
Efficacy of a Short-Term Lifestyle Change Intervention in Healthy Young Men: The FASt Randomized Controlled Trial
 , , and
, , and  on behalf of FASt Study Group
on behalf of FASt Study Group
Abstract
1. Introduction
2. Materials and Methods
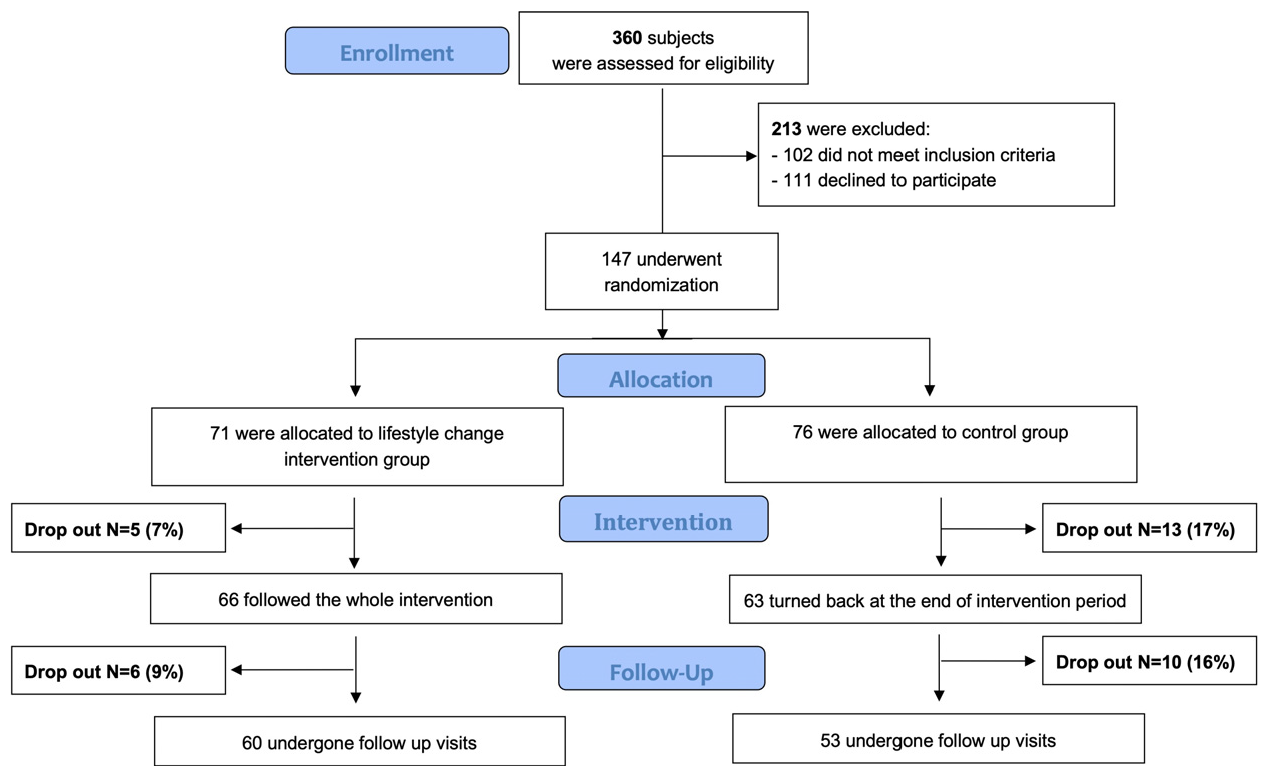
2.1. Study Design
2.2. Inclusion Criteria, Participants, Ethics
2.3. Assessment of Diet and Physical Activity
2.4. Intervention
- -
- Daily vegetables and fruit intake (possibly seasonal and organic)
- -
- Increase pulses intake up to 3/4 times a week
- -
- Increase fish intake up to 3/4 times a week (particularly oily fish)
- -
- Encourage nuts intake, up to 30 g a day
- -
- Encourage consumption of extra virgin olive oil
- -
- Encourage consumption of whole grains and their products
- -
- Limit cheese consumption twice a week (milk, yoghurt and kefir were allowed every day)
- -
- Limit meat intake to 3/4 times a week (2/3 times white meat, once a week red and processed meat)
- -
- Limit alcohol consumption to a maximum of 2 alcohol units a day
- -
- Limit desserts and sweet snacks to once a week
- -
- 1st month: once a week
- -
- 2nd and 3rd months: every two weeks
- -
- 4th month: at the end of the month (final examination)
2.5. Sample Size
2.6. Randomization and Blinding
2.7. Data Management and Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Preventing Chronic Diseases: A Vital Investment. WHO Global Report; World Health Organization: Geneva, Switzerland, 2005. Available online: https://apps.who.int/iris/handle/10665/43314 (accessed on 23 March 2023).
- GBD. Risk Factors Collaborators. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1223–1249. [Google Scholar] [CrossRef] [PubMed]
- Willett, W.; Rockström, J.; Loken, B.; Springmann, M.; Lang, T.; Vermeulen, S.; Garnett, T.; Tilman, D.; DeClerck, F.; Wood, A.; et al. Food in the Anthropocene: The EAT-Lancet Commission on healthy diets from sustainable food systems. Lancet 2019, 393, 447–492, Erratum in Lancet 2019, 393, 530; Erratum in Lancet 2019, 393, 2590; Erratum in Lancet 2020, 395, 338; Erratum in Lancet 2020, 396, e56.. [Google Scholar] [CrossRef] [PubMed]
- Dinu, M.; Pagliai, G.; Casini, A.; Sofi, F. Mediterranean diet and multiple health outcomes: An umbrella review of meta-analyses of observational studies and randomised trials. Eur. J. Clin. Nutr. 2018, 72, 30–43. [Google Scholar] [CrossRef] [PubMed]
- Kargin, D.; Tomaino, L.; Serra-Majem, L. Experimental Outcomes of the Mediterranean Diet: Lessons Learned from the Predimed Randomized Controlled Trial. Nutrients 2019, 11, 2991. [Google Scholar] [CrossRef] [PubMed]
- WCRF. Diet, Nutrition, Physical Activity and Cancer: A Global Perspective. The Third Expert Report. Continuous Update Project Expert Report. World Cancer Research Fund. 2018. Available online: https://www.wcrf.org/diet-and-cancer/ (accessed on 23 March 2023).
- WHO. Global Action Plan on Physical Activity 2018–2030: More Active People for A Healthier World; World Health Organization: Geneva, Switzerland, 2018. Available online: https://www.who.int/publications/i/item/9789241514187 (accessed on 23 March 2023).
- Sawyer, S.M.; Azzopardi, P.S.; Wickremarathne, D.; Patton, G.C. The age of adolescence. Lancet Child Adolesc. Health 2018, 2, 223–228. [Google Scholar] [CrossRef]
- Pérez, E.A.; Olivares, V.M.; Martínez-Espinosa, R.M.; Molina Vila, M.D.; García-Galbis, M.R. New Insights about How to Make an Intervention in Children and Adolescents with Metabolic Syndrome: Diet, Exercise vs. Changes in Body Composition. A Systematic Review of RCT. Nutrients 2018, 10, 878. [Google Scholar] [CrossRef] [PubMed]
- Perkison, W.B.; Adekanye, J.A.; de Oliveira Otto, M.C. Dietary Interventions and Type 2 Diabetes in Youth: A Fresh Look at the Evidence. Curr. Nutr. Rep. 2018, 7, 227–234. [Google Scholar] [CrossRef]
- Blas, E.; Sivasankara Kurup, A.; World Health Organization. Equity, Social Determinants and Public Health Programmes/Editors Erik Blas and Anand Sivasankara Kurup; World Health Organization: Geneva, Switzerland, 2010.
- Montano, L.; Ceretti, E.; Donato, F.; Bergamo, P.; Zani, C.; Viola, G.C.V.; Notari, T.; Pappalardo, S.; Zani, D.; Ubaldi, S.; et al. Effects of a Lifestyle Change Intervention on Semen Quality in Healthy Young Men Living in Highly Polluted Areas in Italy: The FASt Randomized Controlled Trial. Eur. Urol. Focus 2022, 8, 351–359. [Google Scholar] [CrossRef]
- Manuale di Valutazione Antropometrica Dello Stato Nutrizionale. Available online: https://www.yumpu.com/it/document/view/14929068/scarica-il-libro-in-formato-pdf-giorgio-bedogni (accessed on 23 March 2023).
- Martínez-González, M.A.; García-Arellano, A.; Toledo, E.; Salas-Salvado, J.; Buil-Cosiales, P.; Corella, D.; Covas, M.I.; Schröder, H.; Aros, F.; Gomez-Gracia, E.; et al. A 14-item Mediterranean diet assessment tool and obesity indexes among high-risk subjects: The PREDIMED trial. PLoS ONE 2012, 7, e43134. [Google Scholar] [CrossRef]
- Riboli, E.; Kaaks, R. The EPIC Project: Rationale and study design. European Prospective Investigation into Cancer and Nutrition. Int. J. Epidemiol. 1997, 26, 6–14. [Google Scholar] [CrossRef]
- Decarli, A.; Franceschi, S.; Ferraroni, M.; Gnagnarella, P.; Parpinel, M.T.; La Vecchia, C.; Negri, E.; Salvini, S.; Falcini, F.; Giacosa, A. Validation of a food-frequency questionnaire to assess dietary intakes in cancer studies in Italy. Results for specific nutrients. Ann. Epidemiol. 1996, 6, 110–118. [Google Scholar] [CrossRef]
- Pala, V.; Sieri, S.; Palli, D.; Salvini, S.; Berrino, F.; Bellegotti, M.; Frasca, G.; Tumino, R.; Sacerdote, C.; Fiorini, L.; et al. Diet in the Italian EPIC cohorts: Presentation of data and methodological issues. Tumori 2003, 89, 594–607. [Google Scholar] [CrossRef]
- Hagströmer, M.; Oja, P.; Sjöström, M. The International Physical Activity Questionnaire (IPAQ): A study of concurrent and construct validity. Public Health Nutr. 2006, 9, 755–762. [Google Scholar] [CrossRef] [PubMed]
- Lee, P.H.; Macfarlane, D.J.; Lam, T.H.; Stewart, S.M. Validity of the International Physical Activity Questionnaire Short Form (IPAQ-SF): A systematic review. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 115. [Google Scholar] [CrossRef] [PubMed]
- Stonerock, G.L.; Blumenthal, J.A. Role of Counseling to Promote Adherence in Healthy Lifestyle Medicine: Strategies to Improve Exercise Adherence and Enhance Physical Activity. Prog. Cardiovasc. Dis. 2017, 59, 455–462. [Google Scholar] [CrossRef]
- Miller, W.R.; Rollnick, S. Motivational Interviewing: Helping People Change, 3rd ed.; Guilford: New York, NY, USA, 2013. [Google Scholar]
- Naar-King, S.; Suarez, M. Motivational Interviewing with Adolescent and Young Adults, 1st ed.; Guilford Press: New York, NY, USA, 2011. [Google Scholar]
- Miller, W.R.; Rollnick, S. Meeting in the middle: Motivational interviewing and self-determination theory. Int. J. Behav. Nutr. Phys. Act. 2011, 9, 25. [Google Scholar] [CrossRef]
- CREA. 2018 Guidelines for a Healthy Nutrition. Centro di Ricerca Alimenti e Nutrizione (CREA). 2019. Available online: https://www.crea.gov.it/en/web/alimenti-e-nutrizione/-/linee-guida-per-una-sana-alimentazione-2018 (accessed on 23 March 2023).
- O’Connell, N.S.; Dai, L.; Jiang, Y.; Speiser, J.L.; Ward, R.; Wei, W.; Carroll, R.; Gebregziabher, M. Methods for Analysis of Pre-Post Data in Clinical Research: A Comparison of Five Common Methods. J. Biom. Biostat. 2017, 8, 1–8. [Google Scholar] [PubMed]
- Willett, W.C.; Sacks, F.; Trichopoulou, A.; Drescher, G.; Ferro-Luzzi, A.; Helsing, E.; Trichopoulos, D. Mediterranean diet pyramid: A cultural model for healthy eating. Am. J. Clin. Nutr. 1995, 61, 1402S–1406S. [Google Scholar] [CrossRef]
- Martínez-González, M.A.; Salas-Salvadó, J.; Estruch, R.; Corella, D.; Fitó, M.; Ros, E. Predimed Investigators Benefits of the Mediterranean Diet: Insights from the PREDIMED Study. Prog. Cardiovasc. Dis. 2015, 58, 50–60. [Google Scholar] [CrossRef] [PubMed]
- Rees, K.; Takeda, A.; Martin, N.; Ellis, L.; Wijesekara, D.; Vepa, A.; Das, A.; Hartley, L.; Stranges, S. Mediterranean-style diet for the primary and secondary prevention of cardiovascular disease. Cochrane Database Syst. Rev. 2019, 3, CD009825. [Google Scholar] [CrossRef]
- Rosato, V.; Temple, N.J.; La Vecchia, C.; Castellan, G.; Tavani, A.; Guercio, V. Mediterranean diet and cardiovascular disease: A systematic review and meta-analysis of observational studies. Eur. J. Nutr. 2019, 58, 173–191. [Google Scholar] [CrossRef]
- Jemmott, J.B.; Zhang, J.; Jemmott, L.S.; Icard, L.D.; Ngwane, Z.; Makiwane, M.; O’Leary, A. Intervention Increases Physical Activity and Healthful Diet among South African Adolescents over 54 Months: A Randomized Controlled Trial. J. Adolesc. Health 2019, 65, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Cullen, K.W.; Thompson, D.; Boushey, C.; Konzelmann, K.; Chen, T. Evaluation of a web-based program promoting healthy eating and physical activity for adolescents: Teen choice: Food and fitness. Health Educ. Res. 2013, 28, 704–714. [Google Scholar] [CrossRef] [PubMed]
- Chamberland, K.; Sanchez, M.; Panahi, S.; Provencher, V.; Gagnon, J.; Drapeau, V. The impact of an innovative web-based school nutrition intervention to increase fruits and vegetables and milk and alternatives in adolescents: A clustered randomized trial. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 140. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Morze, J.; Hoffmann, G. Mediterranean diet and health status: Active ingredients and pharmacological mechanisms. Br. J. Pharmacol. 2020, 177, 1241–1257. [Google Scholar] [CrossRef]
- Zazpe, I.; Sanchez-Tainta, A.; Estruch, R.; Lamuela-Raventos, R.M.; Schröder, H.; Salas-Salvado, J.; Corella, D.; Fiol, M.; Gomez-Gracia, E.; Aros, F.; et al. A large randomized individual and group intervention conducted by registered dietitians increased adherence to Mediterranean-type diets: The PREDIMED study. J. Am. Diet. Assoc. 2008, 108, 1134–1144. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Feature | INT (N = 66) Mean ± S.D. | CTRL (N = 63) Mean ± S.D. |
|---|---|---|
| age (years) | 20.1 ± 1.2 | 20.0 ± 1.2 |
| weight (kg) | 70.7 ± 9.0 | 70.9 ± 9.3 |
| height (cm) | 177.5 ± 5.9 | 177.4 ± 5.8 |
| BMI (kg/m2) | 22.4 ± 2.2 | 22.5 ± 2.4 |
| Waist circumference (cm) | 83.1 ± 6.0 | 84.1 ± 5.8 |
| Cigarette smokers N (%) | 5 (7.6) | 3 (4.8) |
| Occasional alcohol drinkersN (%) | 44 (66.7) | 48 (76.2) |
| Variable | Group | t0 (Mean ± S.D.) | t4 (Mean ± S.D.) | t8 (Mean ± S.D.) | pa (t4) | pa (t8) |
|---|---|---|---|---|---|---|
| Vegetables (g/day) | INT | 188.12 ± 118.23 | 208.39 ± 99.95 | 190.66 ± 76.22 | <0.0001 | 0.0021 |
| CTRL | 172.23 ± 118.24 | 165.66 ± 95.98 | 164.10 ± 114.61 | |||
| Onion and garlic (g/day) | INT | 19.48 ± 13.33 | 17.07 ± 12.33 | 15.91 ± 10.56 | 0.8889 | 0.9719 |
| CTRL | 18.19 ± 12.96 | 17.43 ± 14.27 | 16.14 ± 12.78 | |||
| Legumes (g/day) | INT | 17.44 ± 14.32 | 36.1 ± 17.32 | 30.09 ± 17.77 | <0.0001 | 0.0011 |
| CTRL | 20.67 ± 20.48 | 24.62 ± 24.02 | 24.25 ± 20.87 | |||
| Fruits (g/day) | INT | 273.11 ± 191.09 | 317.46 ± 150.02 | 295.88 ± 119.57 | 0.0003 | 0.0003 |
| CTRL | 236.33 ± 161.35 | 245.95 ± 160.15 | 217.05 ± 121.76 | |||
| Nuts and seeds (g/day) | INT | 9.52 ± 11.44 | 23.64 ± 9.11 | 18.70 ± 12.27 | <0.0001 | <0.0001 |
| CTRL | 7.30 ± 8.68 | 8.71 ± 9.08 | 8.58 ± 9.25 | |||
| Whole grains (g/day) | INT | 24.78 ± 32.37 | 50.92 ± 43.79 | 51.19 ± 47.71 | <0.0001 | <0.0001 |
| CTRL | 30.23 ± 36.78 | 31.59 ± 44.96 | 28.00 ± 31.99 | |||
| Red meat (g/day) | INT | 94.62 ± 47.21 | 58.09 ± 29.21 | 64.18 ± 35.94 | <0.0001 | 0.0428 |
| CTRL | 92.07 ± 58.86 | 82.70 ± 48.89 | 77.87 ± 44.43 | |||
| White meat (g/day) | INT | 79.46 ± 55.06 | 69.77 ± 34.34 | 66.50 ± 38.92 | 0.3932 | 0.1421 |
| CTRL | 78.81 ± 66.72 | 73.39 ± 57.09 | 64.54 ± 48.38 | |||
| Processed meat (g/day) | INT | 52.81 ± 40.87 | 23.86 ± 21.61 | 27.39 ± 19.97 | <0.0001 | <0.0001 |
| CTRL | 53.60 ± 34.98 | 51.71 ± 33.97 | 44.49 ± 32.01 | |||
| Fish (g/day) | INT | 45.21 ± 26.65 | 73.80 ± 40.41 | 65.08 ± 31.05 | <0.0001 | 0.0001 |
| CTRL | 53.54 ± 38.18 | 50.10 ± 32.94 | 51.09 ± 36.53 | |||
| Olive oil (g/day) | INT | 7.32 ± 5.92 | 8.44 ± 6.42 | 7.35 ± 6.05 | 0.7410 | 0.2707 |
| CTRL | 8.04 ± 7.58 | 8.28 ± 7.29 | 9.12 ± 7.50 | |||
| EVO oil (g/day) | INT | 16.77 ± 13.30 | 20.61 ± 13.02 | 18.65 ± 9.96 | 0.0553 | 0.0700 |
| CTRL | 15.15 ± 9.19 | 15.95 ± 11.03 | 15.18 ± 11.33 | |||
| Total olive oil (g/day) | INT | 24.09 ± 15.44 | 29.04 ± 14.73 | 26.00 ± 11.70 | 0.2465 | 0.5794 |
| CTRL | 23.19 ± 11.32 | 24.23 ± 12.67 | 24.30 ± 11.80 | |||
| Butter (g/day) | INT | 2.50 ± 4.12 | 1.94 ± 3.66 | 1.41 ± 2.23 | 0.5929 | 0.1821 |
| CTRL | 3.05 ± 3.96 | 2.04 ± 2.85 | 2.03 ± 2.20 | |||
| Milk and yogurt (g/day) | INT | 191.56 ± 149.39 | 179.39 ± 133.96 | 171.19 ± 126.60 | 0.3026 | 0.8195 |
| CTRL | 171.77 ± 150.22 | 183.73 ± 150.43 | 185.90 ± 171.00 | |||
| Cheese (g/day) | INT | 58.79 ± 53.70 | 40.33 ± 26.90 | 47.27 ± 33.54 | 0.0007 | 0.0662 |
| CTRL | 72.81 ± 58.50 | 68.83 ± 40.41 | 69.28 ± 50.54 | |||
| Eggs (g/day) | INT | 26.01 ± 16.17 | 25.36 ± 16.87 | 25.67 ± 14.67 | 0.4674 | 0.2772 |
| CTRL | 27.24 ± 16.78 | 27.15± 17.35 | 24.62 ± 15.14 | |||
| Sweets (g/day) | INT | 146.01 ± 129.71 | 91.87 ± 50.89 | 105.62 ± 78.53 | 0.0030 | 0.0020 |
| CTRL | 91.41 ± 52.87 | 99.99 ± 68.74 | 100.92± 65.37 | |||
| Sweetened drinks (mL/day) | INT | 207.43 ± 306.52 | 114.64 ± 104.54 | 112.43 ± 109.38 | 0.0144 | 0.0919 |
| CTRL | 153.37 ± 157.80 | 132.91 ± 137.78 | 147.15 ± 124.11 | |||
| Coffee (mL/day) | INT | 42.77 ± 45.64 | 42.10 ± 35.90 | 42.04 ± 35.22 | 0.8646 | 0.6877 |
| CTRL | 40.93 ± 35.40 | 48.47 ± 39.61 | 50.17± 45.65 | |||
| Water (mL/day) | INT | 1289.92 ± 534.29 | 1226.60 ± 327.03 | 1183.24 ± 313.38 | 0.9812 | 0.9507 |
| CTRL | 1208.81 ± 324.55 | 1210.47 ± 332.20 | 1173.19 ± 334.82 |
| Variable | Group | t0 * (Mean ± S.D.) | t4 * (Mean ± S.D.) | t8 * (Mean ± S.D.) | pa (t4) | pa (t8) |
|---|---|---|---|---|---|---|
| Energy intake (Kcal/day) | INT | 2923.56 ± 1070.16 | 2584.23 ± 663.96 | 2574.75 ± 797.21 | 0.0698 | 0.2481 |
| CTRL | 2779.99 ± 807.53 | 2675.07 ± 628.95 | 2611.54 ± 702.96 | |||
| Total proteins (g/day) | INT | 118.87 ± 39.01 | 102.76 ± 27.51 | 103.56 ± 32.22 | 0.0112 | 0.3274 |
| CTRL | 121.11 ± 39.82 | 113.80 ± 31.35 | 109.88 ± 33.84 | |||
| Animal proteins (g/day) | INT | 83.98 ± 32.74 | 66.90 ± 22.41 | 69.03 ± 24.84 | 0.0002 | 0.0796 |
| CTRL | 86.30 ± 30.90 | 81.51 ± 26.69 | 77.93 ± 27.15 | |||
| Plant proteins (g/day) | INT | 34.85 ± 10.78 | 35.79 ± 9.96 | 34.47 ± 11.05 | 0.0107 | 0.1967 |
| CTRL | 34.74 ± 13.58 | 32.23 ± 9.82 | 31.90 ± 10.69 | |||
| Lipids (g/day) | INT | 117.41 ± 46.02 | 107.72 ± 28.76 | 104.21 ± 32.67 | 0.2772 | 0.2348 |
| CTRL | 112.90 ± 36.69 | 110.62 ± 30.47 | 107.70 ± 33.41 | |||
| Total saturated fats (g/day) | INT | 39.41 ± 18.17 | 30.71 ± 9.81 | 31.55 ± 12.02 | <0.0001 | 0.0050 |
| CTRL | 38.69 ± 15.12 | 37.22 ± 11.99 | 36.18 ± 12.68 | |||
| Mufa (g/day) | INT | 51.55 ± 19.42 | 50.44 ± 13.71 | 47.73 ± 14.35 | 0.8612 | 0.6122 |
| CTRL | 49.32 ± 15.61 | 48.91 ± 13.92 | 47.64 ± 14.81 | |||
| Pufa (g/day) | INT | 16.53 ± 6.15 | 16.93 ± 6.15 | 15.68 ± 5.01 | 0.1064 | 0.7006 |
| CTRL | 15.59 ± 5.01 | 15.22 ± 4.48 | 14.78 ± 4.72 | |||
| Omega-6 fatty acid (g/day) | INT | 13.04 ± 4.98 | 13.59 ± 5.41 | 12.53 ± 4.19 | 0.0371 | 0.5727 |
| CTRL | 12.12 ± 4.08 | 11.91 ± 3.78 | 11.61 ± 4.01 | |||
| Omega-3 fatty acid (g/day) | INT | 1.15 ± 0.38 | 1.29 ± 0.51 | 1.13 ± 0.36 | 0.0043 | 0.4409 |
| CTRL | 1.12 ± 0.36 | 1.09 ± 0.33 | 1.07 ± 0.36 | |||
| Available glucides (g/day) | INT | 363.73 ± 152.25 | 313.82 ± 93.98 | 317.89 ± 115.43 | 0.1771 | 0.3717 |
| CTRL | 331.35 ± 112.86 | 314.61 ± 82.55 | 310.36 ± 89.00 | |||
| Soluble glucides (g/day) | INT | 143.61 ± 89.32 | 121.51 ± 39.72 | 121.95 ± 51.82 | 0.2783 | 0.1980 |
| CTRL | 112.81 ± 35.75 | 116.61 ± 44.11 | 113.57 ± 36.91 | |||
| Fibres (g/day) | INT | 24.37 ± 9.22 | 28.20 ± 7.19 | 26.71 ± 8.34 | <0.0001 | 0.0018 |
| CTRL | 23.44 ± 7.20 | 23.17 ± 6.83 | 22.26 ± 6.27 | |||
| Sodium (mg/day) | INT | 3047.87 ± 1382.52 | 2236.01 ± 754.85 | 2501.36 ± 977.73 | <0.0001 | 0.0174 |
| CTRL | 3232.32 ± 1210.10 | 3126.13 ± 1080.71 | 2903.83 ± 1072.99 | |||
| Vit C (μg/day) | INT | 142.72 ± 66.59 | 158.02 ± 56.21 | 146.76 ± 47.77 | 0.0008 | 0.0398 |
| CTRL | 131.98 ± 53.45 | 127.49 ± 48.95 | 126.09 ± 48.12 | |||
| Vit B6 (mg/day) | INT | 2.42 ± 0.75 | 2.43 ± 0.84 | 2.30 ± 0.70 | 0.2765 | 0.3391 |
| CTRL | 2.32 ± 0.68 | 2.23 ± 0.66 | 2.17 ± 0.71 | |||
| Folic acid (μg/day) | INT | 345.26 ± 113.76 | 357.72 ± 103.72 | 344.01 ± 96.81 | 0.0134 | 0.0605 |
| CTRL | 336.39 ± 94.66 | 318.06 ± 74.10 | 311.16 ± 80.75 | |||
| Retinol equivalents (μg/day) | INT | 1244.94 ± 774.78 | 1268.41 ± 697.34 | 1251.35 ± 834.54 | 0.1019 | 0.1966 |
| CTRL | 1165.99 ± 668.03 | 1098.38 ± 423.56 | 1081.51 ± 424.83 | |||
| Beta-carotene (μg/day) | INT | 3899.63 ± 2504.85 | 4524.72 ± 2429.48 | 4039.25 ± 1851.24 | 0.0001 | 0.0192 |
| CTRL | 3321.99 ± 1588.27 | 3298.04 ± 1644.56 | 3295.26 ± 1766.60 | |||
| Vit E (mg/day) | INT | 16.12 ± 6.40 | 18.43 ± 5.74 | 16.84 ± 5.31 | 0.0002 | 0.0606 |
| CTRL | 14.68 ± 4.35 | 14.80 ± 4.46 | 14.54 ± 4.49 | |||
| Vit D (μg/day) | INT | 4.58 ± 2.04 | 4.59 ± 2.15 | 4.44 ± 1.77 | 0.7813 | 0.7114 |
| CTRL | 4.53 ± 1.96 | 4.49 ± 1.90 | 4.35 ± 2.25 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Donato, F.; Ceretti, E.; Viola, G.C.V.; Marullo, M.; Zani, D.; Ubaldi, S.; Sieri, S.; Lorenzetti, S.; Montano, L., on behalf of FASt Study Group. Efficacy of a Short-Term Lifestyle Change Intervention in Healthy Young Men: The FASt Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2023, 20, 5812. https://doi.org/10.3390/ijerph20105812
Donato F, Ceretti E, Viola GCV, Marullo M, Zani D, Ubaldi S, Sieri S, Lorenzetti S, Montano L on behalf of FASt Study Group. Efficacy of a Short-Term Lifestyle Change Intervention in Healthy Young Men: The FASt Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2023; 20(10):5812. https://doi.org/10.3390/ijerph20105812
Chicago/Turabian StyleDonato, Francesco, Elisabetta Ceretti, Gaia Claudia Viviana Viola, Monica Marullo, Danilo Zani, Stefania Ubaldi, Sabina Sieri, Stefano Lorenzetti, and Luigi Montano on behalf of FASt Study Group. 2023. "Efficacy of a Short-Term Lifestyle Change Intervention in Healthy Young Men: The FASt Randomized Controlled Trial" International Journal of Environmental Research and Public Health 20, no. 10: 5812. https://doi.org/10.3390/ijerph20105812
APA StyleDonato, F., Ceretti, E., Viola, G. C. V., Marullo, M., Zani, D., Ubaldi, S., Sieri, S., Lorenzetti, S., & Montano, L., on behalf of FASt Study Group. (2023). Efficacy of a Short-Term Lifestyle Change Intervention in Healthy Young Men: The FASt Randomized Controlled Trial. International Journal of Environmental Research and Public Health, 20(10), 5812. https://doi.org/10.3390/ijerph20105812