
The Effect of Mindset and Breathing Exercises on Physical and Mental Health in Persons with Spinal Cord Injury—A Pilot Feasibility Study

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Design
2.3. Intervention
2.4. Feasibility
2.5. Efficacy—Physical Health
2.6. Efficacy—Mental Health
2.7. Statistics
3. Results
3.1. Feasibility
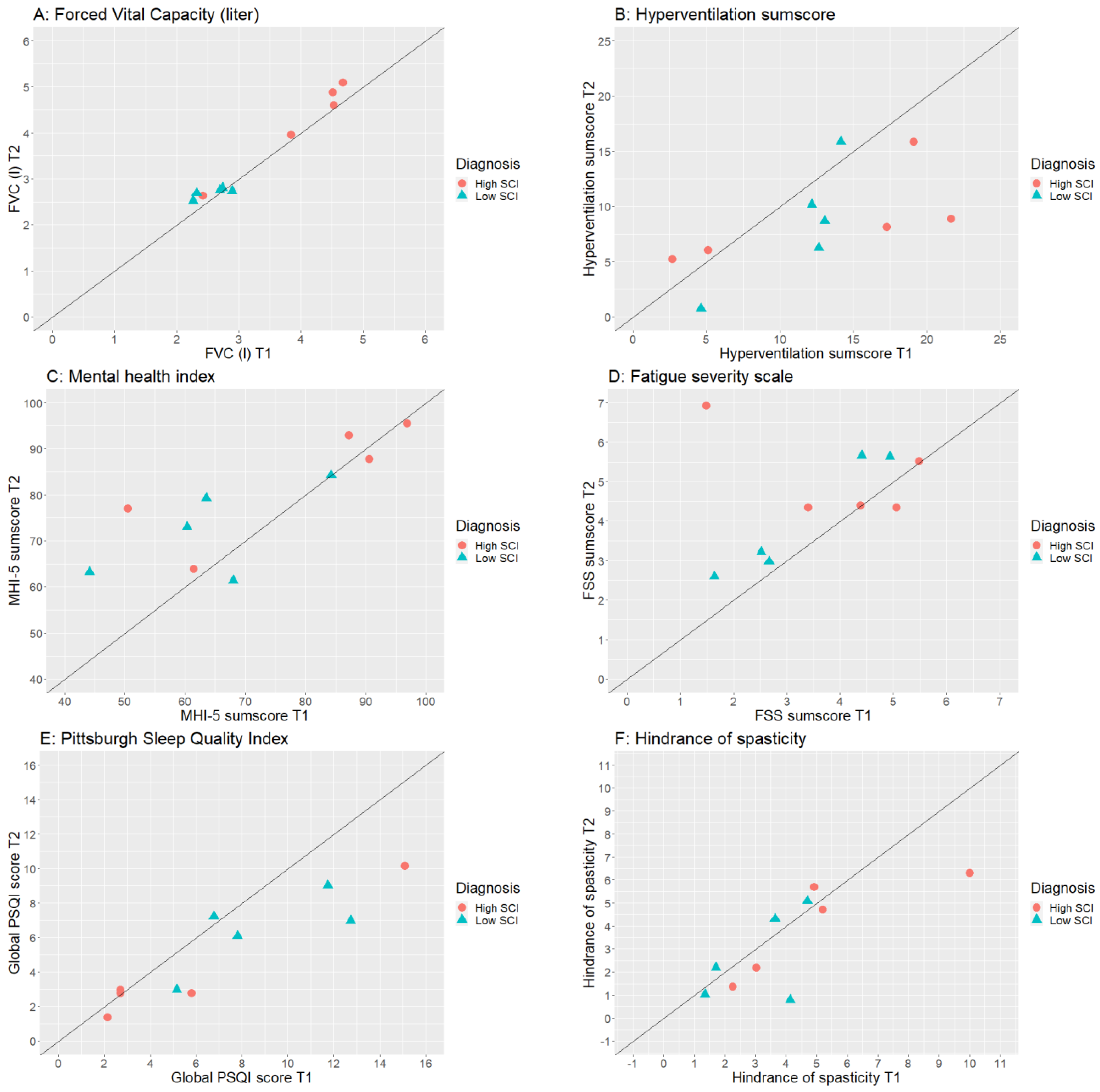
3.2. Physical Health
3.3. Mental Health
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- McKinley, W.O.; Jackson, A.B.; Cardenas, D.D.; DeVivo, M.J. Long-term medical complications after traumatic spinal cord injury: A regional model systems analysis. Arch. Phys. Med. Rehabil. 1999, 80, 1402–1410. [Google Scholar] [CrossRef]
- Zimmer, M.B.; Nantwi, K.; Goshgarian, H.G. Effect of spinal cord injury on the respiratory system: Basic research and current clinical treatment options. J. Spinal Cord Med. 2007, 30, 319–330. [Google Scholar] [CrossRef]
- Brown, R.; DiMarco, A.F.; Hoit, J.D.; Garshick, E. Respiratory dysfunction and management in spinal cord injury. Respir. Care 2006, 51, 853–868; discussion 869–870. [Google Scholar]
- Rintala, D.H.; Robinson-Whelen, S.; Matamoros, R. Subjective stress in male veterans with spinal cord injury. J. Rehabil. Res. Dev. 2005, 42, 291–304. [Google Scholar] [CrossRef]
- Rekand, T.; Hagen, E.M.; Grønning, M. Chronic pain following spinal cord injury. Tidsskr. Nor. Laegeforen. 2012, 132, 974–979. [Google Scholar] [CrossRef] [PubMed]
- Middleton, J.W.; Leong, G.; Mann, L. Management of spinal cord injury in general practice—Part 2. Aust. Fam. Physician 2008, 37, 331–332, 335–338. [Google Scholar]
- Rekand, T.; Hagen, E.M.; Grønning, M. Spasticity following spinal cord injury. Tidsskr. Nor. Laegeforen. 2012, 132, 970–973. [Google Scholar] [CrossRef]
- Buijze, G.A.; De Jong, H.M.Y.; Kox, M.; van de Sande, M.G.; Van Schaardenburg, D.; Van Vugt, R.M.; Popa, C.D.; Pickkers, P.; Baeten, D.L.P. An add-on training program involving breathing exercises, cold exposure, and meditation attenuates inflammation and disease activity in axial spondyloarthritis—A proof of concept trial. PLoS ONE 2019, 14, e0225749. [Google Scholar] [CrossRef] [PubMed]
- Kox, M.; Stoffels, M.; Smeekens, S.P.; van Alfen, N.; Gomes, M.; Eijsvogels, T.M.; Hopman, M.T.; van der Hoeven, J.G.; Netea, M.G.; Pickkers, P. The influence of concentration/meditation on autonomic nervous system activity and the innate immune response: A case study. Psychosom. Med. 2012, 74, 489–494. [Google Scholar] [CrossRef] [PubMed]
- Zwaag, J.; Naaktgeboren, R.; van Herwaarden, A.E.; Pickkers, P.; Kox, M. The Effects of Cold Exposure Training and a Breathing Exercise on the Inflammatory Response in Humans: A Pilot Study. Psychosom. Med. 2022, 84, 457–467. [Google Scholar] [CrossRef] [PubMed]
- Faid, T.; Van Gordon, W.; Taylor, E.C. Breathing Exercises, Cold-Water Immersion, and Meditation: Mind-Body Practices Lead to Reduced Stress and Enhanced Well-Being. Adv. Mind Body Med. 2022, 36, 12–20. [Google Scholar] [PubMed]
- Petraskova Touskova, T.; Bob, P.; Bares, Z.; Vanickova, Z.; Nyvlt, D.; Raboch, J. A novel Wim Hof psychophysiological training program to reduce stress responses during an Antarctic expedition. J. Int. Med. Res. 2022, 50, 3000605221089883. [Google Scholar] [CrossRef] [PubMed]
- Lemos, J.R.; da Cunha, F.A.; Lopes, A.J.; Guimarães, F.S.; do Amaral Vasconcellos, F.V.; Dos Santos Vigário, P. Respiratory muscle training in non-athletes and athletes with spinal cord injury: A systematic review of the effects on pulmonary function, respiratory muscle strength and endurance, and cardiorespiratory fitness based on the FITT principle of exercise prescription. J. Back Musculoskelet. Rehabil. 2020, 33, 655–667. [Google Scholar] [CrossRef] [PubMed]
- Tavoian, D.; Craighead, D.H. Deep breathing exercise at work: Potential applications and impact. Front. Physiol. 2023, 14, 1040091. [Google Scholar] [CrossRef]
- Simpson, R.; Mair, F.S.; Mercer, S.W. Mindfulness-based stress reduction for people with multiple sclerosis—A feasibility randomised controlled trial. BMC Neurol. 2017, 17, 94. [Google Scholar] [CrossRef]
- Hearn, J.H.; Cross, A. Mindfulness for pain, depression, anxiety, and quality of life in people with spinal cord injury: A systematic review. BMC Neurol. 2020, 20, 32. [Google Scholar] [CrossRef]
- Esperland, D.; de Weerd, L.; Mercer, J.B. Health effects of voluntary exposure to cold water—A continuing subject of debate. Int. J. Circumpolar Health 2022, 81, 2111789. [Google Scholar] [CrossRef]
- Standardization of Spirometry, 1994 Update. American Thoracic Society. Am. J. Respir. Crit. Care Med. 1995, 152, 1107–1136. [CrossRef]
- Nachtegaal, J.; van Langeveld, S.A.; Slootman, H.; Post, M.W.M. Implementation of a Standardized Dataset for Collecting Information on Patients with Spinal Cord Injury. Top. Spinal Cord Inj. Rehabil. 2018, 24, 133–140. [Google Scholar] [CrossRef]
- van Cooten, I.P.; Snoek, G.J.; Nene, A.V.; de Groot, S.; Post, M.W. Functional hindrance due to spasticity in individuals with spinal cord injury during inpatient rehabilitation and 1 year thereafter. Spinal Cord 2015, 53, 663–667. [Google Scholar] [CrossRef]
- van Dixhoorn, J.; Duivenvoorden, H.J. Efficacy of Nijmegen Questionnaire in recognition of the hyperventilation syndrome. J. Psychosom. Res. 1985, 29, 199–206. [Google Scholar] [CrossRef]
- van Leeuwen, C.M.; van der Woude, L.H.; Post, M.W. Validity of the mental health subscale of the SF-36 in persons with spinal cord injury. Spinal Cord 2012, 50, 707–710. [Google Scholar] [CrossRef]
- Hoeymans, N.; Garssen, A.A.; Westert, G.P.; Verhaak, P.F. Measuring mental health of the Dutch population: A comparison of the GHQ-12 and the MHI-5. Health Qual. Life Outcomes 2004, 2, 23. [Google Scholar] [CrossRef][Green Version]
- Merkies, I.S.; Schmitz, P.I.; Samijn, J.P.; van der Meché, F.G.; van Doorn, P.A. Fatigue in immune-mediated polyneuropathies. European Inflammatory Neuropathy Cause and Treatment (INCAT) Group. Neurology 1999, 53, 1648–1654. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F., 3rd; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Anderson, K.D.; Cowan, R.E.; Horsewell, J. Facilitators and Barriers to Spinal Cord Injury Clinical Trial Participation: Multi-National Perspective of People Living with Spinal Cord Injury. J. Neurotrauma 2016, 33, 493–499. [Google Scholar] [CrossRef]


{kind=link}
| Participant | Sex | Age (Years) | Spinal Cord Injury Level and Completeness | Time Since Injury (Years) |
|---|---|---|---|---|
| 1 | M | 56 | C3—AIS C | 1 |
| 2 | M | 46 | C3–4—AIS A | 3 |
| 3 | M | 49 | Th3—AIS B | 4 |
| 4 | M | 41 | Th6—AIS A | 3 |
| 5 | F | 31 | Th6—AIS D | 1 |
| 6 | F | 27 | Th7—AIS C | 4 |
| 7 | F | 62 | Th10—AIS A | 3 |
| 8 | F | 53 | Th10—AIS C | 44 |
| 9 | F | 59 | L2—AIS D | 13 |
| 10 | F | 62 | L3—AIS D | 29 |
| What Has the Training Achieved? | N | What Was Difficult about the Training? | N |
|---|---|---|---|
| Better sleep | 4 | Lack of motivation, self-discipline | 4 |
| More relaxed | 4 | Cost a lot of time/effort | 2 |
| More energy | 4 | Difficult alone, easier in group | 2 |
| Less pain | 3 | Giving up control | 2 |
| Physical improvement (e.g., more strength in legs) | 2 | First round of breathing exercise needed to get into it | 1 |
| Better activation of the lungs | 2 | More difficult without music | 1 |
| Less spasms | 2 | Need more and longer guidance | 1 |
| Better concentration | 2 | I was skeptical | 1 |
| Less problems with cold body | 1 | I had less control over diaphragm during the training, now I have more control again | 1 |
| Can breathe through nose when lying supine | 1 | Focus on thoughts before/after exercises | 1 |
| Core is more active | 1 | ||
| Better cough | 1 | ||
| Better fear control | 1 | ||
| Better mood | 1 |
| T1 | T2 | p-Value | Effect Size | |||
|---|---|---|---|---|---|---|
| Outcome Measure | N | Median (IQR) | N | Median (IQR) | ||
| Respiratory function | ||||||
| FVC (l) | 10 | 2.8 (2.4–4.5) | 10 | 2.8 (2.7–4.7) | 0.022 | 0.67 |
| %FVC (%) | 10 | 76.0 (67.0–90.0) | 10 | 79.0 (72.0–92.0) | 0.036 | 0.66 |
| FEV1 (l) | 10 | 2.3 (2.1–3.6) | 10 | 2.4 (2.2–3.7) | 0.059 | 0.60 |
| %FEV1 (%) | 10 | 84.0 (69.0–92.0) | 10 | 85.0 (71.0–94.0) | 0.102 | 0.52 |
| PEF (l/s) | 10 | 5.4 (4.4–8.8) | 10 | 6.6 (5.3–8.6) | 0.059 | 0.60 |
| Blood pressure (mm Hg) | ||||||
| Systolic | 9 | 121.0 (112.0–141.0) | 10 | 121.0 (108.0–121.0) | 0.574 | 0.19 |
| Diastolic | 9 | 75.0 (64.0–90.0) | 10 | 76.0 (68.0–90.0) | 0.477 | 0.24 |
| Average pain intensity last week? (0–10) | ||||||
| Nociceptive pain | 4 | 6.0 (3.3–8.0) | 5 | 3.0 (2.5–5.0) | 0.317 | 0.71 |
| Neuropathic pain | 7 | 5.0 (3.0–8.0) | 6 | 6.5 (2.8–7.8) | 0.713 | 0.15 |
| Other pain | 8 | 3.0 (2.0–6.8) | 5 | 2.0 (2.0–4.0) | 0.059 | 0.95 |
| Pain interference in ADL last week? (0–10) | ||||||
| Nociceptive pain | 4 | 4.5 (0.8–7.5) | 5 | 1.0 (0.0–2.5) | 0.655 | 0.32 |
| Neuropathic pain | 7 | 3.0 (0.0–6.0) | 6 | 0.5 (0.0–3.0) | 0.197 | 0.53 |
| Other pain | 8 | 0.0 (0.0–2.8) | 5 | 0.0 (0.0–0.0) | 0.109 | 0.80 |
| Spasticity | ||||||
| Degree (0–10) | 10 | 3.0 (0.0–7.8) | 10 | 2.0 (0.8–4.3) | 0.320 | 0.31 |
| Discomfort (0–10) | 10 | 3.0 (1.8–7.0) | 10 | 2.5 (0.0–3.5) | 0.088 | 0.54 |
| Hindrance of spasticity | 10 | 4.0 (2.0–5.0) | 10 | 3.0 (1.0–5.3) | 0.131 | 0.48 |
| Hyperventilation | 10 | 13.0 (5.0–17.5) | 10 | 8.5 (5.8–11.5) | 0.036 | 0.66 |
| MHI-5 | 10 | 66.0 (58.0–89.0) | 10 | 78.0 (64.0–89.0) | 0.091 | 0.53 |
| Fatigue severity scale | 10 | 3.9 (2.2–4.9) | 10 | 4.4 (3.2–5.7) | 0.021 | 0.73 |
| Global PSQI score | 10 | 6.5 (3.0–12.2) | 10 | 4.5 (3.0–7.5) | 0.018 | 0.75 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Groot, S.; Ettema, F.W.L.; van Leeuwen, C.M.C.; Achterberg, W.J.; Janssen, T.W.J.; Hoekstra, S.P. The Effect of Mindset and Breathing Exercises on Physical and Mental Health in Persons with Spinal Cord Injury—A Pilot Feasibility Study. Int. J. Environ. Res. Public Health 2023, 20, 6784. https://doi.org/10.3390/ijerph20186784
de Groot S, Ettema FWL, van Leeuwen CMC, Achterberg WJ, Janssen TWJ, Hoekstra SP. The Effect of Mindset and Breathing Exercises on Physical and Mental Health in Persons with Spinal Cord Injury—A Pilot Feasibility Study. International Journal of Environmental Research and Public Health. 2023; 20(18):6784. https://doi.org/10.3390/ijerph20186784
Chicago/Turabian Stylede Groot, Sonja, Frank W. L. Ettema, Christel M. C. van Leeuwen, Wendy J. Achterberg, Thomas W. J. Janssen, and Sven P. Hoekstra. 2023. "The Effect of Mindset and Breathing Exercises on Physical and Mental Health in Persons with Spinal Cord Injury—A Pilot Feasibility Study" International Journal of Environmental Research and Public Health 20, no. 18: 6784. https://doi.org/10.3390/ijerph20186784
APA Stylede Groot, S., Ettema, F. W. L., van Leeuwen, C. M. C., Achterberg, W. J., Janssen, T. W. J., & Hoekstra, S. P. (2023). The Effect of Mindset and Breathing Exercises on Physical and Mental Health in Persons with Spinal Cord Injury—A Pilot Feasibility Study. International Journal of Environmental Research and Public Health, 20(18), 6784. https://doi.org/10.3390/ijerph20186784