
The Effects of Plant-Derived Phytochemical Compounds and Phytochemical-Rich Diets on Females with Polycystic Ovarian Syndrome: A Scoping Review of Clinical Trials


Abstract
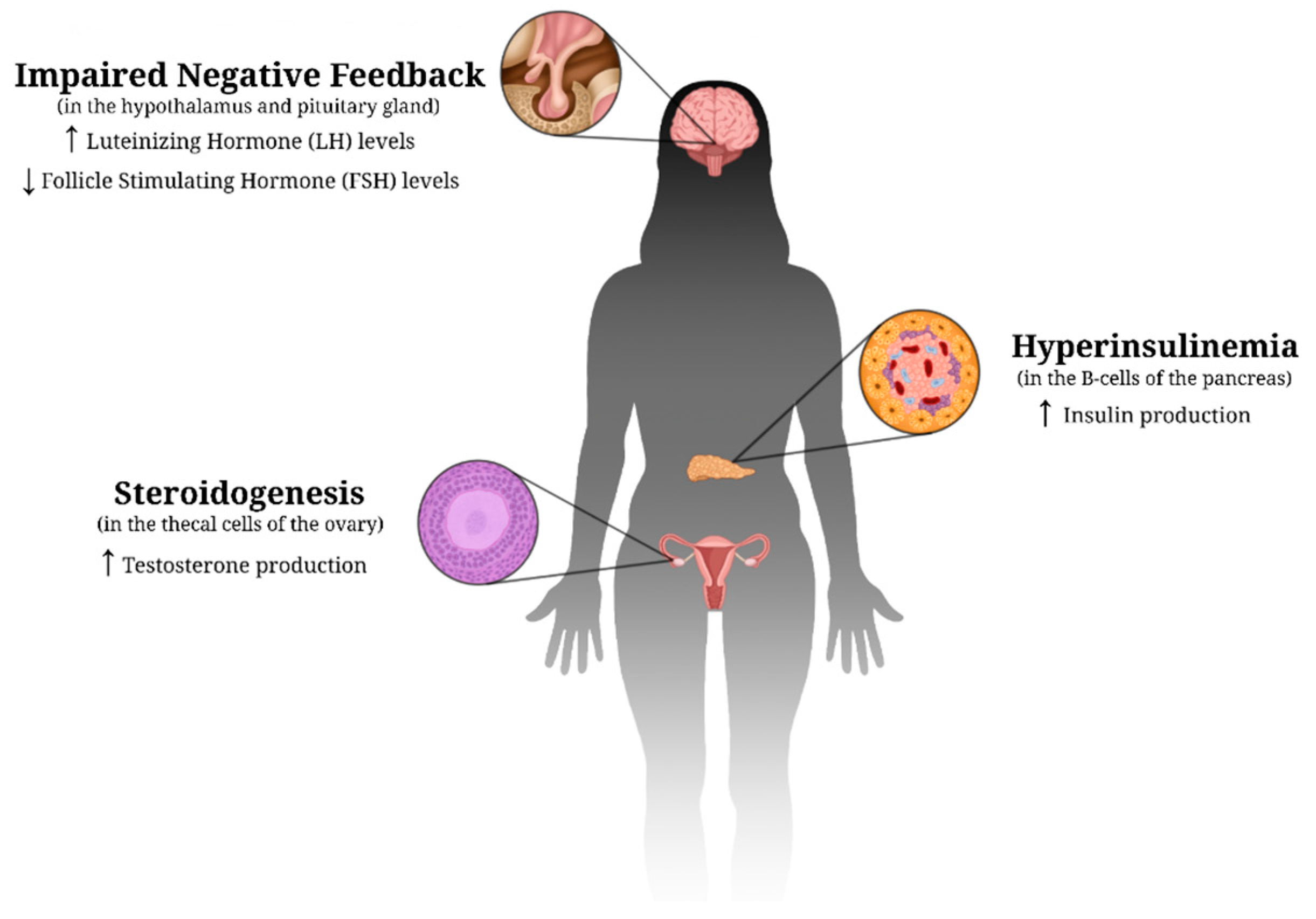
1. Introduction
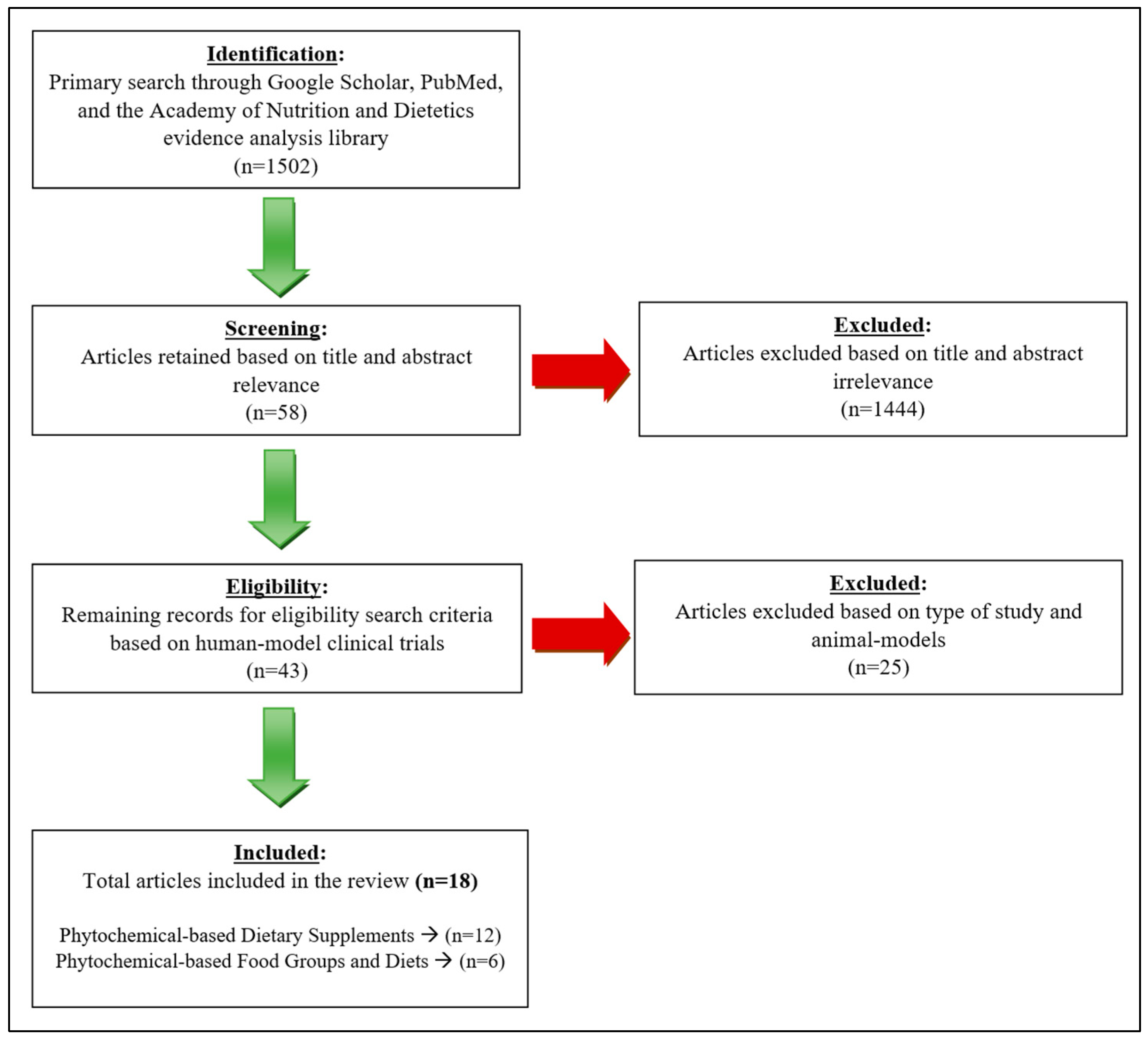
2. Methods
2.1. Participants, Length of Studies, and Treatment
2.2. Anthropometric Measurements
2.3. Biochemical Data
3. Results
4. Discussion
4.1. Phytochemical-Based Supplements and PCOS
4.2. Phytochemical-Based Food Groups/Diets and PCOS
4.3. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Centers for Disease Control and Prevention. PCOS (Polycystic Ovary Syndrome) and Diabetes; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2022. [Google Scholar]
- Wolf, W.M.; Wattick, R.A.; Kinkade, O.N.; Olfert, M.D. Geographical Prevalence of Polycystic Ovary Syndrome as Determined by Region and Race/Ethnicity. Int. J. Environ. Res. Public Health 2018, 15, 2589. [Google Scholar] [CrossRef] [PubMed]
- Deswal, R.; Narwal, V.; Dang, A.; Pundir, C.S. The Prevalence of Polycystic Ovary Syndrome: A Brief Systematic Review. J. Hum. Reprod. Sci. 2020, 13, 261–271. [Google Scholar]
- Rosenfield, R.L.; Ehrmann, D.A. The Pathogenesis of Polycystic Ovary Syndrome (PCOS): The Hypothesis of PCOS as Functional Ovarian Hyperandrogenism Revisited. Endocr. Rev. 2016, 37, 467–520. [Google Scholar] [CrossRef] [PubMed]
- Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome (PCOS). Hum. Reprod. 2004, 19, 41–47. [Google Scholar] [CrossRef]
- Xu, Y.; Qiao, J. Association of Insulin Resistance and Elevated Androgen Levels with Polycystic Ovarian Syndrome (PCOS): A Review of Literature. J. Healthc. Eng. 2022, 2022, 9240569. [Google Scholar] [CrossRef]
- Gainder, S.; Sharma, B. Update on Management of Polycystic Ovarian Syndrome for Dermatologists. Indian Dermatol. Online J. 2019, 10, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Marieb, E.N. Human Anatomy & Physiology, Student Edition, 10th ed.; Pearson: Boston, MA, USA, 2016. [Google Scholar]
- Genazzani, A.R.; Ibáñez, L.; Milewicz, A.; Shah, D. Impact of Polycystic Ovarian Syndrome, Metabolic Syndrome, and Obesity on Women’s Health; Anonymous, Ed.; Springer International Publishing AG: Cham, Switzerland, 2021. [Google Scholar]
- Moghetti, P.; Tosi, F. Insulin Resistance and PCOS: Chicken or Egg? J. Endocrinol. Invest. 2021, 44, 233–244. [Google Scholar] [CrossRef]
- Sanchez-Garrido, M.; Tena-Sempere, M. Metabolic Dysfunction in Polycystic Ovary Syndrome: Pathogenic Role of Androgen Excess and Potential Therapeutic Strategies. Mol. Metab. 2020, 35, 100937. [Google Scholar] [CrossRef]
- Bhatti, J.S.; Bhatti, G.K.; Reddy, P.H. Mitochondrial Dysfunction and Oxidative Stress in Metabolic Disorders—A Step Towards Mitochondria Based Therapeutic Strategies. BBA-Mol. Basis Dis. 2017, 1863, 1066–1077. [Google Scholar] [CrossRef]
- Victor, V.M.; Rovira-Llopis, S.; Bañuls, C.; Diaz-Morales, N.; De Marañon, A.M.; Rios-Navarro, C.; Alvarez, A.; Gomez, M.; Rocha, M.; Hernández-Mijares, A. Insulin Resistance in PCOS Patients Enhances Oxidative Stress and Leukocyte Adhesion: Role of Myeloperoxidase. PLoS ONE 2016, 11, e0151960. [Google Scholar] [CrossRef]
- Uçkan, K.; Demir, H.; Turan, K.; Sarıkaya, E.; Demir, C. Role of Oxidative Stress in Obese and Nonobese PCOS Patients. Int. J. Clin. Pract. 2022, 2022, 4579831. [Google Scholar] [CrossRef]
- Mansour, A.; Hosseini, S.; Larijani, B.; Mohajeri-Tehrani, M. Nutrients as Novel Therapeutic Approaches for Metabolic Disturbances in Polycystic Ovary Syndrome. EXCLI J. 2016, 15, 551–564. [Google Scholar] [PubMed]
- Rudnicka, E.; Suchta, K.; Grymowicz, M.; Calik-ksepka, A.; Smolarczyk, K.; Duszewska, A.M.; Smolarczyk, R.; Meczekalski, B. Chronic Low-Grade Inflammation in Pathogenesis of PCOS. Int. J. Mol. Sci. 2021, 22, 3789. [Google Scholar] [CrossRef] [PubMed]
- Xiong, Y.; Liang, X.; Yang, X.; Li, Y.; Wei, L. Low-Grade Chronic Inflammation in the Peripheral Blood and Ovaries of Women with Polycystic Ovarian Syndrome. Eur. J. Obstet. Gynecol. Reprod. Biol. 2011, 159, 148–150. [Google Scholar] [CrossRef] [PubMed]
- Dabravolski, S.A.; Nikiforov, N.G.; Eid, A.H.; Nedosugova, L.V.; Starodubova, A.V.; Popkova, T.V.; Bezsonov, E.E.; Orekhov, A.N. Mitochondrial Dysfunction and Chronic Inflammation in Polycystic Ovary Syndrome. Int. J. Mol. Sci. 2021, 22, 3923. [Google Scholar] [CrossRef]
- Zhang, Y.; Gan, R.; Li, S.; Zhou, Y.; Li, A.; Xu, D.; Li, H.; Kitts, D.D. Antioxidant Phytochemicals for the Prevention and Treatment of Chronic Diseases. Molecules 2015, 20, 21138–21156. [Google Scholar] [CrossRef]
- Iervolino, M.; Lepore, E.; Forte, G.; Laganà, A.S.; Buzzaccarini, G.; Unfer, V. Natural Molecules in the Management of Polycystic Ovary Syndrome (PCOS): An Analytical Review. Nutrients 2021, 13, 1677. [Google Scholar] [CrossRef]
- Tehrani, H.; Allahdadian, M.; Zarre, F.; Ranjbar, H.; Allahdadian, F. Effect of Green Tea on Metabolic and Hormonal Aspect of Polycystic Ovarian Syndrome in Overweight and Obese Women Suffering from Polycystic Ovarian Syndrome: A Clinical Trial. J. Educ. Health Promot. 2017, 6, 36. [Google Scholar]
- Mombaini, E.; Jafarirad, S.; Husain, D.; Haghighizadeh, M.H.; Padfar, P. The Impact of Green Tea Supplementation on Anthropometric Indices and Inflammatory Cytokines in Women with Polycystic Ovary Syndrome: Green Tea Effect on Anthropometric Indices and Cytokines. Phytother. Res. 2017, 31, 747–754. [Google Scholar] [CrossRef]
- Farhadian, M.; Barati, S.; Mahmoodi, M.; Barati Mosleh, A.; Yavangui, M. Comparison of Green Tea and Metformin Effects on Anthropometric Indicators in Women with Polycystic Ovarian Syndrome: A Clinical Trial Study. J. Rep. Pharm. Sci. 2020, 9, 97–103. [Google Scholar]
- Jamilian, M.; Foroozanfard, F.; Kavossian, E.; Aghadavod, E.; Shafabakhsh, R.; Hoseini, A.; Asemi, Z. Effects of Curcumin on Body Weight, Glycemic Control and Serum Lipids in Women with Polycystic Ovary Syndrome: A Randomized, Double-Blind, Placebo-Controlled Trial. Clin. Nutr. ESPEN 2020, 36, 128–133. [Google Scholar] [CrossRef]
- Heshmati, J.; Moini, A.; Sepidarkish, M.; Morvaridzadeh, M.; Salehi, M.; Palmowski, A.; Mojtahedi, M.F.; Shidfar, F. Effects of Curcumin Supplementation on Blood Glucose, Insulin Resistance and Androgens in Patients with Polycystic Ovary Syndrome: A Randomized Double-Blind Placebo-Controlled Clinical Trial. Phytomedicine 2021, 80, 153395. [Google Scholar] [CrossRef] [PubMed]
- Sohaei, S.; Amani, R.; Tarrahi, M.J.; Ghasemi-Tehrani, H. The Effects of Curcumin Supplementation on Glycemic Status, Lipid Profile and Hs-CRP Levels in Overweight/Obese Women with Polycystic Ovary Syndrome: A Randomized, Double-Blind, Placebo-Controlled Clinical Trial. Complement. Ther. Med. 2019, 47, 102201. [Google Scholar] [CrossRef] [PubMed]
- Khorshidi, M.; Moini, A.; Alipoor, E.; Rezvan, N.; Gorgani-Firuzjaee, S.; Yaseri, M.; Hosseinzadeh-Attar, M. The Effects of Quercetin Supplementation on Metabolic and Hormonal Parameters as Well as Plasma Concentration and Gene Expression of Resistin in Overweight or Obese Women with Polycystic Ovary Syndrome: Quercetin Supplementation and Resistin Level in PCOS. Phytother. Res. 2018, 32, 2282–2289. [Google Scholar] [CrossRef] [PubMed]
- Rezvan, N.; Moini, A.; Gorgani-Firuzjaee, S.; Hosseinzadeh-Attar, M. Oral Quercetin Supplementation Enhances Adiponectin Receptor Transcript Expression in Polycystic Ovary Syndrome Patients: A Randomized Placebo-Controlled Double-Blind Clinical Trial. Cell J. (Yakhteh) 2018, 19, 627–633. [Google Scholar]
- Banaszewska, B.; Wrotyńska-Barczyńska, J.; Spaczynski, R.Z.; Pawelczyk, L.; Duleba, A.J. Effects of Resveratrol on Polycystic Ovary Syndrome: A Double-Blind, Randomized, Placebo-Controlled Trial. J. Clin. Endocrinol. Metab. 2016, 101, 4322–4328. [Google Scholar] [CrossRef]
- Mansour, A.; Samadi, M.; Sanginabadi, M.; Gerami, H.; Karimi, S.; Hosseini, S.; Shirzad, N.; Hekmatdoost, A.; Mahdavi-Gorabi, A.; Mohajeri-Tehrani, M.; et al. Effect of Resveratrol on Menstrual Cyclicity, Hyperandrogenism and Metabolic Profile in Women with PCOS. Clin. Nutr. 2021, 40, 4106–4112. [Google Scholar] [CrossRef]
- Orio, F.; Muscogiuri, G.; Palomba, S.; Savastano, S.; Volpe, A.; Orio, M.; Colarieti, G.; La Sala, G.B.; Colao, A.; Marciano, F.; et al. Berberine improves reproductive features in obese Caucasian women with polycystic ovary syndrome independently of changes of insulin sensitivity. E-SPEN J. 2013, 8, e200–e204. [Google Scholar] [CrossRef]
- An, Y.; Sun, Z.; Zhang, Y.; Liu, B.; Guan, Y.; Lu, M. The use of Berberine for Women with Polycystic Ovary Syndrome Undergoing IVF Treatment. Clin. Endocrinol. 2014, 80, 425–431. [Google Scholar] [CrossRef]
- Esmaeilinezhad, Z.; Babajafari, S.; Sohrabi, Z.; Eskandari, M.-H.; Amooee, S.; Barati-Boldaji, R. Effect of Synbiotic Pomegranate Juice on Glycemic, Sex Hormone Profile and Anthropometric Indices in PCOS: A Randomized, Triple Blind, Controlled Trial. Nutr. Metab. Cardiovasc. Dis. 2019, 29, 201–208. [Google Scholar] [CrossRef]
- Abedini, M.; Ramezani-Jolfaie, N.; Ghasemi-Tehrani, H.; Tarrahi, M.J.; Amani, R. The Effect of Concentrated Pomegranate Juice on Biomarkers of Inflammation, Oxidative Stress, and Sex Hormones in Overweight and Obese Women with Polycystic Ovary Syndrome: A Randomized Controlled Trial. Phytother. Res. 2023, 37, 2255–2261. [Google Scholar] [CrossRef] [PubMed]
- Asemi, Z.; Esmaillzadeh, A. DASH Diet, Insulin Resistance, and Serum Hs-CRP in Polycystic Ovary Syndrome: A Randomized Controlled Clinical Trial. Horm. Metab. Res. 2015, 47, 232–238. [Google Scholar] [PubMed]
- Azadi-Yazdi, M.; Karimi-Zarchi, M.; Salehi-Abargouei, A.; Fallahzadeh, H.; Nadjarzadeh, A. Effects of Dietary Approach to Stop Hypertension Diet on Androgens, Antioxidant Status and Body Composition in Overweight and Obese Women with Polycystic Ovary Syndrome: A Randomised Controlled Trial. J. Hum. Nutr. Diet. 2017, 30, 275–283. [Google Scholar] [CrossRef] [PubMed]
- Foroozanfard, F.; Rafiei, H.; Samimi, M.; Gilasi, H.R.; Gorjizadeh, R.; Heidar, Z.; Asemi, Z. The Effects of Dietary Approaches to Stop Hypertension Diet on Weight Loss, anti-Müllerian Hormone and Metabolic Profiles in Women with Polycystic Ovary Syndrome: A Randomized Clinical Trial. Clin. Endocrinol. 2017, 87, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Mei, S.; Ding, J.; Wang, K.; Ni, Z.; Yu, J. Mediterranean Diet Combined with a Low-Carbohydrate Dietary Pattern in the Treatment of Overweight Polycystic Ovary Syndrome Patients. Front. Nutr. 2022, 9, 876620. [Google Scholar] [CrossRef]
- Hotchkiss, A.K.; Ostby, J.S.; Vandenburgh, J.G.; Gray, L.E., Jr. Androgens and environmental antiandrogens affect reproductive development and play behavior in the Sprague-Dawley rat. Environ. Heal. Perspect. 2002, 110 (Suppl 3), 435–439. [Google Scholar] [CrossRef]
- Ozgen Saydam, B.; Yildiz, B.O. Weight Management Strategies for Patients with PCOS: Current Perspectives. Expert Rev. Endocrinol. Metab. 2021, 16, 49–62. [Google Scholar] [CrossRef]
- Shahwan, M.; Alhumaydhi, F.; Ashraf, G.M.; Hasan, P.M.Z.; Shamsi, A. Role of Polyphenols in Combating Type 2 Diabetes and Insulin Resistance. Int. J. Biol. Macromol. 2022, 206, 567–579. [Google Scholar] [CrossRef]
- Kamal, D.A.M.; Salamt, N.; Zaid, S.S.M.; Mokhtar, M.H. Beneficial Effects of Green Tea Catechins on Female Reproductive Disorders: A Review. Molecules 2021, 26, 2675. [Google Scholar] [CrossRef]
- Maleki, V.; Taheri, E.; Varshosaz, P.; Tabrizi, F.P.F.; Moludi, J.; Jafari-Vayghan, H.; Shadnoush, M.; Jabbari, S.H.Y.; Seifoleslami, M.; Alizadeh, M. A Comprehensive Insight into Effects of Green Tea Extract in Polycystic Ovary Syndrome: A Systematic Review. Reprod. Biol. Endocrinol. 2021, 19, 147. [Google Scholar] [CrossRef]
- Venkatesan, K.; Menon, S.; Firoz, I.N.; Narendrula, R.; Kunnath, J.T.; Kalapurakal, A.M.; Nigil Haroon, N.; Iqbal, A.M.; Ashok, A. Complementary Administration of Curcumin in PCOS: A Systematic Review. Minerva Obstet. Gynecol. 2022, 75, 379–386. [Google Scholar] [CrossRef] [PubMed]
- Bozkurt, O.; Kocaadam-Bozkurt, B.; Yildiran, H. Effects of Curcumin, a Bioactive Component of Turmeric, on Type 2 Diabetes Mellitus and its Complications: An Updated Review. Food Funct. 2022, 13, 11999–12010. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Wang, L.; Weng, Y.; Wang, D.; Wang, R.; Wang, H.; Wang, L.; Shen, S.; Li, Y.; Wang, Y. Curcumin Inhibits Hyperandrogen-Induced IRE1α-XBP1 Pathway Activation by Activating the PI3K/AKT Signaling in Ovarian Granulosa Cells of PCOS Model Rats. Oxidative Med. Cell. Longev. 2022, 2022, 2113293. [Google Scholar] [CrossRef]
- Saadia, Z. Follicle Stimulating Hormone (LH: FSH) Ratio in Polycystic Ovary Syndrome (PCOS)—Obese Vs. Non-Obese Women. Med Arch. 2020, 74, 289–293. [Google Scholar] [CrossRef] [PubMed]
- Pourteymour Fard Tabrizi, F.; Hajizadeh-Sharafabad, F.; Vaezi, M.; Jafari-Vayghan, H.; Alizadeh, M.; Maleki, V. Quercetin and Polycystic Ovary Syndrome, Current Evidence and Future Directions: A Systematic Review. J. Ovarian Res. 2020, 13, 11. [Google Scholar] [CrossRef] [PubMed]
- Ma, C.; Xiang, Q.; Song, G.; Wang, X. Quercetin and Polycystic Ovary Syndrome. Front. Pharmacol. 2022, 13, 1006678. [Google Scholar] [CrossRef]
- Liang, A.; Huang, L.; Liu, H.; He, W.; Lei, X.; Li, M.; Li, S.; Liang, H.; Chen, G.; Tang, J.; et al. Resveratrol Improves Follicular Development of PCOS Rats by Regulating the Glycolytic Pathway. Mol. Nutr. Food Res. 2021, 65, 2100457. [Google Scholar] [CrossRef]
- Shojaei-Zarghani, S.; Rafraf, M. Resveratrol and Markers of Polycystic Ovary Syndrome: A Systematic Review of Animal and Clinical Studies. Reprod. Sci. 2022, 29, 2477–2487. [Google Scholar] [CrossRef]
- Mishra, N.; Verma, R.; Jadaun, P. Study on the Effect of Berberine, Myoinositol, and Metformin in Women with Polycystic Ovary Syndrome: A Prospective Randomised Study. Curēus 2022, 14, e21781. [Google Scholar] [CrossRef]
- Wang, Z.; Nie, K.; Su, H.; Tang, Y.; Wang, H.; Xu, X.; Dong, H. Berberine Improves Ovulation and Endometrial Receptivity in Polycystic Ovary Syndrome. Phytomedicine 2021, 91, 153654. [Google Scholar] [CrossRef]
- Vučić, V.; Grabež, M.; Trchounian, A.; Arsić, A. Composition and Potential Health Benefits of Pomegranate: A Review. Curr. Pharm. Des. 2019, 25, 1817–1827. [Google Scholar] [CrossRef]
- Ibrahim, M.A.A.; Sadek, M.T.; Sharaf Eldin, H.E.M. Role of Pomegranate Extract in Restoring Endometrial Androgen Receptor Expression, Proliferation, and Pinopodes in a Rat Model of Polycystic Ovary Syndrome. Morphologie 2022, 106, 145–154. [Google Scholar] [CrossRef]
- Medjakovic, S.; Jungbauer, A. Pomegranate: A Fruit that Ameliorates Metabolic Syndrome. Food Funct. 2013, 4, 19–39. [Google Scholar] [CrossRef]
- Appel, L.J.; Moore, T.J.; Obarzanek, E.; Vollmer, W.M.; Svetkey, L.P.; Sacks, F.M.; Bray, G.A.; Vogt, T.M.; Cutler, J.A.; Windhauser, M.M.; et al. A Clinical Trial of the Effects of Dietary Patterns on Blood Pressure. DASH Collaborative Research Group. N. Engl. J. Med. 1997, 336, 1117–1124. [Google Scholar] [CrossRef] [PubMed]
- Shang, Y.; Zhou, H.; Hu, M.; Feng, H. Effect of Diet on Insulin Resistance in Polycystic Ovary Syndrome. J. Clin. Endocrinol. Metab. 2020, 105, 3346–3360. [Google Scholar] [CrossRef] [PubMed]
- Daneshzad, E.; Heshmati, J.; Basirat, V.; Keshavarz, S.; Qorbani, M.; Larijani, B.; Bellissimo, N.; Azadbakht, L. The Effect of the Dietary Approaches to Stop Hypertension (DASH) Diet on Sleep, Mental Health, and Hormonal Changes: A Randomized Clinical Trial in Women with Type 2 Diabetes. Front. Nutr. 2022, 9, 775543. [Google Scholar] [CrossRef] [PubMed]
- Liu, N.; Feng, Y.; Luo, X.; Ma, X.; Ma, F. Association between Dietary Inflammatory Index and Sex Hormone Binding Globulin and Sex Hormone in U.S. Adult Females. Front. Public Health 2022, 10, 802945. [Google Scholar] [CrossRef]
- Xing, C.; Zhang, J.; Zhao, H.; He, B. Effect of Sex Hormone-Binding Globulin on Polycystic Ovary Syndrome: Mechanisms, Manifestations, Genetics, and Treatment. Int. J. Women’s Health 2022, 14, 91–105. [Google Scholar] [CrossRef] [PubMed]
- Martínez-González, M.A.; Salas-Salvadó, J.; Estruch, R.; Corella, D.; Fitó Colomer, M.; Ros, E.; Predimed Investigators. Benefits Mediterr. Diet: Insights PREDIMED Study. Prog. Cardiovasc. Dis. 2015, 58, 50–60. [Google Scholar] [CrossRef] [PubMed]
- Kazemi, M.; Jarrett, B.Y.; Vanden Brink, H.; Lin, A.W.; Hoeger, K.M.; Spandorfer, S.D.; Lujan, M.E. Obesity, Insulin Resistance, and Hyperandrogenism Mediate the Link between Poor Diet Quality and Ovarian Dysmorphology in Reproductive-Aged Women. Nutrients 2020, 12, 1953. [Google Scholar] [CrossRef]
- Barrea, L.; Arnone, A.; Annunziata, G.; Muscogiuri, G.; Laudisio, D.; Salzano, C.; Pugliese, G.; Colao, A.; Savastano, S. Adherence to the Mediterranean Diet, Dietary Patterns and Body Composition in Women with Polycystic Ovary Syndrome (PCOS). Nutrients 2019, 11, 2278. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Phytochemical Compound | Author/Year | PCOS Duration, Sample Size, and Treatment Plan | Significant Findings (p < 0.05) |
|---|---|---|---|
| EGCG | (Tehrani, 2017) [21] | 3 months Overweight and obese women 20–40 years old (n = 60) Tx: One 500 mg green tea tablet per day |
|
| (Mombaini, 2017) [22] | 45 days Women aged 18–55 years with BMI 20–35 kg/m2 (n = 45) Tx: One 500 mg green tea leaf powder tablet per day |
| |
| (Farhadian, 2020) [23] | 3 months Overweight women 18–35 years old (n = 15) Tx: One 500 mg green tea leaf powder tablet per day |
| |
| Curcumin | (Jamilian, 2020) [24] | 3 months Women aged 18–40 (n = 60) Tx: 500 mg/day curcumin |
|
| (Heshmati, 2020) [25] | 3 months Women aged 18–49 (n = 67) Tx: 500 mg curcumin powder in a capsule 3 times/day |
| |
| (Sohaei, 2019) [26] | 6 weeks Women aged 18–40 years old (n = 27) Tx: 500 mg curcumin 2 times/day |
| |
| Quercetin | (Khorshidi, 2018) [27] | 3 months Women with BMI 25–40 kg/m2, aged 20–40 (n = 27) Tx: 1000 mg quercetin per day |
|
| (Rezvan, 2018) [28] | 3 months Overweight or obese women, mean age 29 (n = 42) Tx: Two 500 mg capsules of quercetin daily |
| |
| Resveratrol | (Banaszewska, 2016) [29] | 3 months Overweight women (n = 15) Tx: micronized transresveratrol; 1500 mg/day |
|
| (Mansour, 2021) [30] | 3 months Women aged 18–40 (n = 39) Tx: 1000 mg resveratrol/day |
| |
| Berberine | (Orio, 2013) [31] | 6 months Obese women (n = 50) Tx: 588 mg Berberis aristate and 105 mg of Silybum marianum—1 tablet, 2 times/day |
|
| (An, 2014) [32] | 3 months Overweight women (n = 41) Tx: Berberine tablets 500 mg, 3 times/day |
|
| Food Groups | Author/Year | PCOS Duration, Sample Size, and Treatment Plan | Significant Findings (p < 0.05) |
|---|---|---|---|
| Pomegranate juice | (Esmaeilinezhad, 2019) [33] | 8 weeks PCOS women aged 15–48 (n = 23) Tx: 2 L of pomegranate juice per week |
|
| (Abedini, 2023) [34] | 8 weeks Overweight and obese women with PCOS aged 18–40 (n = 21) Tx: 45 mL of concentrated pomegranate juice + 180 mL H2O per day |
| |
| Diets | Author/Year | PCOS Duration, Sample Size, and Treatment Plan | Significant Findings (p < 0.05) |
| DASH diet | (Asemi, 2015) [35] | 8 weeks Overweight and obese women with PCOS (n = 23) Tx: DASH diet (52% carbs, 18% protein, and 30% total fat) |
|
| (Azadi-Yazdi, 2017) [36] | 3 months Obese and overweight women with PCOS aged 20–40 (n = 28) Tx: DASH diet (50–55% carbs, 15–20% protein, and 25–30% total fat) |
| |
| (Foroozanfard, 2017) [37] | 3 months Overweight and obese women with PCOS (n = 30) Tx: Low calorie DASH diet (52–55% carbs, 16–18% protein, and 30% total fat) |
| |
| Mediterranean Diet | (Mei, 2022) [38] | 3 months Overweight women (n = 30) Tx: low carb (<20%) MED diet |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chavez, G.N.; Jaworsky, K.; Basu, A. The Effects of Plant-Derived Phytochemical Compounds and Phytochemical-Rich Diets on Females with Polycystic Ovarian Syndrome: A Scoping Review of Clinical Trials. Int. J. Environ. Res. Public Health 2023, 20, 6534. https://doi.org/10.3390/ijerph20156534
Chavez GN, Jaworsky K, Basu A. The Effects of Plant-Derived Phytochemical Compounds and Phytochemical-Rich Diets on Females with Polycystic Ovarian Syndrome: A Scoping Review of Clinical Trials. International Journal of Environmental Research and Public Health. 2023; 20(15):6534. https://doi.org/10.3390/ijerph20156534
Chicago/Turabian StyleChavez, Guadalupe Nayeli, Kataryna Jaworsky, and Arpita Basu. 2023. "The Effects of Plant-Derived Phytochemical Compounds and Phytochemical-Rich Diets on Females with Polycystic Ovarian Syndrome: A Scoping Review of Clinical Trials" International Journal of Environmental Research and Public Health 20, no. 15: 6534. https://doi.org/10.3390/ijerph20156534
APA StyleChavez, G. N., Jaworsky, K., & Basu, A. (2023). The Effects of Plant-Derived Phytochemical Compounds and Phytochemical-Rich Diets on Females with Polycystic Ovarian Syndrome: A Scoping Review of Clinical Trials. International Journal of Environmental Research and Public Health, 20(15), 6534. https://doi.org/10.3390/ijerph20156534