


Nature Photographs as Complementary Care in Chemotherapy: A Randomized Clinical Trial

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
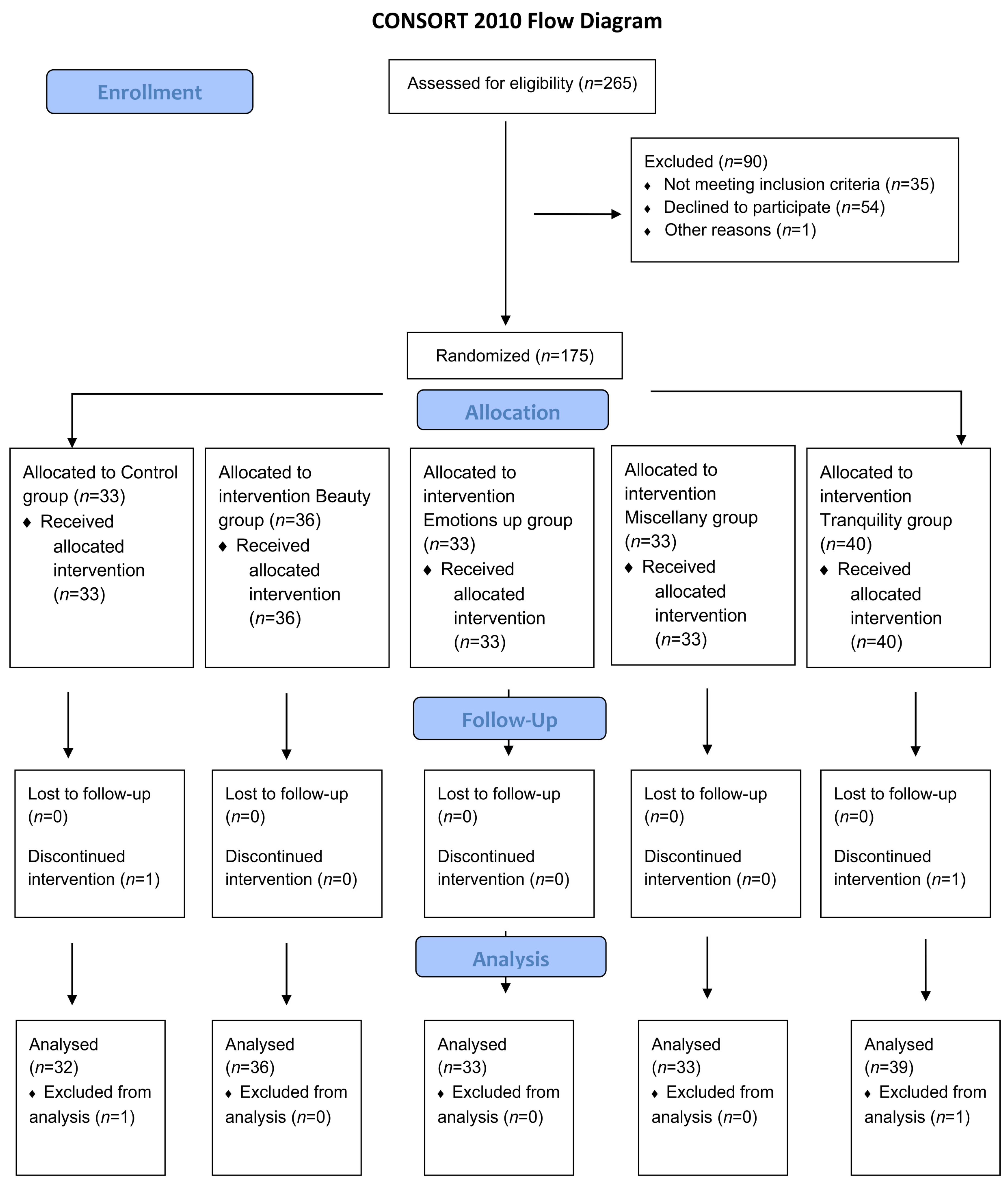
2.2. Randomization and Sample Size
2.3. Data Sources and Measures
2.4. Intervention
- Beauty: related to awe/fascination. Includes white and colorful birds, insects, flowers, and landscapes. Valence range: 6.9–7.8; Arousal range: 3.1–4.2.
- Emotions Up: related to joy and liveliness. Includes water, pale birds, colorful birds, sky, insects, and sea. Valence range: 5.8–8.0; Arousal range: 3.3–5.6.
- Tranquility: related to peace and calm. Includes water, sky, and sea. Valence range: 6.6–8.0; Arousal range: 2.8–4.2.
- Miscellany: includes water, trees, white birds, colorful birds, sky, flowers, insects, and landscapes. Valence range: 5.3–7.5; Arousal range: 3.0–6.1.
2.5. Statistical Analysis
3. Results
3.1. Participant Characterization
3.2. Positive and Negative Affect
3.3. Edmonton Symptom Assessment System (ESAS)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Mattiuzzi, C.; Lippi, G. Current Cancer Epidemiology. J. Epidemiol. Glob. Health 2019, 9, 217–222. [Google Scholar] [CrossRef]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- DeVita, V.T.J.; Lawrence, T.S.; Rosemberg, A.S. Cancer: Principles and Practice of Oncology, 8th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2008. [Google Scholar]
- Krzyszczyk, P.; Acevedo, A.; Davidoff, E.J.; Timmins, L.M.; Marrero-Berrios, I.; Patel, M.; White, C.; Lowe, C.; Sherba, J.J.; Hartmanshenn, C.; et al. The growing role of precision and personalized medicine for cancer treatment. Technology 2018, 6, 79–100. [Google Scholar] [CrossRef]
- Zhong, L.; Li, Y.; Xiong, L.; Wang, W.; Wu, M.; Yuan, T.; Yang, W.; Tian, C.; Miao, Z.; Wang, T.; et al. Small molecules in targeted cancer therapy: Advances, challenges, and future perspectives. Signal Transduct. Target. Ther. 2021, 6, 201. [Google Scholar] [CrossRef] [PubMed]
- Teston, E.F.; Fukumori, E.F.C.; Benedetti, G.M.S.; Spigolon, D.N.; Costa, M.A.R.; Marcon, S.S. Feelings and difficulties experienced by cancer patients along the diagnostic and therapeutic itineraries. Esc. Anna Nery 2018, 22, e20180017. [Google Scholar] [CrossRef]
- Temiz, G.; Durna, Z. Evaluation of Quality of Life and Health Care Needs in Cancer Patients Receiving Chemotherapy. J. Cancer Educ. 2020, 35, 796–807. [Google Scholar] [CrossRef]
- Nightingale, F. Notes on Nursing: What It Is and What It Is Not, 1st ed.; Harrison: London, UK, 1859. [Google Scholar]
- Ulrich, R.S. View through a window may influence recovery from surgery. Science 1984, 224, 420–421. [Google Scholar] [CrossRef] [PubMed]
- Rowlands, J.; Noble, S. How does the environment impact on the quality of life of advanced cancer patients? A qualitative study with implications for ward design. Palliat. Med. 2008, 22, 768–774. [Google Scholar] [CrossRef]
- Blaschke, S. The role of nature in cancer patients’ lives: A systematic review and qualitative meta-synthesis. BMC Cancer 2017, 17, 370. [Google Scholar] [CrossRef] [PubMed]
- San Juan, C.; Subiza-Pérez, M.; Vozmediano, L. Restoration and the City: The Role of Public Urban Squares. Front. Psychol. 2017, 8, 2093. [Google Scholar] [CrossRef]
- Watson, D.; Clark, L.A.; Tellegen, A. Development and validation of brief measures of positive and negative affect: The PANAS scales. J. Pers. Soc. Psychol. 1988, 54, 1063–1070. [Google Scholar] [CrossRef] [PubMed]
- Mayer, F.S.; Frantz, C.M. The Connectedness to Nature Scale: A Measure of Individuals’Feeling in Community with Nature. J. Environ. Psychol. 2004, 24, 503–515. [Google Scholar] [CrossRef]
- Dal Fabbro, D.; Catissi, G.; Borba, G.; Lima, L.; Hingst-Zaher, E.; Rosa, J.; Victor, E.; Bernardes, L.; Souza, T.; Leão, E. e-Nature Positive Emotions Photography Database (e-NatPOEM): Affectively rated nature images promoting positive emotions. Sci. Rep. 2021, 11, 11696. [Google Scholar] [CrossRef] [PubMed]
- American Society of Clinical Oncology. QOPI® Certification Program (QCP™) Manual; American Society of Clinical Oncology: Alexandria, VA, USA, 2020. [Google Scholar]
- Randomizer. Available online: https://www.randomizer.at/ (accessed on 18 June 2023).
- Pessoa, V.S.; Gouveia, V.V.; Soares, A.K.S.; Vilar, R.; Freires, L.A. Escala de conexão com a natureza: Evidências psicométricas no contexto brasileiro. Estud. Psicol. 2016, 33, 271–282. [Google Scholar] [CrossRef]
- Pires, P.; Filgueiras, A.; Ribas, R.; Santana, C. Positive and negative affect schedule: Psychometric properties for the Brazilian Portuguese version. Span. J. Psychol. 2013, 16, E58. [Google Scholar] [CrossRef]
- Joint Commission International. Standards for Hospitals; Joint Commission International: Oak Brook, IL, USA, 2021. [Google Scholar]
- American Nurses Credentialing Center. Magnet Recognition Program: Application Manual; American Nurses Credentialing Center: Silver Spring, MD, USA, 2020. [Google Scholar]
- Liang, K.Y.; Zeger, S.L. Longitudinal Data Analysis Using Generalized Linear Models. Biometrika 1986, 73, 13–22. [Google Scholar] [CrossRef]
- Ciere, Y.; Janse, M.; Almansa, J.; Visser, A.; Sanderman, R.; Sprangers, M.A.G.; Ranchor, A.V.; Fleer, J. Distinct trajectories of positive and negative affect after colorectal cancer diagnosis. Health Psychol. 2017, 36, 521–528. [Google Scholar] [CrossRef]
- Voogt, E.; van der Heide, A.; van Leeuwen, A.F.; Visser, A.P.; Cleiren, M.P.; Passchier, J.; van der Maas, P.J. Positive and negative affect after diagnosis of advanced cancer. Psychooncology 2005, 14, 262–273. [Google Scholar] [CrossRef]
- Fekete, A.; Maidhof, R.M.; Specker, E.; Nater, U.M.; Leder, H. Does art reduce pain and stress? A registered report protocol of investigating autonomic and endocrine markers of music, visual art, and multimodal aesthetic experience. PLoS ONE 2022, 17, e0266545. [Google Scholar] [CrossRef]
- Starcke, K.; Mayr, J.; von Georgi, R. Emotion Modulation through Music after Sadness Induction-The Iso Principle in a Controlled Experimental Study. Int. J. Environ. Res. Public Health 2021, 18, 12486. [Google Scholar] [CrossRef]
- Zhou, X.; Wildschut, T.; Sedikides, C.; Chen, X.; Vingerhoets, A.J. Heartwarming memories: Nostalgia maintains physiological comfort. Emotion 2012, 12, 678–684. [Google Scholar] [CrossRef]
- Umezawa, S.; Higurashi, T.; Uchiyama, S.; Sakai, E.; Ohkubo, H.; Endo, H.; Nonaka, T.; Nakajima, A. Visual distraction alone for the improvement of colonoscopy-related pain and satisfaction. World J. Gastroenterol. 2015, 21, 4707–4714. [Google Scholar] [CrossRef] [PubMed]
- Segrin, C.; Badger, T.A.; Dorros, S.M.; Meek, P.; Lopez, A.M. Interpersonal communication and depression in a cancer support group: Is it more therapeutic than receiving assistance? J. Soc. Clin. Psychol. 2007, 26, 256–276. [Google Scholar]
- Greer, J.A.; Jacobs, J.M.; El-Jawahri, A.; Nipp, R.D.; Gallagher, E.R.; Pirl, W.F.; Park, E.R.; Muzikansky, A.; Jacobsen, J.C.; Jackson, V.A.; et al. Role of patient-clinician communication in the relationship between symptom burden and quality of life in patients with advanced cancer. J. Clin. Oncol. 2018, 36, 718–724. [Google Scholar]
- Gamble, K.R.; Howard, J.H., Jr.; Howard, D.V. Not just scenery: Viewing nature pictures improves executive attention in older adults. Exp. Aging Res. 2014, 40, 513–530. [Google Scholar] [CrossRef] [PubMed]
- Eijlers, R.; Utens, E.M.W.J.; Staals, L.M.; de Nijs, P.F.A.; Berghmans, J.M.; Wijnen, R.M.H.; Hillegers, M.H.J.; Dierckx, B.; Legerstee, J.S. Systematic Review and Meta-analysis of Virtual Reality in Pediatrics: Effects on Pain and Anxiety. Anesth. Analg. 2019, 129, 1344–1353. [Google Scholar] [CrossRef]
- López-Valverde, N.; Muriel-Fernández, J.; López-Valverde, A.; Valero-Juan, L.F.; Ramírez, J.M.; Flores-Fraile, J.; Herrero-Payo, J.; Blanco-Antona, L.A.; Macedo-de-Sousa, B.; Bravo, M. Use of Virtual Reality for the Management of Anxiety and Pain in Dental Treatments: Systematic Review and Meta-Analysis. J. Clin. Med. 2020, 24, 3086. [Google Scholar] [CrossRef] [PubMed]
- Ioannou, A.; Papastavrou, E.; Avraamides, M.N.; Charalambous, A. Virtual Reality and Symptoms Management of Anxiety, Depression, Fatigue, and Pain: A Systematic Review. SAGE Open Nurs. 2020, 6, 23. [Google Scholar] [CrossRef]
- Wiederhold, B.K.; Gao, K.; Sulea, C.; Wiederhold, M.D. Virtual reality as a distraction technique in chronic pain patients. Cyberpsychol. Behav. Soc. Netw. 2014, 17, 346–352. [Google Scholar] [CrossRef]
- Schneider, S.M.; Hood, L.E. Virtual reality: A distraction intervention for chemotherapy. Oncol. Nurs. Forum 2007, 34, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Baños, R.M.; Espinoza, M.; García-Palacios, A.; Cervera, J.M.; Esquerdo, G.; Barrajón, E.; Botella, C. A positive psychological intervention using virtual reality for patients with advanced cancer in a hospital setting: A pilot study to assess feasibility. Support. Care Cancer 2013, 21, 263–270. [Google Scholar] [CrossRef] [PubMed]
- Weigand, R.; Jacobsen, T. Beauty and the busy mind: Occupied working memory resources impair aesthetic experiences in everyday life. PLoS ONE 2021, 16, e0248529. [Google Scholar] [CrossRef] [PubMed]
- Ulrich, R. Aesthetic and affective response to natural environment. Behav. Nat. Environ. 1983, 6, 85–125. [Google Scholar]



{kind=link}
{kind=link}
| Total | Control | Miscellany | Tranquility | Emotions Up | Beauty | |
|---|---|---|---|---|---|---|
| 173 | 32 | 33 | 39 | 33 | 36 | |
| Age (years): | ||||||
| mean (standard deviation) | 57 (14) | 56 (14) | 56 (16) | 57 (12) | 61 (14) | 56 (16) |
| minimum—maximum | 22–90 | 33–86 | 30–87 | 23–78 | 33–79 | 22–90 |
| Sex—n (%) | ||||||
| Female | 98 (56.6) | 18 (56.3) | 22 (66.7) | 22 (56.4) | 17 (51.5) | 19 (52.8) |
| Male | 75 (43.4) | 14 (43.8) | 11 (33.3) | 17 (43.6) | 16 (48.5) | 17 (47.2) |
| Nationality—n (%) | ||||||
| Brasil | 162 (93.6) | 27 (84.4) | 32 (97.0) | 39 (100.0) | 33(100.0) | 31 (86.1) |
| Others * | 11 (6.6) | 5 (15.5) | 1 (3.0) | 0 (0.0) | 0 (0.0) | 5 (15.2) |
| Marital status—n (%) | ||||||
| Single | 17 (9.8) | 3 (9.4) | 6 (18.2) | 1 (2.6) | 3 (9.1) | 4 (11.1) |
| Married/with partner | 127 (73.4) | 22 (68.8) | 23 (69.7) | 31 (79.5) | 23 (69.7) | 28 (77.8) |
| Divorced | 24 (13.9) | 7 (21.9) | 4 (12.1) | 6 (15.4) | 5 (15.2) | 2 (5.6) |
| Widowed | 5 (2.9) | 0 (0.0) | 0 (0.0) | 1 (2.6) | 2 (6.1) | 2 (5.6) |
| Education—n (%) | ||||||
| Primary school | 3 (1.8) | 2 (6.2) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (2.8) |
| High school | 18 (10.4) | 2 (6.3) | 4 (12.1) | 4 (10.3) | 2 (6.1) | 6 (16.7) |
| Graduation | 92 (53.2) | 17 (53.1) | 14 (42.4) | 23 (59.0) | 19 (57.6) | 19 (52.8) |
| Postgraduate | 60 (34.7) | 11 (34.4) | 15 (45.5) | 12 (30.8) | 12 (36.3) | 10 (27.8) |
| Born in—n (%) | ||||||
| Rural areas | 10 (5.8) | 4 (12.5) | 0 (0.0) | 3 (7.7) | 3 (9.1) | 0 (0.0) |
| Urban areas | 163 (94.2) | 28 (87.5) | 33 (100.0) | 36 (92.3) | 30 (90.9) | 36(100.0) |
| Background living area—n (%) | ||||||
| Urban | 146 (84.4) | 26 (81.3) | 31 (93.9) | 33 (84.6) | 27 (81.8) | 29 (80.6) |
| Both | 25 (14.5) | 5 (15.6) | 2 (6.1) | 5 (12.8) | 6 (18.2) | 7 (19.4) |
| Rural | 2 (1.2) | 1 (3.1) | 0 (0.0) | 1 (2.6) | 0 (0.0) | 0 (0.0) |
| Frequency of intentional contact with nature—n (%) | ||||||
| Daily | 71 (41.0) | 17 (53.1) | 13 (39.4) | 12 (30.8) | 13 (39.4) | 16 (44.4) |
| 5–6 days/week | 2 (1.2) | 0 (0.0) | 0 (0.0) | 2 (5.1) | 0 (0.0) | 0 (0.0) |
| 3–4 days/week | 14 (8.1) | 1 (3.1) | 5 (15.2) | 5 (12.8) | 1 (3.0) | 2 (5.6) |
| 1–2 days/week | 35 (20.2) | 4 (12.5) | 7 (21.2) | 8 (20.5) | 8 (24.2) | 8 (22.2) |
| Fortnightly | 16 (9.2) | 4 (12.5) | 3 (9.1) | 4 (10.3) | 3 (9.1) | 2 (5.6) |
| Monthly | 24 (13.9) | 6 (18.8) | 4 (12.1) | 5 (12.8) | 5 (15.2) | 4 (11.1) |
| Yearly | 11 (6.4) | 0 (0.0) | 1 (3.0) | 3 (7.7) | 3 (9.1) | 4 (11.1) |
| Total | Control | Miscellany | Tranquility | Emotions Up | Beauty | |
|---|---|---|---|---|---|---|
| 173 | 32 | 33 | 39 | 33 | 36 | |
| 1st chemotherapy session in life—n (%) | ||||||
| No | 102 (59.0) | 18 (56.3) | 20 (60.6) | 26 (66.7) | 20 (60.6) | 18 (50.0) |
| Yes | 71 (41.0) | 14 (43.8) | 13 (39.4) | 13 (33.3) | 13 (39.4) | 18 (50.0) |
| Time since diagnosis—n (%) | ||||||
| Less than 1 month | 15 (8.7) | 4 (12.5) | 0 (0.0) | 4 (10.3) | 3 (9.1) | 4 (11.1) |
| 1–2 months | 34 (19.7) | 7 (21.9) | 6 (18.2) | 8 (20.5) | 6 (18.2) | 7 (19.4) |
| 3–6 months | 44 (25.4) | 5 (15.6) | 10 (30.3) | 8 (20.5) | 10 (30.3) | 11 (30.6) |
| 6 months-1 year | 21 (12.1) | 3 (9.4) | 5 (15.2) | 5 (12.8) | 4 (12.1) | 4 (11.1) |
| 1–5 years | 44 (25.4) | 10 (31.3) | 8 (24.2) | 9 (23.1) | 9 (27.3) | 8 (22.2) |
| More than 5 years | 15 (8.7) | 3 (9.4) | 4 (12.1) | 5 (12.8) | 1 (3.0) | 2 (5.6) |
| Estimated duration of treatment—n (%) | ||||||
| Less than 1 month | 3 (1.7) | 1 (3.1) | 2 (6.1) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| 1–2 months | 11 (6.4) | 1 (3.1) | 0 (0.0) | 4 (10.3) | 2 (6.1) | 4 (11.1) |
| 3–6 months | 44 (25.4) | 11 (34.4) | 7 (21.2) | 9 (23.1) | 7 (21.2) | 10 (27.8) |
| 6 months-1 year | 52 (30.1) | 8 (25.0) | 11 (33.3) | 9 (23.1) | 12 (36.4) | 12 (33.3) |
| 1–5 years | 43 (24.9) | 7 (21.9) | 9 (27.3) | 11 (28.2) | 9 (27.3) | 7 (19.4) |
| More than 5 years | 20 (11.6) | 4 (12.5) | 4 (12.1) | 6 (15.4) | 3 (9.1) | 3 (8.3) |
| Pre-Intervention | Post-Intervention | p-Value Pre vs. Post Intervention * | |
|---|---|---|---|
| Estimated Mean (CI 95%) | Estimated Mean (CI 95%) | ||
| Negative aspects | |||
| Intervention | 17.15 (16.01; 18.38) | 14.45 (13.42; 15.56) | <0.001 |
| Control | 16.30 (13.95; 19.06) | 14.96 (12.89; 17.36) | 0.034 |
| p-value (Groups) | 0.553 | 0.688 | |
| Negative aspects | |||
| Beauty | 16.86 (14.60; 19.47) | 13.90 (11.96; 16.17) | 0.017 |
| Emotions Up | 17.24 (14.81; 20.08) | 14.52 (12.48; 16.88) | 0.013 |
| Tranquility | 16.97 (14.96; 19.24) | 14.98 (13.02; 17.23) | 0.038 |
| Miscellany | 17.61 (15.45; 20.07) | 14.36 (12.39; 16.65) | <0.001 |
| Control | 16.30 (13.95; 19.06) | 14.96 (12.89; 17.36) | 0.034 |
| p-value (Groups) | 0.963 | 0.953 | |
| Positive aspects | |||
| Intervention | 33.88 (32.76; 35.05) | 34.16 (32.80; 35.58) | 0.620 |
| Control | 34.01 (31.76; 36.43) | 32.92 (30.25; 35.82) | 0.189 |
| p-value (Groups) | 0.924 | 0.433 | |
| Positive aspects | |||
| Beauty | 34.00 (31.87; 36.27) | 35.49 (32.81; 38.39) | 0.268 |
| Emotions Up | 35.94 (33.61; 38.43) | 35.61 (32.70; 38.77) | 0.763 |
| Tranquility | 31.89 (29.75; 34.19) | 32.46 (30.32; 34.75) | 0.458 |
| Miscellany | 34.06 (32.04; 36.21) | 33.27 (30.40; 36.42) | 0.499 |
| Control | 34.01 (31.76; 36.43) | 32.92 (30.25; 35.82) | 0.189 |
| p-value (Groups) | 0.203 | 0.322 |
| Pre-Intervention | Post-Intervention | p-Value Pre vs. Post Intervention * | |
|---|---|---|---|
| Estimated Mean (CI 95%) * | Estimated Mean (CI 95%) | ||
| Pain | |||
| Intervention | 0.97 (0.72; 1.31) | 0.66 (0.46; 0.95) | <0.001 |
| Control | 1.13 (0.76; 1.68) | 0.88 (0.50; 1.53) | 0.258 |
| p-value (Groups) | 0.574 | 0.433 | |
| Tiredness | |||
| Intervention | 2.82 (2.41; 3.29) | 2.26 (1.88; 2.73) | 0.002 |
| Control | 3.59 (2.71; 4.77) | 3.03 (2.19; 4.20) | 0.086 |
| p-value (Groups) | 0.169 | 0.160 | |
| Nausea | |||
| Intervention | 0.75 (0.52; 1.08) | 0.60 (0.40; 0.90) | 0.157 |
| Control | 1.41 (0.80; 2.48) | 1.13 (0.58; 2.20) | 0.297 |
| p-value (Groups) | 0.128 | 0.196 | |
| Depression | |||
| Intervention | 1.90 (1.51; 2.40) | 1.32 (1.00; 1.74) | 0.003 |
| Control | 1.91 (1.21; 3.01) | 1.34 (0.84; 2.15) | 0.139 |
| p-value (Groups) | 0.991 | 0.947 | |
| Anxiety, | |||
| Intervention | 3.01 (2.56; 3.55) | 2.12 (1.72; 2.62) | <0.001 |
| Control | 3.06 (2.23; 4.20) | 2.41 (1.68; 3.45) | 0.046 |
| p-value (Groups) | 0.930 | 0.566 | |
| Drowsiness | |||
| Intervention | 2.88 (2.46; 3.38) | 2.96 (2.53; 3.46) | 0.738 |
| Control | 3.47 (2.55; 4.71) | 3.50 (2.60; 4.72) | 0.931 |
| p-value (Groups) | 0.319 | 0.352 | |
| Appetite | |||
| Intervention | 3.45 (2.99; 3.97) | 2.72 (2.30; 3.23) | 0.001 |
| Control | 3.75 (2.80; 5.02) | 3.22 (2.32; 4.47) | 0.220 |
| p-value (Groups) | 0.619 | 0.400 | |
| Wellbeing | |||
| Intervention | 3.30 (2.90; 3.75) | 2.91 (2.50; 3.38) | 0.054 |
| Control | 4.13 (3.22; 5.28) | 3.63 (2.74; 4.80) | 0.365 |
| p-value (Groups) | 0.142 | 0.204 | |
| Shortness of breath | |||
| Intervention | 0.74 (0.48; 1.14) | 0.52 (0.32; 0.84) | 0.050 |
| Control | 0.59 (0.21; 1.71) | 0.41 (0.13; 1.23) | 0.579 |
| p-value (Groups) | 0.690 | 0.671 | |
| Sleep disturbance | |||
| Intervention | 2.86 (2.46; 3.32) | 2.80 (2.40; 3.27) | 0.753 |
| Control | 4.03 (3.14; 5.18) | 3.41 (2.51; 4.62) | 0.171 |
| p-value (Groups) | 0.036 | 0.291 |
| Pre-Intervention | Post-Intervention | p-Value Pre vs. Post Intervention * | |
|---|---|---|---|
| Estimated Mean (CI 95%) | Estimated Mean (CI 95%) | ||
| Pain | |||
| Beauty | 0.69 (0.35; 1.37) | 0.38 (0.11; 1.26) | 0.001 |
| Emotions Up | 1.15 (0.67; 1.99) | 0.76 (0.37; 1.57) | 0.035 |
| Tranquility | 1.18 (0.67; 2.08) | 0.79 (0.46; 1.36) | 0.063 |
| Miscellany | 0.85 (0.47; 1.53) | 0.70 (0.35; 1.39) | 0.393 |
| Control | 1.13 (0.76; 1.68) | 0.88 (0.50; 1.53) | 0.258 |
| p-value (Groups) | 0.612 | 0.616 | |
| Tiredness | |||
| Beauty | 1.92 (1.24; 2.95) | 1.92 (1.29; 2.85) | >0.99 |
| Emotions Up | 3.12 (2.34; 4.16) | 2.15 (1.44; 3.22) | 0.003 |
| Tranquility | 2.95 (2.28; 3.81) | 2.82 (2.06; 3.86) | 0.713 |
| Miscellany | 3.33 (2.47; 4.49) | 2.09 (1.42; 3.09) | <0.001 |
| Control | 3.59 (2.71; 4.77) | 3.03 (2.19; 4.20) | 0.086 |
| p-value (Groups) | 0.085 | 0.315 | |
| Nausea | |||
| Beauty | 0.42 (0.20; 0.88) | 0.36 (0.14; 0.96) | 0.682 |
| Emotions Up | 0.94 (0.45; 1.96) | 0.58 (0.23; 1.42) | 0.057 |
| Tranquility | 0.72 (0.35; 1.49) | 0.87 (0.44; 1.72) | 0.543 |
| Miscellany | 0.97 (0.53; 1.77) | 0.58 (0.29; 1.14) | 0.071 |
| Control | 1.41 (0.80; 2.48) | 1.13 (0.58; 2.20) | 0.297 |
| p-value (Groups) | 0.115 | 0.353 | |
| Depression | |||
| Beauty | 2.08 (1.31; 3.32) | 0.94 (0.45; 1.97) | 0.031 |
| Emotions Up | 1.61 (0.87; 2.96) | 1.33 (0.78; 2.28) | 0.328 |
| Tranquility | 1.85 (1.22; 2.79) | 1.87 (1.22; 2.88) | 0.941 |
| Miscellany | 2.06 (1.41; 3.02) | 1.06 (0.60; 1.89) | 0.002 |
| Control | 1.91 (1.21; 3.01) | 1.34 (0.84; 2.15) | 0.139 |
| p-value (Groups) | 0.956 | 0.473 | |
| Anxiety | |||
| Beauty | 2.94 (2.08; 4.17) | 1.61 (0.95; 2.74) | 0.006 |
| Emotions Up | 2.85 (1.99; 4.08) | 2.06 (1.37; 3.09) | 0.043 |
| Tranquility | 2.85 (2.08; 3.89) | 2.54 (1.84; 3.51) | 0.459 |
| Miscellany | 3.45 (2.61; 4.58) | 2.24 (1.41; 3.57) | 0.003 |
| Control | 3.06 (2.23; 4.20) | 2.41 (1.68; 3.45) | 0.046 |
| p-value (Groups) | 0.902 | 0.596 |
| Pre-Intervention | Post-Intervention | p-Value Pre vs. Post Intervention * | |
|---|---|---|---|
| Estimated Mean (CI 95%) * | Estimated Mean (CI 95%) | ||
| Drownsiness | |||
| Beauty | 2.78 (1.98; 3.89) | 2.83 (2.07; 3.88) | 0.883 |
| Emotions Up | 2.48 (1.73; 3.58) | 2.58 (1.74; 3.80) | 0.807 |
| Tranquility | 3.08 (2.38; 3.98) | 3.33 (2.55; 4.36) | 0.613 |
| Miscellany | 3.15 (2.27; 4.38) | 3.03 (2.23; 4.12) | 0.831 |
| Control | 3.47 (2.55; 4.71) | 3.50 (2.60; 4.72) | 0.931 |
| p-value (Groups) | 0.681 | 0.702 | |
| Appetite | |||
| Beauty | 2.83 (2.02; 3.98) | 2.42 (1.62; 3.60) | 0.231 |
| Emotions Up | 3.58 (2.74; 4.67) | 2.33 (1.60; 3.40) | 0.006 |
| Tranquility | 4.15 (3.31; 5.22) | 3.56 (2.73; 4.65) | 0.142 |
| Miscellany | 3.15 (2.32; 4.29) | 2.45 (1.75; 3.44) | 0.158 |
| Control | 3.75 (2.80; 5.02) | 3.22 (2.32; 4.47) | 0.220 |
| p-value (Groups) | 0.354 | 0.248 | |
| Wellbeing | |||
| Beauty | 3.11 (2.35; 4.12) | 2.22 (1.58; 3.13) | 0.024 |
| Emotions Up | 3.76 (2.94; 4.81) | 3.30 (2.47; 4.42) | 0.233 |
| Tranquility | 3.38 (2.70; 4.25) | 3.26 (2.54; 4.18) | 0.758 |
| Miscellany | 2.94 (2.27; 3.81) | 2.85 (2.06; 3.94) | 0.821 |
| Control | 4.13 (3.22; 5.28) | 3.63 (2.74; 4.80) | 0.365 |
| p-value (Groups) | 0.364 | 0.176 | |
| Shortness of breath | |||
| Beauty | 0.50 (0.21; 1.17) | 0.22 (0.06; 0.78) | 0.038 |
| Emotions Up | 1.30 (0.64; 2.65) | 1.09 (0.53; 2.25) | 0.432 |
| Tranquility | 0.54 (0.21; 1.35) | 0.49 (0.19; 1.24) | 0.793 |
| Miscellany | 0.67 (0.25; 1.81) | 0.30 (0.11; 0.87) | 0.200 |
| Control | 0.59 (0.21; 1.71) | 0.41 (0.13; 1.23) | 0.579 |
| p-value (Groups) | 0.641 | 0.321 | |
| Sleep disturbance | |||
| Beauty | 2.28 (1.63; 3.18) | 2.83 (2.04; 3.93) | 0.108 |
| Emotions Up | 2.48 (1.78; 3.46) | 2.33 (1.62; 3.37) | 0.618 |
| Tranquility | 3.38 (2.57; 4.45) | 3.10 (2.39; 4.03) | 0.342 |
| Miscellany | 3.24 (2.53; 4.16) | 2.88 (2.14; 3.86) | 0.436 |
| Control | 4.03 (3.14; 5.18) | 3.41 (2.51; 4.62) | 0.171 |
| p-value (Groups) | 0.040 | 0.581 |
| Group | Clinical Improvement |
|---|---|
| Beauty | Pain, Depression, Anxiety, Well-being, Shortness of breath |
| Emotions Up | Tiredness, Depression, Anxiety |
| Tranquility | Pain, Tiredness, Anxiety, Appetite |
| Miscellany | No significant improvement |
| Control | Anxiety |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Catissi, G.; de Oliveira, L.B.; da Silva Victor, E.; Savieto, R.M.; Borba, G.B.; Hingst-Zaher, E.; Lima, L.M.; Bomfim, S.B.; Leão, E.R. Nature Photographs as Complementary Care in Chemotherapy: A Randomized Clinical Trial. Int. J. Environ. Res. Public Health 2023, 20, 6555. https://doi.org/10.3390/ijerph20166555
Catissi G, de Oliveira LB, da Silva Victor E, Savieto RM, Borba GB, Hingst-Zaher E, Lima LM, Bomfim SB, Leão ER. Nature Photographs as Complementary Care in Chemotherapy: A Randomized Clinical Trial. International Journal of Environmental Research and Public Health. 2023; 20(16):6555. https://doi.org/10.3390/ijerph20166555
Chicago/Turabian StyleCatissi, Giulia, Leticia Bernardes de Oliveira, Elivane da Silva Victor, Roberta Maria Savieto, Gustavo Benvenutti Borba, Erika Hingst-Zaher, Luciano Moreira Lima, Sabrina Bortolossi Bomfim, and Eliseth Ribeiro Leão. 2023. "Nature Photographs as Complementary Care in Chemotherapy: A Randomized Clinical Trial" International Journal of Environmental Research and Public Health 20, no. 16: 6555. https://doi.org/10.3390/ijerph20166555
APA StyleCatissi, G., de Oliveira, L. B., da Silva Victor, E., Savieto, R. M., Borba, G. B., Hingst-Zaher, E., Lima, L. M., Bomfim, S. B., & Leão, E. R. (2023). Nature Photographs as Complementary Care in Chemotherapy: A Randomized Clinical Trial. International Journal of Environmental Research and Public Health, 20(16), 6555. https://doi.org/10.3390/ijerph20166555