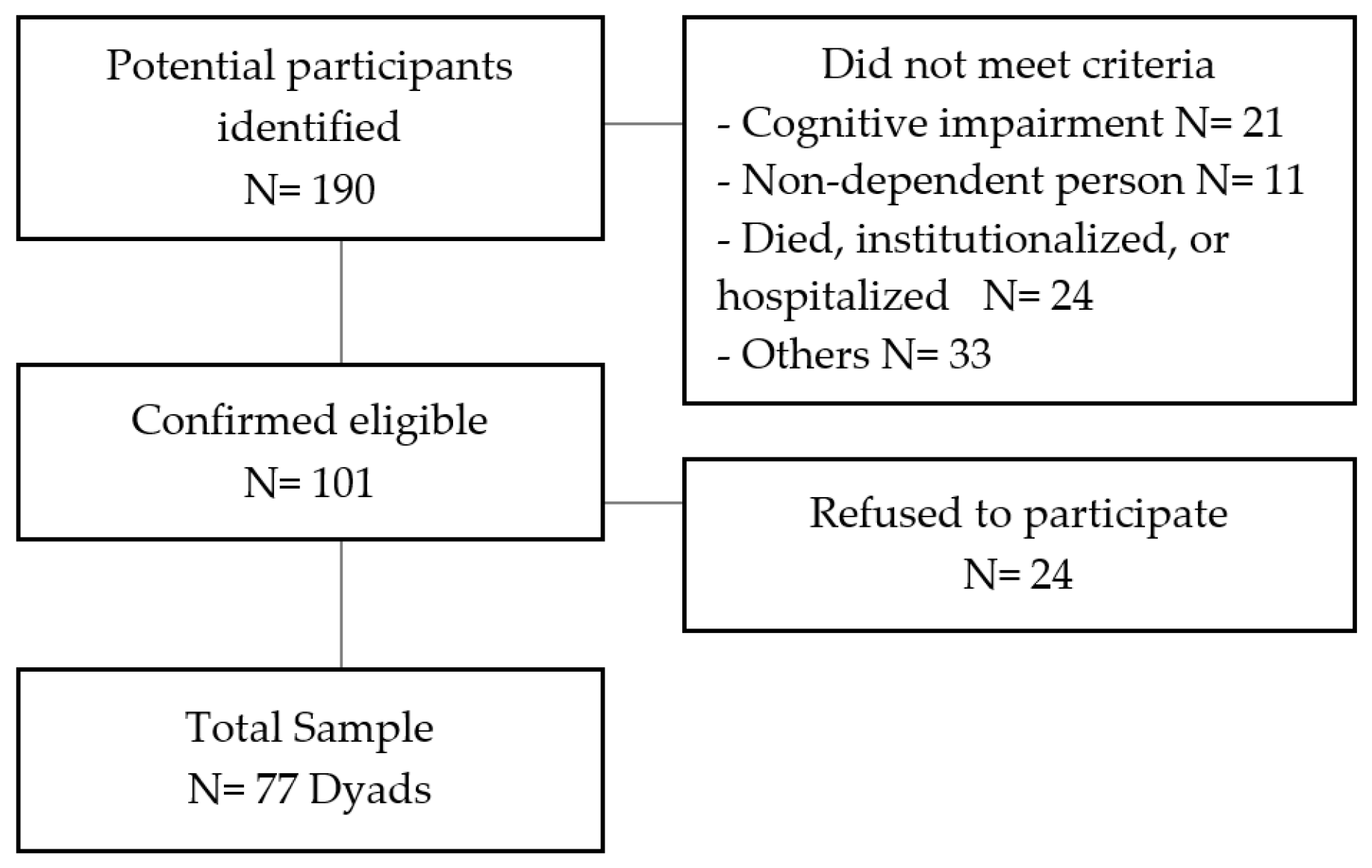
2.1. Sample
2.2. Consent Procedure and Data Collection
2.3. Instruments
2.3.1. Administered to Older People
Camberwell Assessment of Need for the Elderly (CANE)
Mini-Mental State Examination (MMSE)
Barthel Index of Activities of Daily Living
2.3.2. Administered to Older Persons and Their Caregivers
EuroQoL-5D: Visual Analog Scale (VAS)
Hospital Anxiety and Depression Scale (HADS)
Multidimensional Scale of Perceived Social Support
2.3.3. Self-Administered by Caregivers
Zarit Burden Interview
Revised Self-Efficacy for Caregiving Scale
2.4. Statistical Analyses
3. Results
3.1. Characterization of Dependent Older People
3.2. Demographic and Clinical Characteristics of Caregivers
3.3. Older People’s Met and Unmet Needs
3.4. Factors Associated with and Predictors of Unmet Needs
4. Discussion
4.1. Unmet Needs of Older Dependent People in Chile
4.2. Factors Associated with Unmet Needs
4.3. Predictors of Unmet Needs
4.4. Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Prince, M.J.; Wu, F.; Guo, Y.; Gutierrez Robledo, L.M.; O’Donnell, M.; Sullivan, R.; Yusuf, S. The Burden of Disease in Older People and Implications for Health Policy and Practice. Lancet 2015, 385, 549–562. [Google Scholar] [CrossRef] [PubMed]
- Thumala, D.; Kennedy, B.K.; Calvo, E.; Gonzalez-Billault, C.; Zitko, P.; Lillo, P.; Villagra, R.; Ibáñez, A.; Assar, R.; Andrade, M.; et al. Aging and Health Policies in Chile: New Agendas for Research. Health Syst. Reform. 2017, 3, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Ministerio de Desarrollo Social. Encuesta de Caracterización Socioeconómica Nacional: Evolución Del Proceso de Envejecimiento; Encuesta CASEN: Santiago, Chile, 2017; pp. 1–173.
- SENAMA. Estudio Nacional de La Dependencia En Las Personas Mayores; Gobierno de Chile: Santiago, Chile, 2009; pp. 1–122.
- Servicio Nacional de la Discapacidad. II Estudio Nacional de La Discapacidad; Departamento de Estudios: Santiago, Chile, 2015; ISBN 9789568441067. [Google Scholar]
- Villalobos, P. Panorama de La Dependencia En Chile: Avances y Desafíos. Rev. Med. Chile 2019, 147, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Ashaye, K.; Jayalath, D.; Hoe, J. An Introduction to Needs Assessment and Use of the Camberwell Assessment of Need for the Elderly. In Camberwell Assessment of Need for the Elderly; Hoe, J., Orrell, M., Eds.; Cambridge University Press: Cambridge, UK, 2021; pp. 1–9. [Google Scholar]
- World Health Organization. World Report on Ageing and Health; World Health Organization: Geneva, Switzerland, 2015; pp. 1–246. [Google Scholar]
- Beran, D. Needs and Needs Assessments: A Gap in the Literature for Chronic Diseases. Sage Open 2015, 5, 2158244015580375. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence. Supporting Adult Carers. In NICE Guideline; National Institute for Health and Care Excellence: London, UK, 2020. [Google Scholar]
- Hermsen, L.A.H.; Hoogendijk, E.O.; van der Wouden, J.C.; Smalbrugge, M.; Leone, S.S.; van der Horst, H.E.; Dekker, J. Self-Perceived Care Needs in Older Adults with Joint Pain and Comorbidity. Aging Clin. Exp. Res. 2017, 30, 449–455. [Google Scholar] [CrossRef]
- Hoogendijk, E.O.; Muntinga, M.E.; van Leeuwen, K.M.; van der Horst, H.E.; Deeg, D.J.H.; Frijters, D.H.M.; Hermsen, L.A.H.; Jansen, A.P.D.; Nijpels, G.; van Hout, H.P.J. Self-Perceived Met and Unmet Care Needs of Frail Older Adults in Primary Care. Arch. Gerontol. Geriatr. 2014, 58, 37–42. [Google Scholar] [CrossRef]
- Dostálová, V.; Bártová, A.; Bláhová, H.; Holmerová, I. The Needs of Older People Receiving Home Care: A Scoping Review. Aging Clin. Exp. Res. 2021, 33, 495–504. [Google Scholar] [CrossRef]
- Hoe, J.; Orrell, M. (Eds.) Camberwell Assessment of Need for the Elderly, 2nd ed.; Cambridge University Press: Cambridge, UK, 2021; ISBN 9781911623373. [Google Scholar]
- Reynolds, T.; Thornicrof, G.; Abas, M.; Woods, B.; Hoe, J.; Leese, M.; Orrell, M. Camberwell Assessment of Need for the Elderly Development, Validity and Reliability. Br. J. Psychiatry 2000, 176, 444–452. [Google Scholar] [CrossRef]
- Carvacho, R.; Carrasco, M.; Lorca, M.B.F.; Miranda-Castillo, C. Met and Unmet Needs of Dependent Older People According to the Camberwell Assessment of Need for the Elderly (CANE): A Scoping Review. Rev. Esp. Geriatr. Gerontol. 2021, 56, 225–235. [Google Scholar] [CrossRef]
- Mazurek, J.; Szcześniak, D.; Rymaszewska, J. Needs of Older People in Long-Term Care Settings. In Camberwell Assessment of Need for the Elderly: CANE; Hoe, J., Orrell, M., Eds.; Cambridge University Press: Cambridge, UK, 2021; pp. 86–90. ISBN 9781911623366. [Google Scholar]
- Tapia, T.; Slachevsky, A.; León-Campos, M.O.; Madrid, M.; Caqueo-Urízar, A.; Rohde, G.C.; Miranda-Castillo, C. Predictors of Unmet Needs in Chilean Older People with Dementia: A Cross-Sectional Study. BMC Geriatr. 2019, 19, 106. [Google Scholar] [CrossRef]
- Houtjes, W.; Van Meijel, B.; Deeg, D.J.H.; Beekman, A.T.F. Major Depressive Disorder in Late Life: A Multifocus Perspective on Care Needs. Aging Ment. Health 2010, 14, 874–880. [Google Scholar] [CrossRef]
- Stein, J.; Pabst, A.; Weyerer, S.; Werle, J.; Maier, W.; Heilmann, K.; Scherer, M.; Stark, A.; Kaduszkiewicz, H.; Wiese, B.; et al. The Assessment of Met and Unmet Care Needs in the Oldest Old with and without Depression Using the Camberwell Assessment of Need for the Elderly (CANE): Results of the AgeMooDe Study. J. Affect. Disord. 2016, 193, 309–317. [Google Scholar] [CrossRef]
- Stein, J.; Liegert, P.; Dorow, M.; König, H.H.; Riedel-Heller, S.G. Unmet Health Care Needs in Old Age and Their Association with Depression—Results of a Population-Representative Survey. J. Affect. Disord. 2019, 245, 998–1006. [Google Scholar] [CrossRef] [PubMed]
- Stein, J.; Luppa, M.; König, H.H.; Riedel-Heller, S.G. Assessing Met and Unmet Needs in the Oldest-Old and Psychometric Properties of the German Version of the Camberwell Assessment of Need for the Elderly (CANE)—A Pilot Study. Int. Psychogeriatr. 2014, 26, 285–295. [Google Scholar] [CrossRef] [PubMed]
- Dautzenberg, G.; Lans, L.; Meesters, P.D.; Kupka, R.; Beekman, A.; Stek, M.L.; Dols, A. The Care Needs of Older Patients with Bipolar Disorder. Aging Ment. Health 2016, 20, 899–907. [Google Scholar] [CrossRef] [PubMed]
- Field, E.; Walker, M.; Orrell, M.; Hancock, G. CANE–Camberwell Assessment of Need for the Elderly; Gaskell: London, UK, 2004. [Google Scholar]
- Quiroga, P.; Albala, C.; Klaasen, G. Validación de Un Test de Tamizaje Para El Diagnóstico de Demencia Asociada a Edad, En Chile. Rev. Med. Chile 2004, 132, 467–478. [Google Scholar] [CrossRef] [PubMed]
- Cid Ruzafa, J.; Damian-Moreno, J. Valoracion de La Discapacidad Fisica: El Indice de Barthel. Rev. Esp. Salud Publica 1997, 71, 411–418. [Google Scholar] [CrossRef]
- Solís, C.; Arrioja, S.; Manzano, A. Índice de Barthel (IB): Un Instrumento Esencial Para La Evaluación Funcional y La Rehabilitación. Plast. Restauración Neurol. 2005, 4, 81–85. [Google Scholar]
- Hurst, N.P.; Kind, P.; Ruta, D.; Hunter, M.; Stubbings, A. Health-Related Quality of Life in Rheumatoid Arthritis: Validity, Responsiveness and Reliability of EuroQol (EQ-5D). Br. J. Rheumatol. 1997, 36, 551–559. [Google Scholar] [CrossRef] [PubMed]
- Olivares-Tirado, P. Calidad de Vida Relacionada a La Salud En Población General; Superintendencia de Salud: Santiago, Chile, 2005. [Google Scholar]
- Zarate, V.; Kind, P.; Valenzuela, P.; Vignau, A.; Olivares-Tirado, P.; Munoz, A. Social Valuation of EQ-5D Health States: The Chilean Case. Value Health 2011, 14, 1135–1141. [Google Scholar] [CrossRef]
- Snaith, R.P. The Hospital Anxiety and Depression Scale. Health Qual. Life Outcomes 2003, 1, 29. [Google Scholar] [CrossRef] [PubMed]
- Quintana, J.; Padierna, A.; Esteban, C.; Arostegui, I.; Bilbao, A.; Ruiz, I. Evaluation of the Psychometric Characteristics of the Spanish Version of the Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 2003, 107, 216–221. [Google Scholar] [CrossRef] [PubMed]
- Villoria, E.; Lara, L. Assessment of the Hospital Anxiety and Depression Scale for Cancer Patients. Rev. Med. Chile 2018, 146, 300–307. [Google Scholar] [CrossRef]
- Arechabala, M.; Miranda, C. Validación de Una Escala de Apoyo Social Percibido. Cienc. Enfermería 2002, 8, 49–55. [Google Scholar] [CrossRef]
- Breinbauer, H.; Vásquez, H.; Mayanz, S.; Guerraa, C.; Millán, T. Original and Abbreviated Zarit Caregiver Burden Scales. Validation in Chile. Rev. Med. Chile 2009, 137, 657–665. [Google Scholar] [CrossRef]
- Márquez-González, M.; Losada, A.; López, J.; Peñacoba, C. Reliability and Validity of the Spanish Version of the Revised Scale for Caregiving Self-Efficacy. Clin. Gerontol. 2009, 32, 347–357. [Google Scholar] [CrossRef]
- Steffen, A.M.; McKibbin, C.; Zeiss, A.M.; Gallagher-Thompson, D.; Bandura, A. The Revised Scale for Caregiving Self-Efficacy: Reliability and Validity Studies. J. Gerontol. B Psychol. Sci. Soc. Sci. 2002, 57, P74–P86. [Google Scholar] [CrossRef]
- Merluzzi, T.V.; Philip, E.J.; Vachon, D.O.; Heitzmann, C.A. Assessment of Self-Efficacy for Caregiving: The Critical Role of Self-Care in Caregiver Stress and Burden. Palliat. Support Care 2011, 9, 15–24. [Google Scholar] [CrossRef]
- Mazanec, S.R.; Flocke, S.A.; Daly, B.J. Health Behaviors in Family Members of Patients Completing Cancer Treatment. Oncol. Nurs. Forum 2015, 42, 54–62. [Google Scholar] [CrossRef] [PubMed]
- Rush, C.L.; Darling, M.; Elliott, M.G.; Febus-Sampayo, I.; Kuo, C.; Muñoz, J.; Duron, Y.; Torres, M.; Galván, C.C.; Gonzalez, F.; et al. Engaging Latina Cancer Survivors, Their Caregivers, and Community Partners in a Randomized Controlled Trial: Nueva Vida Intervention. Qual. Life Res. 2015, 24, 1107–1118. [Google Scholar] [CrossRef]
- Shiovitz-Ezra, S.; Shemesh, J.; McDonnell-Naughton, M. Pathways from Ageism to Loneliness. In Contemporary Perspectives on Ageism; Ayalon, L., Tesch-Römer, C., Eds.; Springer International Publishing: Cham, Switzerland, 2018; pp. 131–147. ISBN 978-3-319-73820-8. [Google Scholar]
- Burnes, D.; Sheppard, C.; Henderson, C.R., Jr.; Wassel, M.; Cope, R.; Barber, C.; Pillemer, K. Interventions to Reduce Ageism Against Older Adults: A Systematic Review and Meta-Analysis. Am. J. Public Health 2019, 109, 1–9. [Google Scholar] [CrossRef]
- Shen, T.; Li, D.; Hu, Z.; Li, J.; Wei, X. The Impact of Social Support on the Quality of Life among Older Adults in China: An Empirical Study Based on the 2020 CFPS. Front. Public Health 2022, 10, 914707. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.K.; Oh, J. Health-Related Quality of Life in Older Adults: Its Association with Health Literacy, Self-Efficacy, Social Support, and Health-Promoting Behavior. Healthcare 2020, 8, 407. [Google Scholar] [CrossRef] [PubMed]
- De Maria, M.; Tagliabue, S.; Ausili, D.; Vellone, E.; Matarese, M. Perceived Social Support and Health-Related Quality of Life in Older Adults Who Have Multiple Chronic Conditions and Their Caregivers: A Dyadic Analysis. Soc. Sci. Med. 2020, 262, 113193. [Google Scholar] [CrossRef] [PubMed]
- Matud, M.P.; García, M.C.; Fortes, D. Relevance of Gender and Social Support in Self-Rated Health and Life Satisfaction in Elderly Spanish People. Int. J. Environ. Res. Public Health 2019, 16, 2725. [Google Scholar] [CrossRef]
- Şahin, D.S.; Özer, Ö.; Yanardağ, M.Z. Perceived Social Support, Quality of Life and Satisfaction with Life in Elderly People. Educ. Gerontol. 2019, 45, 69–77. [Google Scholar] [CrossRef]
- Troncoso, M. Cuidado Informal a Mayores Dependientes En Chile: Quienes Cuidan y Con Que Politicas Sociales Cuentan. Am. Lat. Hoy 2015, 71, 83–101. [Google Scholar] [CrossRef]
- Orientación Técnica Programa Más Adultos Mayores Autovalentes. Available online: http://www.bibliotecaminsal.cl/wp/wp-content/uploads/2018/01/013.Orientaci%C3%B3n-T%C3%A9cnica-Programa-Ms-Autovalentes.pdf (accessed on 29 August 2023).
- Ní Mhaoláin, A.M.; Fan, C.W.; Romero-Ortuno, R.; Cogan, L.; Cunningham, C.; Kenny, R.-A.; Lawlor, B. Frailty, Depression, and Anxiety in Later Life. Int. Psychogeriatr. 2012, 24, 1265–1274. [Google Scholar] [CrossRef] [PubMed]
- Vaughan, L.; Goveas, J.; Corbin, A. Depression and Frailty in Later Life: A Systematic Review. Clin. Interv. Aging 2015, 10, 1947. [Google Scholar] [CrossRef]
- Villarroel, S.; Medina, S. Telemedicina En Chile: Uso, Desarrollo y Controversias En Una Red de Salud Pública Del Sur Del País. Rev. Chil. Salud Pública 2022, 26, 48–57. [Google Scholar] [CrossRef]
- Zhu, W.; Jiang, Y. A Meta-Analytic Study of Predictors for Informal Caregiver Burden in Patients with Stroke. J. Stroke Cerebrovasc. Dis. 2018, 27, 3636–3646. [Google Scholar] [CrossRef] [PubMed]
- Balladares, J.; Carvacho, R.; Basualto, P.; Coli Acevedo, J.; Molina Garzón, M.; Catalán, L.; Gray-Gariazzo, N.; Aracena Alvarez, M. Cuidar a Los Que Cuidan: Experiencias de Cuidadores Informales de Personas Mayores Dependientes En Contexto COVID-19 Taking Care for Those Who Take Care: Experiences of Informal Caregivers of Dependent Elderly People in a COVID-19. 2021. Available online: https://www.psicoperspectivas.cl/index.php/psicoperspectivas/article/viewFile/2397/1508 (accessed on 6 September 2022).
- Rudnicka, E.; Napierała, P.; Podfigurna, A.; Męczekalski, B.; Smolarczyk, R.; Grymowicz, M. The World Health Organization (WHO) Approach to Healthy Ageing. Maturitas 2020, 139, 6–11. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Sociodemographic Characteristics | Levels | Freq (%)/Mean (SD) |
|---|---|---|
| Age (years) | Mean (SD) | 79.9 (9.9) |
| 60–73 | 22 (28.6) | |
| 74–83 | 26 (33.8) | |
| 84–101 | 29 (37.7) | |
| Gender | Female | 52 (67.5) |
| Male | 25 (32.5) | |
| Marital status | Single | 6 (7.8) |
| Married/living with a partner | 30 (39) | |
| Separated/divorced | 6 (7.8) | |
| Widowed | 35 (45.5) | |
| Educational level | Primary education or less | 21 (27.3) |
| Incomplete secondary education | 28 (36.4) | |
| Completed secondary education | 18 (23.4) | |
| Professional or technician | 10 (13) | |
| Living with the caregiver | Yes | 64 (83.1) |
| No | 13 (16.9) | |
| Clinical characteristics | ||
| Diagnosis | High blood pressure | 61 (79.2) |
| Diabetes | 30 (39) | |
| Rheumatological diseases | 29 (37.7) | |
| Chronic respiratory diseases | 15 (19.5) | |
| Chronic renal insufficiency | 10 (13) | |
| Cancer | 9 (11.7) | |
| Sensory impairments | 13 (16.9) | |
| Level of dependency | Mean (SD) | 70.4 (21.3) |
| Mild | 57 (74) | |
| Moderate | 14 (18.2) | |
| Severe | 6 (7.8) | |
| Depressive symptomatology | Mean (SD) | 6.3 (4) |
| No symptoms | 43 (55.8) | |
| Presents symptoms | 22 (28.6) | |
| Possible disorder | 12 (15.6) | |
| Anxious symptomatology | Mean (SD) | 6.6 (4.8) |
| No symptoms | 47 (61) | |
| Presents symptoms | 15 (19.5) | |
| Possible disorder | 15 (19.5) |
| Sociodemographic Characteristics | Levels | N (%)/Mean (SD) |
|---|---|---|
| Age (years) | Mean (SD) | 55.7 (14.34) |
| 18–40 | 11 (14.3) | |
| 41–60 | 37 (48) | |
| 61–83 | 29 (37.7) | |
| Gender | Female | 65 (84.4) |
| Male | 12 (15.6) | |
| Educational level | Incomplete high school education | 20 (26) |
| Completed high school education | 23 (29) | |
| Professional or technician | 34 (44.2) | |
| Relationship with the older person | Partner/spouse | 15 (19.5) |
| Son/daughter | 52 (67.5) | |
| Sibling | 3 (3.9) | |
| Grandchild | 6 (7.8) | |
| Mother | 1 (1.3) | |
| Clinical characteristics | ||
| Diagnosis | Hypertension | 33 (42.9) |
| Diabetes | 10 (13) | |
| Depression | 10 (13) | |
| No diseases | 18 (23.4) | |
| Caregiver burden | Mean (SD) | 51.3 (16.7) |
| Absence of burden | 32 (41.6) | |
| Moderate burden | 16 (20.8) | |
| Intense burden | 29 (37.7) | |
| Depressive symptomatology | Mean (SD) | 6.5 (4.4) |
| No symptoms | 47 (61) | |
| Presents symptoms | 11 (14.3) | |
| Possible disorder | 19 (24.7) | |
| Anxious symptomatology | Mean (SD) | 8 (4.9) |
| No symptoms | 33 (42.9) | |
| Presents symptoms | 19 (24.7) | |
| Possible disorder | 25 (32.5) |
| Needs (N = 77) | Met (%) | Unmet (%) | Total 1 (%) |
|---|---|---|---|
| Accommodation | 42.9 | 1.3 | 44.2 |
| Looking after home | 77.9 | 1.3 | 79.2 |
| Food | 79.2 | 1.3 | 80.5 |
| Self-care | 68.8 | 0.0 | 68.8 |
| Caring for another | 7.8 | 0.0 | 7.8 |
| Daytime activities | 18.2 | 33.8 | 51.9 |
| Memory | 7.8 | 2.6 | 10.4 |
| Eyesight/hearing | 70.1 | 19.5 | 89.6 |
| Mobility | 46.8 | 7.8 | 54.5 |
| Continence | 39.0 | 5.2 | 44.2 |
| Physical health | 93.5 | 5.2 | 98.7 |
| Drugs | 45.5 | 6.5 | 51.9 |
| Psychotic symptoms | 5.2 | 2.6 | 7.8 |
| Psychological distress | 26.0 | 24.7 | 50.6 |
| Information | 27.3 | 14.3 | 41.6 |
| Deliberate self-harm | 3.9 | 2.6 | 6.5 |
| Accidental self-Harm | 6.5 | 0.0 | 6.5 |
| Abuse/neglect | 1.3 | 1.3 | 2.6 |
| Behavior | 0.0 | 0.0 | 0.0 |
| Alcohol | 0.0 | 0.0 | 0.0 |
| Company | 11.7 | 23.4 | 35.1 |
| Intimate relationships | 10.4 | 14.3 | 24.7 |
| Money | 29.9 | 3.9 | 33.8 |
| Social benefits | 26.0 | 23.4 | 49.4 |
| Correlation | p | |
|---|---|---|
| Older Person Factors | ||
| Functionality | Rs = −0.53 | 0.00 ** |
| Number of medications | Rs = 0.22 | 0.06 |
| Health-related quality of life | Rs = −0.16 | 0.18 |
| Social support | Rs = −0.25 | 0.02 * |
| Depressive symptomatology | Rs = 0.47 | 0.00 ** |
| Anxious symptomatology | Rs = 0.35 | 0.00 ** |
| Caregiver Factors | ||
| Burden | Rs = 0.14 | 0.21 |
| Social support | Rs = −0.04 | 0.71 |
| Depressive symptomatology | Rs = 0.18 | 0.11 |
| Anxious symptomatology | Rs = 0.14 | 0.23 |
| Self-efficacy | Rs = −0.15 | 0.18 |
| Variable | Beta 1 | p Value |
|---|---|---|
| Functionality (Barthel) | −0.38 | 0.00 ** |
| Anxious symptoms (HADS-A) | 0.33 | 0.00 ** |
| R2 | 0.33 | |
| Adjusted R2 | 0.31 | |
| F | 18.24 | 0.00 ** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carvacho, R.; Carrasco, M.; Fernández, M.B.; Miranda-Castillo, C. Predictors of Unmet Needs in Chilean Older People with Dependency: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2023, 20, 6928. https://doi.org/10.3390/ijerph20206928
Carvacho R, Carrasco M, Fernández MB, Miranda-Castillo C. Predictors of Unmet Needs in Chilean Older People with Dependency: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2023; 20(20):6928. https://doi.org/10.3390/ijerph20206928
Chicago/Turabian StyleCarvacho, Raffaela, Marcela Carrasco, María Beatriz Fernández, and Claudia Miranda-Castillo. 2023. "Predictors of Unmet Needs in Chilean Older People with Dependency: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 20, no. 20: 6928. https://doi.org/10.3390/ijerph20206928
APA StyleCarvacho, R., Carrasco, M., Fernández, M. B., & Miranda-Castillo, C. (2023). Predictors of Unmet Needs in Chilean Older People with Dependency: A Cross-Sectional Study. International Journal of Environmental Research and Public Health, 20(20), 6928. https://doi.org/10.3390/ijerph20206928