
What Concept of Manual Therapy Is More Effective to Improve Health Status in Women with Fibromyalgia Syndrome? A Study Protocol with Preliminary Results

 ,
,  , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
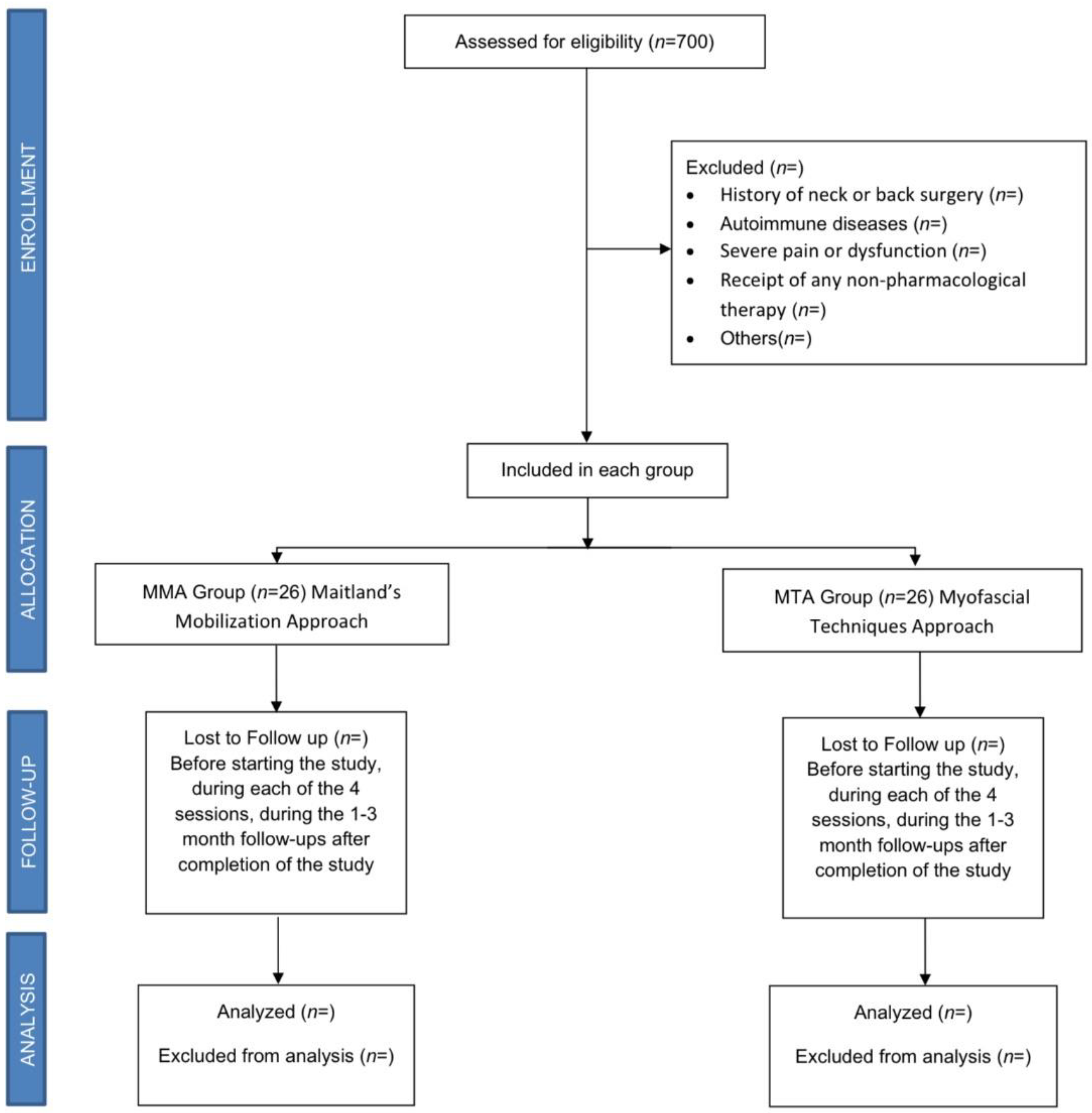
2.1. Study Design
2.2. Sample
Sample Size
2.3. Intervention
2.3.1. MMA Group
2.3.2. MTA Group
- -
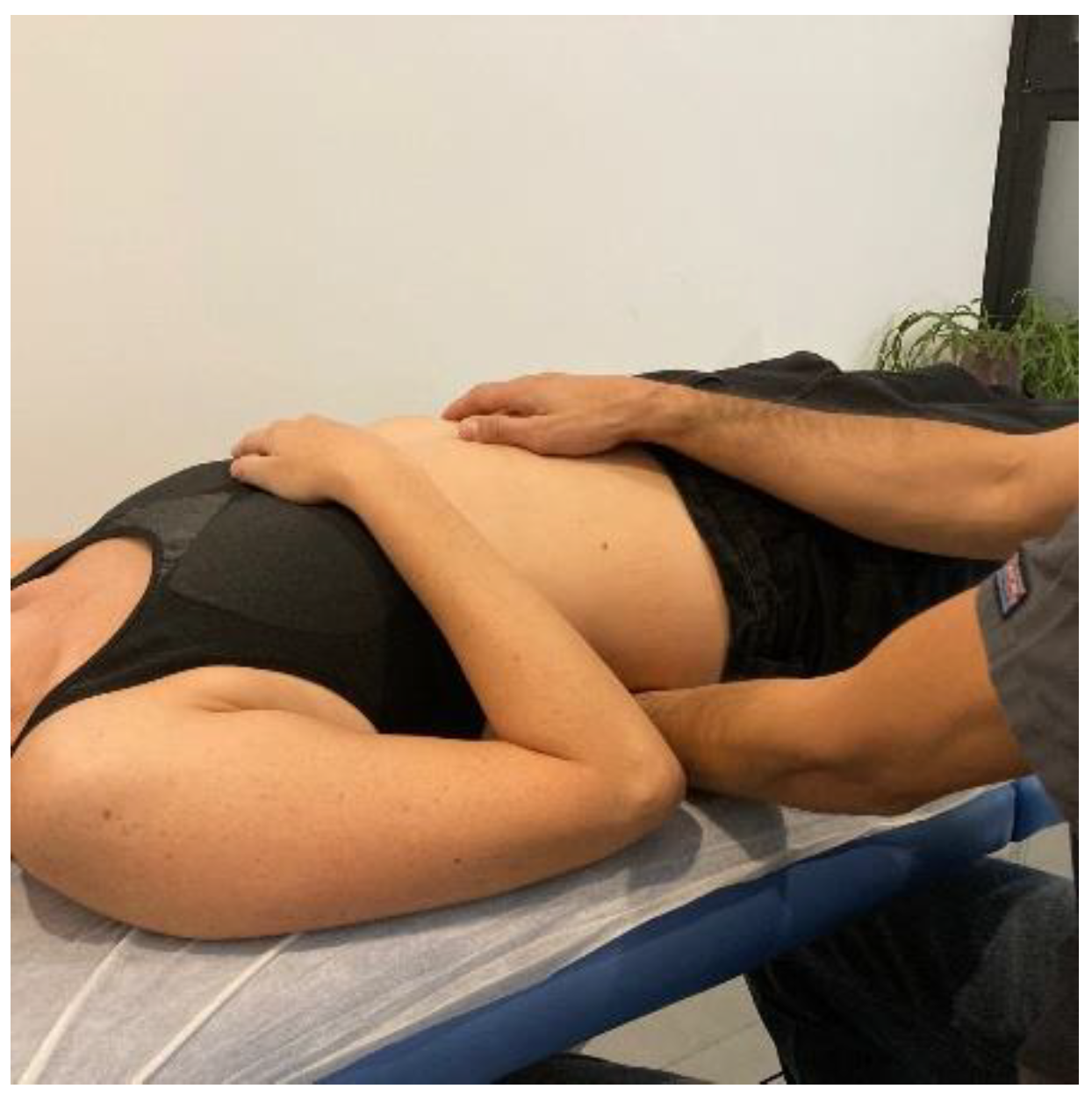
- Transverse planes on the thoracolumbar fascia (TCL) and abdomen: the physical therapist, seated on one side of the table, places his hands facing each other so that one hand is between the table and the patient’s TCL and the other on the abdomen (leaving the navel between the first commissure) (Figure 5, myofascial technique 1).
- -
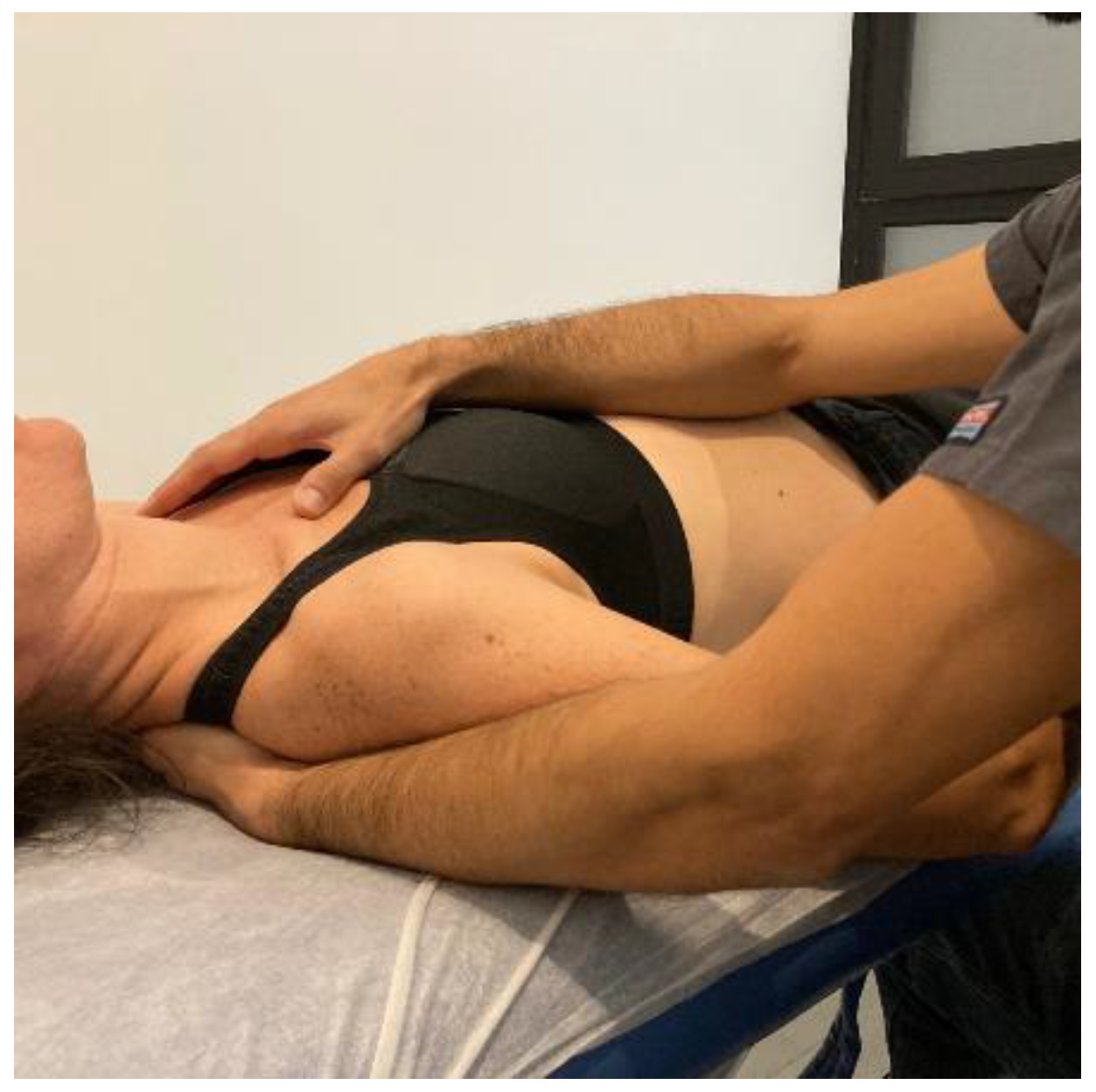
- Transverse planes at C7-D3 and sternum: the physical therapist, seated on one side of the table, places his hands facing each other so that one hand is between the table and the patient’s first 4 thoracic vertebrae (C7-T4) and the other on the sternum (thumb and index finger on each of the sternoclavicular joints) (Figure 6, Myofascial technique 2).
- -
- Suboccipital inhibition: in a first phase, the physiotherapist, seated at the head of the table, places his hands under the patient’s head transversely between the occipital and the spinous process of C2, so that the metacarpophalangeal joints are at 90° and the head is suspended with only this contact. In a second phase, the head is lowered in such a way that the occipital bone rests on the tenar eminences and a slight traction is maintained cranially (Figure 7, Myofascial technique 3).



2.4. Randomization and Blinding
2.5. Outcomes Measurement
2.5.1. Widespread Pain
2.5.2. Symptom Severity
2.5.3. Impact of FM on Quality of Life
2.5.4. Assessment of Perceived Pain and Sensitization-Associated
2.5.5. Sleep Quality
2.5.6. Physical Activity
2.5.7. Psychological, Cognitive, and Emotional Factors
2.5.8. Patient Satisfaction
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Müller, W.; Schneider, E.M.; Stratz, T. The classification of fibromyalgia syndrome. Rheumatol. Int. 2007, 27, 1005–1010. [Google Scholar] [CrossRef]
- Giesecke, T.; Williams, D.A.; Harris, R.E.; Cupps, T.R.; Tian, X.; Tian, T.X.; Gracely, R.H.; Clauw, D.J. Subgrouping of fibromyalgia patients on the basis of pressure-pain thresholds and psychological factors. Arthritis Rheum. 2003, 48, 2916–2922. [Google Scholar] [CrossRef]
- Morera, L.M.T. Fibromialgia. Rev. Soc. Esp. Dolor. 2008, 15, 501–502. [Google Scholar]
- Mohabbat, A.B.; Mohabbat, N.M.L.; Wight, E.C. Fibromyalgia and Chronic Fatigue Syndrome in the Age of COVID-19. Mayo Clin. Proc. Innov. Qual. Outcomes 2020, 4, 764–766. [Google Scholar] [CrossRef]
- Cabo-Meseguer, A.; Cerdá-Olmedo, G.; Trillo-Mata, J.L. Fibromyalgia: Prevalence, epidemiologic profiles and economic costs. Med. Clín. 2017, 149, 441–448. [Google Scholar] [CrossRef]
- Romero, E.A.S.; Martínez Rolando, L.; Villafañe, J.H. Impact of Lockdown on Patients with Fibromyalgia. Electron. J. Gen. Med. 2022, 19, em366. [Google Scholar] [CrossRef]
- Drozd, M.; Marzęda, M.; Blicharz, A.; Czarnota, J.; Piecewicz-Szczęsna, H. Unclear etiology and current hypotheses of the pathogenesis of fibromyalgia. J. Educ. Health Sport. 2020, 10, 338. [Google Scholar] [CrossRef]
- Bellato, E.; Marini, E.; Castoldi, F.; Barbasetti, N.; Mattei, L.; Bonasia, D.E.; Blonna, D. Fibromyalgia syndrome: Etiology, pathogenesis, diagnosis, and treatment. Pain Res. Treat. 2012, 2012, 426130. [Google Scholar] [CrossRef]
- Adams, L.M.; Turk, D.C. Central sensitization and the biopsychosocial approach to understanding pain. J. Appl. Biobehav. Res. 2018, 23, e12125. [Google Scholar] [CrossRef]
- Stilwell, P.; Harman, K. An enactive approach to pain: Beyond the biopsychosocial model. Phenomenol. Cogn. Sci. 2019, 18, 637–665. [Google Scholar] [CrossRef]
- Romero, E.A.S.; Martínez-Pozas, O.; García-González, M.; de-Pedro, M.; González-Álvarez, M.E.; Esteban-González, P.; Cid-Verdejo, R.; Villafañe, J.H. Association between Sleep Disorders and Sleep Quality in Patients with Temporomandibular Joint Osteoarthritis: A Systematic Review. Biomedicines 2022, 10, 2143. [Google Scholar] [CrossRef]
- Häuser, W.; Welsch, P.; Klose, P.; Derry, S.; Straube, S.; Wiffen, P.J.; Moore, R.A. Pharmacological therapies for fibromyalgia in adults—An overview of Cochrane Reviews. Cochrane Database Syst. Rev. 2018, 2018, CD013151. [Google Scholar] [CrossRef]
- Hernando-Garijo, I.; Jiménez-Del-Barrio, S.; Mingo-Gómez, T.; Medrano-de-la-Fuente, R.; Ceballos-Laita, L. Effectiveness of non-pharmacological conservative therapies in adults with fibromyalgia: A systematic review of high-quality clinical trials. J. Back Musculoskelet. Rehabil. 2022, 35, 3–20. [Google Scholar] [CrossRef] [PubMed]
- Castro-Sánchez, A.M.; Aguilar-Ferrándiz, M.E.; Matarán-Peñarrocha, G.A.; Sánchez-Joya Mdel, M.; Arroyo-Morales, M.; Fernández-de-las-Peñas, C. Short-term effects of a manual therapy protocol on pain, physical function, quality of sleep, depressive symptoms, and pressure sensitivity in women and men with fibromyalgia syndrome: A randomized controlled trial. Clin. J. Pain. 2014, 30, 589–597. [Google Scholar] [CrossRef] [PubMed]
- Moustafa, I.M.; Diab, A.A. The addition of upper cervical manipulative therapy in the treatment of patients with fibromyalgia: A randomized controlled trial. Rheumatol. Int. 2015, 35, 1163–1174. [Google Scholar] [CrossRef] [PubMed]
- Reis, M.S.; Durigan, J.L.; Arena, R.; Rossi, B.R.; Mendes, R.G.; Borghi-Silva, A. Effects of posteroanterior thoracic mobilization on heart rate variability and pain in women with fibromyalgia. Rehabil. Res. Pract. 2014, 2014, 898763. [Google Scholar] [CrossRef] [PubMed]
- Castro-Sánchez, A.M.; Matarán-Peñarrocha, G.A.; Sánchez-Labraca, N.; Quesada-Rubio, J.M.; Granero-Molina, J.; Moreno-Lorenzo, C. A randomized controlled trial investigating the effects of craniosacral therapy on pain and heart rate variability in fibromyalgia patients. Clin. Rehabil. 2011, 25, 25–35. [Google Scholar] [CrossRef]
- Bialosky, J.E.; Beneciuk, J.M.; Bishop, M.D.; Coronado, R.A.; Penza, C.W.; Simon, C.B.; George, S.Z. Unraveling the Mechanisms of Manual Therapy: Modeling an Approach. J. Orthop. Sports Phys. Ther. 2018, 48, 8–18. [Google Scholar] [CrossRef]
- Ughreja, R.A.; Venkatesan, P.; Balebail Gopalakrishna, D.; Singh, Y.P. Effectiveness of myofascial release on pain, sleep, and quality of life in patients with fibromyalgia syndrome: A systematic review. Complement. Ther. Clin. Pract. 2021, 45, 101477. [Google Scholar] [CrossRef]
- Wolfe, F.; Smythe, H.A.; Yunus, M.B.; Bennett, R.M.; Bombardier, C.; Goldenberg, D.L.; Tugwell, P.; Campbell, S.M.; Abeles, M.; Clark, P.; et al. The American College of Rheumatology 1990 criteria for the classification of fibromyalgia. Arthritis Rheum. 1990, 33, 160–172. [Google Scholar] [CrossRef]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.-A.; Goldenberg, D.L.; Katz, R.S.; Mease, P.; Russell, A.S.; Russell, I.J.; Winfield, J.B.; Yunus, M.B. The American College of Rheumatology Preliminary Diagnostic Criteria for Fibromyalgia and Measurement of Symptom Severity. Arthritis Care Res. 2010, 62, 600–610. [Google Scholar] [CrossRef] [PubMed]
- Moyano, S.; Kilstein, J.G.; Alegre de Miguel, C. Nuevos criterios diagnósticos de fibromialgia: ¿vinieron para quedarse? Reumatol. Clin. 2015, 11, 210–214. [Google Scholar] [CrossRef]
- Sánchez-Romero, E.A.; González-Zamorano, Y.; Arribas-Romano, A.; Martínez-Pozas, O.; Espinar, E.F.; Pedersini, P.; Villafañe, J.H.; Pérez, J.L.A.; Fernández-Carnero, J. Efficacy of Manual Therapy on Facilitatory Nociception and Endogenous Pain Modulation in Older Adults with Knee Osteoarthritis: A Case Series. Appl. Sci. 2021, 11, 1895. [Google Scholar] [CrossRef]
- Maitland, G.D.; Hengeveld, E.; English, K.; Banks, K. Maitland’s Vertebral Manipulation, 7th ed.; Butterworth–Heinemann: Oxford, UK, 2000. [Google Scholar]
- Terhorst, L.; Schneider, M.J.; Kim, K.H.; Goozdich, L.M.; Stilley, C.S. Complementary and alternative medicine in the treatment of pain fibromialgia: A systematic review. JMPT 2011, 34, 486–496. [Google Scholar]
- Castro-Sánchez, A.M.; Matarán-Peñarrocha, G.A.; Arroyo-Morales, M.; Saavedra-Hernández, M.; Fernández-Sola, C.; Moreno-Lorenzo, C. Effects of myofascial release techniques on pain, physical function, and postural stability in patients with fibromyalgia: A randomized controlled trial. Clin. Rehabil. 2011, 25, 800–813. [Google Scholar] [CrossRef]
- Romero, E.A.S.; Fernández-Carnero, J.; Calvo-Lobo, C.; Sáez, V.O.; Caballero, V.B.; Pecos-Martín, D. Is a Combination of Exercise and Dry Needling Effective for Knee OA? Pain Med. 2020, 21, 349–363. [Google Scholar]
- Elkana, O.; Nimni, Y.; Ablin, J.N.; Shorer, R.; Aloush, V. The Montreal Cognitive Assessment Test (MoCA) as a screening tool for cognitive dysfunction in fibromyalgia. Clin. Exp. Rheumatol. 2022, 40, 1136–1142. [Google Scholar] [CrossRef]
- Wolfe, F. New American College of Rheumatology criteria for fibromyalgia: A twenty-year journey. Arthritis Care Res. 2010, 62, 583–584. [Google Scholar] [CrossRef]
- Gelman, S.M.; Lera, S.; Caballero, F.; López, M.J. Multidisciplinary treatment of fibromyalgia. Prospective controlled pilot study. Rev. Esp. Reumatol. 2005, 32, 99–105. [Google Scholar]
- Esteve-Vives, J.; Redondo, J.R.; Salvat, M.S.; de García Blanco, M.; de Miquel, C.A. Propuesta de una versión de consenso del Fibromyalgia Impact Questionnaire (FIQ) para la población española. Reumatol. Clin. 2007, 3, 21–24. [Google Scholar] [CrossRef]
- Ramos-Goñi, J.M.; Craig, B.M.; Oppe, M.; Ramallo-Fariña, Y.; Pinto-Prades, J.L.; Luo, N.; Rivero-Arias, O. Handling Data Quality Issues to Estimate the Spanish EQ-5D-5L Value Set Using a Hybrid Interval Regression Approach. Value Health 2018, 21, 596–604. [Google Scholar] [CrossRef] [PubMed]
- Liew, B.X.W.; Valera-Calero, J.A.; Varol, U.; Nijs, J.; Arendt-Nielsen, L.; Plaza-Manzano, G.; Fernández-de-las-Peñas, C. Distress and Sensitization as Main Mediators of Severity in Women with Fibromyalgia: A Structural Equation Model. Biomedicines 2022, 10, 1188. [Google Scholar] [CrossRef] [PubMed]
- Neblett, R.; Cohen, H.; Choi, Y.; Hartzell, M.M.; Williams, M.; Mayer, T.G.; Gatchel, R.J. The Central Sensitization Inventory (CSI): Establishing clinically significant values for identifying central sensitivity syndromes in an outpatient chronic pain sample. J. Pain 2013, 14, 438–445. [Google Scholar] [CrossRef]
- Tel Adıgüzel, K.; Köroğlu, Ö.; Yaşar, E.; Tan, A.K.; Samur, G. The relationship between dietary total antioxidant capacity, clinical parameters, and oxidative stress in fibromyalgia syndrome: A novel point of view. Turk. J. Phys. Med. Rehabil. 2022, 68, 262–270. [Google Scholar] [CrossRef] [PubMed]
- Alvarez, M.C.; Albuquerque, M.L.L.; Neiva, H.P.; Cid, L.; Rodrigues, F.; Teixeira, D.S.; Matos, R.; Antunes, R.; Morales-Sánchez, V.; Monteiro, D. Exploring the Relationship between Fibromyalgia-Related Fatigue, Physical Activity, and Quality of Life. Int. J. Environ. Res. Public Health 2022, 19, 4870. [Google Scholar] [CrossRef]
- Benitez-Porres, J.; Delgado, M.; Ruiz, J.R. Comparison of physical activity estimates using International Physical Activity Questionnaire (IPAQ) and accelerometry in fibromyalgia patients: The Al-Andalus study. J. Sports Sci. 2013, 31, 1741–1752. [Google Scholar] [CrossRef]
- Inal, O.; Aras, B.; Salar, S. Investigation of the relationship between kinesiophobia and sensory processing in fibromyalgia patients. Somatosens. Mot. Res. 2020, 37, 92–96. [Google Scholar] [CrossRef]
- Gómez-Pérez, L.; López-Martínez, A.E.; Ruiz-Párraga, G.T. Psychometric Properties of the Spanish Version of the Tampa Scale for Kinesiophobia (TSK). J. Pain 2011, 12, 425–435. [Google Scholar] [CrossRef]
- de Paula, T.M.H.; Castro, M.S.; Medeiros, L.F.; Paludo, R.H.; Couto, F.F.; da Costa, T.R.; Fortes, J.P.; Salbego, M.d.O.; Behnck, G.S.; de Moura, T.A.M.; et al. Association of low-dose naltrexone and transcranial direct current stimulation in fibromyalgia: A randomized, double-blinded, parallel clinical trial. Braz. J. Anesthesiol. 2022. [Google Scholar] [CrossRef]
- Arnau, R.C.; Meagher, M.W.; Norris, M.P.; Bramson, R. Psychometric evaluation of the Beck Depression Inventory-II with primary care medical patients. Health psychology. Off. J. Div. Health Psychol. Am. Psychol. Assoc. 2001, 20, 112–119. [Google Scholar]
- Van Overmeire, R.; Vesentini, L.; Vanclooster, S.; Muysewinkel, E.; Bilsen, J. Body Image, Medication Use, and Mental Health among Women with Fibromyalgia in Flanders, Belgium. Int. J. Environ. Res. Public Health 2022, 19, 1418. [Google Scholar] [CrossRef]
- Justyn, W. You Get Used to It, Or Do You: Symptom Length Predicts Less Fibromyalgia Physical Impairment, but only for those with Above-Average Self-Efficacy. Physiol. Behav. 2017, 176, 139–148. [Google Scholar]
- Kaleth, A.S. Predictors of physical therapy activity in patients with fibromyalgia: A path analysis. J. Clin. Rheumatol. 2020, 28, e203–e209. [Google Scholar] [CrossRef] [PubMed]
- Martín-Aragón, M.; Pastor, M.A.; Rodríguez-Marín, J.; March, M.K.; Lledó, A.; López-Roig, S. Percepción de autoeficacia en dolor crónico. Adaptación y validación de la Chronic Pain Self-Efficacy Scale. J. Health Psychol. 1999, 11, 53–75. [Google Scholar]
- Romero, E.A.S.; Lim, T.; Villafañe, J.H.; Boutin, G.; Aguado, V.R.; Pintado-Zugasti, A.M.; Pérez, J.L.A.; Carnero, J.F. The Influence of Verbal Suggestion on Post-Needling Soreness and Pain Processing after Dry Needling Treatment: An Experimental Study. Int. J. Environ. Res. Public Health 2021, 18, 4206. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Carnero, J.; Beltrán-Alacreu, H.; Arribas-Romano, A.; Cerezo-Téllez, E.; Cuenca-Zaldivar, J.N.; Sánchez-Romero, E.A.; Lara, S.L.; Villafañe, J.H. Prediction of Patient Satisfaction after Treatment of Chronic Neck Pain with Mulligan’s Mobilization. Life 2023, 13, 48. [Google Scholar] [CrossRef]
- Jaeschke, R.; Singer, J.; Guyatt, G.H. Measurement of Health Status: Ascertaining the Minimal Clinically Important Difference. Control. Clin. Trials 1989, 10, 407–415. [Google Scholar] [CrossRef]
- Bennett, R.M.; Bushmakin, A.G.; Cappelleri, J.C.; Zlateva, G.; Sadosky, A.B. Minimal clinically important difference in the fibromyalgia impact questionnaire. J. Rheumatol. 2009, 36, 1304–1311. [Google Scholar] [CrossRef]
- Coste, J.; Medkour, T.; Maigne, J.Y.; Pérez, M.; Laroche, F.; Perrot, S. Osteopathic medicine for fibromyalgia: A sham-controlled randomized clinical trial. Ther. Adv. Musculoskelet. Dis. 2021, 13, 1759720X211009017. [Google Scholar] [CrossRef]
- Nijs, J.; George, S.; Clauw, D.; Fernández-de-las-Peñas, C.; Kosek, E.; Ickmans, K.; Fernández-Carnero, J.; Polli, A.; Kapreli, E.; Huysmans, E.; et al. Central sensitisation in chronic pain conditions: Latest discoveries and their potential for precision medicine. Lancet Rheumatol. 2021, 3, e383–e392. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| MTA Group | MMA Group | |
|---|---|---|
| Mean (±SD) | Mean (±SD) | |
| n | 8 | 5 |
| Age (y) | 58.57 (±5.38) | 57 (±9.77) |
| Time with pain (y) | 15.14 (±8.13) | 24.2 (±16.2) |
| Time from diagnosis (y) | 8.14 (±4.91) | 9.8 (±3.03) |
| Has a job | Yes: 37.7%; No: 50%; N/A: 12.5% | Yes: 80%; No: 20% |
| Annual Salary | <25.000: 0 >25.000 > 40.000: 37.5% >40.000: 0 W/S: %: 62.5% | <25.000: 80% >25.000 > 40.000: 0 >40.000: 0 W/S: 20% |
| Lives Alone | Yes: 87.5%; N/A: 12.5 | Yes: 20% No: 80% |
| MTA Group | MMA Group | U-Mann-Whitney | |
|---|---|---|---|
| Mean (±SD) | Mean (±SD) | p | |
| NPRS | 6.13 (1.24) | 6.40 (0.548) | 0.696 |
| IPAQ | 1.63 (0.74) | 2.20 (0.837) | 0.212 |
| GHQ12 | 8.13 (7.75) | 19.20 (3.7) | 0.658 |
| EuroQol-5D | 0.81 (0.83) | 0.681 (11.51) | 0.079 |
| BDI-II | 2.29 (1.254) | 3.20 (0.837) | 0.2 |
| STAI | 32.75 (11.33) | 36.8 (7.62) | 0.419 |
| PSQI | 14.63 (3.7) | 12.4 (4.45) | 0.302 |
| FIQ | 52.28 (17.25) | 54.87 (11.27) | 0.884 |
| CSI | 5563 (10.65) | 63.80 (12.05) | 0.213 |
| TSK | 25.38 (6.65) | 19.40 (2.6) | 0.056 |
| MTA Group | MMA Group | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | p Values | Mean ± SD | p Values | |||||||||
| Post | 1 m | 2 m | Pre-Post | Pre-1 m | Pre-2 m | Post | 1 m | 2 m | Pre-Post | Pre-1 m | Pre-2 m | |
| NPRS | 3.13 ± 2.29 | 5.63 ± 2.06 | 5.64 ± 2.75 | 0.018 * | 0.518 | 0.735 | 4.6 ± 24 | 7.40 ± 0.89 | 6.6 ± 1.14 | 0.136 | 0.129 | 0.655 |
| IPAQ | 2.12 ± 0.835 | 2.13 ± 0.99 | 1.57 ± 0.535 | 0.102 | 0.102 | 0.564 | 2.20 ± 0.44 | 1.6 ± 0.55 | 1.8 ± 0.48 | 1 | 0.18 | 0.157 |
| GHQ12 | 8.25 ± 3.96 | 12.63 ± 5.01 | 14.8 ± 4.45 | 0.011 * | 0.05* | 0.446 | 18.6 ± 9.18 | 22.4 ± 6.1 | 16 ± 8.27 | 0.5 | 0.144 | 0.416 |
| EuroQol-5D | 0.78 ± 0.12 | 0.76 ± 0.09 | 0.8 ± 0.15 | 0.553 | 0.263 | 1 | 0.67 ± 0.15 | 0.67 ± 0.11 | 0.72 ± 0.13 | 0.9 | 0.893 | 0.686 |
| BDI-II | 1.63 ± 0.744 | 1.75 ± 0.7 | 1.43 ± 0.78 | 0.102 | 0.317 | 0.180 | 2.60 ± 1.52 | 2.4 ± 0.89 | 2.20 ± 1.3 | 0.18 | 0.102 | 0.197 |
| STAI | 27.25 ± 10.05 | 28.13 ± 8.04 | 31.29 ± 8.9 | 0.107 | 0.207 | 0.733 | 34.2 ± 3.56 | 37.4 ± 8.56 | 33.8 ± 6.38 | 0.273 | 1 | 0.465 |
| PSQI | 13 ± 4.20 | 16.13 ± 3.52 | 15.29 ± 2.21 | 0.446 | 0.396 | 0.461 | 11.8 ± 4.44 | 13.6 ± 6.02 | 14.4 ± 5.46 | 0.581 | 0.686 | 0.496 |
| FIQ | 44.07 ± 13.14 | 41.33 ± 8.20 | 44.78 ± 11.87 | 0.036 * | 0.036 * | 0.31 | 58.41 ± 24.6 | 51.66 ± 14.66 | 49.07 ± 9.57 | 0.893 | 0.5 | 0.5 |
| CSI | 49.75 ± 11.46 | 53.5 ± 12.23 | 54 ± 6.08 | 0.012 * | 0.324 | 0.865 | 62.6 ± 11.13 | 58.2 ± 18.17 | 60.4 ± 10.33 | 0.686 | 0.345 | 0.138 |
| TSK | 24.63 ± 7.46 | 24 ± 7.54 | 22.71 ± 6.72 | 0.778 | 0.395 | 0.672 | 18.2 ± 3.83 | 24 ± 9.48 | 20.8 ± 3.96 | 0.588 | 0.5 | 0.496 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Audoux, C.R.; Estrada-Barranco, C.; Martínez-Pozas, O.; Gozalo-Pascual, R.; Montaño-Ocaña, J.; García-Jiménez, D.; Vicente de Frutos, G.; Cabezas-Yagüe, E.; Sánchez Romero, E.A. What Concept of Manual Therapy Is More Effective to Improve Health Status in Women with Fibromyalgia Syndrome? A Study Protocol with Preliminary Results. Int. J. Environ. Res. Public Health 2023, 20, 1061. https://doi.org/10.3390/ijerph20021061
Audoux CR, Estrada-Barranco C, Martínez-Pozas O, Gozalo-Pascual R, Montaño-Ocaña J, García-Jiménez D, Vicente de Frutos G, Cabezas-Yagüe E, Sánchez Romero EA. What Concept of Manual Therapy Is More Effective to Improve Health Status in Women with Fibromyalgia Syndrome? A Study Protocol with Preliminary Results. International Journal of Environmental Research and Public Health. 2023; 20(2):1061. https://doi.org/10.3390/ijerph20021061
Chicago/Turabian StyleAudoux, Carine Romane, Cecilia Estrada-Barranco, Oliver Martínez-Pozas, Rodrigo Gozalo-Pascual, Juan Montaño-Ocaña, David García-Jiménez, Gonzalo Vicente de Frutos, Elena Cabezas-Yagüe, and Eleuterio A. Sánchez Romero. 2023. "What Concept of Manual Therapy Is More Effective to Improve Health Status in Women with Fibromyalgia Syndrome? A Study Protocol with Preliminary Results" International Journal of Environmental Research and Public Health 20, no. 2: 1061. https://doi.org/10.3390/ijerph20021061
APA StyleAudoux, C. R., Estrada-Barranco, C., Martínez-Pozas, O., Gozalo-Pascual, R., Montaño-Ocaña, J., García-Jiménez, D., Vicente de Frutos, G., Cabezas-Yagüe, E., & Sánchez Romero, E. A. (2023). What Concept of Manual Therapy Is More Effective to Improve Health Status in Women with Fibromyalgia Syndrome? A Study Protocol with Preliminary Results. International Journal of Environmental Research and Public Health, 20(2), 1061. https://doi.org/10.3390/ijerph20021061