
Validation of the Glover–Nilsson Smoking Behavioral Questionnaire (GN-SBQ) to Evaluate Nicotine Dependence in Spanish Clinical Settings


Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measures
2.2.1. Psychological Symptoms of Tobacco Addiction
2.2.2. Variables Related to Psychological Symptoms of Tobacco Addiction
Sociodemographic and Smoking-Related Variables
Tobacco Addiction
Nicotine Withdrawal Symptoms
Exhaled Carbon Monoxide
Alcohol Use
2.3. Procedure
2.4. Data Analysis
3. Results
3.1. Descriptive Statistics and Reliability
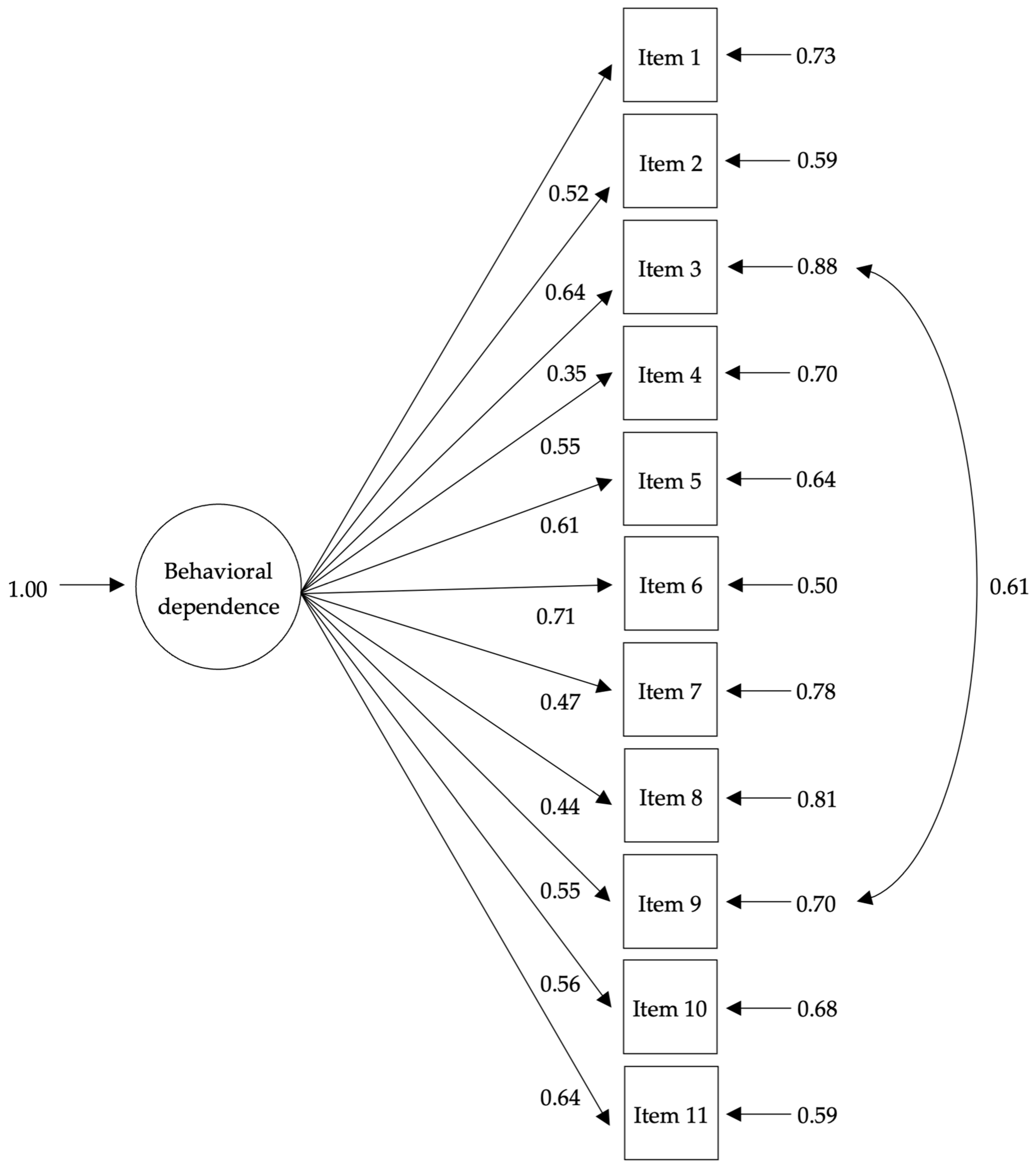
3.2. Factorial Validity
3.3. Convergent and Discriminant Validity
3.4. Mean Differences between GN-SBQ Levels of Addiction
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Reitsma, M.B.; Kendrick, P.J.; Ababneh, E.; Abbafati, C.; Abbasi-Kangevari, M.; Abdoli, A.; Abedi, A.; Abhilash, E.S.; Abila, D.B.; Aboyans, V.; et al. Spatial, Temporal, and Demographic Patterns in Prevalence of Smoking Tobacco Use and Attributable Disease Burden in 204 Countries and Territories, 1990–2019: A Systematic Analysis from the Global Burden of Disease Study 2019. Lancet 2021, 397, 2337–2360. [Google Scholar] [CrossRef] [PubMed]
- Peacock, A.; Leung, J.; Larney, S.; Colledge, S.; Hickman, M.; Rehm, J.; Giovino, G.A.; West, R.; Hall, W.; Griffiths, P.; et al. Global Statistics on Alcohol, Tobacco and Illicit Drug Use: 2017 Status Report. Addiction 2018, 113, 1905–1926. [Google Scholar] [CrossRef]
- Observatorio Español de las Drogas y las Adicciones. Report 2021. Alcohol, Tobacco and Illegal Drugs in Spain. Available online: https://pnsd.sanidad.gob.es/profesionales/sistemasInformacion/sistemaInformacion/pdf/2019-20_Informe_EDADES.pdf (accessed on 28 October 2022).
- World Health Organization WHO Global Report on Trends in Prevalence of Tobacco Use 2000-2025, Third Edition. Available online: https://www.who.int/publications-detail-redirect/who-global-report-on-trends-in-prevalence-of-tobacco-use-2000-2025-third-edition (accessed on 28 October 2022).
- Benowitz, N.L. Nicotine Addiction. N. Engl. J. Med. 2010, 362, 2295–2303. [Google Scholar] [CrossRef] [PubMed]
- DiFranza, J.R.; Wellman, R.J.; Savageau, J.A. Does Progression through the Stages of Physical Addiction Indicate Increasing Overall Addiction to Tobacco? Psychopharmacology 2012, 219, 815–822. [Google Scholar] [CrossRef] [PubMed]
- Rosenthal, D.G.; Weitzman, M.; Benowitz, N.L. Nicotine Addiction: Mechanisms and Consequences. Int. J. Ment. Health 2011, 40, 22–38. [Google Scholar] [CrossRef]
- White, C.M.; Hatsukami, D.K.; Donny, E.C. Reducing the Relative Value of Cigarettes: Considerations for Nicotine and Non-Nicotine Factors. Neuropharmacology 2020, 175, 108200. [Google Scholar] [CrossRef]
- Bickel, W.K.; Mellis, A.M.; Snider, S.E.; Athamneh, L.N.; Stein, J.S.; Pope, D.A. 21st Century Neurobehavioral Theories of Decision Making in Addiction: Review and Evaluation. Pharmacol. Biochem. Behav. 2018, 164, 4–21. [Google Scholar] [CrossRef]
- Russo, C.; Walicka, M.; Caponnetto, P.; Cibella, F.; Maglia, M.; Alamo, A.; Campagna, D.; Frittitta, L.; Di Mauro, M.; Caci, G.; et al. Efficacy and Safety of Varenicline for Smoking Cessation in Patients With Type 2 Diabetes. JAMA Netw. Open 2022, 5, e2217709. [Google Scholar] [CrossRef]
- Caponnetto, P.; Polosa, R. Are We Addressing Relevant Determinants of Smoking Cessation? Eur. Respir. J. 2017, 50, 1701615. [Google Scholar] [CrossRef]
- Fagerström, K.O. Measuring Degree of Physical Dependence to Tobacco Smoking with Reference to Individualization of Treatment. Addict. Behav. 1978, 3, 235–241. [Google Scholar] [CrossRef]
- Shiffman, S.; Waters, A.; Hickcox, M. The Nicotine Dependence Syndrome Scale: A Multidimensional Measure of Nicotine Dependence. Nicotine Tob. Res. 2004, 6, 327–348. [Google Scholar] [CrossRef]
- Glover, E.D.; Nilsson, F.; Westin, A.; Glover, P.N.; Laflin, M.T.; Persson, B. Developmental History of the Glover-Nilsson Smoking Behavioral Questionnaire. Am. J. Health Behav. 2005, 29, 443–455. [Google Scholar] [CrossRef]
- Rocha, V.; Guerra, M.P.; Lemos, M.S.; Glover, E.D. Validation of the Glover-Nilsson Smoking Behavioral Questionnaire for the Portuguese Population: A Psychometric Process. Am. J. Health Behav. 2014, 38, 801–806. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.-C.; Chen, H.-F.; Peng, H.-L.; Lee, L.-Y.; Chiang, T.-Y.; Chiu, H.-C. Psychometric Testing of the Chinese-Version Glover-Nilsson Smoking Behavioral Questionnaire (GN-SBQ-C) for the Identification of Nicotine Dependence in Adult Smokers in Taiwan. Int. J. Behav. Med. 2017, 24, 272–279. [Google Scholar] [CrossRef]
- Rath, J.M.; Sharma, E.; Beck, K.H. Reliability and Validity of the Glover-Nilsson Smoking Behavioral Questionnaire. Am. J. Health Behav. 2013, 37, 310–317. [Google Scholar] [CrossRef] [PubMed]
- Bully, P.; Sanchez, A.; Grandes, G.; Pombo, H.; Arietalenizbeaskoa, M.S.; Arce, V.; Martinez, C. Metric Properties of the “Prescribe Healthy Life” Screening Questionnaire to Detect Healthy Behaviors: A Cross-Sectional Pilot Study. BMC Public Health 2016, 16, 1228. [Google Scholar] [CrossRef]
- Caponnetto, P.; Cibella, F.; Mancuso, S.; Campagna, D.; Arcidiacono, G.; Polosa, R. Effect of a Nicotine-Free Inhalator as Part of a Smoking-Cessation Programme. Eur. Respir. J. 2011, 38, 1005–1011. [Google Scholar] [CrossRef]
- Garcia-Portilla, M.P.; Garcia-Alvarez, L.; Saiz, P.A.; Diaz-Mesa, E.; Galvan, G.; Sarramea, F.; Garcia-Blanco, J.; Elizagarate, E.; Bobes, J. Effectiveness of a Multi-Component Smoking Cessation Support Programme (McSCSP) for Patients with Severe Mental Disorders: Study Design. Int. J. Environ. Res. Public. Health 2014, 11, 373–389. [Google Scholar] [CrossRef]
- Garcia-Portilla, M.P.; Garcia-Alvarez, L.; Sarramea, F.; Galvan, G.; Diaz-Mesa, E.; Bobes-Bascaran, T.; Al-Halabi, S.; Elizagarate, E.; Iglesias, C.; Saiz Martínez, P.A.; et al. It Is Feasible and Effective to Help Patients with Severe Mental Disorders to Quit Smoking: An Ecological Pragmatic Clinical Trial with Transdermal Nicotine Patches and Varenicline. Schizophr. Res. 2016, 176, 272–280. [Google Scholar] [CrossRef] [PubMed]
- Maglia, M.; Caponnetto, P.; Polosa, R.; Russo, C.; Santisi, G. Impact of a Soft Tip Nicotine-Free Harmless Cigarette as Part of a Smoking Cessation Program with Psychological Support and Varenicline: An Integrated Workplace Smoking Cessation Intervention. Health Psychol. Res. 2021, 9, 24506. [Google Scholar] [CrossRef]
- Nerín, I.; Crucelaegui, A.; Novella, P.; Beamonte, A.; Sobradiel, N.; Bernal, V.; Gargallo, P. Evaluación de la dependencia psicológica mediante el test de Glover-Nilsson en el tratamiento del tabaquismo. Arch. Bronconeumol. 2005, 41, 493–498. [Google Scholar] [CrossRef] [PubMed]
- Villalbí, J.R.; Suelves, J.M.; Martínez, C.; Valverde, A.; Cabezas, C.; Fernández, E.; Villalbí, J.R.; Suelves, J.M.; Martínez, C.; Valverde, A.; et al. El Control Del Tabaquismo En España: Situación Actual y Prioridades. Rev. Esp. De Salud Publica 2019, 93, e201907044. [Google Scholar]
- DiFranza, J.R.; Savageau, J.A.; Wellman, R.J. A Comparison of the Autonomy over Tobacco Scale and the Fagerström Test for Nicotine Dependence. Addict. Behav. 2012, 37, 856–861. [Google Scholar] [CrossRef] [PubMed]
- Bucklin, M. A 5-Factor Framework for Assessing Tobacco Use Disorder. Tob. Use Insights 2021, 14, 1179173X21998355. [Google Scholar] [CrossRef] [PubMed]
- Piñeiro, B.; Lopez-Duran, A.; Fernandez del Rio, E.; Martinez, U.; Brandon, T.H.; Becona, E. Craving and Nicotine Withdrawal in a Spanish Smoking Cessation Sample. Adicciones 2014, 26, 230–237. [Google Scholar] [CrossRef]
- Ussher, M.; Kakar, G.; Hajek, P.; West, R. Dependence and Motivation to Stop Smoking as Predictors of Success of a Quit Attempt among Smokers Seeking Help to Quit. Addict. Behav. 2016, 53, 175–180. [Google Scholar] [CrossRef]
- Muñiz, J.; Fonseca-Pedrero, E. Diez pasos para la construcción de un test. Psicothema 2019, 31, 7–16. [Google Scholar] [CrossRef]
- Becoña, E.; Vázquez, F.L. The Fagerström Test for Nicotine Dependence in a Spanish Sample. Psychol. Rep. 1998, 83, 1455–1458. [Google Scholar] [CrossRef]
- Chabrol, H.; Niezborala, M.; Chastan, E.; Montastruc, J.-L.; Mullet, E. A Study of the Psychometric Properties of the Fagestrom Test for Nicotine Dependence. Addict. Behav. 2003, 28, 1441–1445. [Google Scholar] [CrossRef]
- Etter, J.-F. A Comparison of the Content-, Construct- and Predictive Validity of the Cigarette Dependence Scale and the Fagerström Test for Nicotine Dependence. Drug Alcohol Depend. 2005, 77, 259–268. [Google Scholar] [CrossRef]
- Becoña, E.; del Río, E.F.; López, A.; del Carmen Míguez, M.; Castro, J.; Nogueiras, L.; Flórez, G.; Alvarez, S.; Vázquez, D. The Short Nicotine Dependence Syndrome Scale (NDSS-S) in Spanish smokers. Psicothema 2011, 23, 126–132. [Google Scholar] [PubMed]
- Broms, U.; Madden, P.A.F.; Heath, A.C.; Pergadia, M.L.; Shiffman, S.; Kaprio, J. The Nicotine Dependence Syndrome Scale in Finnish Smokers. Drug Alcohol Depend. 2007, 89, 42–51. [Google Scholar] [CrossRef] [PubMed]
- Piper, M.E.; McCarthy, D.E.; Bolt, D.M.; Smith, S.S.; Lerman, C.; Benowitz, N.; Fiore, M.C.; Baker, T.B. Assessing Dimensions of Nicotine Dependence: An Evaluation of the Nicotine Dependence Syndrome Scale (NDSS) and the Wisconsin Inventory of Smoking Dependence Motives (WISDM). Nicotine Tob. Res. 2008, 10, 1009–1020. [Google Scholar] [CrossRef] [PubMed]
- Hughes, J.R.; Hatsukami, D. Signs and Symptoms of Tobacco Withdrawal. Arch. Gen. Psychiatry 1986, 43, 289–294. [Google Scholar] [CrossRef] [PubMed]
- Blebil, A.Q.; Sulaiman, S.A.S.; Hassali, M.A.; Dujaili, J.A.; Zin, A.M. Evaluation of the Psychometric Properties of the Malay Version of the Minnesota Nicotine Withdrawal Scale. Value Health Reg. Issues 2014, 3, 19–23. [Google Scholar] [CrossRef] [PubMed]
- Svicher, A.; Beghè, A.; Mangiaracina, G.; Cosci, F. Factor Analysis and Psychometric Properties of the Minnesota Nicotine Withdrawal Scale and the Minnesota Nicotine Withdrawal Scale-Revised: Italian Version. Eur. Addict. Res. 2017, 23, 157–162. [Google Scholar] [CrossRef]
- Toll, B.A.; O’Malley, S.S.; McKee, S.A.; Salovey, P.; Krishnan-Sarin, S. Confirmatory Factor Analysis of the Minnesota Nicotine Withdrawal Scale. Psychol. Addict. Behav. 2007, 21, 216–225. [Google Scholar] [CrossRef]
- Babaoğlu, E.; Karalezli, A.; Er, M.; Hasanoğlu, H.; Ötzuna, D. Exhaled Carbon Monoxide Is a Marker of Heavy Nicotine Dependence. Turk. J. Med. Sci. 2016, 46, 1677–1681. [Google Scholar] [CrossRef]
- Saunders, J.B.; Aasland, O.G.; Babor, T.F.; de la Fuente, J.R.; Grant, M. Development of the Alcohol Use Disorders Identification Test (AUDIT): WHO Collaborative Project on Early Detection of Persons with Harmful Alcohol Consumption-II. Addiction 1993, 88, 791–804. [Google Scholar] [CrossRef]
- Guillamón, M.C.; Solé, A.G.; Farran, J.C. Test para la identificación de transtornos por uso de alcohol (AUDIT): Traducción y validación del AUDIT al catalán y castellano. Adicciones 1999, 11, 337–347. [Google Scholar] [CrossRef]
- Rubio Valladolid, G.; Bermejo Vicedo, J.; Caballero Sánchez-Serrano, M.C.; Santo-Domingo Carrasco, J. Validation of the Alcohol Use Disorders Identification Test (AUDIT) in primary care. Rev. Clin. Esp. 1998, 198, 11–14. [Google Scholar] [PubMed]
- Rosseel, Y. Lavaan: An R Package for Structural Equation Modeling. J. Stat. Softw. 2012, 48, 1–36. [Google Scholar] [CrossRef]
- Kelley, K. Methods for the Behavioral, Educational, and Social Sciences: An R Package. Behav. Res. Methods 2007, 39, 979–984. [Google Scholar] [CrossRef]
- Kallner, A. Handbook of Formulas and Terms. In Laboratory Statistics, 2nd ed.; Kallner, A., Ed.; Elsevier: Amsterdam, The Netherlands, 2018; pp. 1–140. ISBN 978-0-12-814348-3. [Google Scholar]
- Ebel, R.; Frisbie, D. Essentials of Educational Measurement; Prentice-Hall: Englewood Cliffs, NJ, USA, 1991. [Google Scholar]
- Nunnally, J.; Jum, N.; Bernstein, I.H.; Bernstein, I. Psychometric Theory, 3rd ed.; McGraw-Hill: New York, NY, USA, 1994; ISBN 978-0-07-047849-7. [Google Scholar]
- Holgado-Tello, F.P.; Morata-Ramirez, M.Á.; García, M.I.B. Confirmatory Factor Analysis of Ordinal Variables: A Simulation Study Comparing the Main Estimation Methods. Av. En Psicol. Latinoam. 2018, 36, 601–617. [Google Scholar] [CrossRef]
- Hu, L.; Bentler, P.M. Cutoff Criteria for Fit Indexes in Covariance Structure Analysis: Conventional Criteria versus New Alternatives. Struct. Equ. Model. A Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- MacCallum, R.C.; Browne, M.W.; Sugawara, H.M. Power Analysis and Determination of Sample Size for Covariance Structure Modeling. Psychol. Methods 1996, 1, 130–149. [Google Scholar] [CrossRef]
- Marsh, H.W.; Hau, K.-T. Assessing Goodness of Fit. J. Exp. Educ. 1996, 64, 364–390. [Google Scholar] [CrossRef]
- Sörbom, D. Model Modification. Psychometrika 1989, 54, 371–384. [Google Scholar] [CrossRef]
- Whittaker, T.A. Using the Modification Index and Standardized Expected Parameter Change for Model Modification. J. Exp. Educ. 2012, 80, 26–44. [Google Scholar] [CrossRef]
- Floyd, F.J.; Widaman, K.F. Factor Analysis in the Development and Refinement of Clinical Assessment Instruments. Psychol. Assess. 1995, 7, 286–299. [Google Scholar] [CrossRef]
- Smith, R.A.; Levine, T.R.; Lachlan, K.A.; Fediuk, T.A. The High Cost of Complexity in Experimental Design and Data Analysis: Type I and Type II Error Rates in Multiway ANOVA. Hum. Commun. Res. 2002, 28, 515–530. [Google Scholar] [CrossRef]
- Kang, H. The Prevention and Handling of the Missing Data. Korean J. Anesthesiol. 2013, 64, 402–406. [Google Scholar] [CrossRef] [PubMed]
- Senyurek, V.Y.; Imtiaz, M.H.; Belsare, P.; Tiffany, S.; Sazonov, E. Smoking Detection Based on Regularity Analysis of Hand to Mouth Gestures. Biomed. Signal Process. Control 2019, 51, 106–112. [Google Scholar] [CrossRef] [PubMed]
- Barrett, P. Structural Equation Modelling: Adjudging Model Fit. Personal. Individ. Differ. 2007, 42, 815–824. [Google Scholar] [CrossRef]
- Schermelleh-Engel, K.; Moosbrugger, H.; Müller, H. Evaluating the Fit of Structural Equation Models: Tests of Significance and Descriptive Goodness-of-Fit Measures. Methods Psychol. Res. 2003, 8, 23–74. [Google Scholar]
- Grace, R.C.; Kivell, B.M.; Laugesen, M. Predicting Decreases in Smoking with a Cigarette Purchase Task: Evidence from an Excise Tax Rise in New Zealand. Tob. Control 2015, 24, 582–587. [Google Scholar] [CrossRef]
- Etikan, I.; Musa, S.A.; Alkassim, R.S. Comparison of Convenience Sampling and Purposive Sampling. Am. J. Theor. Appl. Stat. 2015, 5, 1. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Total Sample (N = 341) |
|---|---|
| Demographics | |
| Age (years), Mean (SD) | 56.26 (9.88) |
| Women, % (n) | 53.1 (181) |
| Marital Status, % (n) | |
| Single | 11.7 (40) |
| Married | 62.2 (212) |
| Divorced | 18.2 (62) |
| Widow | 7.9 (27) |
| Academic degree, % (n) | |
| None | 3.8 (13) |
| Primary education | 15.5(53) |
| Secondary education | 52.5 (179) |
| University education | 28.2 (96) |
| Employees, % (n) | 40.2 (137) |
| Tobacco use, Mean (SD) | |
| Age at onset | 17.40 (5.75) |
| Years smoking | 34.97 (12.03) |
| Daily cigarettes | 17.48 (8.31) |
| GN-SBQ | 17.30 (7.51) |
| FTND | 5.46 (2.2) |
| NDSS | 15.83 (5.64) |
| MTWS | 10.55 (6.4) |
| CO | 15.48 (8.24) |
| AUDIT, Mean (SD) | 3.99 (3.08) |
| GN-SBQ Items | Mean (SD) | Skewness | Kurtosis | Corrected Item—Total Correlation | if Item Deleted | if Item Deleted |
|---|---|---|---|---|---|---|
| 1. My cigarette habit is very important to me. | 2.35 (1.35) | −0.59 | −0.84 | 0.405 | 0.739 | 0.742 |
| 2. I handle and manipulate my cigarette as part of the ritual of smoking. | 0.50 (1.01) | 1.96 | 2.71 | 0.405 | 0.740 | 0.747 |
| 3. Do you place something in your mouth to distract you from smoking? | 0.75 (1.15) | 1.30 | 0.50 | 0.284 | 0.753 | 0.759 |
| 4. Do you reward yourself with a cigarette after accomplishing a task? | 2.39 (1.42) | −0.53 | −0.99 | 0.452 | 0.732 | 0.736 |
| 5. If you find yourself without cigarettes, will you have difficulties in concentrating before attempting a task? | 2.00 (1.52) | −0.07 | −1.44 | 0.476 | 0.729 | 0.731 |
| 6. If you are not allowed to smoke in certain places, do you then play with your cigarette pack or a cigarette? | 0.25 (0.70) | 3.37 | 11.99 | 0.421 | 0.743 | 0.749 |
| 7. Do certain environmental cues trigger your smoking, e.g., favorite chair, sofa, room, car, or drinking alcohol? | 2.89 (1.21) | −1.10 | 0.39 | 0.369 | 0.743 | 0.747 |
| 8. Do you find yourself lighting up a cigarette routinely (without craving)? | 2.54 (1.21) | −0.70 | −0.24 | 0.372 | 0.743 | 0.747 |
| 9. Do you find yourself placing an unlit cigarette or other objects (pen, toothpick, chewing gum, etc.) in your mouth and sucking to get relief from stress, tension, or frustration, etc.? | 0.65 (1.11) | 1.62 | 1.52 | 0.433 | 0.736 | 0.745 |
| 10. Does part of your enjoyment of smoking come from the steps (ritual) you take when lighting up? | 1.49 (1.47) | 0.40 | −1.30 | 0.404 | 0.739 | 0.746 |
| 11. When you are alone in a restaurant, bus terminal, party, etc., do you feel safe, secure, or more confident if you are holding a cigarette? | 1.49 (1.52) | 0.42 | −1.33 | 0.485 | 0.727 | 0.728 |
| Model | gl | CFI | TLI | PNFI | RMSEA (CI 90%) | SRMR | |
|---|---|---|---|---|---|---|---|
| Original | |||||||
| One-factor (Glover et al., 2005) [14] | 194.386 | 44 | 0.925 | 0.907 | 0.726 | 0.099 (0.085, 0.113) | 0.092 |
| Two-factors (Rocha et al., 2014) [15] † | 188.318 | 43 | 0.928 | 0.908 | 0.712 | 0.098 (0.084, 0.113) | 0.090 |
| Respecified †† | |||||||
| One-factor model with correlated errors | 125.682 | 43 | 0.959 | 0.947 | 0.735 | 0.075 (0.060, 0.090) | 0.074 |
| Two-factor model with correlated errors † | 124.929 | 42 | 0.959 | 0.946 | 0.718 | 0.075 (0.060, 0.091) | 0.074 |
| Items | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 |
|---|---|---|---|---|---|---|---|---|---|
| 1. GN-SBQ | |||||||||
| 2. FTND | 0.409 ** | ||||||||
| 3. NDSS | 0.499 ** | 0.0406 ** | |||||||
| 4. AUDIT | −0.006 | −0.008 | −0.025 | ||||||
| 5. CO | 0.102 | 0.400 ** | 0.157 ** | −0.029 | |||||
| 6. Age | −0.336 ** | -0.245 ** | −0.152 * | −0.101 | −0.186 ** | ||||
| 7. Years of smoking | −0.123 * | −0.073 | −0.051 | −0.076 | −0.097 | 0.636 ** | |||
| 8. Daily cigarettes | 0.143 ** | 0.532 ** | 0.154 ** | 0.077 | 0.475 ** | −0.152 * | −0.038 | ||
| 9. MTWS | 0.352 ** | 0.213 ** | 0.405 ** | −0.104 | 0.026 | −0.120 * | −0.043 | 0.024 |
| Variables | Mild (n = 87) Mean (SD) | Moderate (n = 175) Mean (SD) | Strong (n = 79) Mean (SD) | H (p) | ηp2 |
|---|---|---|---|---|---|
| FTND | 4.32 (2.00) a | 5.43 (2.12) b | 6.82 (1.84) c | 53.37 (0.001) | 0.152 |
| NDSS | 12.15 (4.49) a | 15.86 (5.03) b | 19.81 (5.37) c | 75.28 (0.001) | 0.217 |
| MTWS | 7.86 (5.23) a | 10.12 (6.05) b | 14.44 (6.59) c | 46.46 (0.001) | 0.132 |
| Age | 61.17 (8.88) a | 55.60 (9.74) b | 52.39 (9.19) c | 36.15 (0.001) | 0.101 |
| Daily cigarettes | 16.43 (8.23) a | 17.02 (8.16) a | 18.86 (8.98) a | 4.99 (0.083) | 0.009 |
| Years of smoking | 36.23 (13.12) a | 35.02 (11.77) a | 33.50 (11.37) a | 3.38 (0.185) | 0.004 |
| AUDIT | 3.36 (2.78) a | 3.22 (2.81) a | 3.23 (2.80) a | 0.62 (0.735) | 0.004 |
| CO | 14.43 (7.09) a | 15.28 (8.73) ab | 17.01 (8.17) b | 4.81 (0.090) | 0.008 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carballo, J.L.; Rodríguez-Espinosa, S.; Sancho-Domingo, C.; Coloma-Carmona, A. Validation of the Glover–Nilsson Smoking Behavioral Questionnaire (GN-SBQ) to Evaluate Nicotine Dependence in Spanish Clinical Settings. Int. J. Environ. Res. Public Health 2023, 20, 1119. https://doi.org/10.3390/ijerph20021119
Carballo JL, Rodríguez-Espinosa S, Sancho-Domingo C, Coloma-Carmona A. Validation of the Glover–Nilsson Smoking Behavioral Questionnaire (GN-SBQ) to Evaluate Nicotine Dependence in Spanish Clinical Settings. International Journal of Environmental Research and Public Health. 2023; 20(2):1119. https://doi.org/10.3390/ijerph20021119
Chicago/Turabian StyleCarballo, José Luis, Sara Rodríguez-Espinosa, Clara Sancho-Domingo, and Ainhoa Coloma-Carmona. 2023. "Validation of the Glover–Nilsson Smoking Behavioral Questionnaire (GN-SBQ) to Evaluate Nicotine Dependence in Spanish Clinical Settings" International Journal of Environmental Research and Public Health 20, no. 2: 1119. https://doi.org/10.3390/ijerph20021119
APA StyleCarballo, J. L., Rodríguez-Espinosa, S., Sancho-Domingo, C., & Coloma-Carmona, A. (2023). Validation of the Glover–Nilsson Smoking Behavioral Questionnaire (GN-SBQ) to Evaluate Nicotine Dependence in Spanish Clinical Settings. International Journal of Environmental Research and Public Health, 20(2), 1119. https://doi.org/10.3390/ijerph20021119