
Reimagining the Role of Health Departments and Their Partners in Addressing Climate Change: Revising the Building Resilience against Climate Effects (BRACE) Framework

 ,
, 

{kind=link}
{kind=link}
Abstract
1. Introduction
1.1. The Role of Public Health in Addressing Climate Change
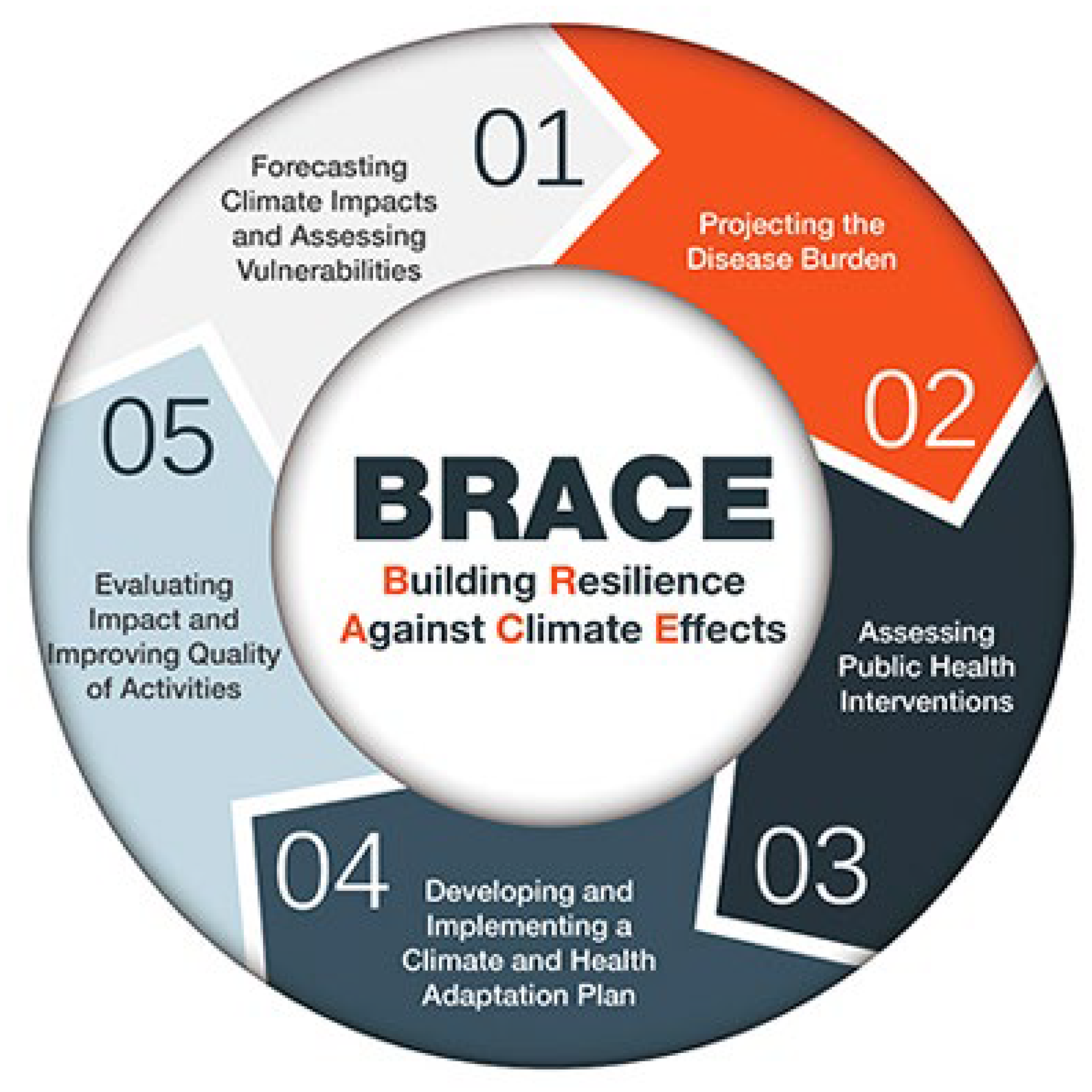
1.2. The Building Resilience against Climate Effects (BRACE) Framework
- Step 1: Anticipate Climate Impacts and Assess Vulnerabilities
- Step 2: Project the Disease Burden
- Step 3: Assess Public Health Interventions
- Step 4: Develop and Implement a Climate and Health Adaptation Plan
- Step 5: Evaluate Impact and Improve Quality of Activities
1.3. Identified Gaps with BRACE Framework
1.4. Aim
2. Methods
2.1. Planned Revisions to the BRACE Framework
2.1.1. Alignment with Public Health 3.0
2.1.2. Emphasis on Health Equity
2.1.3. Inclusion of Climate Change Mitigation Strategies
2.1.4. Application to Diverse Settings
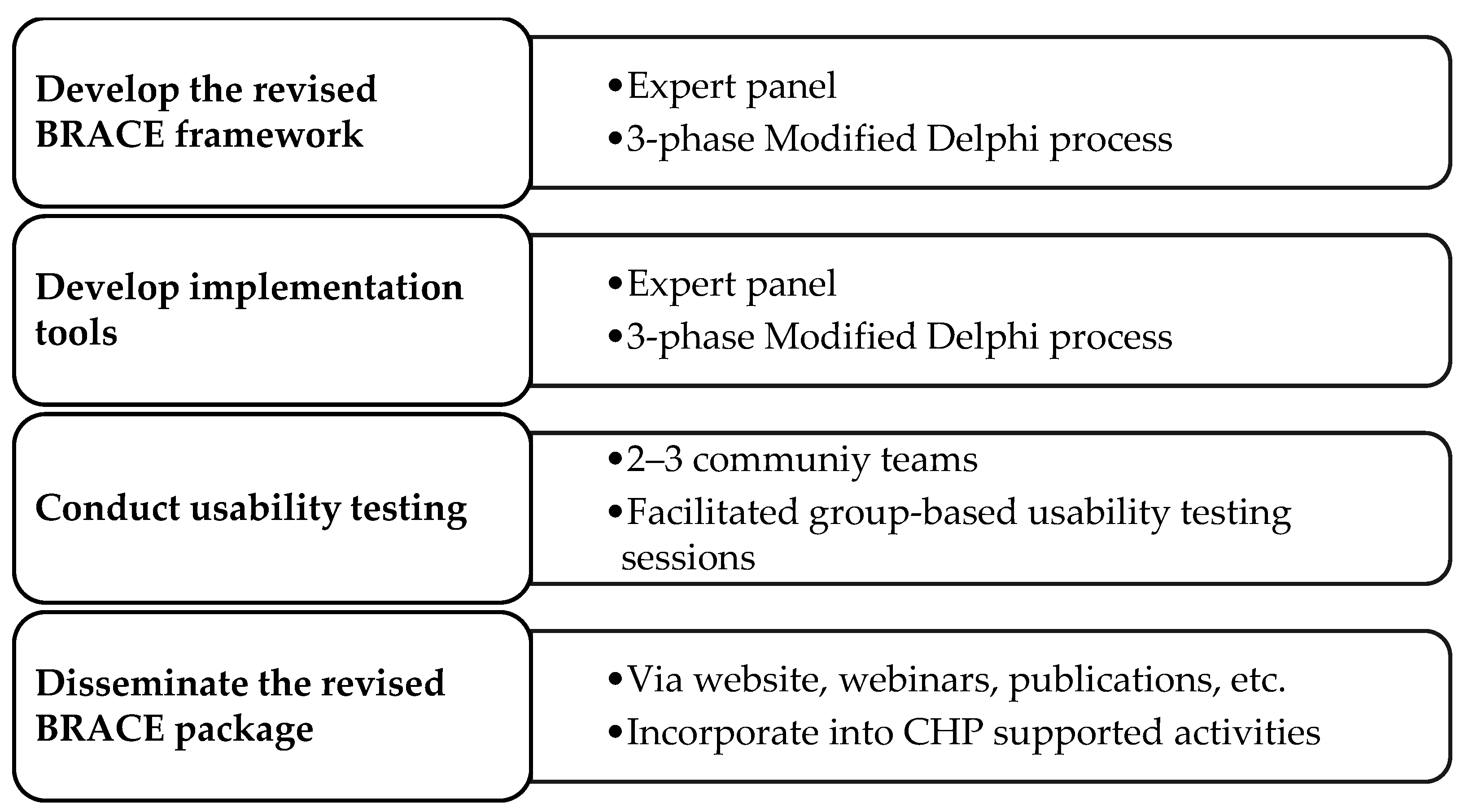
2.2. Methodology to Revise the BRACE Framework and Create Implementation Tools
2.2.1. Expert Panel
2.2.2. Approach to Creating the Revised BRACE Framework
2.2.3. Approach to Creating Implementation Tools
2.2.4. Usability Testing
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- United Nations. Climate Change ‘Biggest Threat Modern Humans Have Ever Faced’. World-Renowned Naturalist Tells Security Council. Calls for Greater Global Cooperation. Available online: https://www.un.org/press/en/2021/sc14445.doc.htm (accessed on 28 June 2023).
- Watts, N.; Amann, M.; Arnell, N.; Ayeb-Karlsson, S.; Beagley, J.; Belesova, K.; Boykoff, M.; Byass, P.; Cai, W.; Campbell-Lendrum, D. The 2020 report of The Lancet Countdown on health and climate change: Responding to converging crises. Lancet 2021, 397, 129–170. [Google Scholar] [CrossRef] [PubMed]
- Swinburn, B.A.; Kraak, V.I.; Allender, S.; Atkins, V.J.; Baker, P.I.; Bogard, J.R.; Brinsden, H.; Calbillo, A.; De Schutter, O.; Devarajan, R. The global syndemic of obesity, undernutrition, and climate change: The Lancet Commission report. Lancet 2019, 393, 791–846. [Google Scholar] [CrossRef]
- Rocque, R.J.; Beaudoin, C.; Ndjaboue, R.; Cameron, L.; Poirier-Bergeron, L.; Poulin-Rhealt, R.A.; Fallon, C.; Tricco, A.C.; Witterman, H.O. Health effects of climate change: An overview of systematic reviews. BMJ Open 2021, 11, e046333. [Google Scholar] [CrossRef]
- Patz, J.A.; Frumkin, H.; Holloway, T.; Vimont, D.J.; Haines, A. Climate change: Challenges and opportunities for global health. JAMA 2014, 312, 1565–1580. [Google Scholar] [CrossRef] [PubMed]
- Romanello, M.; McGushin, A.; DiNapoli, C.; Drummond, P.; Hughes, N.; Jamart, L.; Kennard, H.; Lampard, P.; Rodriguez, B.S.; Arnell, N.; et al. The 2021 report of the Lancet Countdown on health and climate change: Code red for a healthy future. Lancet 2021, 398, 1619–1662. [Google Scholar] [CrossRef]
- Berberian, A.G.; Gonzalez, D.J.X.; Cushing, L.J. Racial disparities in climate change-related health effects in the United States. Curr. Envir. Health Rpt. 2022, 9, 451–464. [Google Scholar] [CrossRef]
- Clayton, S. Climate anxiety: Psychological responses to climate change. J. Anxiety Disord. 2020, 74, 102263. [Google Scholar] [CrossRef]
- Davenport, L. Emotional Resiliency in the Era of Climate Change: A Clinician’s Guide; Jessica Kingsley Publishers: Philadelphia, PA, USA; London, UK, 2017. [Google Scholar]
- Zang, S.M.; Benjenk, I.; Breakey, S.; Pusey-Reid, E.; Nicholas, P.K. The intersection of climate change with the era of COVID-19. Public Health Nurs. 2021, 38, 321–335. [Google Scholar] [CrossRef] [PubMed]
- American Security Project. Current Recap: Climate Change as a Threat Multiplier. Available online: https://www.americansecurityproject.org/event-recap-climate-change-as-a-threat-multiplier (accessed on 5 July 2023).
- Rossiello, M.R.; Szema, A. Health effects of climate change-induced wildfires and heatwaves. Cureus 2019, 11, e4771. [Google Scholar] [CrossRef] [PubMed]
- Salvador, C.; Nieto, R.; Vicente-Serrano, S.M.; García-Herrera, R.; Gimeno, L.; Vicedo-Cabrera, A.M. Public health implications of drought in a climate change context: A critical review. Annu. Rev. Public Health 2023, 44, 213–232. [Google Scholar] [CrossRef] [PubMed]
- Ebi, K.L.; Vanos, J.; Baldwin, J.W.; Bell, J.E.; Hondula, D.M.; Errett, N.A.; Hayes, K.; Reid, C.E.; Saha, S.; Spector, J.; et al. Extreme weather and climate change: Population health and health system implications. Annu. Rev. Public Health 2021, 42, 293–315. [Google Scholar] [CrossRef]
- Kirshen, P.; Burdick, D.; Aytur, S.; Lippmann, T.; Nick, S.; Watson, C. Protecting the build environment in a barrier beach and marsh system: A case study of the Hampton-Seabrook estuary, New Hampshire. Shore Beach 2023, 91, 29. [Google Scholar]
- Limaye, V. The Costs of Inaction: The Economic Burden of Fossil Fuels and Climate Change on Health in the United States. Available online: https://www.nrdc.org/sites/default/files/costs-inaction-burden-health-report.pdf (accessed on 22 February 2023).
- Levy, B.S.; Patz, J.A. Climate change, human rights, and social justice. Ann. Glob. Health 2015, 81, 310–322. [Google Scholar] [CrossRef] [PubMed]
- Benmarhnia, T.; Desuen, S.; Kaufman, J.S.; Smargiassi, A. A review article: Vulnerability to heat-related mortality: A systematic review, meta-analysis, and meta-regression analysis. Epidemiology 2015, 26, 781–793. [Google Scholar] [CrossRef]
- Reidmiller, D.R.; Avery, C.W.; Easterling, D.R.; Kukel, K.E.; Lewis, K.L.M.; Maycock, T.K.; Stewart, B.C.L. Impacts, risks, and adaptation in the United States: The Fourth National Climate Assessment; Volume II. Available online: https://nca2018.globalchange.gov/ (accessed on 3 July 2023).
- Li, Y.; Odame, E.A.; Silver, K.; Zheng, S. Comparing urban and rural vulnerability to heat-related mortality: A systematic review and meta-analysis. J. Glob. Epidemiol. Environ. Health 2017, 9–15. [Google Scholar] [CrossRef]
- Benevolenza, M.A.; DeRigne, L. The impact of climate change and natural disasters on vulnerable populations: A systematic review. J. Soc. Behav. Sci. 2019, 29, 266–281. [Google Scholar] [CrossRef]
- Albright, K.; Shah, P.; Santodomingo, M.; Scandlyn, J. Dissemination of information about climate change by State and Local Public Health Departments: United States, 2019–2020. Am. J. Public Health 2020, 110, 1184–1190. [Google Scholar] [CrossRef]
- Schramm, P.J.; Cordero, A.; Protzel Berman, P.; McCoy, T.; Gaines, C.; Svendsen, E.; Malilay, J.; Yip, F.; Sarisky, J.; Allwood, P.; et al. Building a comprehensive approach in CDC’s national center for environmental health to address the health effects of climate change. J. Clim. Change Health 2021, 4, 100071. [Google Scholar] [CrossRef]
- American Public Health Association, Why Is Climate Change a Public Health Issue? Available online: https://www.apha.org/Topics-and-Issues/Climate-Change (accessed on 23 February 2023).
- World Health Organization, Climate Change & Health. Available online: https://aspph.org/advocacy/climate-change-health/ (accessed on 12 January 2023).
- Association of State and Territorial Health Organizations, Climate and Health. Available online: https://www.astho.org/topic/environmental-health/climate/ (accessed on 12 February 2023).
- National Association of County and City Health Officials, Climate Change. Available online: https://www.naccho.org/programs/environmental-health/hazards/climate-change (accessed on 12 February 2023).
- Schramm, P.J.; Ahmed, M.; Siegel, H.; Donatuto, J.; Campbell, L.; Raab, K.; Svendsen, E. Climate change and health: Local solutions to local challenges. Curr. Environ. Health Rep. 2020, 7, 363–370. [Google Scholar] [CrossRef] [PubMed]
- Roser-Renouf, C.; Maibach, E.W.; Li, J. Adapting to the changing climate: An assessment of local health department preparations for climate change-related health threats, 2008–2012. PLoS ONE 2016, 11, e0151558. [Google Scholar] [CrossRef] [PubMed]
- Fox, M.; Zuidema, C.; Bauman, B.; Burke, T.; Sheehan, M. Integrating public health into climate change policy and planning: State of practice update. Int. J. Environ. Res. Public Health 2019, 16, 3232. [Google Scholar] [CrossRef] [PubMed]
- Maibach, E.W.; Chadwick, A.; McBride, D.; Chuk, M.; Ebi, K.L.; Balbus, J. Climate change and local public health in the United States: Preparedness, programs and perceptions of local public health department directors. PLoS ONE 2008, 3, e2838. [Google Scholar] [CrossRef]
- Maani, N.; Galea, S. COVID-19 and underinvestment in the public health infrastructure of the United States. Milbank Q. 2020, 98, 250–259. [Google Scholar] [CrossRef] [PubMed]
- Errett, N.A.; Dolan, K.; Hartwell, C.; Vickery, J.; Hess, J.J. Climate change adaptation activities and needs in US state and territorial health agencies. J. Public Health Manag. Pract. 2023, 29, E115–E123. [Google Scholar] [CrossRef]
- Aylett, A. Institutionalizing the urban governance of climate change adaptation: Results of an international survey. Urban Clim. 2015, 14, 4–16. [Google Scholar] [CrossRef]
- Eckkstrom, J.A.; Moser, S.C. Identifying and overcoming barriers in urban climate adaptation: Case study findings from the San Francisco Bay Area, California, USA. Urban Clim. 2014, 9, 54–74. [Google Scholar] [CrossRef]
- Himmelstein, D.U.; Woolhandler, S. Public health’s falling share of US health spending. Am. J. Public Health 2016, 106, 56–57. [Google Scholar] [CrossRef] [PubMed]
- Mallen, E.; Joseph, H.A.; McLaughlin, M.; English, D.Q.; Olmedo, C.; Roach, M.; Tirdea, C.; Vargo, J.; Wolff, M.; York, E. Overcoming barriers to successful climate and health adaptation practice: Notes from the field. Int. J. Environ. Res. Public Health 2022, 19, 7169. [Google Scholar] [CrossRef]
- Pendrey, C.G.; Quilty, S.; Gruen, R.L.; Weeramanthri, T.; Lucas, R.M. Is climate change exacerbating health-care workforce shortages for underserved populations? Lancet Planet Health 2021, 5, e183–e184. [Google Scholar] [CrossRef]
- Rosenstock, L.; Silver, G.B.; Helsing, K.; Evashwick, C.; Katz, R.; Klag, M.; Kominski, G.; Richter, D.; Sumaya, C. Confronting the public health workforce crisis: ASPH statement on the public health workforce. Public Health Rep. 2008, 123, 395–398. [Google Scholar] [CrossRef]
- Caron, R.M.; Aytur, S.; Foster, H. The Institute of Medicine’s call to action revisited: Assuring access to public health education for U.S. college students. Front. Pub. Health 2023, 11, 1185845. [Google Scholar] [CrossRef] [PubMed]
- McCarney, P.; Blanco, H.; Carmin, J.; Colley, M. Cities and climate change. In Climate Change and Cities: First Assessment Report of the Urban Climate Change Research Network; Rosenzweig, C., Solecki, W.D., Hammer, S.A., Mehrota, S., Eds.; Cambridge University Press: Cambridge, UK, 2011; pp. 249–269. [Google Scholar]
- Sheehan, M.C.; Fox, M.A.; Kaye, C.; Resnick, B. Integrating health into local climate response: Lessons from the U.S. CDC Climate-Ready States and Cities Initiative. Environ. Health Perspect. 2017, 125, 094501. [Google Scholar] [CrossRef] [PubMed]
- The CDC Foundation, Assessment of Local Public Health Department Capacity to Adapt to Climate Change and Build Community Partnerships to Protect Public Health. Available online: https://www.cdcfoundation.org/sites/default/files/2020-10/ClimateHealth-Full-Report.pdf (accessed on 24 January 2023).
- NACCHO, Are We Ready? Report 2. Preparing for the Public Health Challenges of Climate Change. Available online: https://www.naccho.org/uploads/downloadable-resources/NA609PDF-AreWeReady2.pdf (accessed on 24 January 2023).
- Marinucci, G.D.; Luber, G.; Uejio, C.K.; Saha, S.; Hess, J.J. Building resilience against climate effects-A novel framework to facilitate climate readiness in public health agencies. Int. J. Environ. Res. Public Health 2014, 11, 6433–6458. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention, CRSCI Grant Recipients. Available online: https://www.cdc.gov/climateandhealth/crsci_grantees.htm (accessed on 1 July 2023).
- Centers for Disease Control and Prevention, Climate and Health Technical Report Series. Available online: https://www.cdc.gov/climateandhealth/docs/exposureresponsefunctions_508.pdf (accessed on 24 January 2023).
- American Public Health Association. Climate Change and Health Playbook: Adaptation Planning for Justice, Equity, Diversity and Inclusion. Available online: https://apha.org/climate/JEDI (accessed on 24 January 2023).
- Schramm, P.J.; Al Janabi, A.L.; Campbell, L.W.; Donatuto, J.L.; Gaughen, S.C. How indigenous communities are adapting to climate change: Insights from The Climate-Ready Tribes Initiative. Health Aff. 2020, 38, 2153–2159. [Google Scholar] [CrossRef]
- Joseph, H.A.; Mallen, E.; McLaughlin, M.; Grossman, E.; Joseph Holmes, T.; Locklear, A.; Powell, E.; Thie, L.; Uejio, C.; Vacca, K. Evaluating public health strategies for climate adaptation: Challenges and opportunities from the climate ready states and cities initiative. PLoS Clim. 2023, 2, e000012. [Google Scholar] [CrossRef]
- Hartwell, C.; Lovell, S.; Hess, J.J.; Dolan, K.; Vickery, J.; Errett, N.A. Barriers and facilitators to state public health agency climate and health action: A qualitative assessment. BMC Public Health 2023, 23, 145. [Google Scholar] [CrossRef]
- DeSalvo, K.B.; Wang, Y.C.; Harris, A.; Auerbach, J.; Koo, D.; O’Carroll, P. Public Health 3.0: A call to action for public health to meet the challenges of the 21st Century. Prev. Chronic Dis. 2017, 14, E78. [Google Scholar] [CrossRef]
- Quam, V.G.M.; Rocklov, J.; Quam, M.B.M.; Lucas, R.A.I. Assessing greenhouse gas emissions and health co-benefits: A structured review of lifestyle-related climate change mitigation strategies. Int. J. Envrion. Res. Public Health 2017, 14, 468. [Google Scholar] [CrossRef]
- Beebe, J. Rapid Qualitative Inquiry: A Field Guide to Team-Based Assessment, 2nd ed.; Rowman & Littlefield: Lanham, MD, USA, 2014. [Google Scholar]
- Landeta, J. Current validity of the Delphi method in social sciences. Technol. Forecast. Soc. Change 2006, 73, 467–482. [Google Scholar] [CrossRef]
- Taylor, B.; Henshall, C.; Kenyon, S.; Litchfield, I.; Greenfield, S. Can rapid approaches to qualitative analysis deliver timely, valid findings to clinical leaders? A mixed methods study comparing rapid and thematic analysis. BMJ Open 2018, 8, e019993. [Google Scholar] [CrossRef]
- Palinkas, L.A.; Mendon, S.J.; Hamilton, A.B. Innovations in mixed methods evaluations. Annu. Rev. Public Health 2019, 40, 423–442. [Google Scholar] [CrossRef]
- Joosten, Y.A.; Israel, T.L.; Williams, N.A.; Boone, L.R.; Schlundt, D.G.; Mouton, C.P.; Dittus, R.S.; Bernard, G.R.; Wilkins, C.H. Community Engagement Studios: A structured approach to obtaining meaningful input from stakeholders to inform research. Acad. Med. 2015, 90, 1646–1650. [Google Scholar] [CrossRef] [PubMed]
- Joosten, Y.A.; Israel, T.L.; Head, A.; Vaughn, Y.; Gil, V.V.; Mouton, C.; Wilkins, C.H. Enhancing translational researchers’ ability to collaborate with community stakeholders: Lessons from the Community Engagement Studio. J. Clin. Transl. Sci. 2018, 2, 201–207. [Google Scholar] [CrossRef] [PubMed]
- Weiner, B.J.; Lewis, C.C.; Stanick, C.; Powell, B.J.; Dorsey, C.N.; Clary, A.S.; Boynton, M.H.; Halko, H. Psychometric assessment of three newly developed implementation outcome measures. Implement. Sci. 2017, 12, 108. [Google Scholar] [CrossRef]
- Van de Ven, A.H.; Delbecq, A.L. The nominal group as a research instrument for exploratory health studies. Am. J. Public Health 1972, 62, 337–342. [Google Scholar] [CrossRef]
- Fernandez, M.E.; Ten Hoor, G.A.; van Lieshout, S.; Rodriguez, S.A.; Beidas, R.S.; Parcel, G.; Ruiter, R.A.C.; Markham, C.M.; Kok, G. Implementation mapping: Using intervention mapping to develop implementation strategies. Front. Public Health 2019, 7, 158. [Google Scholar] [CrossRef] [PubMed]
- Wandersman, A.; Duffy, J.; Flaspohler, P.D.; Noonan, R.; Lubell, K.; Stillman, L.; Blachman, M.; Dunville, R.; Saul, J. Bridging the gap between prevention research and practice: The interactive systems framework for dissemination and implementation. Am. J. Community Psychol. 2008, 41, 171–181. [Google Scholar] [CrossRef] [PubMed]
- Barnum, C.M. Usability Testing Essentials: Ready, Set... Test! 2nd ed.; Morgan Kaufmann: Cambridge, MA, USA, 2020. [Google Scholar]
- Hessburg, P.F.; Prichard, S.J.; Hagmann, K.; Povak, N.A.; Lake, F.K. Wildfire and climate change adaptation of western North American forests: A case for intentional management. Ecol. Adapt. 2021, 31, e02432. [Google Scholar] [CrossRef]
- U.S. Department of Agriculture. 2017; A Synopsis of Presentations and Ideas from the Drought Adaptation Workshop in Region 8. Available online: https://www.fs.usda.gov/ccrc/sites/default/files/documents/files/r8-droughtfactsheet.pdf (accessed on 20 July 2023).
- Wellenius, G.A.; Eliot, M.N.; Bush, K.F.; Holt, D.; Lincoln, R.A.; Smith, A.E.; Gold, J. Heat-related morbidity and mortality in New England: Evidence for local policy. Environ. Res. 2017, 156, 845–853. [Google Scholar] [CrossRef]
- Wolff, T.; Minkler, M.; Wolfe, S.M.; Berkowitz, B.; Bowen, L.; Butterfoss, F.D.; Cristens, B.D.; Fransisco, V.T.; Himmelman, A.T.; Lee, K.S. Collaborating for Equity and Justice: Moving Beyond Collective Impact. Non-Profit Quarterly. Available online: https://nonprofitquarterly.org/collaborating-equity-justice-moving-beyond-collective-impact/ (accessed on 1 July 2023).


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lemon, S.C.; Joseph, H.A.; Williams, S.; Brown, C.; Aytur, S.; Catalano, K.; Chacker, S.; Goins, K.V.; Rudolph, L.; Whitehead, S.; et al. Reimagining the Role of Health Departments and Their Partners in Addressing Climate Change: Revising the Building Resilience against Climate Effects (BRACE) Framework. Int. J. Environ. Res. Public Health 2023, 20, 6447. https://doi.org/10.3390/ijerph20156447
Lemon SC, Joseph HA, Williams S, Brown C, Aytur S, Catalano K, Chacker S, Goins KV, Rudolph L, Whitehead S, et al. Reimagining the Role of Health Departments and Their Partners in Addressing Climate Change: Revising the Building Resilience against Climate Effects (BRACE) Framework. International Journal of Environmental Research and Public Health. 2023; 20(15):6447. https://doi.org/10.3390/ijerph20156447
Chicago/Turabian StyleLemon, Stephenie C., Heather A. Joseph, Samantha Williams, Claudia Brown, Semra Aytur, Katherine Catalano, Stacey Chacker, Karin V. Goins, Linda Rudolph, Sandra Whitehead, and et al. 2023. "Reimagining the Role of Health Departments and Their Partners in Addressing Climate Change: Revising the Building Resilience against Climate Effects (BRACE) Framework" International Journal of Environmental Research and Public Health 20, no. 15: 6447. https://doi.org/10.3390/ijerph20156447
APA StyleLemon, S. C., Joseph, H. A., Williams, S., Brown, C., Aytur, S., Catalano, K., Chacker, S., Goins, K. V., Rudolph, L., Whitehead, S., Zimmerman, S., & Schramm, P. J. (2023). Reimagining the Role of Health Departments and Their Partners in Addressing Climate Change: Revising the Building Resilience against Climate Effects (BRACE) Framework. International Journal of Environmental Research and Public Health, 20(15), 6447. https://doi.org/10.3390/ijerph20156447