
Patients’ Perspectives on the Use of a Newly Developed “Patients’ Guide for Doctor’s Visit”: DocVISITguide


Abstract
1. Introduction
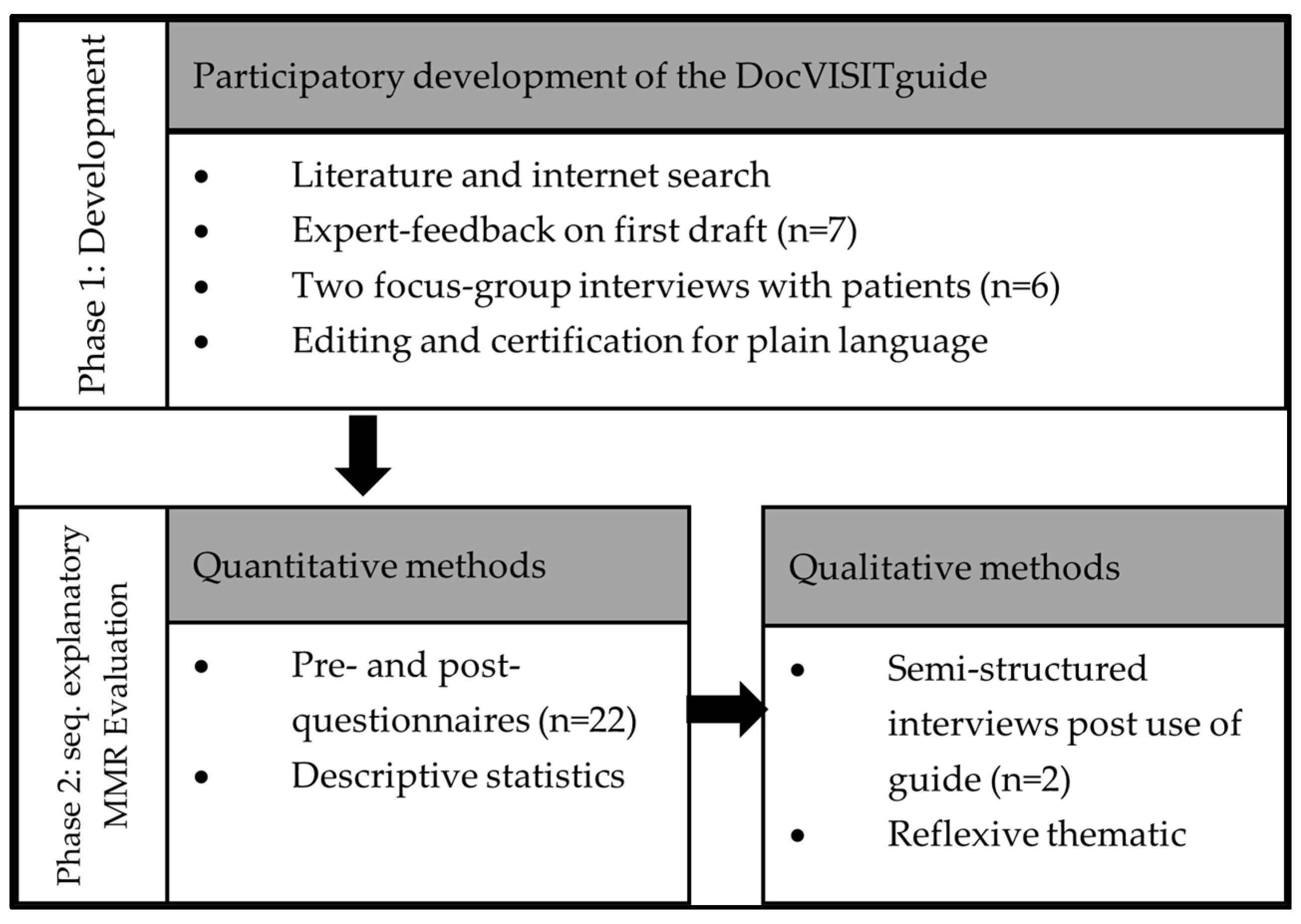
2. Materials and Methods
2.1. Phase 1: Development of the Patients’ Guide for Doctor’s Visit (DocVISITguide)
2.1.1. Literature and Internet Search
2.1.2. Expert-Feedback and Focus Groups with Patients
2.1.3. Editing and Certification for Plain Language
2.2. Phase 2: Sequential Explanatory Mixed Methods Design
2.2.1. Sample and Recruitment
2.2.2. Data Collection
2.2.3. Data Analysis
3. Results
3.1. Description of the DocVISITguide
3.2. Use of the DocVISITguide before and after the Doctor’s Visit
3.2.1. Sample Characteristics
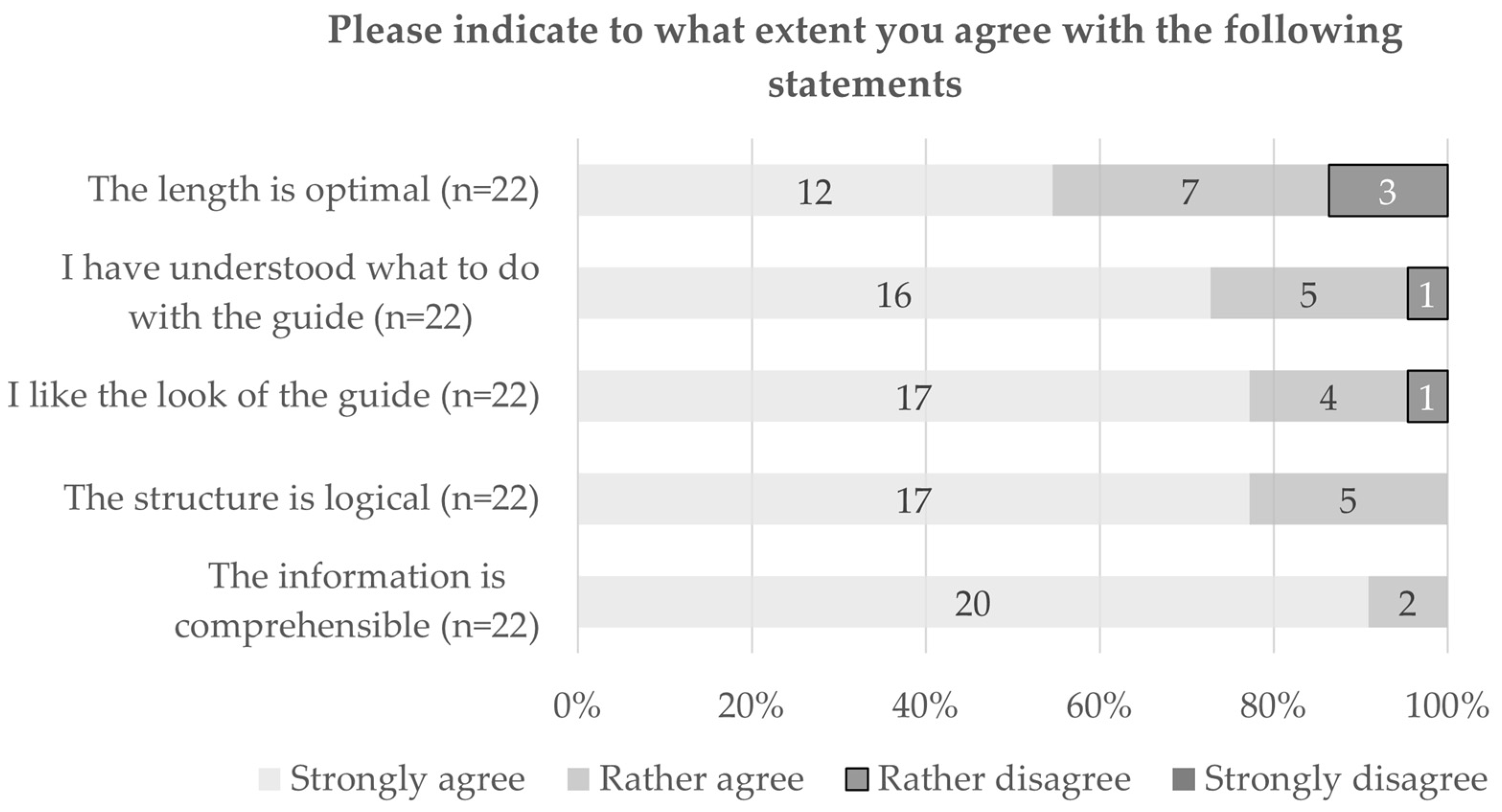
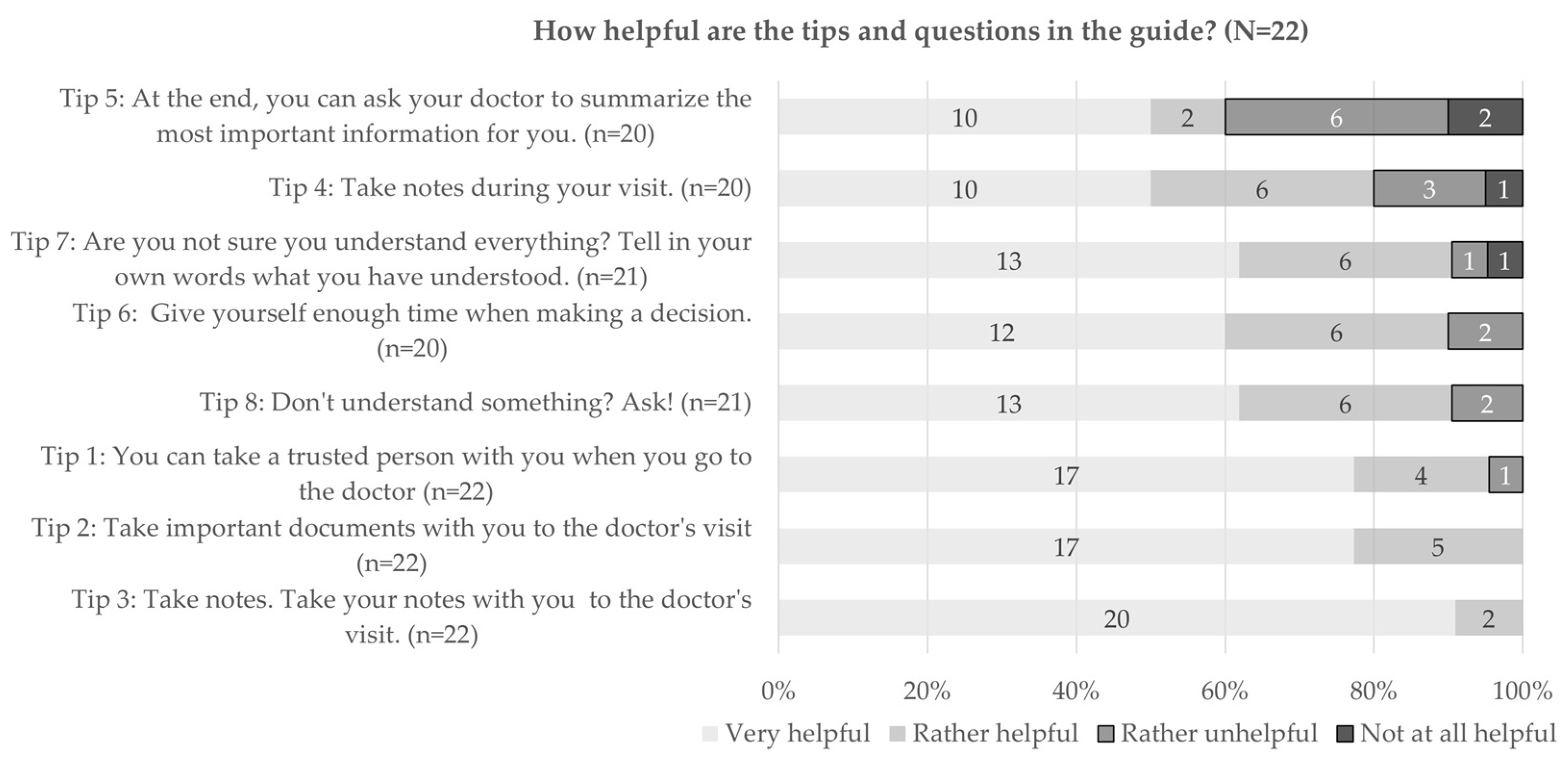
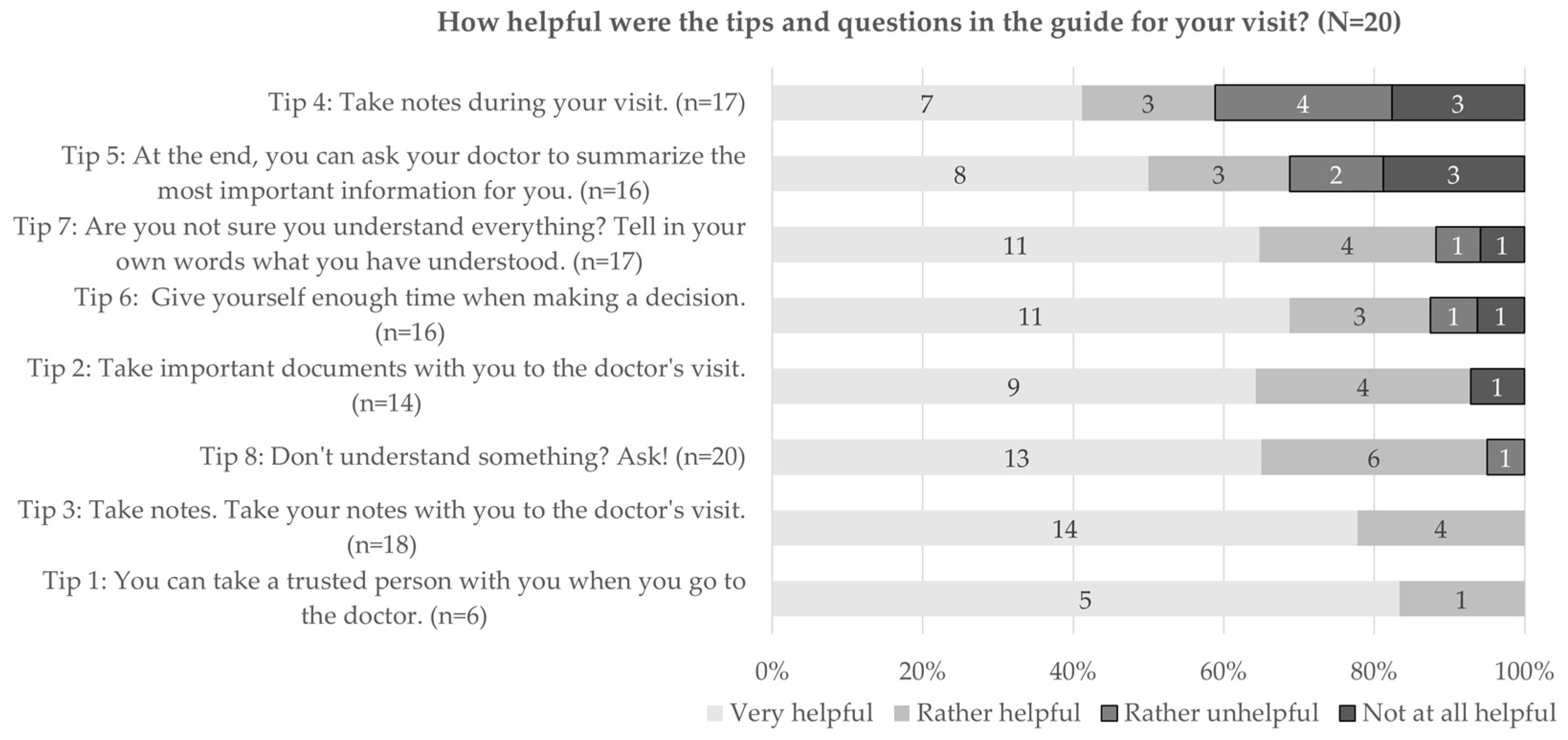
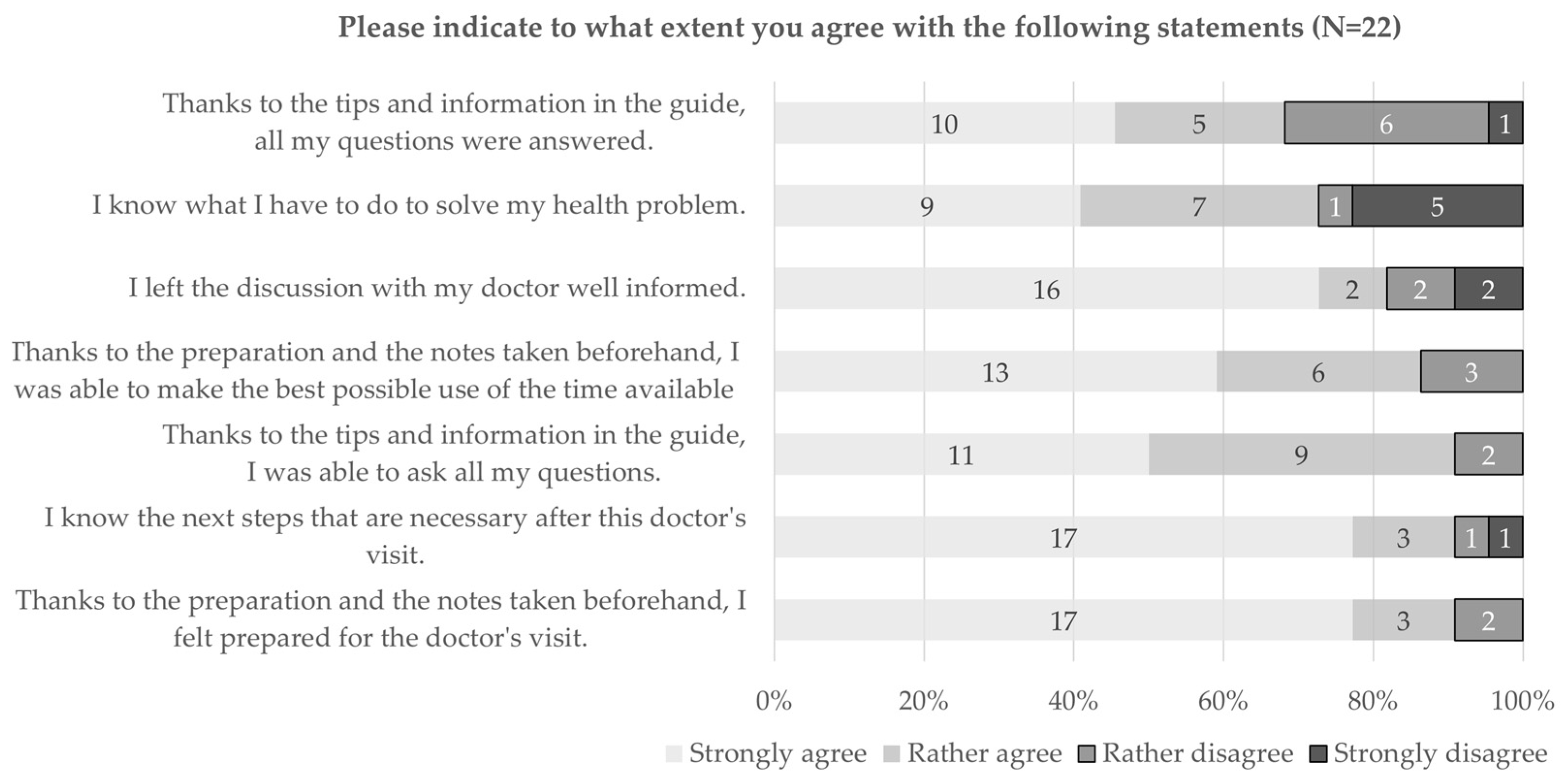
3.2.2. Quantitative Results
3.2.3. Qualitative Findings
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Federal Statistical Office. Arztpraxen. 2018. Available online: https://www.bfs.admin.ch/bfs/de/home/statistiken/gesundheit/gesundheitswesen/arztpraxen.html (accessed on 12 May 2023).
- Street, R.L.; Gordon, H.S.; Ward, M.M.; Krupat, E.; Kravitz, R.L. Patient participation in medical consultations: Why some patients are more involved than others. Med. Care 2005, 43, 960–969. [Google Scholar] [CrossRef] [PubMed]
- Rubio-Valera, M.; Pons-Vigués, M.; Martínez-Andrés, M.; Moreno-Peral, P.; Berenguera, A.; Fernández, A. Barriers and facilitators for the implementation of primary prevention and health promotion activities in primary care: A synthesis through meta-ethnography. PLoS ONE 2014, 9, e89554. [Google Scholar] [CrossRef] [PubMed]
- De Gani, S.M.; Jaks, R.; Bieri, U.; Kocher, J.P. Health Literacy Survey Schweiz 2019–2021; Careum Stiftung: Zürich, Switzerland, 2021. [Google Scholar]
- Sørensen, K.; Pelikan, J.M.; Röthlin, F.; Ganahl, K.; Slonska, Z.; Doyle, G.; Fullam, J.; Kondilis, B.; Agrafiotis, D.; Uiters, E.; et al. Health literacy in Europe: Comparative results of the European health literacy survey (HLS-EU). Eur. J. Public Health 2015, 25, 1053–1058. [Google Scholar] [CrossRef] [PubMed]
- The HLS19 Consortium. International Report on the Methodology, Results, and Recomendations of the European Health Literacy Population Survey 2019–2021 (HLS19) of M-POHL; Austrian National Public Health Institute: Vienna, Austria, 2021. [Google Scholar]
- Sørensen, K.; Van Den Broucke, S.; Fullam, J.; Doyle, G.; Pelikan, J.; Slonska, Z.; Brand, H. Health literacy and public health: A systematic review and integration of definitions and models. BMC Public Health 2012, 12, 80. [Google Scholar] [CrossRef] [PubMed]
- Brabers, A.E.M.; Rademakers, J.J.D.J.M.; Groenewegen, P.P.; van Dijk, L.; Jong, J.D.d. What role does health literacy play in patients’ involvement in medical decision-making? PLoS ONE 2017, 12, e0173316. [Google Scholar] [CrossRef] [PubMed]
- Aboumatar, H.J.; Carson, K.A.; Beach, M.C.; Roter, D.L.; Cooper, L.A. The impact of health literacy on desire for participation in healthcare, medical visit communication, and patient reported outcomes among patients with hypertension. J. Gen. Intern. Med. 2013, 28, 1469–1476. [Google Scholar] [CrossRef] [PubMed]
- Coleman, C.A.; Hudson, S.; Maine, L.L. Health literacy practices and educational competencies for health professionals: A consensus study. J. Health Commun. 2013, 18 (Suppl. S1), 82–102. [Google Scholar] [CrossRef]
- Karuranga, S.; Sørensen, K.; Coleman, C.; Mahmud, A.J. Health Literacy Competencies for European Health Care Personnel. Health Lit. Res. Pract. 2017, 1, e247–e256. [Google Scholar] [CrossRef]
- O’Malley, P.G.; Jackson, J.L.; Becher, D.; Hanson, J.; Lee, J.K.; Grace, K.A. Tool to improve patient-provider interactions in adult primary care: Randomized controlled pilot study. Can. Fam. Physician 2022, 68, e49–e58. [Google Scholar] [CrossRef]
- Balogh, E.P.; Miller, B.T.; Ball, J.R. (Eds.) Improving Diagnosis in Health Care; National Academies Press: Washington, DC, USA, 2015. [Google Scholar]
- Prasad, K.; Poplau, S.; Brown, R.; Yale, S.; Grossman, E.; Varkey, A.B.; Williams, E.; Neprash, H.; Linzer, M. Time Pressure During Primary Care Office Visits: A Prospective Evaluation of Data from the Healthy Work Place Study. J. Gen. Intern. Med. 2020, 35, 465–472. [Google Scholar] [CrossRef]
- Tsiga, E.; Panagopoulou, E.; Sevdalis, N.; Montgomery, A.; Benos, A. The influence of time pressure on adherence to guidelines in primary care: An experimental study. BMJ Open 2013, 3, e002700. [Google Scholar] [CrossRef] [PubMed]
- Denton, C.P.; Laird, B.; Moros, L.; Luna Flores, J.L. Things left unsaid: Important topics that are not discussed between patients with systemic sclerosis, their carers and their healthcare professionals-a discourse analysis. Clin. Rheumatol. 2021, 40, 1399–1407. [Google Scholar] [CrossRef] [PubMed]
- Kuosmanen, L.; Hupli, M.; Ahtiluoto, S.; Haavisto, E. Patient participation in shared decision-making in palliative care—An integrative review. J. Clin. Nurs. 2021, 30, 3415–3428. [Google Scholar] [CrossRef] [PubMed]
- Edwards, A.; Elwyn, G. Inside the black box of shared decision making: Distinguishing between the process of involvement and who makes the decision. Health Expect. 2006, 9, 307–320. [Google Scholar] [CrossRef] [PubMed]
- Castro, C.M.; Wilson, C.; Wang, F.; Schillinger, D. Babel babble: Physicians’ use of unclarified medical jargon with patients. Am. J. Health Behav. 2007, 31 (Suppl. S1), S85–S95. [Google Scholar] [CrossRef]
- McCabe, R.; Healey, P.G.T. Miscommunication in Doctor-Patient Communication. Top. Cogn. Sci. 2018, 10, 409–424. [Google Scholar] [CrossRef] [PubMed]
- Brown, M.T.; Bussell, J.; Dutta, S.; Davis, K.; Strong, S.; Mathew, S. Medication Adherence: Truth and Consequences. Am. J. Med. Sci. 2016, 351, 387–399. [Google Scholar] [CrossRef]
- Santana, M.J.; Manalili, K.; Jolley, R.J.; Zelinsky, S.; Quan, H.; Lu, M. How to practice person-centred care: A conceptual framework. Health Expect. 2018, 21, 429–440. [Google Scholar] [CrossRef]
- Elwyn, G.; Frosch, D.; Thomson, R.; Joseph-Williams, N.; Lloyd, A.; Kinnersley, P.; Cording, E.; Tomson, D.; Dodd, C.; Rollnick, S.; et al. Shared decision making: A model for clinical practice. J. Gen. Intern. Med. 2012, 27, 1361–1367. [Google Scholar] [CrossRef]
- Harrington, J.; Noble, L.M.; Newman, S.P. Improving patients’ communication with doctors: A systematic review of intervention studies. Patient Educ. Couns. 2004, 52, 7–16. [Google Scholar] [CrossRef]
- Gaston, C.M.; Mitchell, G. Information giving and decision-making in patients with advanced cancer: A systematic review. Soc. Sci. Med. 2005, 61, 2252–2264. [Google Scholar] [CrossRef] [PubMed]
- Kinnersley, P.; Edwards, A.; Hood, K.; Cadbury, N.; Ryan, R.; Prout, H.; Owen, D.; MacBeth, F.; Butow, P.; Butler, C. Interventions before consultations for helping patients address their information needs. Cochrane Database Syst. Rev. 2007, 2007, CD004565. [Google Scholar] [CrossRef] [PubMed]
- Coulter, A. Patient engagement—What works? J. Ambul. Care Manag. 2012, 35, 80–89. [Google Scholar] [CrossRef] [PubMed]
- Sansoni, J.E.; Grootemaat, P.; Duncan, C. Question Prompt Lists in health consultations: A review. Patient Educ. Couns. 2015, 98, 1454–1464. [Google Scholar] [CrossRef]
- Creswell, J.W.; Plano Clark, V.L. Designing and Conducting Mixed Methods Research, 2nd ed.; SAGE Publications: Los Angeles, CA, USA, 2011. [Google Scholar]
- Proctor, E.; Silmere, H.; Raghavan, R.; Hovmand, P.; Aarons, G.; Bunger, A.; Griffey, R.; Hensley, M. Outcomes for implementation research: Conceptual distinctions, measurement challenges, and research agenda. Adm. Policy Ment. Health 2011, 38, 65–76. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Thematic Analysis: A Practical Guide; SAGE Publications: Los Angeles, CA, USA, 2021. [Google Scholar]
- Wagner, E.H. Organizing Care for Patients With Chronic Illness Revisited. Milbank Q. 2019, 97, 659–664. [Google Scholar] [CrossRef]
- Irving, G.; Neves, A.L.; Dambha-Miller, H.; Oishi, A.; Tagashira, H.; Verho, A.; Holden, J. International variations in primary care physician consultation time: A systematic review of 67 countries. BMJ Open 2017, 7, e017902. [Google Scholar] [CrossRef]
- Tracy, M.; Ayre, J.; Mac, O.; Copp, T.; Trevena, E.L.; Shepherd, H. Question prompt lists and endorsement of question-asking support patients to get the information they seek—A longitudinal qualitative study. Health Expect. 2022, 25, 1652–1663. [Google Scholar] [CrossRef]
- Moser, A.; von Wyl, V.; Höglinger, M. Health and social behaviour through pandemic phases in Switzerland: Regional time-trends of the COVID-19 Social Monitor panel study. PLoS ONE 2021, 16, e0256253. [Google Scholar] [CrossRef]
- Höglinger, M.; Brunner, B.; Stucki, M.; Wieser, S. Gesundheitsökonomische Aspekte der Corona-Krise in der Schweiz: Resultate des COVID-19 Social Monitor. Gesundheitsökonomie Qual. 2020, 25, 233–238. [Google Scholar] [CrossRef]
- Hekler, E.B.; Klasnja, P.; Riley, W.T.; Buman, M.P.; Huberty, J.; Rivera, D.E.; Martin, C.A. Agile science: Creating useful products for behavior change in the real world. Transl. Behav. Med. 2016, 6, 317–328. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Quantitative Survey (Paired Cases) n (%) |
|---|---|
| Total, N (%) | 22 (100%) |
| Gender, n (%) | |
| Male | 6 (27%) |
| Female | 16 (73%) |
| Age, n (%) | |
| Younger than 30 years | – |
| Between 31 and 40 years | 7 (32%) |
| Between 41 and 50 years | 3 (14%) |
| Between 51 and 60 years | 2 (9%) |
| Between 61 and 70 years | 5 (23%) |
| Older than 71 years | 5 (23%) |
| Education, n (%) | |
| Compulsory school | 2 (9%) |
| Upper secondary level | 5 (23%) |
| Tertiary level | 15 (68%) |
| Education in the health sector, n (%) | |
| Yes | 11 (50%) |
| No | 11 (50%) |
| Country of birth, n (%) | |
| Switzerland | 18 (82%) |
| Other country | 4 (18%) |
| Mother language, n (%) * | |
| German | 21 (88%) |
| French | 0 (0%) |
| Italian | 1 (4%) |
| Other | 2 (8%) |
| Chronic disease, n (%) | |
| Yes | 17 (77%) |
| No | 5 (23%) |
| Key Quantitative Results | Exploration by Two Case Studies |
|---|---|
| Expectations before using the guide | |
Acceptability
| “What can they teach me”—trying out the guide with low expectations When learning about the project and guide:
After reading the guide for the first time:
|
| After having used the guide for preparation and potentially during a doctor’s visit | |
| Feasibility: in respect to preparation with guide
in respect to use of guide
| “The guide helps against all odds”—experiencing a positive effect through use of the guide After using the guide for preparation:
|
Adoption
| “Better not to show it off”—not wanting to use the guide during the visit When remembering the use of the guide:
|
| No matching quantitative data | “Building bridges”—involving professionals to take full advantage of the guide When reflecting about their use of the guide:
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jaks, R.; Guggiari, E.; De Gani, S.M.; Nicca, D. Patients’ Perspectives on the Use of a Newly Developed “Patients’ Guide for Doctor’s Visit”: DocVISITguide. Int. J. Environ. Res. Public Health 2023, 20, 6414. https://doi.org/10.3390/ijerph20146414
Jaks R, Guggiari E, De Gani SM, Nicca D. Patients’ Perspectives on the Use of a Newly Developed “Patients’ Guide for Doctor’s Visit”: DocVISITguide. International Journal of Environmental Research and Public Health. 2023; 20(14):6414. https://doi.org/10.3390/ijerph20146414
Chicago/Turabian StyleJaks, Rebecca, Elena Guggiari, Saskia Maria De Gani, and Dunja Nicca. 2023. "Patients’ Perspectives on the Use of a Newly Developed “Patients’ Guide for Doctor’s Visit”: DocVISITguide" International Journal of Environmental Research and Public Health 20, no. 14: 6414. https://doi.org/10.3390/ijerph20146414
APA StyleJaks, R., Guggiari, E., De Gani, S. M., & Nicca, D. (2023). Patients’ Perspectives on the Use of a Newly Developed “Patients’ Guide for Doctor’s Visit”: DocVISITguide. International Journal of Environmental Research and Public Health, 20(14), 6414. https://doi.org/10.3390/ijerph20146414