
Heart Rate Variability in Individuals with Down Syndrome: A Scoping Review with Methodological Considerations




 and
and 
Abstract
1. Introduction
2. Materials and Methods
- (1)
- First author and year of publication;
- (2)
- Participant characteristics (experimental group—individuals with DS; control group);
- (3)
- Conditions for RR interval acquisition;
- (4)
- HRV analysis methods;
- (5)
- Results of HRV analysis.
- (i)
- Study sample (experimental and control group sizes);
- (ii)
- The acquisition and processing of data, in which we analyzed the following:
- -
- Device, software, sampling frequency and duration of recordings;
- -
- Environmental conditions during recordings: time of day, room conditions (lighting/sounds/temperature), behaviors prior to recordings (sleep, physical activity, meals, beverages and toilet before) and heart rate stabilization;
- -
- Respiratory rate during recordings and breathing control;
- -
- Position during recordings.
- (iii)
- HRV analysis, focusing on the following points:
- -
- Software, artifact/ectopic beats correction, time series length (time/beats) and data normality;
- -
- Parameters, bands for frequency-domain analysis and analysis method.
- (iv)
- HRV correction for HR.
3. Results
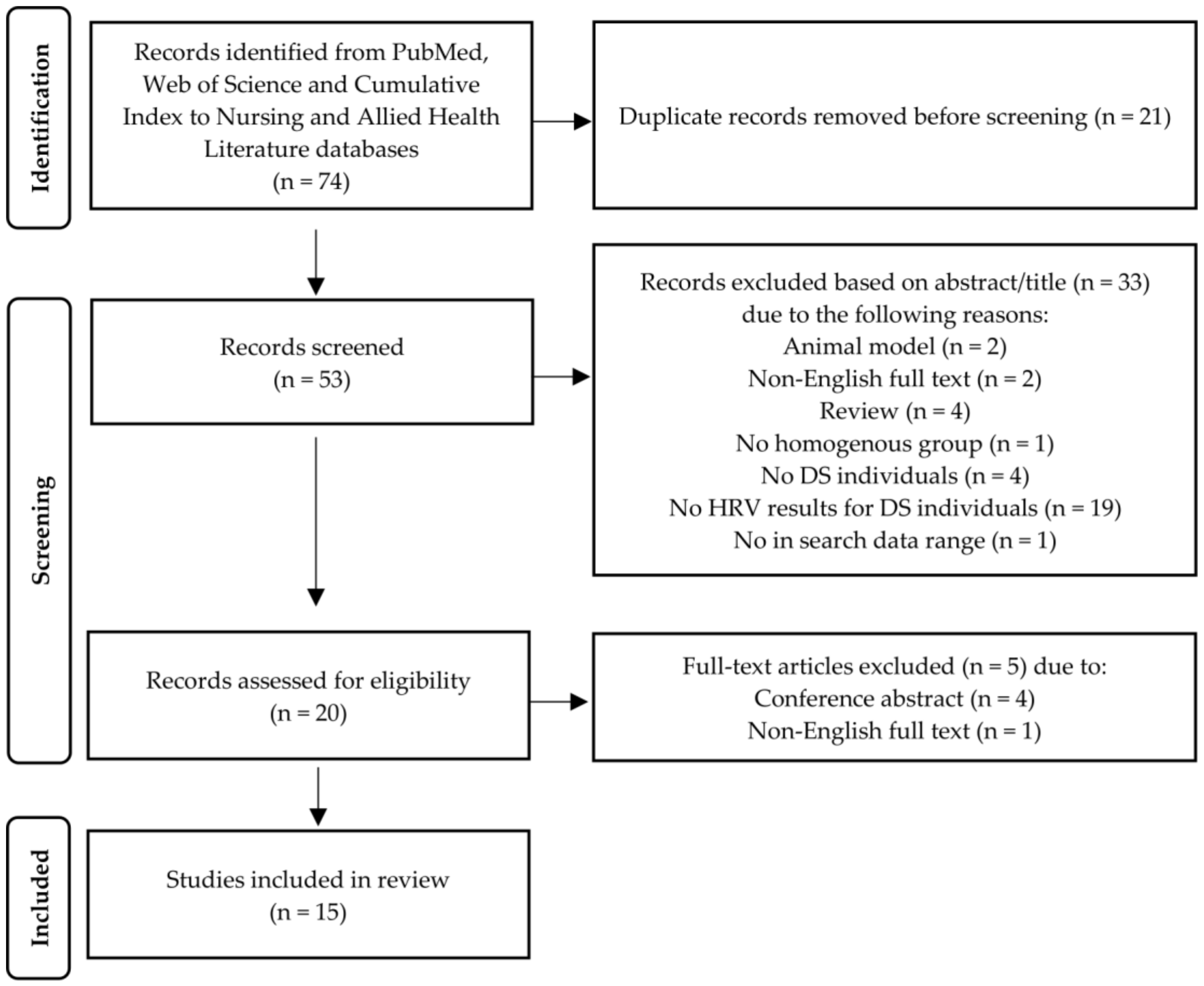
3.1. Selection of the Studies
3.2. Information Provided by the Selected Studies
3.2.1. Participants/Demographic Data
3.2.2. RR Interval Recordings
3.2.3. HRV Measurement
3.2.4. HRV Results
4. Discussion
4.1. Study Sample
4.2. Data Acquisition and Processing (Device, Duration of Recordings and Sampling Frequency)
4.3. Environmental Conditions during Recordings: Time of Day, Room Conditions (Lightings/Sounds/Temperature), Behaviors Prior to Recordings (Sleep, Physical Activity, Meals, Beverages and Toilet before) and Heart Rate Stabilization
4.4. Respiratory Rate during Recordings and Breathing Control
4.5. HRV Analysis
4.5.1. Software, Artifact Correction, Time Series Length (Time/Beats), Information about Data Normality
4.5.2. Frequency-Domain and Nonlinear Parameters
4.5.3. Correction for HR
4.6. Summary—Implications and Applications for Future Studies
4.7. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Antonarakis, S.E.; Skotko, B.G.; Rafii, M.S.; Strydom, A.; Pape, S.E.; Bianchi, D.W.; Sherman, S.L.; Reeves, R.H. Down syndrome. Nat. Rev. Dis. Prim. 2020, 6, 9. [Google Scholar] [CrossRef]
- Seale, A.; Shinebourne, E.A. Cardiac problems in Down syndrome. Curr. Pediatr. 2004, 14, 33–38. [Google Scholar] [CrossRef]
- Blom, N.A.; Ottenkamp, J.; Wenink, A.C.G.; Gittenberger-de Groot, A.C. Defficiency of vestibukar spine in atrioventricular septal defect in human fetuses with Down syndrome. Am. J. Cardiol. 2003, 91, 180–184. [Google Scholar] [CrossRef] [PubMed]
- Briggs, L.E.; Kakarla, J.; Wessels, A. The pathogenesis of atrial and atrioventricular septal defects with special emphasis on the role of the dorsal mesenchymal protrusion. Differentiation 2012, 84, 117–130. [Google Scholar] [CrossRef]
- Kertesz, N.J. The conduction system and arrhythmias in common atrioventricular canal. Prog. Pediatr. Cardiol. 1999, 10, 153–159. [Google Scholar] [CrossRef]
- Calkoen, E.; Adriaanse, B.; Haak, M.; Bartelings, M.; Kolesnik, A.; Niszczota, C.; van Vugt, J.; Roest, A.; Blom, N.; Gittenberger-de Groot, A.; et al. How Normal is a “Normal” Heart in Fetuses and Infants with Down Syndrome? Fetal. Diagn. Ther. 2016, 39, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Banks, M.A.; Jenson, J.; Kugler, J.D. Late Development of Atrioventricular Block After Congenital Heart Surgery in Down Syndrome. Am. J. Cardiol. 2001, 88, 86–89. [Google Scholar] [CrossRef]
- Guerra, M.; Llorens, N.; Fernhall, B. Chronotropic incompetence in persons with down syndrome. Arch. Phys. Med. Rehabil. 2003, 84, 1604–1608. [Google Scholar] [CrossRef]
- Fernhall, B.; Otterstetter, M. Attenuated responses to sympathoexcitation in individuals with Down syndrome. J. Appl. Physiol. 2003, 94, 2158–2165. [Google Scholar] [CrossRef] [PubMed]
- Heffernan, K.S.; Baynard, T.; Goulopoulou, S.; Giannopoulou, I.; Collier, S.R.; Figueroa, A.; Fernhall, B. Baroreflex sensitivity during static exercise in individuals with Down Syndrome. Med. Sci. Sports Exerc. 2005, 37, 2026–2031. [Google Scholar] [CrossRef]
- Fernhall, B.; Figueroa, A.; Collier, S.; Baynard, T.; Giannopoulou, I.; Goulopoulou, S. Blunted heart rate response to upright tilt in people with Down syndrome. Arch. Phys. Med. Rehabil. 2005, 86, 813–818. [Google Scholar] [CrossRef]
- Fernhall, B.; Mendonca, G.V.; Baynard, T. Reduced work capacity in individuals with Down syndrome: A consequence of autonomic dysfunction? Exerc. Sport Sci. Rev. 2013, 41, 138–147. [Google Scholar] [CrossRef] [PubMed]
- Fujii, Y.; Aida, N.; Niwa, T.; Enokizono, M.; Nozawa, K.; Inoue, T. A small pons as a characteristic finding in Down syndrome: A quantitative MRI study. Brain Dev. 2017, 39, 298–305. [Google Scholar] [CrossRef]
- Novak, V.; Novak, P.; deMarchie, M.; Schondorf, R. The effect of severe brainstem injury on heart rate and blood pressure oscillations. Clin. Auton. Res. 1995, 5, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Pierce, M.; Ramsey, K.; Pinter, J. Trends in Obesity and Overweight in Oregon Children With Down Syndrome. Glob. Pediatr. Health 2019, 6, 2333794X19835640. [Google Scholar] [CrossRef] [PubMed]
- Bertapelli, F.; Pitetti, K.; Agiovlasitis, S.; Guerra-Junior, G. Overweight and obesity in children and adolescents with Down syndrome-prevalence, determinants, consequences, and interventions: A literature review. Res. Dev. Disabil. 2016, 57, 181–192. [Google Scholar] [CrossRef]
- Esposito, P.E.; MacDonald, M.; Hornyak, J.E.; Ulrich, D.A. Physical activity patterns of youth with Down syndrome. Intellect Dev. Disabil. 2012, 50, 109–119. [Google Scholar] [CrossRef] [PubMed]
- Agiovlasitis, S.; Choi, P.; Allred, A.T.; Xu, J.; Motl, R.W. Systematic review of sedentary behaviour in people with Down syndrome across the lifespan: A clarion call. J. Appl. Res. Intellect Disabil. 2020, 33, 146–159. [Google Scholar] [CrossRef]
- Versacci, P.; Di Carlo, D.; Digilio, M.C.; Marino, B. Cardiovascular disease in Down syndrome. Curr. Opin. Pediatr. 2018, 30, 616–622. [Google Scholar] [CrossRef]
- Sobey, C.G.; Judkins, C.P.; Sundararajan, V.; Phan, T.G.; Drummond, G.R.; Srikanth, V.K. Risk of Major Cardiovascular Events in People with Down Syndrome. PLoS ONE 2015, 10, e0137093. [Google Scholar] [CrossRef]
- Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Heart rate variability: Standards of measurement, physiological interpretation and clinical use. Circulation 1996, 93, 1043–1065. [Google Scholar] [CrossRef]
- Shaffer, F.; McCraty, R.; Zerr, C.L. A healthy heart is not a metronome: An integrative review of the heart’s anatomy and heart rate variability. Front. Psychol. 2014, 5, 1040. [Google Scholar] [CrossRef]
- Kemper, K.J.; Hamilton, C.; Atkinson, M. Heart rate variability: Impact of differences in outlier identification and management strategies on common measures in three clinical populations. Pediatr. Res. 2007, 62, 337–342. [Google Scholar] [CrossRef] [PubMed]
- Thayer, J.F.; Yamamoto, S.S.; Brosschot, J.F. The relationship of autonomic imbalance, heart rate variability and cardiovascular disease risk factors. Int. J. Cardiol. 2010, 141, 122–131. [Google Scholar] [CrossRef] [PubMed]
- Xhyheri, B.; Manfrini, O.; Mazzolini, M.; Pizzi, C.; Bugiardini, R. Heart rate variability today. Prog. Cardiovasc. Dis. 2012, 55, 321–331. [Google Scholar] [CrossRef]
- Billman, G.E. Heart rate variability—A historical perspective. Front. Physiol. 2011, 2, 86. [Google Scholar] [CrossRef]
- Billman, G.E.; Sacha, J.; Werner, B.; Jelen, P.J.; Gąsior, J.S. Editorial: Heart Rate Variability and Other Autonomic Markers in Children and Adolescents. Front. Physiol. 2019, 10, 1265. [Google Scholar] [CrossRef] [PubMed]
- Gang, Y.; Malik, M. Heart rate variability analysis in general medicine. Indian Pacing ElectroPhysiol. J. 2003, 3, 34–40. [Google Scholar] [PubMed]
- Peltola, M.A. Role of editing of R-R intervals in the analysis of heart rate variability. Front. Physiol. 2012, 3, 148. [Google Scholar] [CrossRef]
- Sacha, J. Why should one normalize heart rate variability with respect to average heart rate. Front. Physiol. 2013, 4, 306. [Google Scholar] [CrossRef]
- Billman, G.E. The effect of heart rate on the heart rate variability response to autonomic interventions. Front. Physiol. 2013, 4, 222. [Google Scholar] [CrossRef] [PubMed]
- Heathers, J.A. Everything Hertz: Methodological issues in short-term frequency-domain HRV. Front. Physiol. 2014, 5, 177. [Google Scholar] [CrossRef]
- Quintana, D.S.; Heathers, J.A. Considerations in the assessment of heart rate variability in biobehavioral research. Front. Psychol 2014, 5, 805. [Google Scholar] [CrossRef]
- Quintana, D.S.; Alvares, G.A.; Heathers, J.A. Guidelines for Reporting Articles on Psychiatry and Heart rate variability (GRAPH): Recommendations to advance research communication. Transl. Psychiatry 2016, 6, e803. [Google Scholar] [CrossRef]
- Billman, G.E.; Huikuri, H.V.; Sacha, J.; Trimmel, K. An introduction to heart rate variability: Methodological considerations and clinical applications. Front. Physiol. 2015, 6, 55. [Google Scholar] [CrossRef]
- Shaffer, F.; Ginsberg, J.P. An overview of heart rate variability metrics and norms. Front. Public Health 2017, 5, 258. [Google Scholar] [CrossRef] [PubMed]
- Ernst, G. Heart-rate variability-more than heart beats? Front. Public Health 2017, 5, 240. [Google Scholar] [CrossRef] [PubMed]
- Laborde, S.; Mosley, E.; Thayer, J.F. Heart rate variability and cardiac vagal tone in psychophysiological research—Recommendations for experiment planning, data analysis, and data reporting. Front. Psychol. 2017, 8, 213. [Google Scholar] [CrossRef]
- Singh, N.; Moneghetti, K.J.; Christle, J.W.; Hadley, D.; Plews, D.; Froelicher, V. Heart Rate Variability: An Old Metric with New Meaning in the Era of using mHealth Technologies for Health and Exercise Training Guidance. Part One: Physiology and Methods. Arrhythm. ElectroPhysiol. Rev. 2018, 7, 193–198. [Google Scholar] [CrossRef]
- Hayano, J.; Yuda, E. Pitfalls of assessment of autonomic function by heart rate variability. J. Physiol. Anthropol. 2019, 38, 3. [Google Scholar] [CrossRef]
- De Geus, E.J.C.; Gianaros, P.J.; Brindle, R.C.; Jennings, J.R.; Berntson, G.G. Should heart rate variability be “corrected” for heart rate? Biological, quantitative, and interpretive considerations. Psychophysiology 2019, 56, e13287. [Google Scholar] [CrossRef]
- Li, K.; Rüdiger, H.; Ziemssen, T. Spectral Analysis of Heart Rate Variability: Time Window Matters. Front. Neurol. 2019, 10, 545. [Google Scholar] [CrossRef] [PubMed]
- Malik, M.; Hnatkova, K.; Huikuri, H.V.; Lombardi, F.; Schmidt, G.; Zabel, M. CrossTalk proposal: Heart rate variability is a valid measure of cardiac autonomic responsiveness. J. Physiol. 2019, 597, 2595–2598. [Google Scholar] [CrossRef]
- Shaffer, F.; Meehan, Z.M.; Zerr, C.L. A Critical Review of Ultra-Short-Term Heart Rate Variability Norms Research. Front. Neurosci. 2020, 14, 594880. [Google Scholar] [CrossRef] [PubMed]
- Gąsior, J.S.; Zamunér, A.R.; Silva, L.E.V.; Williams, C.A.; Baranowski, R.; Sacha, J.; Machura, P.; Kochman, W.; Werner, B. Heart Rate Variability in Children and Adolescents with Cerebral Palsy-A Systematic Literature Review. J. Clin. Med. 2020, 9, 1141. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, T.D.; Massetti, T.; Silva, T.D.D.; Crocetta, T.B.; Guarnieri, R.; Vanderlei, L.C.M.; Monteiro, C.B.M.; Garner, D.M.; Ferreira, C. Heart rate variability in individuals with Down syndrome—A systematic review and meta-analysis. Auton. Neurosci. 2018, 213, 23–33. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Ferri, R.; Curzi-Dascalova, L.; Del Gracco, S.; Elia, M.; Musumeci, S.A.; Pettinato, S. Heart rate variability and apnea during sleep in Down’s syndrome. J. Sleep Res. 1998, 7, 282–287. [Google Scholar] [CrossRef] [PubMed]
- Baynard, T.; Pitetti, K.H.; Guerra, M.; Fernhall, B. Heart rate variability at rest and during exercise in persons with Down syndrome. Arch. Phys. Med. Rehabil. 2004, 85, 1285–1290. [Google Scholar] [CrossRef]
- Figueroa, A.; Collier, S.R.; Baynard, T.; Giannopoulou, I.; Goulopoulou, S.; Fernhall, B. Impaired vagal modulation of heart rate in individuals with Down syndrome. Clin. Auton. Res. 2005, 15, 45–50. [Google Scholar] [CrossRef]
- Iellamo, F.; Galante, A.; Legramante, J.M.; Lippi, M.E.; Condoluci, C.; Albertini, G.; Volterrani, M. Altered autonomic cardiac regulation in individuals with Down syndrome. Am. J. Physiol. Heart Circ. Physiol. 2005, 289, H2387–H2391. [Google Scholar] [CrossRef]
- Goulopoulou, S.; Baynard, T.; Collier, S.; Giannopoulou, I.; Figueroa, A.; Beets, M.; Pitetti, K.; Fernhall, B. Cardiac autonomic control in individuals with Down syndrome. Am. J. Ment. Retard. 2006, 111, 27–34. [Google Scholar] [CrossRef]
- Agiovlasitis, S.; Collier, S.R.; Baynard, T.; Echols, G.H.; Goulopoulou, S.; Figueroa, A.; Beets, M.W.; Pitetti, K.H.; Fernhall, B. Autonomic response to upright tilt in people with and without Down syndrome. Res. Dev. Disabil. 2010, 31, 857–863. [Google Scholar] [CrossRef]
- Giagkoudaki, F.; Dimitros, E.; Kouidi, E.; Deligiannis, A. Effects of exercise training on heart-rate-variability indices in individuals with Down Syndrome. J. Sport Rehabil. 2010, 19, 173–183. [Google Scholar] [CrossRef]
- Agiovlasitis, S.; Baynard, T.; Pitetti, K.H.; Fernhall, B. Heart rate complexity in response to upright tilt in persons with Down syndrome. Res. Dev. Disabil. 2011, 32, 2102–2107. [Google Scholar] [CrossRef] [PubMed]
- Mendonca, G.V.; Pereira, F.D.; Fernhall, B. Cardiac autonomic function during submaximal treadmill exercise in adults with Down syndrome. Res. Dev. Disabil. 2011, 32, 532–539. [Google Scholar] [CrossRef] [PubMed]
- Mendonca, G.V.; Pereira, F.D.; Fernhall, B. Fractal scaling properties of heart rate dynamics in persons with Down syndrome. Auton Neurosci 2011, 161, 110–115. [Google Scholar] [CrossRef] [PubMed]
- Mendonca, G.V.; Pereira, F.D.; Fernhall, B. Heart rate recovery and variability following combined aerobic and resistance exercise training in adults with and without Down syndrome. Res. Dev. Disabil. 2013, 34, 353–361. [Google Scholar] [CrossRef]
- Bunsawat, K.; Goulopoulou, S.; Collier, S.R.; Figueroa, A.; Pitetti, K.H.; Baynard, T. Normal HR with tilt, yet autonomic dysfunction in persons with Down syndrome. Med. Sci. Sports Exerc. 2015, 47, 250–256. [Google Scholar] [CrossRef] [PubMed]
- De Carvalho, T.D.; de Abreu, L.C.; Mustacchi, Z.; Vanderlei, L.C.; Godoy, M.F.; Raimundo, R.D.; Ferreira Filho, C.; da Silva, T.D.; Guilhoto, L.; Perico, V.; et al. Cardiac autonomic modulation of children with Down syndrome. Pediatr. Cardiol. 2015, 36, 344–349. [Google Scholar] [CrossRef] [PubMed]
- Bunsawat, K.; Baynard, T. Cardiac autonomic modulation and blood pressure responses to isometric handgrip and submaximal cycling exercise in individuals with down syndrome. Clin. Auton. Res. 2016, 26, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Cunha, A.S.; Silva-Filho, A.C.; Dias, C.J.; Durans, R.; Brito-Monzani, J.O.; Rodrigues, B.; Mostarda, C.T. Impacts of low or vigorous levels of physical activity on body composition, hemodynamics and autonomic modulation in Down syndrome subjects. Mot. Rev. De Educ. Física 2018, 24, e1018132. [Google Scholar] [CrossRef][Green Version]
- Fatisson, J.; Oswald, V.; Lalonde, F. Influence diagram of physiological and environmental factors affecting heart rate variability: An extended literature overview. Heart Int. 2016, 11, e32–e40. [Google Scholar] [CrossRef]
- Vila, X.A.; Lado, M.J.; Cuesta-Morales, P. Evidence Based Recommendations for Designing Heart Rate Variability Studies. J. Med. Syst. 2019, 43, 311. [Google Scholar] [CrossRef]
- Quintana, D.S. Statistical considerations for reporting and planning heart rate variability case-control studies. Psychophysiology 2017, 54, 344–349. [Google Scholar] [CrossRef]
- Gilgen-Ammann, R.; Schweizer, T.; Wyss, T. RR interval signal quality of a heart rate monitor and an ECG Holter at rest and during exercise. Eur. J. Appl. Physiol. 2019, 119, 1525–1532. [Google Scholar] [CrossRef]
- Flatt, A.A.; Esco, M.R. Validity of the ithlete™ Smart Phone Application for Determining Ultra-Short-Term Heart Rate Variability. J. Hum. Kinet. 2013, 39, 85–92. [Google Scholar] [CrossRef]
- Pereira, R.A.; Alves, J.L.B.; Silva, J.H.D.C.; Costa, M.D.S.; Silva, A.S. Validity of a Smartphone Application and Chest Strap for Recording RR Intervals at Rest in Athletes. Int. J. Sports Physiol. Perform. 2020, 15, 896–899. [Google Scholar] [CrossRef]
- Jeyhani, V.; Mahdiani, S.; Peltokangas, M.; Vehkaja, A. Comparison of HRV parameters derived from photoplethysmography and electrocardiography signals. Conf. Proc. IEEE Eng. Med. Biol. Soc. 2015, 2015, 5952–5955. [Google Scholar]
- Weippert, M.; Kumar, M.; Kreuzfeld, S.; Arndt, D.; Rieger, A.; Stoll, R. Comparison of three mobile devices for measuring R-R intervals and heart rate variability: Polar S810i, Suunto t6 and an ambulatory ECG system. Eur. J. Appl. Physiol. 2010, 109, 779–786. [Google Scholar] [CrossRef] [PubMed]
- Vasconcellos, F.V.; Seabra, A.; Cunha, F.A.; Montenegro, R.A.; Bouskela, E.; Farinatti, P. Heart rate variability assessment with fingertip photoplethysmography and polar RS800cx as compared with electrocardiography in obese adolescents. Blood Press. Monit. 2015, 20, 351–360. [Google Scholar] [CrossRef] [PubMed]
- Pinheiro, N.; Couceiro, R.; Henriques, J.; Muehlsteff, J.; Quintal, I.; Goncalves, L.; Carvalho, P. Can PPG be used for HRV analysis? Conf. Proc. IEEE Eng. Med. Biol. Soc. 2016, 2016, 2945–2949. [Google Scholar]
- Guzik, P.; Piekos, C.; Pierog, O.; Fenech, N.; Krauze, T.; Piskorski, J.; Wykretowicz, A. Classic electrocardiogram-based and mobile technology derived approaches to heart rate variability are not equivalent. Int. J. Cardiol. 2018, 258, 154–156. [Google Scholar] [CrossRef]
- Malik, M.; Camm, A.J.; Huikuri, H.; Lombardi, F.; Schmidt, G.; Schwartz, P.J.; Zabel, M.; e-Rhythm Study Group of EHRA. Electronic gadgets and their health-related claims. Int. J. Cardiol. 2018, 258, 163–164. [Google Scholar] [CrossRef]
- Williams, D.P.; Jarczok, M.N.; Ellis, R.J.; Hillecke, T.K.; Thayer, J.F.; Koenig, J. Two-week test-retest reliability of the Polar® RS800CX™ to record heart rate variability. Clin. Physiol. Funct. Imaging 2017, 37, 776–781. [Google Scholar] [CrossRef] [PubMed]
- Caro, M.; Conde, D.; Pérez-Riera, A.R.; de Almeida, A.P.; Baranchuk, A. The electrocardiogram in Down syndrome. Cardiol. Young 2015, 25, 8–14. [Google Scholar] [CrossRef]
- Quintana, D.S.; Heathers, J.A.; Kemp, A.H. On the validity of using the Polar RS800 heart rate monitor for heart rate variability research. Eur. J. Appl. Physiol. 2012, 112, 4179–4180. [Google Scholar] [CrossRef]
- Merri, M.; Farden, D.C.; Mottley, J.G.; Titlebaum, E.L. Sampling frequency of the electrocardiogram for spectral analysis of the heart rate variability. IEEE Trans. Biomed. Eng. 1990, 37, 99–106. [Google Scholar] [CrossRef]
- Patel, K.; Rössler, A.; Lackner, H.K.; Trozic, I.; Laing, C.; Lorr, D.; Green, D.A.; Hinghofer-Szalkay, H.; Goswami, N. Effect of postural changes on cardiovascular parameters across gender. Medicine 2016, 95, e4149. [Google Scholar] [CrossRef]
- Alsubie, H.S.; Rosen, D. The evaluation and management of respiratory disease in children with Down syndrome (DS). Paediatr. Respir. Rev. 2018, 26, 49–54. [Google Scholar] [CrossRef]
- Santoro, S.L.; Chicoine, B.; Jasien, J.M.; Kim, J.L.; Stephens, M.; Bulova, P.; Capone, G. Pneumonia and respiratory infections in Down syndrome: A scoping review of the literature. Am. J. Med. Genet. A 2021, 185, 286–299. [Google Scholar] [CrossRef]
- Alimi, A.; Taytard, J.; Abou Taam, R.; Houdouin, V.; Forgeron, A.; Lubrano Lavadera, M.; Cros, P.; Gibertini, I.; Derelle, J.; Deschildre, A.; et al. Pulmonary hemosiderosis in children with Down syndrome: A national experience. Orphanet. J. Rare Dis. 2018, 13, 60. [Google Scholar] [CrossRef]
- George, M.; Amodio, J.; Lee, H. Cystic Lung Disease in Down Syndrome: A Case Report and Literature Review. Case Rep. Pediatr. 2016, 2016, 4048501. [Google Scholar] [CrossRef]
- Pandit, C.; Fitzgerald, D.A. Respiratory problems in children with Down syndrome. J. Paediatr. Child. Health 2012, 48, E147–E152. [Google Scholar] [CrossRef] [PubMed]
- Verstegen, R.H.; van Hout, R.W.; de Vries, E. Epidemiology of respiratory symptoms in children with Down syndrome: A nationwide prospective web-based parent-reported study. BMC Pediatr. 2014, 14, 103. [Google Scholar] [CrossRef]
- Al-Khaledi, B.; Lewis, M.; Maclean, J.E. Case 2: Recurrent lower respiratory tract infections in a child with Down syndrome. Paediatr. Child. Health 2014, 19, 19–21. [Google Scholar] [CrossRef][Green Version]
- Stebbens, V.A.; Dennis, J.; Samuels, M.P.; Croft, C.B.; Southall, D.P. Sleep related upper airway obstruction in a cohort with Down’s syndrome. Arch. Dis Child. 1991, 66, 1333–1338. [Google Scholar] [CrossRef] [PubMed]
- Hirsch, J.A.; Bishop, B. Respiratory sinus arrhythmia in humans: How breathing pattern modulates heart rate. Am. J. Physiol. Heart Circ. Physiol. 1981, 241, H620–H629. [Google Scholar] [CrossRef] [PubMed]
- Brown, T.E.; Beightol, L.A.; Koh, J.; Eckberg, D.L. Important influence of respiration on human RR interval power spectra is largely ignored. J. Appl. Physiol. 1993, 75, 2310–2317. [Google Scholar] [CrossRef] [PubMed]
- Młyńczak, M.; Krysztofiak, H. Cardiorespiratory Temporal Causal Links and the Differences by Sport or Lack Thereof. Front. Physiol. 2019, 10, 45. [Google Scholar] [CrossRef]
- Bernardi, L.; Wdowczyk-Szulc, J.; Valenti, C.; Castoldi, S.; Passino, C.; Spadacini, G.; Sleight, P. Effects of controlled breathing, mental activity and mental stress with or without verbalization on heart rate variability. J. Am. Coll. Cardiol. 2000, 35, 1462–1469. [Google Scholar] [CrossRef]
- Młyńczak, M.; Niewiadomski, W.; Żyliński, M.; Cybulski, G. Ambulatory devices measuring cardiorespiratory activity with motion. In Proceedings of the 10th International Joint Conference on Biomedical Engineering Systems and Technologies, Porto, Portugal, 21–23 February 2017; pp. 91–97. [Google Scholar]
- Młyńczak, M.; Niewiadomski, W.; Żyliński, M.; Cybulski, G.P. Ambulatory Impedance Pneumography Device for Quantitative Monitoring of Volumetric Parameters in Respiratory and Cardiac Applications. In Proceedings of the Computing in Cardiology Conference (CinC), Cambridge, MA, USA, 7–10 September 2014. [Google Scholar]
- Gąsior, J.S.; Sacha, J.; Jeleń, P.J.; Zieliński, J.; Przybylski, J. Heart Rate and Respiratory Rate Influence on Heart Rate Variability Repeatability: Effects of the Correction for the Prevailing Heart Rate. Front. Physiol. 2016, 7, 356. [Google Scholar] [CrossRef]
- Sinnecker, D.; Dommasch, M.; Barthel, P.; Müller, A.; Dirschinger, R.J.; Hapfelmeier, A.; Huster, K.M.; Laugwitz, K.L.; Malik, M.; Schmidt, G. Assessment of mean respiratory rate from ECG recordings for risk stratification after myocardial infarction. J. Electrocardiol. 2014, 47, 700–704. [Google Scholar] [CrossRef]
- Hoffmann, B.; Flatt, A.A.; Silva, L.E.V.; Młyńczak, M.; Baranowski, R.; Dziedzic, E.; Werner, B.; Gąsior, J.S. A Pilot Study of the Reliability and Agreement of Heart Rate, Respiratory Rate and Short-Term Heart Rate Variability in Elite Modern Pentathlon Athletes. Diagnostics 2020, 10, 833. [Google Scholar] [CrossRef] [PubMed]
- Sandercock, G.; Gladwell, V.; Dawson, S.; Nunan, D.; Brodie, D.; Beneke, R. Association between RR interval and high-frequency heart rate variability acquired during short-term, resting recordings with free and paced breathing. Physiol. Meas. 2008, 29, 795–802. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, H. Does paced breathing improve the reproducibility of heart rate variability measurements? J. Physiol. Anthropol. 2009, 28, 225–230. [Google Scholar] [CrossRef] [PubMed]
- Frederiks, J.; Swenne, C.A.; TenVoorde, B.J.; Honzíková, N.; Levert, J.V.; Maan, A.C.; Schalij, M.J.; Bruschke, A.V. The importance of high-frequency paced breathing in spectral baroreflex sensitivity assessment. J. Hypertens. 2000, 18, 1635–1644. [Google Scholar] [CrossRef] [PubMed]
- Faes, L.; Nollo, G.; Porta, A. Information domain approach to the investigation of cardio-vascular, cardio-pulmonary, and vasculo-pulmonary causal couplings. Front. Physiol. 2011, 2, 80. [Google Scholar] [CrossRef]
- Wang, Y.P.; Kuo, T.B.; Lai, C.T.; Chu, J.W.; Yang, C.C. Effects of respiratory time ratio on heart rate variability and spontaneous baroreflex sensitivity. J. Appl. Physiol. 2013, 115, 1648–1655. [Google Scholar] [CrossRef]
- Shaffer, F.; Combatalade, D.C. Don’t add or miss a beat: A guide to cleaner heart rate variability recordings. Biofeedback 2013, 41, 121–130. [Google Scholar] [CrossRef]
- Rincon Soler, A.I.; Silva, L.E.V.; Fazan, R., Jr.; Murta, L.O., Jr. The impact of artifact correction methods of RR series on heart rate variability parameters. J. Appl. Physiol. 2018, 124, 646–652. [Google Scholar] [CrossRef] [PubMed]
- Morelli, D.; Rossi, A.; Cairo, M.; Clifton, D.A. Analysis of the Impact of Interpolation Methods of Missing RR-intervals Caused by Motion Artifacts on HRV Features Estimations. Sensors 2019, 19, 3163. [Google Scholar] [CrossRef]
- Alcantara, J.M.A.; Plaza-Florido, A.; Amaro-Gahete, F.J.; Acosta, F.M.; Migueles, J.H.; Molina-Garcia, P.; Sacha, J.; Sanchez-Delgado, G.; Martinez-Tellez, B. Impact of Using Different Levels of Threshold-Based Artefact Correction on the Quantification of Heart Rate Variability in Three Independent Human Cohorts. J. Clin. Med. 2020, 9, 325. [Google Scholar] [CrossRef] [PubMed]
- Kaufmann, T.; Sütterlin, S.; Schulz, S.M.; Vögele, C. ARTiiFACT: A tool for heart rate artifact processing and heart rate variability analysis. Behav. Res. Methods 2011, 43, 1161–1170. [Google Scholar] [CrossRef]
- Vest, A.N.; Da Poian, G.; Li, Q.; Liu, C.; Nemati, S.; Shah, A.J.; Clifford, G.D. An open source benchmarked toolbox for cardiovascular waveform and interval analysis. Physiol. Meas. 2018, 39, 105004. [Google Scholar] [CrossRef]
- Rogers, B.; Giles, D.; Draper, N.; Mourot, L.; Gronwald, T. Influence of Artefact Correction and Recording Device Type on the Practical Application of a Non-Linear Heart Rate Variability Biomarker for Aerobic Threshold Determination. Sensors 2021, 21, 821. [Google Scholar] [CrossRef]
- Clifford, G.D.; Tarassenko, L. Quantifying errors in spectral estimates of HRV due to beat replacement and resampling. IEEE Trans. Biomed. Eng. 2005, 52, 630–638. [Google Scholar] [CrossRef]
- Jarrin, D.C.; McGrath, J.J.; Giovanniello, S.; Poirier, P.; Lambert, M. Measurement fidelity of heart rate variability signal processing: The devil is in the details. Int. J. PsychoPhysiol. 2012, 86, 88–97. [Google Scholar] [CrossRef]
- Królak, A.; Wiktorski, T.; Bjørkavoll-Bergseth, M.F.; Ørn, S. Artifact Correction in Short-Term HRV during Strenuous Physical Exercise. Sensors 2020, 20, 6372. [Google Scholar] [CrossRef] [PubMed]
- Lipponen, J.A.; Tarvainen, M.P. A robust algorithm for heart rate variability time series artefact correction using novel beat classification. J. Med. Eng. Technol. 2019, 43, 173–181. [Google Scholar] [CrossRef]
- Plaza-Florido, A.; Alcantara, J.M.A.; Amaro-Gahete, F.J.; Sacha, J.; Ortega, F.B. Cardiovascular Risk Factors and Heart Rate Variability: Impact of the Level of the Threshold-Based Artefact Correction Used to Process the Heart Rate Variability Signal. J. Med. Syst. 2020, 45, 2. [Google Scholar] [CrossRef]
- Peng, C.K.; Havlin, S.; Stanley, H.E.; Goldberger, A.L. Quantification of scaling exponents and crossover phenomena in nonstationary heartbeat time series. Chaos 1995, 5, 82–87. [Google Scholar] [CrossRef]
- Porta, A.; Guzzetti, S.; Montano, N.; Furlan, R.; Pagani, M.; Malliani, A.; Cerutti, S. Entropy, entropy rate, and pattern classification as tools to typify complexity in short heart period variability series. IEEE Trans. Biomed. Eng. 2001, 48, 1282–1291. [Google Scholar] [CrossRef] [PubMed]
- Costa, M.; Goldberger, A.L.; Peng, C.K. Multiscale entropy analysis of biological signals. Phys. Rev. E Stat. Nonlin. Soft Matter Phys. 2005, 71, 021906. [Google Scholar] [CrossRef] [PubMed]
- Heathers, J.A.J. The last word. Exp. Physiol. 2013, 98, 348. [Google Scholar] [CrossRef] [PubMed]
- Pichon, A.; Roulaud, M.; Antoine-Jonville, S.; de Bisschop, C.; Denjean, A. Spectral analysis of heart rate variability: Interchangeability between autoregressive analysis and fast Fourier transform. J. Electrocardiol. 2006, 39, 31–37. [Google Scholar] [CrossRef]
- Sassi, R.; Cerutti, S.; Lombardi, F.; Malik, M.; Huikuri, H.V.; Peng, C.K.; Schmidt, G.; Yamamoto, Y. Advances in heart rate variability signal analysis: Joint position statement by the e-Cardiology ESC Working Group and the European Heart Rhythm Association co-endorsed by the Asia Pacific Heart Rhythm Society. Europace 2015, 17, 1341–1353. [Google Scholar] [CrossRef]
- Henriques, T.; Ribeiro, M.; Teixeira, A.; Castro, L.; Antunes, L.; Costa-Santos, C. Nonlinear Methods Most Applied to Heart-Rate Time Series: A Review. Entropy 2020, 22, 309. [Google Scholar] [CrossRef]
- Voss, A.; Schulz, S.; Schroeder, R.; Baumert, M.; Caminal, P. Methods derived from nonlinear dynamics for analysing heart rate variability. Philos. Trans. A Math. Phys. Eng. Sci. 2009, 367, 277–296. [Google Scholar] [CrossRef] [PubMed]
- Sacha, J.; Barabach, S.; Statkiewicz-Barabach, G.; Sacha, K.; Müller, A.; Piskorski, J.; Barthel, P.; Schmidt, G. How to strengthen or weaken the HRV dependence on heart rate—Description of the method and its perspectives. Int. J. Cardiol. 2013, 168, 1660–1663. [Google Scholar] [CrossRef]
- Sacha, J.; Sobon, J.; Sacha, K.; Barabach, S. Heart rate impact on the reproducibility of heart rate variability analysis. Int. J. Cardiol. 2013, 168, 4257–4259. [Google Scholar] [CrossRef]
- Monfredi, O.; Lyashkov, A.E.; Johnsen, A.B.; Inada, S.; Schneider, H.; Wang, R.; Nirmalan, M.; Wisloff, U.; Maltsev, V.A.; Lakatta, E.G.; et al. Biophysical characterization of the underappreciated and important relationship between heart rate variability and heart rate. Hypertension 2014, 64, 1334–1343. [Google Scholar] [CrossRef] [PubMed]
- Silva, L.E.; Salgado, H.C.; Fazan, R., Jr. Mean Heart Rate Level Does Not Affect All Heart Rate Variability Indices. Hypertension 2017, 69, e21–e22. [Google Scholar] [CrossRef] [PubMed]
- Huikuri, H.V.; Mäkikallio, T.; Airaksinen, K.E.; Mitrani, R.; Castellanos, A.; Myerburg, R.J. Measurement of heart rate variability: A clinical tool or a research toy? J. Am. Coll. Cardiol. 1999, 34, 1878–1883. [Google Scholar] [CrossRef] [PubMed]
- Plaza-Florido, A.; Alcantara, J.M.A.; Migueles, J.H.; Amaro-Gahete, F.J.; Acosta, F.M.; Mora-Gonzalez, J.; Sacha, J.; Ortega, F.B. Inter- and intra-researcher reproducibility of heart rate variability parameters in three human cohorts. Sci. Rep. 2020, 10, 11399. [Google Scholar] [CrossRef]
- Farah, B.Q.; Lima, A.H.; Cavalcante, B.R.; de Oliveira, L.M.; Brito, A.L.; de Barros, M.V.; Ritti-Dias, R.M. Intra-individuals and inter- and intra-observer reliability of short-term heart rate variability in adolescents. Clin. Physiol. Funct. Imaging 2016, 36, 33–39. [Google Scholar] [CrossRef]
- Tarvainen, M.P.; Niskanen, J.P.; Lipponen, J.A.; Ranta-Aho, P.O.; Karjalainen, P.A. Kubios HRV—Heart rate variability analysis software. Comput. Methods Programs Biomed. 2014, 113, 210–220. [Google Scholar] [CrossRef]
- Silva, L.E.V.; Fazan, R., Jr.; Marin-Neto, J.A. PyBioS: A freeware computer software for analysis of cardiovascular signals. Comput. Methods Programs Biomed. 2020, 197, 105718. [Google Scholar] [CrossRef]
- Plaza-Florido, A.; Sacha, J.; Alcantara, J. Short-term heart rate variability in resting conditions: Methodological considerations. Kardiol. Pol. 2021, 79, 745–755. [Google Scholar] [CrossRef]
- Eckberg, D.L. Sympathovagal balance: A critical appraisal. Circulation 1997, 96, 3224–3232. [Google Scholar] [CrossRef]
- Moak, J.P.; Goldstein, D.S.; Eldadah, B.A.; Saleem, A.; Holmes, C.; Pechnik, S.; Sharabi, Y. Supine low-frequency power of heart rate variability reflects baroreflex function, not cardiac sympathetic innervation. Heart Rhythm. 2007, 4, 1523–1529. [Google Scholar] [CrossRef]
- Goldstein, D.S.; Bentho, O.; Park, M.Y.; Sharabi, Y. Low-frequency power of heart rate variability is not a measure of cardiac sympathetic tone but may be a measure of modulation of cardiac autonomic outflows by baroreflexes. Exp. Physiol. 2011, 96, 1255–1261. [Google Scholar] [CrossRef]
- Rahman, F.; Pechnik, S.; Gross, D.; Sewell, L.; Goldstein, D.S. Low frequency power of heart rate variability reflects baroreflex function, not cardiac sympathetic innervation. Clin. Auton. Res. 2011, 21, 133–141. [Google Scholar] [CrossRef] [PubMed]
- Heathers, J.A. Sympathovagal balance from heart rate variability: An obituary. Exp. Physiol. 2012, 97, 556. [Google Scholar] [CrossRef]
- Billman, G.E. The LF/HF ratio does not accurately measure cardiac sympatho-vagal balance. Front. Physiol. 2013, 4, 26. [Google Scholar] [CrossRef] [PubMed]
- Draghici, A.E.; Taylor, J.A. The physiological basis and measurement of heart rate variability in humans. J. Physiol. Anthropol. 2016, 35, 22. [Google Scholar] [CrossRef]
- Del Paso, G.A.R.; Langewitz, W.; Mulder, L.J.; van Roon, A.; Duschek, S. The utility of low frequency heart rate variability as an index of sympathetic cardiac tone: A review with emphasis on a reanalysis of previous studies. Psychophysiology 2013, 50, 477–487. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| First Author and Year of Publication | Experimental Group | Control Group | RR Intervals Acquisition | ||||
|---|---|---|---|---|---|---|---|
| Software for RR Intervals Acquisition, Sampling Frequency and Duration of Recordings | Time of the Day and Room (Lights/Voices/Temperature) | Behaviors before Data Acquisition (Sleep Routine, Physical Activities, Meal, Drinks, Toilet before) and Instructions Given. Rest or Heart Rate Stabilization before Recordings | Respiratory Rate (Breathing Control) during Recording | Position during Recordings | |||
| Ferri et al., 1998 [49] | 7 DS children Age: 13.9 years (range: 8.6–16.5) Additional characteristics: BMI | 6 normally developed children Age: 12.8 years (range: 8.0–17.5) | Software: ECG: Oxford MPA-II recorder Sampling: 128 Hz Duration: 10 min | Subjects slept in laboratory for two consecutive nights, the recording of data carried out during the second night. | Measurements carried out during sleeping. | NR Respiratory pauses and oxygen desaturations detected automatically by the software Oxford Medilog 9200 System. | During sleeping |
| Baynard et al., 2004 [50] | 16 individuals with DS (10♂) with mental retardation (MR) Age: 20.8 ± 0.9 years Additional characteristics: height, weight, BMI, VO2 peak, RER peak, VE peak | 15 patients with MR (8♂) Age: 19.7 ± 2.3 years | Software: HRM: Polar Electro Oy, Kempele, Finland Sampling: resolution 1 ms Duration: 5 min seated rest; 4 min submaximal exercise stages | NR | Participants familiarized with the laboratory setting, treadmill walking, and use of the headgear and mouthpiece. Participants: rested quietly in a seated position for 5 min; performed 4 min submaximal exercise stages on a treadmill (treadmill protocol individualized); asked not to eat or drink caffeinated beverages 4 h before testing. 5 min | NR Oxygen consumption measured during the entire exercise period. | Seated (5 min) and 4 min submaximal exercise stages on a treadmill. |
| Figueroa et al., 2005 [51] | 13 individuals with DS (8♂) Age: 27.8 ± 8.1 years Additional characteristics: height, weight, BMI, maximal grip strength | 14 without DS (6♂) Age: 26.4 ± 7.5 years | Software: one lead ECG (BIOPAC) Sampling: NR Duration: 2 min period at rest, handgrip strength test and recovery | NR | Participants underwent laboratory familiarization with testing procedures prior to data collection. Participants: - tested in a post-prandial state (~3 h) and refrained from vigorous exercise 24 h before the testing; - asked to refrain from caffeine ingestion on the testing day. 5 min | NR Participants: breathing spontaneously; instructed to refrain from holding their breath and avoid Valsalva maneuver during the handgrip strength test | Seated, sustained handgrip at 30% MVC |
| Iellamo et al., 2005 [52] | 10 individuals with DS (4♂) Age: 26.3 ± 2.3 years Additional characteristics: BMI | 10 healthy volunteers (4♂)Age: 26.1 ± 4.0 years | Software: ECG—precordial chest lead (Biopac System) Sampling: 300 Hz/channelDuration: 10 min | Experiments performed in the morning in a laboratory at ambient temperature (22–24 °C). | Participants required not to eat or drink coffee for at least 2 h. The participants lay in a room made dark and noiseless. After instrumentation, the subjects lay supine for 15 min before experiments to relax (dark room, noiseless). | Respiratory signal recorded by means of a thoracic belt (Biopac). Respiratory spectra used to assess the main respiratory frequency and to locate the respiratory component of the power spectral analysis of RR interval variability. | 10 min of supine rest followed by 10 min of active orthostatism. |
| Goulopoulou et al., 2006 [53] | 50 individuals with DS (27♂) Age: 24 ± 0.9 years Additional characteristics: height, weight, BMI, VO2 peak | 24 healthy controls (12♂) Age: 26 ± 1.1 years | Software: Modified CM5 ECG lead (Biopac Systems, CA, USA) Sampling: 1000 Hz Duration: 5 min | NR | Participants tested 4 h after their last meal and asked to refrain from exercise 24 h prior to testing and from caffeine ingestion on testing days. Prior to data collection, participants familiarized with all testing procedures. Sessions continued until each participant could comfortably walk on a motorized treadmill. 5 min | Breathing rate was visually monitored and averaged between 14 and 18 breaths per minute. | Rest and treadmill exercise test |
| Agiovlasitis et al., 2010 [54] | 26 DS individuals (18♂) Age: 26.5 ± 7.6 (16–40) years Additional characteristics: height, weight, BMI | 11 individuals without DS (5♂) Age: 25.5 ± 7.3 (17–39) years | Software: Finger photo-plethysmography (Portapres, TNO Biomedical Instrumentation Amsterdam, The Netherlands) Sampling: 200 Hz Duration: 5 min | NR | No food for at least 4 h prior, no caffeine or exercise for 24 h prior to testing. 5 min | NR | Supine and 80° head-up tilt using a tilt table |
| Giagkoudaki et al., 2010 [55] | 10 DS individuals (4♂) Age 24.2 ± 5.1 years Additional characteristics: height, weight, BMI | 10 healthy sedentary individuals (5♂) Age 23.3 ± 4.6 years | Software: 3-channel ECG Holter recorder with WinTer Holter Analyzer software (Galix Biomedical) Sampling: NR Duration: 24 h | Assessments made at baseline and after 6 months. 6-month exercise-training program conducted 3 times per week and lasted 60 min, led by three expert exercise trainers. | Participants asked to avoid caffeine and alcoholic beverages, any activity other than their daily activities that could affect heart rhythm, during the recording, to abstain from exercise when HRV data were collected at the beginning of the study and after the 6-month exercise-training program. | NR | 24 h ambulatory ECG Holter |
| Agiovlasitis et al., 2011 [56] | 16 DS individuals (8♂) Age: 26 ± 8 years Additional characteristics: height, weight, BMI | 16 individuals without DS (8♂) Age: 26 ± 7 years | Software: ECG CM5 configuration (Biopac Systems, Goleta, CA, USA) Sampling: 1000 HzDuration: 10 min rest and 10 min upright tilt | NR | Participants familiarized with the experimental procedures, refrained from food for at least 4 h and from caffeine and exercise for 24 h prior to testing. 10 min in the supine position | NR | Supine and 80° head-up tilt |
| Mendonca et al., 2011 [57] | 13 individuals with DS (9♂) Age: 34.9 ± 1.1 years (27–48) Additional characteristics: height, weight, BMI, VO2 peak, RER peak, VE peak, VO2VT | 12 individuals without DS (8♂) Age: 34.8 ± 2.0 years (27–48) | Software: HRM: Polar RS 800 G3 Heart Rate monitor (Polar Electro, Kempele, Finland) Sampling: 1000 Hz Duration: 5 min | Tests carried out in the laboratory with temperature between 21 and 24 °C and a relative humidity between 44 and 56% between the hours of 7.00 and 11.00 h at approx. the same time of day for all individuals. Visits minimum of 2 days apart and a maximum of 7 days apart. | Participants familiarized with the laboratory setting, treadmill protocols, and use of the headgear and face mask. Participants asked to abstain from caffeine and vigorous exercise for 24 h prior to testing and be at least 3 h post-prandial before testing. 5 min | NR Expired gas measurements made using a computerized on-line breath-by-breath system (Quark b2, Cosmed Srl-Italy) | Seated rest, standing, submaximal treadmill exercise, standing post-exercise recovery |
| Mendonca et al., 2011 [58] | 14 individuals with DS (10♂) Age: 35.1 ± 7.8 years (18–50) Additional characteristics: height, weight, BMI, VO2 peak, RER peak, VE peak | 12 individuals without DS (8♂) Age: 36.0 ± 7.7 years (20–49) | Software: HRM: Polar RS 800 G3 Heart Rate monitor (Polar Electro, Kempele, Finland) Sampling: 1000 Hz Duration: NR | As above [57] | As above [57] | NR Expired gas measurements made using a portable mixing chamber system (MetaMax® I, Cortex, Leipzig, Germany) | Standing rest, submaximal treadmill exercise, standing post-exercise recovery |
| Mendonca et al., 2013 [59] | 13 individuals with DS (10♂) Age: 36.5 ± 1.5 years (27–50) Additional characteristics: height, weight, BMI | 12 individuals without DS (9♂) Age: 38.7 ± 2.4 years (27–50) | Software: HRM: Polar RR Recorder, Polar Electro, Kempele, Finland) Sampling: 1000 Hz Duration: 10 min | Participants evaluated pre- and post-training periods: first performed a treadmill, second rested position on a bed in a quiet, semi-dark environment. Tests carried out in the laboratory with a controlled temperature (21–24 °C) and humidity (44–56%). | Participants tested in the postprandial state (12 h) and asked to refrain from caffeine and exercise for 24 h before testing. After the 12 weeks of training, all participants repeated the testing procedures under the same conditions and at the same time of day. Participants asked to remain quietly without speaking or making any movements for 15 min. | Spontaneous breathing conditions. To control for the stability of breathing rate and tidal volume, participants monitored during the 10 min of supine rest using a portable mixing chamber system (Metamax1 I, Cortex, Leipzig, Germany). | First visit—treadmill graded exercise test. Second visit (48 h after the first visit) rested while lying down in the supine position on a bed. |
| Bunsawat et al., 2015 [60] | 26 persons with DS: not matched for HR change (n = 11, 6♂)—age: 28 ± 3 years; matched for HR change (n = 15, 8♂)—age: 25 ± 2 years; Additional characteristics: height, weight, BMI, VO2 peak, RER peak, VE peak | 15 persons without DS (6♂) Age: 27 ± 2 years | Software: single-lead ECG (BIOPAC, Santa Barbara, CA) Sampling: 1000 HzDuration: 5 min in supine (the last 5 min of the 10 min period) and 5 during an 80° head-up tilt | The passive upright tilt performed on the second day in the morning at ambient temperature (22–24 °C) | Participants in the postprandial state for 4 h and refrained from caffeine and exercise for 24 h before data collection on each testing day. The first day of testing consisted of a maximal exercise test on a motorized treadmill. | NR | Supine position for 10 min and 5 min 80° head-up tilt |
| de Carvalho et al., 2015 [61] | 25 individuals with DS (16♂) Age: 8.6 ± 1.4 years Additional characteristics: height, weight, BMI | 25 individuals without DS (16♂) Age 9.1 ± 1.2 years | Software: HRM: Polar RS800 CX monitor, Polar Electro OY, Kempele, Finland Sampling: NRDuration: 20 min | Data collected under controlled temperature (21–23 °C) and humidity (40–60%). Evaluations between 8:00 am and 11:00 am. Parents/guardian of the children stayed in the room, during all protocol. | Participants instructed to avoid consuming caffeine for 24 h before evaluation. | Spontaneous breathing | Supine |
| Bunsawat et al., 2016 [62] | HGS test study: 10 subjects with DS (6♂) Age: 26 ± 3 years Submaximal cycling exercise (SCE test): 9 subjects with DS (9♂) Age: 30 ± 2 Subjects with and without DS were matched for HR change during SCE test. Additional characteristics: height, weight, BMI, VO2 peak | HGS test study: 8 controls without DS (2♂) Age: 28 ± 3 years SCE test: 9 controls without DS (3♂) Age: 27 ± 3 | Software: CM5 lead ECG (BIOPAC, Santa Barbara, CA) Sampling: 1000 Hz Duration: HGS test: 2 min periods: rest–HGS test (30% MVC)–recoverySCE test: two 6 min stages | Ambient temperature (22–24 °C) | Participants in the postprandial state for 4 h and refrained from caffeine and exercise for 24 h before data collection. | Participants encouraged to breath spontaneously without performing the Valsalva during HGS test. | HGS test—seated position; SCE test |
| Cunha et al., 2018 [63] | 36 male DS subjects (3 groups):15 sedentary subjects Age: 26 ± 7 years 9 subjects with low intensity levels of PA Age: 26 ± 1 years 12 subjects with vigorous intensity levels of PA Age: 24 ± 2 years Additional characteristics: height, weight, BMI, lean and fat mass, IPAQ, MET | 13 individuals without DS Age: 29 ± 4 years | Software: ECG (Wincardio Micromed 600 Hz, Brasilia, DF, Brazil) Sampling: 600 Hz Duration: 10 min | NR | NR | NR | Supine position with head elevation of 30° |
| First Author and Year of Publication | Software | Artifact Correction | Time Series Length (Time/Beats) | Information about Data Normality | Time Domain Parameters (Units) | Frequency Domain Parameters and Bands (Units) | Frequency Analysis Method with Details | Nonlinear Parameters |
|---|---|---|---|---|---|---|---|---|
| Ferri et al., 1998 [49] | NR | 10 min epoch ECG signals analyzed for automatic detection of R waves with a self-made program utilizing a simple threshold plus first derivative algorithm. Careful visual inspection for possible errors performed on all epochs. | 10 min period within the first or second sleep cycle: W + S1 (sleep Stage 1, including wake around sleep), S2 (sleep Stage 2), SWS (sleep Stages 3 and/or 4) and REM sleep. The first 512 RR intervals from each epoch utilized for subsequent analysis steps. | NR | mRR (s), SDNN (NR), RMSSD (NR), pNN50 (%) | VLF <0.04 (s2/beat, cycles/beat), LF 0.04–0.15 Hz (s2/beat, cycles/beat), HF 0.15–0.4 Hz (s2/beat, cycles/beat), TP (s2/beat, cycles/beat), LF% (nu), HF% (nu), LF/HF | Parabolic interpolation used. FFT | Did not perform nonlinear analysis |
| Baynard et al., 2004 [50] | Heart Signal Co, Oulu, Finland | RR intervals visually inspected and filtered to eliminate undesirable noise or premature beats. Any RR interval that deviated > than 30% from the previous one was considered premature. Only recordings in which fewer than 2% of beats were filtered were included in HRV analysis. | Final 2 min of each submaximal stage, and the first 2 submaximal stages used for HRV analysis. | NR | SDNN (ms), RMSSD (ms2), pNN50 (%) | LF 0.04–0.15 Hz (ms2, nu), HF 0.15–0.40 Hz (ms2, nu), LF/HF Values in nu—graphical presentation | AR | Did not perform nonlinear analysis |
| Figuero et al., 2005 [51] | Heart Signal software (Oulu, Finland) | ECG data visually analyzed and edited for arrhythmias and artifacts. | HRV analyses performed for a 2 min period at rest, handgrip and recovery. Components detected from segments of 500 beats. | NR Parameters transformed to their natural logarithm for statistical analysis because of their skewed distribution. | Did not perform time domain analysis | LF 0.04–0.15 Hz (ms2) HF 0.15–0.40 Hz (ms2) LF/HF | AR (model order 10) | Did not perform nonlinear analysis |
| Iellamo et al., 2005 [52] | NR | NR | NR | Kolmogorov–Smirnov test | Did not perform time domain analysis | LF 0.03–0.15 Hz (ms2, nu) HF 0.15–0.40 Hz (ms2, nu) | The harmonic components of RR interval variability evaluated by the AR method (model order 8–12). | Did not perform nonlinear analysis |
| Goulopoulou et al., 2006 [53] | HEARTSTM, Finland | Visual and automatic editing to eliminate noise or premature beats. The filtering and analysis procedure: any time between heart beat interval that deviated > than 30% from the previous interval was considered premature. Recordings in which more than 2% of beats were filtered were repeated. | NR | Data not normally distributed. Logarithmic transformation was performed. | SDNN (ms) RMSSD (ms) | LF 0.04–0.14 Hz (ms2) HF 0.15–0.40 Hz (ms2) LF/HF TP | AR model (order 10) | Did not perform nonlinear analysis |
| Agiovlasitis et al., 2010 [54] | WinCPRS software (Absolute Aliens, Turku, Finland) | Ectopic beats and artifacts confirmed by visual inspection. | NR | NR | Did not perform time domain analysis | LF: 0.04–0.15 Hz (nu)HF: 0.15–0.40 Hz (nu) TP (ms2) LF/HF | From the blood pressure waves, the software generated the time series of the RR intervals analyzed to obtain the spectral components of HRV (AR). | Did not perform nonlinear analysis |
| Giagkoudaki et al., 2010 [55] | WinTer Holter Analyzer software | Ectopic beats and artifacts automatically and manually discarded. | NR | NR | SDNN (ms) SDANN (ms) SDNN index (ms) rMSSD (ms) pNN50 (ms) | LF: 0.04–0.15 Hz (ms2, nu) HF: 0.15–0.40 Hz (ms2, nu) | FFT The data were neither resampled nor interpolated. | Did not perform nonlinear analysis. |
| Agiovlasitis et al., 2011 [56] | WinCPRS software (Absolute Aliens, Turku, Finland) | RR intervals were steady-state and free of artifact and ectopy | 550 continuous RR intervals | NR | mRR (ms) | Did not perform frequency domain analysis. | RR intervals detrended and resampled at 5 Hz. | ApEn (embedding dimension = 2, filter parameter = 20%), correlation dimension, StatAv - stationarity of the HR signal |
| Mendonca et al., 2011 [57] |
| Visually inspected for undesirable premature beats and noise. RR interval interpreted as premature if it deviated from the previous interval by >30%. | 256 consecutive RR intervals | Data tested for normality and homoscedasticity with the Kolmogorov–Smirnov and Levene’s tests | Did not perform time domain analysis. | LF: 0.04–0.15 Hz (ms2) HF: 0.15–1.00 Hz [ms2] | Time series detrended and resampled at 4 Hz. AR (model order 16). | Did not perform nonlinear analysis. |
| Mendonca et al., 2011 [58] |
| Visually inspected for undesirable premature beats and noise. | 256 consecutive RR intervals | Data tested for normality and homoscedasticity with the Kolmogorov–Smirnov and Levene’s tests | Did not perform time domain analysis. | Did not perform frequency domain analysis. | NR | DFA—short-term (4–16 beats) scaling exponent |
| Mendonca et al., 2013 [59] |
| Analyses performed from the RR interval epochs free from ectopic beats and technical artifacts. | 10 min | Data tested for normality and homoscedasticity with the Kolmogorov–Smirnov and Levene’s tests | Did not perform time domain analysis. | LF: 0.04–0.15 Hz (ms2, nu) HF: 0.15–0.40 Hz (ms2, nu) TP: 0.04–0.4 Hz | RR interval series resampled at 4 Hz (linear interpolation). A polynomial filter used to remove low frequency trends. AR (model order 16). | Did not perform nonlinear analysis |
| Bunsawat et al., 2015 [60] | HRV analyzed offline using Heart Signal software (Oulu, Finland) | ECG automatically and visually analyzed, edited for arrhythmias and artifacts. | RR interval variability evaluated from segments of 500 beats. | Shapiro–Wilk tests | RMSSD (ms) | LF: 0.04–0.15 Hz (ms2) HF: 0.15–0.40 Hz (ms2) | AR method (model order 10) | Did not perform nonlinear analysis |
| de Carvalho et al., 2015 [61] |
| Manually complemented, visual inspection of the time series showed absence of artifacts. | 1000 consecutive RR intervals | Shapiro–Wilks test | mRR (ms) SDNN (ms) RMSSD (ms) NN50 (ms) pNN50 (ms) | LF: 0.04–0.15 Hz (ms2, nu) HF: 0.15–0.40 Hz (ms2, nu) LF/HF | FFT | Did not perform nonlinear analysis. |
| Bunsawat et al., 2016 [62] | Heart Signal software (Oulu, Finland) | ECG automatically, visually analyzed, edited for arrhythmias and artifacts. | NR | Shapiro–Wilk tests | RMSSD (ms) | LF: 0.04–0.15 Hz (ms2) HF: 0.15–0.40 Hz (ms2) | AR method (model order 10) | Did not perform nonlinear analysis |
| Cunha et al., 2018 [63] | Kubios HRV 2.0 (Biosignal Analysis and Medical Imaging Group, Kuopio, Finland) | NR | 5 min | Shapiro–Wilk tests | SDNN and RMSSD were chosen, in tables results for RR (ms) and total variability (ms2) provided | LF: 0.04–0.15 Hz (ms2, nu) HF: 0.15–0.40 Hz (ms2, nu) LF/HF | FFT Interpolation of 4 Hz, overlapped by 50% | Symbolic analysis: 0V, 1V, 2LV, 2UV |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gąsior, J.S.; Zamunér, A.R.; Madeyska, M.; Tomik, A.; Niszczota, C.; Williams, C.A.; Werner, B. Heart Rate Variability in Individuals with Down Syndrome: A Scoping Review with Methodological Considerations. Int. J. Environ. Res. Public Health 2023, 20, 941. https://doi.org/10.3390/ijerph20020941
Gąsior JS, Zamunér AR, Madeyska M, Tomik A, Niszczota C, Williams CA, Werner B. Heart Rate Variability in Individuals with Down Syndrome: A Scoping Review with Methodological Considerations. International Journal of Environmental Research and Public Health. 2023; 20(2):941. https://doi.org/10.3390/ijerph20020941
Chicago/Turabian StyleGąsior, Jakub S., Antonio Roberto Zamunér, Margaret Madeyska, Anna Tomik, Cezary Niszczota, Craig A. Williams, and Bożena Werner. 2023. "Heart Rate Variability in Individuals with Down Syndrome: A Scoping Review with Methodological Considerations" International Journal of Environmental Research and Public Health 20, no. 2: 941. https://doi.org/10.3390/ijerph20020941
APA StyleGąsior, J. S., Zamunér, A. R., Madeyska, M., Tomik, A., Niszczota, C., Williams, C. A., & Werner, B. (2023). Heart Rate Variability in Individuals with Down Syndrome: A Scoping Review with Methodological Considerations. International Journal of Environmental Research and Public Health, 20(2), 941. https://doi.org/10.3390/ijerph20020941