

Positive Impacts of a Four-Week Neuro-Meditation Program on Cognitive Function in Post-Acute Sequelae of COVID-19 Patients: A Randomized Controlled Trial

Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
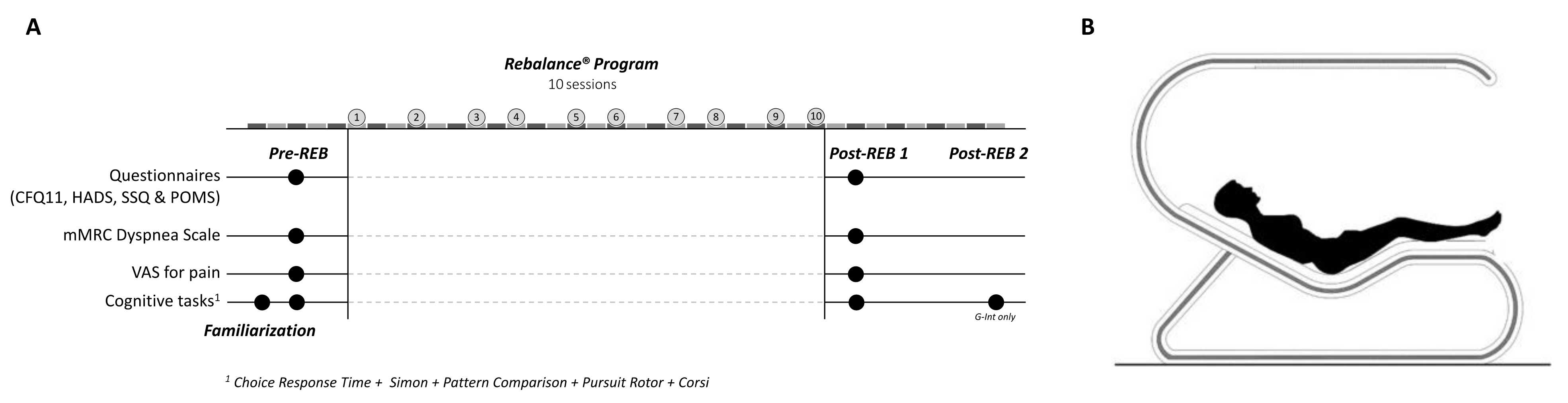
2.2. Study Design and Procedures
2.2.1. The Rebalance Program
2.2.2. Measures
Self-Administered Questionnaires
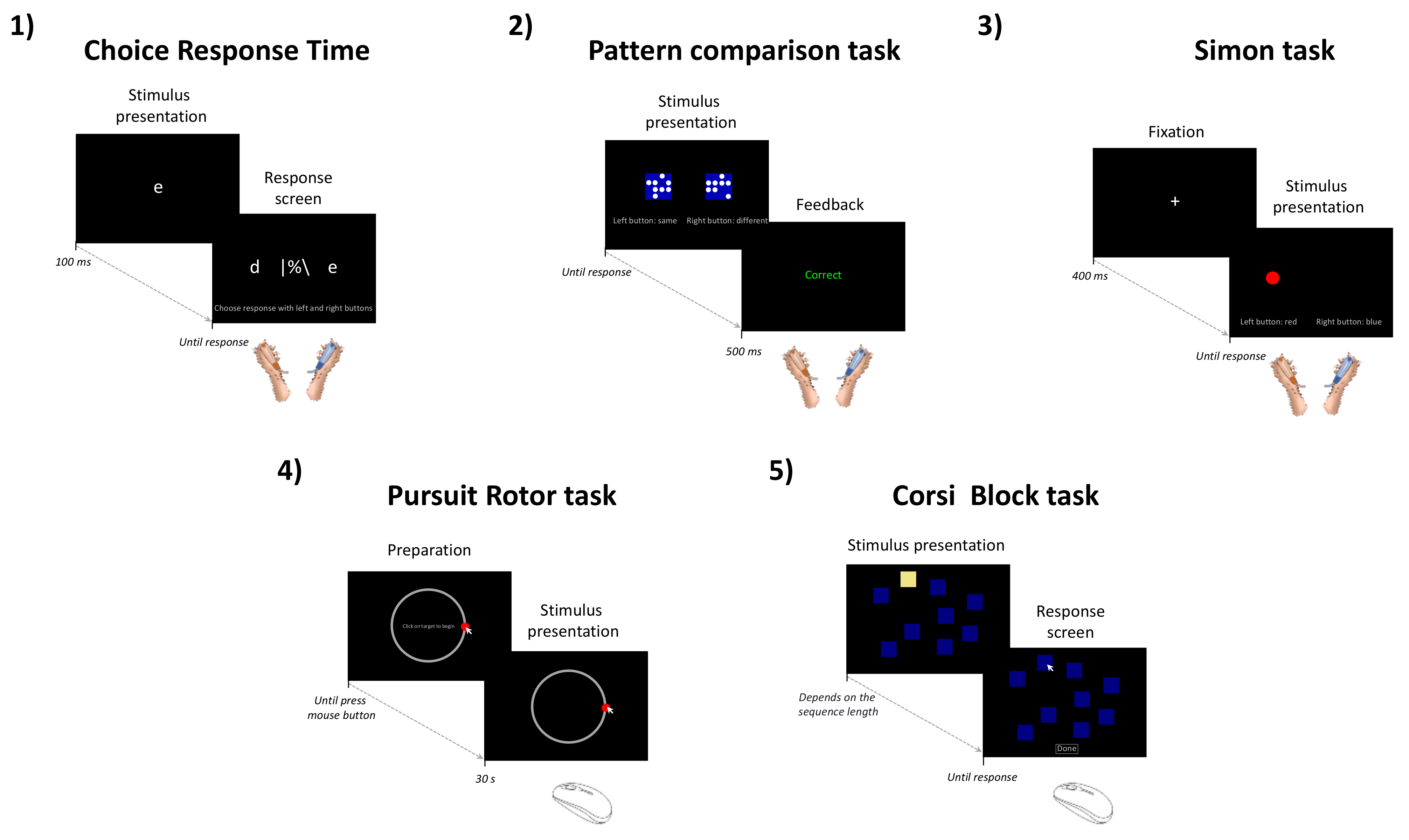
Cognitive Tasks
- Choice Response Time (CRT)
- 2.
- Pattern Comparison Task (PC)
- 3.
- Simon Task
- 4.
- Pursuit Rotor Task
- 5.
- Corsi Block-Tapping Task
2.2.3. Data Analysis
- The percentage of time-on-target and the mean deviation of the mouse cursor from the target (in pixels) for the pursuit rotor task;
- The block span (i.e., the longest length at which at least one pattern was correctly recalled) and the total score (i.e., the span × the number of trials total that were correctly recalled) for the Corsi block-tapping task.
3. Results
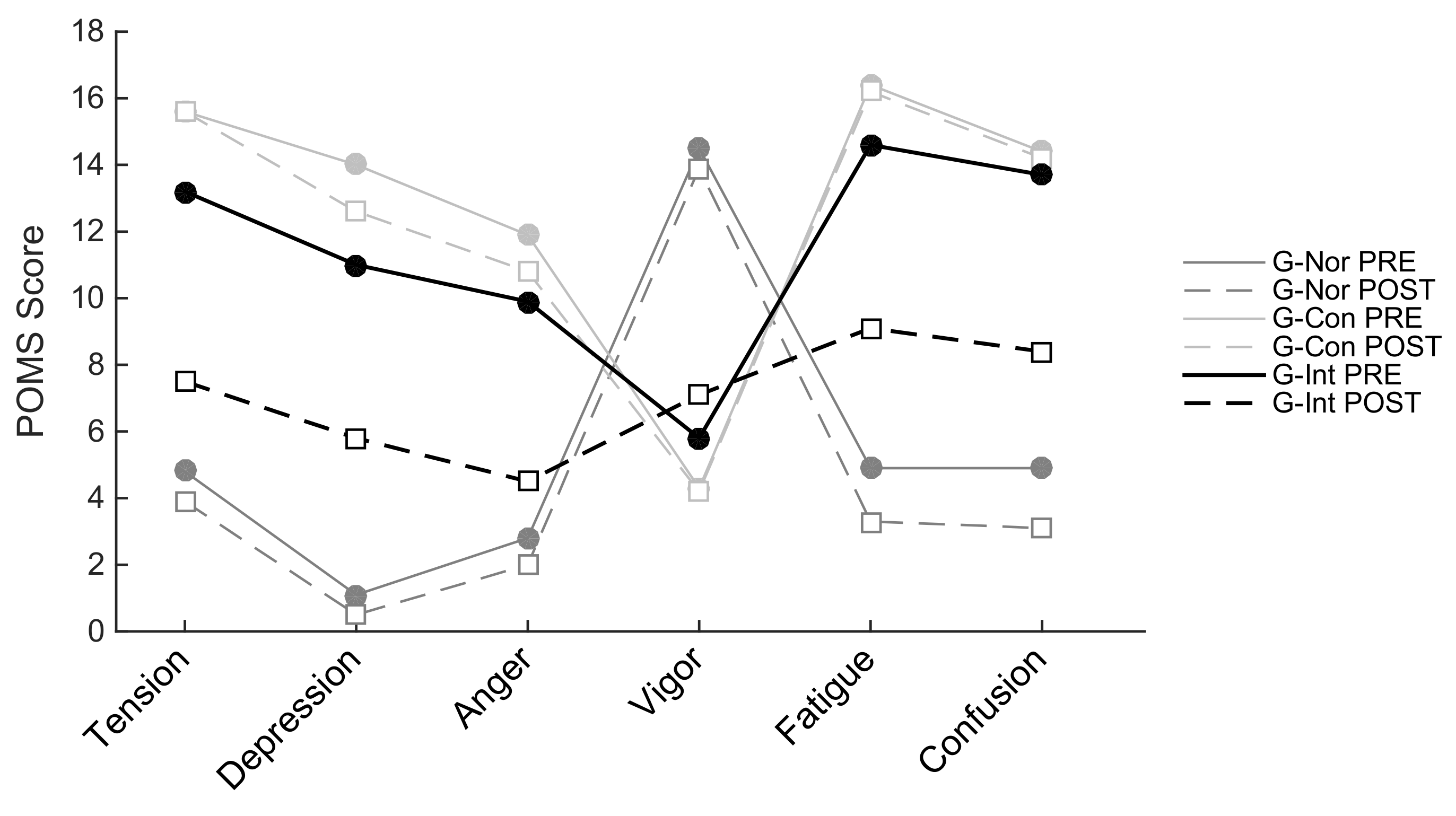
3.1. Self-Report Data
3.2. Cognitive Tasks
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Carfì, A.; Bernabei, R.; Landi, F. Persistent Symptoms in Patients after Acute COVID-19. JAMA 2020, 324, 603–605. [Google Scholar] [CrossRef] [PubMed]
- Nalbandian, A.; Sehgal, K.; Gupta, A.; Madhavan, M.V.; McGroder, C.; Stevens, J.S.; Cook, J.R.; Nordvig, A.S.; Shalev, D.; Sehrawat, T.S.; et al. Post-acute COVID-19 syndrome. Nat. Med. 2021, 27, 601–615. [Google Scholar] [CrossRef]
- Davis, H.E.; Assaf, G.S.; McCorkell, L.; Wei, H.; Low, R.J.; Re’Em, Y.; Redfield, S.; Austin, J.P.; Akrami, A. Characterizing long COVID in an international cohort: 7 months of symptoms and their impact. Eclinicalmedicine 2021, 38, 101019. [Google Scholar] [CrossRef]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-month consequences of COVID-19 in patients discharged from hospital: A cohort study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef] [PubMed]
- Tenforde, M.W.; Kim, S.S.; Lindsell, C.J.; Billig Rose, E.; Shapiro, N.I.; Files, D.C.; Gibbs, K.W.; Erickson, H.L.; Steingrub, J.S.; Smithline, H.A.; et al. Symptom Duration and Risk Factors for Delayed Return to Usual Health among Outpatients with COVID-19 in a Multistate Health Care Systems Network—United. MMWR Morb. Mortal Wkly. Rep. 2020, 69, 993–998. [Google Scholar] [CrossRef] [PubMed]
- Ellul, M.A.; Benjamin, L.; Singh, B.; Lant, S.; Michael, B.D.; Easton, A.; Kneen, R.; Defres, S.; Sejvar, J.; Solomon, T. Neurological associations of COVID-19. Lancet Neurol. 2020, 19, 767–783. [Google Scholar] [CrossRef] [PubMed]
- Paterson, R.W.; Brown, R.L.; Benjamin, L.; Nortley, R.; Wiethoff, S.; Bharucha, T.; Jayaseelan, D.L.; Kumar, G.; Raftopoulos, R.E.; Zambreanu, L.; et al. The emerging spectrum of COVID-19 neurology: Clinical, radiological and laboratory findings. Brain 2020, 143, 3104–3120. [Google Scholar] [CrossRef] [PubMed]
- Helms, J.; Kremer, S.; Merdji, H.; Clere-Jehl, R.; Schenck, M.; Kummerlen, C.; Collange, O.; Boulay, C.; Fafi-Kremer, S.; Ohana, M.; et al. Neurologic Features in Severe SARS-CoV-2 Infection. N. Engl. J. Med. 2020, 382, 2268–2270. [Google Scholar] [CrossRef]
- Toscano, G.; Palmerini, F.; Ravaglia, S.; Ruiz, L.; Invernizzi, P.; Cuzzoni, M.G.; Franciotta, D.; Baldanti, F.; Daturi, R.; Postorino, P.; et al. Guillain–Barré Syndrome Associated with SARS-CoV-2. N. Engl. J. Med. 2020, 382, 2574–2576. [Google Scholar] [CrossRef]
- Ferrier, L.; Ski, C.F.; O’Brien, C.; Jenkins, Z.; Thompson, D.R.; Moore, G.; Ward, G.; Castle, D.J. Bridging the gap between diabetes care and mental health: Perspectives of the Mental health IN DiabeteS Optimal Health Program (MINDS OHP). BMC Endocr. Disord. 2021, 21, 96. [Google Scholar] [CrossRef]
- Creswell, J.D. Mindfulness Interventions. Annu. Rev. Psychol. 2017, 68, 491–516. [Google Scholar] [CrossRef] [PubMed]
- Hausswirth, C.; Nesi, X.; Dubois, A.; Duforez, F.; Rougier, Y.; Slattery, K. Four Weeks of a Neuro-Meditation Program Improves Sleep Quality and Reduces Hypertension in Nursing Staff during the COVID-19 Pandemic: A Parallel Randomized Controlled Trial. Front. Psychol. 2022, 13. [Google Scholar] [CrossRef] [PubMed]
- Stern, A.F. The Hospital Anxiety and Depression Scale. Occup. Med. 2014, 64, 393–394. [Google Scholar] [CrossRef] [PubMed]
- Chalder, T.; Berelowitz, G.; Pawlikowska, T.; Watts, L.; Wessely, S.; Wright, D.; Wallace, E.P. Development of a fatigue scale. J. Psychosom. Res. 1993, 37, 147–153. [Google Scholar] [CrossRef]
- Klimm, H.D.; Dreyfus, J.F.; Delmotte, M. Zopiclone versus Nitrazepam: A Double-Blind Comparative Study of Efficacy and Tolerance in Elderly Patients with Chronic Insomnia. Sleep 1987, 10, 73–78. [Google Scholar] [CrossRef]
- Cheron, G.; Ristori, D.; Petieau, M.; Simar, C.; Zarka, D.; Cebolla, A.-M. Effects of Pulsed-Wave Chromotherapy and Guided Relaxation on the Theta-Alpha Oscillation during Arrest Reaction. Front. Psychol. 2022, 13. [Google Scholar] [CrossRef]
- Krigolson, O.E.; Williams, C.C.; Norton, A.; Hassall, C.D.; Colino, F.L. Choosing MUSE: Validation of a Low-Cost, Portable EEG System for ERP Research. Front. Neurosci. 2017, 11, 109. [Google Scholar] [CrossRef]
- Spiegel, R. Sleep and sleepiness in advanced age. Adv. Sleep Res. 1981, 272, 23–37. [Google Scholar]
- Grove, J.; Prapavessis, H. Preliminary evidence for the reliability and validity of an abbreviated Profile of Mood States. Int. J. Sport Psychol. 1992, 23, 93–109. [Google Scholar]
- Mahler, D.A.; Wells, C.K. Evaluation of Clinical Methods for Rating Dyspnea. Chest 1988, 93, 580–586. [Google Scholar] [CrossRef]
- Hawker, G.A.; Mian, S.; Kendzerska, T.; French, M. Measures of adult pain: Visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP). Arthr. Care Res. 2011, 63, S240–S252. [Google Scholar] [CrossRef]
- Logan, G.D.; Cowan, W.B.; Davis, K.A. On the ability to inhibit simple and choice reaction time responses: A model and a method. J. Exp. Psychol. Hum. Percept. Perform. 1984, 10, 276–291. [Google Scholar] [CrossRef] [PubMed]
- Perez, W.A.; Masline, P.J.; Ramsey, E.G.; Urban, K.E. Unified Tri-Services Cognitive Performance Assessment Battery: Review and methodology. DTIC Doc. 1987, 1, 164–183. [Google Scholar] [CrossRef]
- Yamaguchi, M.; Proctor, R.W. Multidimensional vector model of stimulus–response compatibility. Psychol. Rev. 2012, 119, 272–303. [Google Scholar] [CrossRef] [PubMed]
- Piper, B.J. Age, handedness, and sex contribute to fine motor behavior in children. J. Neurosci. Methods 2011, 195, 88–91. [Google Scholar] [CrossRef]
- Corsi, P.M. Human Memory and the Medial Temporal Region of the Brain. Ph.D. Dissertation, McGill University, Montreal, QC, Canada, 1972; p. 891B. [Google Scholar]
- Kessels, R.P.C.; Van Zandvoort, M.J.E.; Postma, A.; Kappelle, L.J.; de Haan, E. The Corsi Block-Tapping Task: Standardization and Normative Data. Appl. Neuropsychol. 2000, 7, 252–258. [Google Scholar] [CrossRef] [PubMed]
- Schmit, C.; Davranche, K.; Easthope, C.S.; Colson, S.S.; Brisswalter, J.; Radel, R. Pushing to the limits: The dynamics of cognitive control during exhausting exercise. Neuropsychologia 2015, 68, 71–81. [Google Scholar] [CrossRef]
- Bakeman, R. Recommended effect size statistics for repeated measures designs. Behav. Res. Methods 2005, 37, 379–384. [Google Scholar] [CrossRef]
- Cohen, J. The effect size. Stat. Power Anal. Behav. Sci. 1988, 2, 77–83. [Google Scholar]
- Morgan, W.P.; Brown, D.R.; Raglin, J.S.; O’Connor, P.J.; A Ellickson, K. Psychological monitoring of overtraining and staleness. Br. J. Sports Med. 1987, 21, 107–114. [Google Scholar] [CrossRef]
- Duarte, D.F.B.; Libório, J.R.; Cavalcante, G.M.E.; de Aquino, T.L.; Bezerra, L.D.C.; Martin, A.L.D.A.R.; de Lacerda, J.V.R.; Friary, V.; Paula, J.D.A.D. The effects of mindfulness-based interventions in COVID-19 times: A systematic review. J. Hum. Growth Dev. 2022, 32, 315–326. [Google Scholar] [CrossRef]
- Witarto, B.S.; Visuddho, V.; Witarto, A.P.; Bestari, D.; Sawitri, B.; Melapi, T.A.S.; Wungu, C.D.K. Effectiveness of online mindfulness-based interventions in improving mental health during the COVID-19 pandemic: A systematic review and meta-analysis of randomized controlled trials. PLoS ONE 2022, 17, e0274177. [Google Scholar] [CrossRef] [PubMed]
- Jensen, M.P.; Chen, C.; Brugger, A.M. Interpretation of visual analog scale ratings and change scores: A reanalysis of two clinical trials of postoperative pain. J. Pain 2003, 4, 407–414. [Google Scholar] [CrossRef]
- Carter, S.J.; Baranauskas, M.N.; Raglin, J.S.; Pescosolido, B.A.; Perry, B.L. Functional Status, Mood State, and Physical Activity among Women with Post-Acute COVID-19 Syndrome. Int. J. Public Health 2022, 67. [Google Scholar] [CrossRef] [PubMed]
- Townsend, L.; Dyer, A.H.; Jones, K.; Dunne, J.; Mooney, A.; Gaffney, F.; O’Connor, L.; Leavy, D.; O’Brien, K.; Dowds, J.; et al. Persistent fatigue following SARS-CoV-2 infection is common and independent of severity of initial infection. PLoS ONE 2020, 15, e0240784. [Google Scholar] [CrossRef] [PubMed]
- Stavem, K.; Ghanima, W.; Olsen, M.K.; Gilboe, H.M.; Einvik, G. Persistent symptoms 1.5–6 months after COVID-19 in non-hospitalised subjects: A population-based cohort study. Thorax 2020, 76, 405–407. [Google Scholar] [CrossRef]
- Sudre, C.H.; Murray, B.; Varsavsky, T.; Graham, M.S.; Penfold, R.S.; Bowyer, R.C.; Pujol, J.C.; Klaser, K.; Antonelli, M.; Canas, L.S.; et al. Attributes and predictors of long COVID. Nat. Med. 2021, 27, 626–631. [Google Scholar] [CrossRef]
- Pelà, G.; Goldoni, M.; Solinas, E.; Cavalli, C.; Tagliaferri, S.; Ranzieri, S.; Frizzelli, A.; Marchi, L.; Mori, P.A.; Majori, M.; et al. Sex-Related Differences in Long-COVID-19 Syndrome. J. Women’s Health 2022, 31, 620–630. [Google Scholar] [CrossRef]
- Shanbehzadeh, S.; Tavahomi, M.; Zanjari, N.; Ebrahimi-Takamjani, I.; Amiri-Arimi, S. Physical and mental health complications post-COVID-19: Scoping review. J. Psychosom. Res. 2021, 147, 110525. [Google Scholar] [CrossRef]
- Bliddal, S.; Banasik, K.; Pedersen, O.B.; Nissen, J.; Cantwell, L.; Schwinn, M.; Tulstrup, M.; Westergaard, D.; Ullum, H.; Brunak, S.; et al. Acute and persistent symptoms in non-hospitalized PCR-confirmed COVID-19 patients. Sci. Rep. 2021, 11, 13153. [Google Scholar] [CrossRef]
- Cirulli, E.T.; Barrett, K.M.S.; Riffle, S.; Bolze, A.; Neveux, I.; Dabe, S. Long-term COVID-19 symptoms in a large unselected population. MedRxiv 2020. [Google Scholar] [CrossRef]
- Ziauddeen, N.; Gurdasani, D.; O’Hara, M.E.; Hastie, C.; Roderick, P.; Yao, G.; Alwan, N.A. P108 Characteristics of long COVID: Findings from a social media survey. J. Epidemiol. Commun. Health 2021, 75, A90. [Google Scholar] [CrossRef]
- Douaud, G.; Lee, S.; Alfaro-Almagro, F.; Arthofer, C.; Wang, C.; McCarthy, P.; Lange, F.; Andersson, J.L.R.; Griffanti, L.; Duff, E.; et al. SARS-CoV-2 is associated with changes in brain structure in UK Biobank. Nature 2022, 604, 697–707. [Google Scholar] [CrossRef]
- Hampshire, A.; Trender, W.; Chamberlain, S.R.; Jolly, A.E.; Grant, J.E.; Patrick, F.; Mazibuko, N.; Williams, S.C.; Barnby, J.M.; Hellyer, P.; et al. Cognitive deficits in people who have recovered from COVID-19. Eclinicalmedicine 2021, 39, 101044. [Google Scholar] [CrossRef]
- Botvinick, M.M.; Braver, T.S.; Barch, D.M.; Carter, C.S.; Cohen, J.D. Conflict monitoring and cognitive control. Psychol. Rev. 2001, 108, 624–652. [Google Scholar] [CrossRef] [PubMed]
- Graham, E.L.; Clark, J.R.; Orban, Z.S.; Lim, P.H.; Szymanski, A.L.; Taylor, C.; DiBiase, R.M.; Jia, D.T.; Balabanov, R.; Ho, S.U.; et al. Persistent neurologic symptoms and cognitive dysfunction in non-hospitalized COVID-19 “long haulers”. Ann. Clin. Transl. Neurol. 2021, 8, 1073–1085. [Google Scholar] [CrossRef]
- Schmit, C.; Brisswalter, J. Executive functioning during prolonged exercise: A fatigue-based neurocognitive perspective. Int. Rev. Sport Exerc. Psychol. 2018, 13, 21–39. [Google Scholar] [CrossRef]
- Dettmers, C.; Fink, G.R.; Lemon, R.N.; Stephan, K.M.; Passingham, R.E.; Silbersweig, D.; Holmes, A.; Ridding, M.C.; Brooks, D.; Frackowiak, R. Relation between cerebral activity and force in the motor areas of the human brain. J. Neurophysiol. 1995, 74, 802–815. [Google Scholar] [CrossRef]
- Alemanno, F.; Houdayer, E.; Parma, A.; Spina, A.; Del Forno, A.; Scatolini, A.; Angelone, S.; Brugliera, L.; Tettamanti, A.; Beretta, L.; et al. COVID-19 cognitive deficits after respiratory assistance in the subacute phase: A COVID-rehabilitation unit experience. PLoS ONE 2021, 16, e0246590. [Google Scholar] [CrossRef]
- Muraven, M.; Baumeister, R.F. Self-regulation and depletion of limited resources: Does self-control resemble a muscle? Psychol. Bull. 2000, 126, 247–259. [Google Scholar] [CrossRef]
- Guo, P.; Ballesteros, A.B.; Yeung, S.P.; Liu, R.; Saha, A.; Curtis, L.; Kaser, M.; Haggard, M.P.; Cheke, L.G. COVCOG 2: Cognitive and Memory Deficits in Long COVID: A Second Publication from the COVID and Cognition Study. Front. Aging Neurosci. 2022, 14. [Google Scholar] [CrossRef] [PubMed]
- Mrazek, A.J.; Mrazek, M.D.; Cherolini, C.M.; Cloughesy, J.N.; Cynman, D.J.; Gougis, L.J.; Landry, A.P.; Reese, J.V.; Schooler, J.W. The future of mindfulness training is digital, and the future is now. Curr. Opin. Psychol. 2018, 28, 81–86. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Intervention Group G-Int (n = 17) | Control Group G-Con (n = 17) | Normative Control G-Nor (n = 15) | |
|---|---|---|---|
| Demographic characteristics | |||
| Age at the baseline visit (in years) | 47.1 ± 8.3 | 48.7 ± 10.4 | 45.9 ± 11.8 |
| Sex ratio (M/F) | 0.3 (4/13) | 0.4 (5/12) | 0.5 (5/10) |
| ICU admission | 2/17 | 1/17 | 0/15 |
| Vascular factors | |||
| Systolic blood pressure, mm Hg | 123.8 ± 15.4 | 122.9 ± 11.8 | 124.6 ± 13.7 |
| Diastolic blood pressure, mm Hg | 75.8 ± 10.9 | 78 ± 9.7 | 73.3 ± 9.8 |
| Heart rate at rest | 72.6 ± 11.3 | 74.5 ± 16.1 | 67.5 ± 14.3 |
| Lifestyle factors | |||
| Severity of dyspnea (mMRC) | 1.5 ± 0.9 | 1.4 ± 0.7 | 0.2 ± 0.4 |
| Anxiety (HADS) | 10.8 ± 3.5 | 12.9 ± 3.2 | 4.0 ± 2.4 |
| Depression (HADS) | 11.9 ± 2.7 | 12.5 ± 4.3 | 2.0 ± 1.3 |
| Physical fatigue (CFQ) | 17.8 ± 2.2 | 18.4 ± 2.4 | 6.8 ± 1.4 |
| Mental fatigue (CFQ) | 10.4 ± 1.6 | 10.9 ± 1.5 | 4 ± 0.4 |
| Sleep quality (SSQ) | 15.1 ± 3.8 | 14.0 ± 3.8 | 20.5 ± 3.1 |
| Total Mood Disturbance (POMS-abbreviated) | 45.5 ± 22.8 | 58.9 ± 22 | −14.2 ± 11.3 |
| Questionnaire | Dimensions (Score Min–Max) | Group | Baseline | Post | Diff Base-Post |
|---|---|---|---|---|---|
| CFQ 11 | Physical fatigue (0–21) ††† | G-Nor | 6.8 ± 1.4 | 7.2 ± 1.1 | +0.4 |
| G-Con | 18.4 ± 2.4 ∆∆∆ | 17.8 ± 2.2 ∆∆∆ | −0.6 | ||
| G-Int | 17.8 ± 2.2 ∆∆∆ | 4.8 ± 4.1 °°°*** | −13 | ||
| Mental fatigue (0–12) ††† | G-Nor | 4 ± 0.4 | 4.3 ± 0.7 | +0.3 | |
| G-Con | 10.9 ± 1.5 ∆∆∆ | 10.6 ± 1.7 ∆∆∆ | −0.3 | ||
| G-Int | 10.4 ± 1.6 ∆∆∆ | 2.7 ± 3.1 °°°*** | −7.7 | ||
| HADS | Anxiety (0–21) † | G-Nor | 4.0 ± 2.4 | 3.3 ± 1.2 | −0.7 |
| G-Con | 12.9 ± 3.2 ∆∆∆ | 11.4 ± 3.5 ∆∆∆ | −1.5 | ||
| G-Int | 10.8 ± 3.5 ∆∆∆ | 7.2 ± 3.0 ∆∆°°*** | −3.6 | ||
| Depression (0–21) ††† | G-Nor | 2.0 ± 1.3 | 2.7 ± 1.6 | +0.7 | |
| G-Con | 12.5 ± 4.3 ∆∆∆ | 11.9 ± 4.6 ∆∆∆ | −0.6 | ||
| G-Int | 11.9 ± 2.7 ∆∆∆ | 6.7 ± 3.6 ∆°°°*** | −5.2 | ||
| mMRC | Dyspnea (0–4) | G-Nor | 0.2 ± 0.4 | 0.2 ± 0.4 | 0 |
| G-Con | 1.4 ± 0.7 ∆∆∆ | 1.2 ± 0.7 ∆∆∆ | −0.2 | ||
| G-Int | 1.5 ± 0.9 ∆∆∆ | 1.1 ± 0.7∆∆* | −0.4 | ||
| VAS Pain | Muscle and Joint (0–10) † | G-Nor | 1.7 ± 1.5 | 1.0 ± 1.1 | −0.7 |
| G-Con | 7.1 ± 1.4 ∆∆∆ | 6.8 ± 1.4 ∆∆∆ | −0.3 | ||
| G-Int | 6.4 ± 1.6 ∆∆∆ | 4.6 ± 2.2 ∆∆∆°°°** | −1.8 | ||
| Headaches (0–10) †† | G-Nor | 0.7 ± 1.0 | 0.3 ± 0.7 | −0.4 | |
| G-Con | 7.2 ± 1.7 ∆∆∆ | 6.5 ± 2.2 ∆∆∆ | −0.7 | ||
| G-Int | 5.3 ± 2.6 ∆∆∆ | 2.8 ± 1.7 ∆∆°°°*** | −2.5 | ||
| SSQ | Sleep quality (0–30) | G-Nor | 20.5 ± 3.1 | 22.1 ± 2.9 | +1.6 |
| G-Con | 14.0 ± 3.8 ∆∆∆ | 16.0 ± 3.1 ∆∆∆ | +2.0 | ||
| G-Int | 15.1 ± 3.8 ∆∆∆ | 18.5 ± 4.5 * | +3.4 | ||
| POMS | Tension-Anxiety (0–24) ††† | G-Nor | 4.8 ± 1.8 | 3.9 ± 2.6 | −0.9 |
| G-Con | 15.6 ± 4.1 ∆∆∆ | 15.6 ± 6.2 ∆∆∆ | 0 | ||
| G-Int | 13.2 ± 5.2 ∆∆∆ | 7.5 ± 4.8 °°°*** | −5.7 | ||
| Anger-Hostility (0–24) ††† | G-Nor | 2.8 ± 1.7 | 2.0 ± 1.7 | −0.8 | |
| G-Con | 11.9 ± 3.4 ∆∆∆ | 10.8 ± 6.1 ∆∆∆ | −1.1 | ||
| G-Int | 9.9 ± 5.9 ∆∆∆ | 4.5 ± 4.2 °°°*** | −5.4 | ||
| Fatigue-Inertia (0–20) ††† | G-Nor | 4.9 ± 3.5 | 3.3 ± 2.3 | −1.6 | |
| G-Con | 16.4 ± 3.3 ∆∆∆ | 16.2 ± 3.4 ∆∆∆ | −0.2 | ||
| G-Int | 14.6 ± 2.8 ∆∆∆ | 9.1 ± 3.6 ∆∆∆°°°*** | −5.5 | ||
| Depression-Dejection (0–28) †† | G-Nor | 1.1 ± 1.5 | 0.5 ± 0.5 | −0.6 | |
| G-Con | 14.0 ± 7.1 ∆∆∆ | 12.6 ± 8.2 ∆∆∆ | −1.4 | ||
| G-Int | 11.0 ± 6.4 ∆∆∆ | 5.8 ± 4.8 °°*** | −5.2 | ||
| Esteem-related affect (0–24) ††† | G-Nor | 18.4 ± 1.8 | 16.9 ± 2.8 | −1.5 | |
| G-Con | 9.0 ± 3.3 ∆∆∆ | 9.5 ± 3.6 ∆∆∆ | +0.5 | ||
| G-Int | 11.1 ± 3.4 ∆∆∆ | 13.9 ± 3.2 °°** | +2.8 | ||
| Vigor-Activity (0–20) | G-Nor | 14.5 ± 3.7 | 13.9 ± 3.5 | −0.6 | |
| G-Con | 4.3 ± 3.3 ∆∆∆ | 4.2 ± 2.3 ∆∆∆ | −0.1 | ||
| G-Int | 5.8 ± 1.8 ∆∆∆ | 7.1 ± 4.1 ∆∆∆ | +1.3 | ||
| Confusion-Bewilderment (0–24) ††† | G-Nor | 4.9 ± 2.6 | 3.1 ± 2.2 | −1.8 | |
| G-Con | 14.4 ± 3.1 ∆∆∆ | 14.2 ± 4.0 ∆∆∆ | −0.2 | ||
| G-Int | 13.7 ± 3.4 ∆∆∆ | 8.4 ± 3.2 ∆∆∆°°°*** | −5.3 | ||
| Total Mood Disturbance (−44–76) ††† | G-Nor | −14.2 ± 11.3 | −17.5 ± 14.0 | −3.3 | |
| G-Con | 58.9 ± 22.0 ∆∆∆ | 55.6 ± 30.3 ∆∆∆ | −3.3 | ||
| G-Int | 45.5 ± 22.8 ∆∆∆ | 14.2 ± 21.7 ∆∆°°°*** | −31.3 |
| Questionnaire | Subscale | Baseline | Post |
|---|---|---|---|
| CFQ 11 | Physical fatigue | 0.94 | 0.85 |
| Mental fatigue | 0.93 | 0.90 | |
| HADS | Anxiety | 0.88 | 0.81 |
| Depression | 0.86 | 0.82 | |
| POMS | Tension | 0.91 | 0.89 |
| Anger | 0.92 | 0.88 | |
| Fatigue-Inertia | 0.94 | 0.92 | |
| Depression | 0.93 | 0.88 | |
| Esteem-related affect | 0.84 | 0.73 | |
| Vigor | 0.93 | 0.89 | |
| Confusion-Bewilderment | 0.86 | 0.79 | |
| SSQ | 0.76 | 0.73 |
| Cognitive Task | Parameter | Group | Baseline | Post 1 | Change Post1-Base (%) | Post 2 | Change Post2-Post1 (%) |
|---|---|---|---|---|---|---|---|
| CRT | Accuracy | G-Nor | 0.98 ± 0.01 | 0.97 ± 0.03 | −1.0 | ||
| G-Con | 0.95 ± 0.08 | 0.93 ± 0.1 | −2.1 | ||||
| G-Int | 0.96 ± 0.05 | 0.97 ± 0.05 | +1.0 | 0.97 ± 0.04 | 0 | ||
| RT (ms) † | G-Nor | 491 ± 61 | 495 ± 67 | +0.8 | |||
| G-Con | 587 ± 136 | 551 ± 121 | −6.1 | ||||
| G-Int | 593 ± 121 | 535 ± 83 ** | −9.8 | 521 ± 86 *** | −2.6 | ||
| Pattern comparison | Accuracy CO †† | G-Nor | 0.97 ± 0.02 | 0.95 ± 0.04 * | −2.1 | ||
| G-Con | 0.98 ± 0.03 | 0.97 ± 0.03 | −1.0 | ||||
| G-Int | 0.98 ± 0.04 | 0.99 ± 0.03 | +1.0 | 0.97 ± 0.04 | −2.0 | ||
| RT CO (ms) | G-Nor | 975 ± 121 | 949 ± 145 | −2.7 | |||
| G-Con | 1371 ± 467 ∆∆ | 1353 ± 388 ∆∆ | −1.3 | ||||
| G-Int | 1277 ± 393 p=0.06 | 1198 ± 331 | −6.2 | 1128 ± 281 | −5.8 | ||
| Accuracy IN | G-Nor | 0.94 ± 0.03 | 0.94 ± 0.03 | 0 | |||
| G-Con | 0.97 ± 0.03 | 0.96 ± 0.03 | −1.0 | ||||
| G-Int | 0.97 ± 0.03 ∆∆ | 0.98 ± 0.02 ∆∆ | +1.0 | 0.96 ± 0.03 | −2.0 | ||
| RT IN (ms) † | G-Nor | 1006 ± 130 | 974 ± 164 | −3.2 | |||
| G-Con | 1277 ± 378 | 1275 ± 391 | −0.2 | ||||
| G-Int | 1244 ± 315 | 1156 ± 243 | −7.1 | 1079 ± 213 *** | −6.7 | ||
| Simon | Accuracy CO | G-Nor | 0.98 ± 0.01 | 0.99 ± 0.01 | +1.0 | ||
| G-Con | 1.0 ± 0.01 ∆§ | 1.0 ± 0.01 ∆§ | 0 | ||||
| G-Int | 0.99 ± 0.01 | 0.99 ± 0.02 | 0 | 0.99 ± 0.01 | 0 | ||
| RT CON (ms) | G-Nor | 448 ± 59 | 449 ± 64 | +0.2 | |||
| G-Con | 515 ± 128 | 509 ± 131 | −1.2 | ||||
| G-Int | 511 ± 125 | 473 ± 88 | −7.4 | 477 ± 134 | +0.8 | ||
| Accuracy IN | G-Nor | 0.95 ± 0.03 | 0.95 ± 0.04 | 0 | |||
| G-Con | 0.97 ± 0.03 | 0.96 ± 0.04 | −1.0 | ||||
| G-Int | 0.97 ± 0.03 | 0.97 ± 0.02 | 0 | 0.97 ± 0.03 | 0 | ||
| RT IN (ms) | G-Nor | 479 ± 72 | 459 ± 66 | −4.2 | |||
| G-Con | 532 ± 100 | 525 ± 99 | −1.3 | ||||
| G-Int | 539 ± 123 | 507 ± 86 p=0.13 | −5.9 | 494 ± 134 ** | −2.6 | ||
| Psychomotor task | Time-on-target (%) † | G-Nor | 92.8 ± 1.8 | 90.3 ± 5.0 | −2.7 | ||
| G-Con | 92.6 ± 2.6 | 93.9 ± 2.2∆ | +1.4 | ||||
| G-Int | 93.1 ± 2.9 | 93.4 ± 2.3 | +0.3 | 93.3 ± 3.3 | −0.1 | ||
| Mean deviation | G-Nor | 14.7 ± 1.5 | 14.5 ± 1.7 | −1.4 | |||
| G-Con | 18.4 ± 4.7 ∆ | 18.3 ± 4.8 ∆ | −0.5 | ||||
| G-Int | 17.2 ± 2.3 | 16.6 ± 2.5 | −3.5 | 16.3 ± 2.3 | −1.8 | ||
| Corsi | Total score ††† | G-Nor | 53.1 ± 8.6 | 65.0 ± 16.2 *** | +22.4 | ||
| G-Con | 44.5 ± 10.7 ∆∆∆ | 43.3 ± 12.8 ∆∆ | −2.7 | ||||
| G-Int | 43.5 ± 10.4 ∆∆∆ | 41.4 ± 9.9 ∆∆ | −4.8 | 43.6 ± 10.4 ∆∆∆ | +5.3 | ||
| Longest sequence † | G-Nor | 7.8 ± 0.7 | 8.2 ± 0.9 p=0.09 | +5.1 | |||
| G-Con | 6.9 ± 1.3 ∆∆ | 7.0 ± 1.0 ∆∆ | +1.4 | ||||
| G-Int | 7.1 ± 0.9 ∆∆ | 6.9 ± 0.8 ∆∆ | −2.8 | 7.0 ± 0.7 ∆∆ | +1.4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hausswirth, C.; Schmit, C.; Rougier, Y.; Coste, A. Positive Impacts of a Four-Week Neuro-Meditation Program on Cognitive Function in Post-Acute Sequelae of COVID-19 Patients: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2023, 20, 1361. https://doi.org/10.3390/ijerph20021361
Hausswirth C, Schmit C, Rougier Y, Coste A. Positive Impacts of a Four-Week Neuro-Meditation Program on Cognitive Function in Post-Acute Sequelae of COVID-19 Patients: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2023; 20(2):1361. https://doi.org/10.3390/ijerph20021361
Chicago/Turabian StyleHausswirth, Christophe, Cyril Schmit, Yann Rougier, and Alexandre Coste. 2023. "Positive Impacts of a Four-Week Neuro-Meditation Program on Cognitive Function in Post-Acute Sequelae of COVID-19 Patients: A Randomized Controlled Trial" International Journal of Environmental Research and Public Health 20, no. 2: 1361. https://doi.org/10.3390/ijerph20021361
APA StyleHausswirth, C., Schmit, C., Rougier, Y., & Coste, A. (2023). Positive Impacts of a Four-Week Neuro-Meditation Program on Cognitive Function in Post-Acute Sequelae of COVID-19 Patients: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health, 20(2), 1361. https://doi.org/10.3390/ijerph20021361