
Who Is at High Risk for Child Abuse and Neglect: Risk Assessment among Battered Women Using Shelter Services

 ,
, 
 ,
, 

Abstract
1. Introduction
1.1. The Intersection of IPV and CAN: High Co-Occurrence and Severe Consequences
1.2. Risk Factors for Co-Occurrence of IPV and CAN
1.3. The Current Study
2. Materials and Methods
2.1. Research Site and Sample
2.2. Measures
2.2.1. Demographic Characteristics
2.2.2. IPV against Women
2.2.3. Child Abuse and Neglect
2.2.4. Risk Assessment
2.3. Statistical Analysis
3. Results
3.1. Victimization Experiences and Health Outcomes of Battered Women
3.2. Victimization Experiences of the Children Living in Shelters
3.3. Risk Factors of CAN among Battered Women
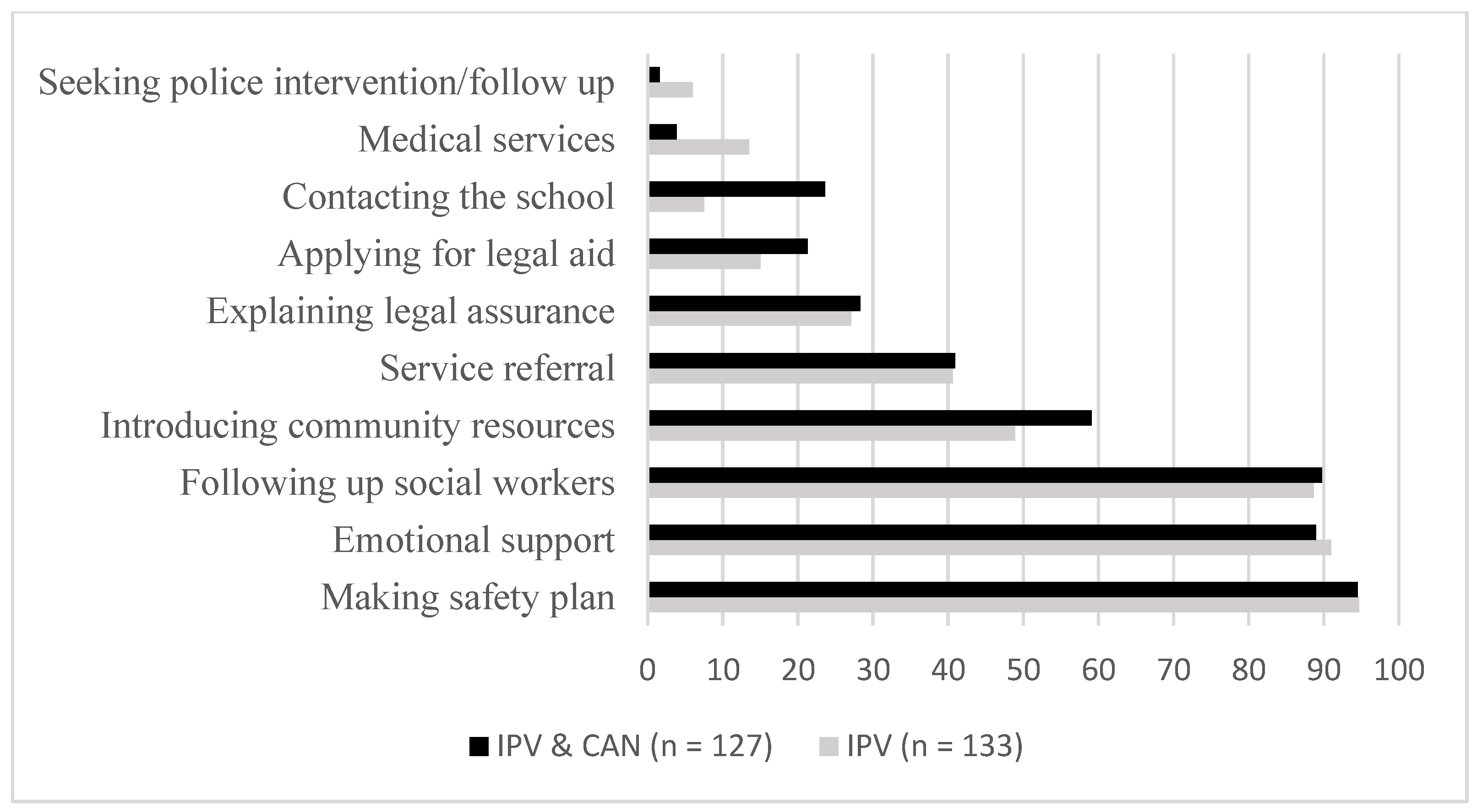
3.4. Risk Assessment and Management
4. Discussion
4.1. Implications
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Guedes, A.; Bott, S.; Garcia-Moreno, C.; Colombini, M. Bridging the Gaps: A Global Review of Intersections of Violence Against Women and Violence Against Children. Glob. Health Action 2016, 9, 31516. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Understanding and Addressing Violence Against Women. Available online: chrome-extension://efaidnbmnnnibpcajpcglclefindmkaj/https://apps.who.int/iris/bitstream/handle/10665/77432/WHO_RHR_12.36_eng.pdf;jsessionid=23A9DC1FC47B5BB1E0E51A85D277876A?sequence=1 (accessed on 10 December 2022).
- World Health Organization. Violence Against Children. Available online: https://www.who.int/health-topics/violence-against-children#tab=tab_1 (accessed on 10 December 2022).
- Chan, K.L.; Chen, Q.; Chen, M. Prevalence and Correlates of the Co-Occurrence of Family Violence: A Meta-Analysis on Family Polyvictimization. Trauma Violence Abus. 2021, 22, 289–305. [Google Scholar] [CrossRef] [PubMed]
- Dixon, L.; Hamilton-Giachritsis, C.; Browne, K.; Ostapuik, E. The Co-Occurrence of Child and Intimate Partner Maltreatment in the Family: Characteristics of the Violent Perpetrators. J. Fam. Violence 2007, 22, 675–689. [Google Scholar] [CrossRef]
- Herrenkohl, T.I.; Sousa, C.; Tajima, E.A.; Herrenkohl, R.C.; Moylan, C.A. Intersection of Child Abuse and Children’s Exposure to Domestic Violence. Trauma Violence Abus. 2008, 9, 84–99. [Google Scholar] [CrossRef]
- Jouriles, E.N.; McDonald, R.; Smith Slep, A.M.; Heyman, R.E.; Garrido, E. Child Abuse in the Context of Domestic Violence: Prevalence, Explanations, and Practice Implications. Violence Vict. 2008, 23, 221–235. [Google Scholar] [CrossRef]
- Jarvis, K.L.; Gordon, E.E.; Novaco, R.W. Psychological Distress of Children and Mothers in Domestic Violence Emergency Shelters. J. Fam. Violence 2005, 20, 389–402. [Google Scholar] [CrossRef]
- Holden, G.W. Children Exposed to Domestic Violence and Child Abuse: Terminology and Taxonomy. Clin. Child Fam. Psychol. Rev. 2003, 6, 151–160. [Google Scholar] [CrossRef]
- Forke, C.M.; Myers, R.K.; Fein, J.A.; Catallozzi, M.; Localio, A.R.; Wiebe, D.J.; Grisso, J.A. Witnessing Intimate Partner Violence as a Child: How Boys and Girls Model Their Parents’ Behaviors in Adolescence. Child Abus. Negl. 2018, 84, 241–252. [Google Scholar] [CrossRef]
- Brownridge, D.A.; Taillieu, T.; Afifi, T.; Chan, K.L.; Emery, C.; Lavoie, J.; Elgar, F. Child Maltreatment and Intimate Partner Violence among Indigenous and Non-Indigenous Canadians. J. Fam. Violence 2017, 32, 607–619. [Google Scholar] [CrossRef]
- Chan, K.L. Association between Childhood Sexual Abuse and Adult Sexual Victimization in a Representative Sample in Hong Kong Chinese. Child Abus. Negl. 2011, 35, 220–229. [Google Scholar] [CrossRef]
- Chan, K.L.; Yan, E.; Brownridge, D.A.; Tiwari, A.; Fong, D.Y.T. Childhood Sexual Abuse Associated with Dating Partner Violence and Suicidal Ideation in a Representative Household Sample in Hong Kong. J. Interpers. Violence. 2011, 26, 1763–1784. [Google Scholar] [CrossRef] [PubMed]
- Fulu, E.; Miedema, S.; Roselli, T.; McCook, S.; Chan, K.L.; Haardörfer, R.; Jewkes, R.; Fulu, E.; Jewkes, R.; Warner, X.; et al. Pathways between Childhood Trauma, Intimate Partner Violence, and Harsh Parenting: Findings from the UN Multi-Country Study on Men and Violence in Asia and the Pacific. Lancet Public Health 2017, 5, e512–e522. [Google Scholar] [CrossRef] [PubMed]
- Smith-Marek, E.N.; Cafferky, B.; Dharnidharka, P.; Mallory, A.B.; Dominguez, M.; High, J.; Stith, S.M.; Mendez, M. Effects of Childhood Experiences of Family Violence on Adult Partner Violence: A Meta-Analytic Review. J. Fam. Theory Rev. 2015, 7, 498–519. [Google Scholar] [CrossRef]
- Haselschwerdt, M.L.; Savasuk-Luxton, R.; Hlavaty, K. A Methodological Review and Critique of the “Intergenerational Transmission of Violence” Literature. Trauma Violence Abus. 2017, 20, 168–182. [Google Scholar] [CrossRef]
- Appel, A.E.; Holden, G.W. The Co-Occurrence of Spouse and Physical Child Abuse: A Review and Appraisal. J. Fam. Psychol. 1998, 12, 578–599. [Google Scholar] [CrossRef]
- Chiesa, A.E.; Kallechey, L.; Harlaar, N.; Rashaan Ford, C.; Garrido, E.F.; Betts, W.R.; Maguire, S. Intimate Partner Violence Victimization and Parenting: A Systematic Review. Child Abus. Negl. 2018, 80, 285–300. [Google Scholar] [CrossRef]
- Pu, D.F.; Rodriguez, C.M. Spillover and Crossover Effects: Mothers’ and Fathers’ Intimate Partner Violence, Parent-Child Aggression Risk, and Child Behavior Problems. Child Maltreat. 2021, 26, 420–430. [Google Scholar] [CrossRef]
- Chan, K.L. Children Exposed to Child Maltreatment and Intimate Partner Violence: A Study of Co-Occurrence among Hong Kong Chinese Families. Child Abus. Negl. 2011, 35, 532–542. [Google Scholar] [CrossRef][Green Version]
- Chan, K.L. Association between Intimate Partner Violence and Child Maltreatment in a Representative Student Sample in Hong Kong. Violence Against Women 2015, 21, 500–515. [Google Scholar] [CrossRef]
- Campbell, J.C. Health Consequences of Intimate Partner Violence. Lancet 2002, 359, 1331–1336. [Google Scholar] [CrossRef]
- Gilbert, R.; Widom, C.S.; Browne, K.; Fergusson, D.; Webb, E.; Janson, S. Burden and Consequences of Child Maltreatment in High-Income Countries. Lancet 2009, 373, 68–81. [Google Scholar] [CrossRef] [PubMed]
- Sousa, C.; Herrenkohl, T.I.; Moylan, C.A.; Tajima, E.A.; Klika, J.B.; Herrenkohl, R.C.; Russo, M.J. Longitudinal Study on the Effects of Child Abuse and Children’s Exposure to Domestic Violence, Parent-Child Attachments, and Antisocial Behavior in Adolescence. J. Interpers. Violence. 2010, 26, 111–136. [Google Scholar] [CrossRef] [PubMed]
- Fogarty, C.T.; Fredman, L.; Heeren, T.C.; Liebschutz, J. Synergistic Effects of Child Abuse and Intimate Partner Violence on Depressive Symptoms in Women. Prev. Med. 2008, 46, 463–469. [Google Scholar] [CrossRef]
- Goldstein, B.L.; Briggs-Gowan, M.J.; Grasso, D.J. The Effects of Intimate Partner Violence and a History of Childhood Abuse on Mental Health and Stress During Pregnancy. J. Fam. Violence 2021, 36, 337–346. [Google Scholar] [CrossRef] [PubMed]
- Fernández-González, L.; Calvete, E.; Orue, I.; Mauri, A. Victims of Domestic Violence in Shelters: Impacts on Women and Children. Span. J. Psychol. 2018, 21, E18. [Google Scholar] [CrossRef]
- Chan, K.L. Family Polyvictimization and Elevated Levels of Addiction and Psychopathology among Parents in a Chinese Household Sample. J. Interpers. Violence. 2017, 32, 2433–2452. [Google Scholar] [CrossRef]
- Sijtsema, J.J.; Stolz, E.A.; Bogaerts, S. Unique Risk Factors of the Co-Occurrence between Child Maltreatment and Intimate Partner Violence Perpetration. Eur. Psychol. 2020, 25, 122–133. [Google Scholar] [CrossRef]
- Gracia, E.; Rodriguez, C.M.; Martín-Fernández, M.; Lila, M. Acceptability of Family Violence: Underlying Ties between Intimate Partner Violence and Child Abuse. J. Interpers. Violence. 2017, 35, 3217–3236. [Google Scholar] [CrossRef]
- Humphreys, C. Domestic Violence and Child Protection: Exploring the Role of Perpetrator Risk Assessments. Child Fam. Soc. Work 2007, 12, 360–369. [Google Scholar] [CrossRef]
- Chan, K.L.; Brownridge, D.A.; Fong, D.Y.T.; Tiwari, A.; Leung, W.C.; Ho, P.C. Violence Against Pregnant Women Can Increase the Risk of Child Abuse: A Longitudinal Study. Child Abus. Negl. 2012, 36, 275–284. [Google Scholar] [CrossRef]
- Krishnakumar, A.; Buehler, C. Interparental Conflict and Parenting Behaviors: A Meta-Analytic Review. Fam. Relat. 2000, 49, 25–44. [Google Scholar] [CrossRef]
- Gracia, E.; López-Quílez, A.; Marco, M.; Lila, M. Neighborhood Characteristics and Violence behind Closed Doors: The Spatial Overlap of Child Maltreatment and Intimate Partner Violence. PLoS ONE 2018, 13, e0198684. [Google Scholar] [CrossRef] [PubMed]
- Gobin, R.L.; Iverson, K.M.; Mitchell, K.; Vaughn, R.; Resick, P.A. The Impact of Childhood Maltreatment on PTSD Symptoms among Female Survivors of Intimate Partner Violence. Violence Vict. 2013, 28, 984–999. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, C.M. Emotional Functioning, Attachment Style, and Attributions as Predictors of Child Abuse Potential in Domestic Violence Victims. Violence Vict. 2006, 21, 199–212. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Anderson, R.E.; Edwards, L.J.; Silver, K.E.; Johnson, D.M. Intergenerational Transmission of Child Abuse: Predictors of Child Abuse Potential among Racially Diverse Women Residing in Domestic Violence Shelters. Child Abus. Negl. 2018, 85, 80–90. [Google Scholar] [CrossRef]
- Straus, M.A.; Hamby, S.L.; Finkelhor, D.; Moore, D.W.; Runyan, D. Identification of Child Maltreatment with the Parent–Child Conflict Tactics Scales: Development and Psychometric Data for a National Sample of American Parents. Child Abus. Negl. 1998, 22, 249–270. [Google Scholar] [CrossRef]
- Chan, K.L. Co-Occurrence of Intimate Partner Violence and Child Abuse in Hong Kong Chinese families. J. Interpers. Violence. 2011, 26, 1322–1342. [Google Scholar] [CrossRef]
- Chan, K.L. Report on the Development of Risk Assessment Tools for Spouse Battering and Child Abuse in Hong Kong Chinese Families; A Consultancy Study Commissioned by the SWD of the HKSAR; Department of Social Work & Social Administration, The University of Hong Kong: Hong Kong, China, 2007. [Google Scholar]
- Choi, S.Y.P.; Cheung, Y.W.; Cheung, A.K.L. Social Isolation and Spousal Violence: Comparing Female Marriage Migrants with Local Women. J. Marriage Fam. 2012, 74, 444–461. [Google Scholar] [CrossRef]
- Lui, H.-K. Cross-Border Marriages in Pre- and Post-Handover Hong Kong. Popul. Space Place 2022. [Google Scholar] [CrossRef]
- Chiu, T.Y. Marriage Migration as a Multifaceted System: The Intersectionality of Intimate Partner Violence in Cross-Border Marriages. Violence Against Women 2016, 23, 1293–1313. [Google Scholar] [CrossRef]
- Carlson, B.E. Children Exposed to Intimate Partner Violence: Research Findings and Implications for Intervention. Trauma Violence Abus. 2000, 1, 321–342. [Google Scholar] [CrossRef]
- MacMillan, H.L.; Wathen, C.N.; Barlow, J.; Fergusson, D.M.; Leventhal, J.M.; Taussig, H.N. Interventions to Prevent Child Maltreatment and Associated Impairment. Lancet 2009, 373, 250–266. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.; Chan, K.L. Effects of Parenting Programs on Child Maltreatment Prevention: A Meta-Analysis. Trauma Violence Abus. 2016, 17, 88–104. [Google Scholar] [CrossRef] [PubMed]
- Leung, L. It’s a Matter of Trust: Policing Domestic Violence in Hong Kong. J. Interpers. Violence 2013, 29, 82–101. [Google Scholar] [CrossRef] [PubMed]
- Tonsing, K.N.; Tonsing, J.C. Exploring South Asian Qomen’s Experiences of Domestic Violence and Help-Seeking within the Sociocultural Context in Hong Kong. Violence Against Women 2019, 25, 1417–1432. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Total (N = 260) | IPV Only (N = 133) | IPV and CAN (N = 127) | χ2/t | |||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| Age range, in years | 41.75 *** | ||||||
| 18–30 | 45 | 17.4 | 23 | 17.3 | 22 | 17.5 | |
| 31–40 | 102 | 39.4 | 35 | 26.3 | 67 | 53.2 | |
| 41–50 | 69 | 26.6 | 35 | 26.3 | 34 | 27.0 | |
| >50 | 43 | 16.6 | 40 | 30.1 | 3 | 2.4 | |
| Age: Mean, SD | 40.6 | 11.4 | 43.8 | 13.8 | 37.2 | 6.9 | 4.95 *** |
| Ethnicity | 0.11 | ||||||
| Chinese | 238 | 91.5 | 121 | 91.0 | 117 | 92.1 | |
| Non-Chinese | 22 | 8.5 | 12 | 9 | 10 | 8.9 | |
| No. of children: Mean, SD | 1.7 | 0.75 | 1.68 | 0.69 | 1.74 | 0.83 | −0.58 |
| Residence | 12.82 *** | ||||||
| Born in HK | 68 | 26.2 | 43 | 32.3 | 25 | 19.7 | |
| <7 years in HK (new immigrants) | 84 | 32.3 | 30 | 22.5 | 54 | 42.5 | |
| 7 years or longer | 99 | 38.1 | 55 | 41.4 | 44 | 34.6 | |
| Non-local | 9 | 3.5 | 5 | 3.8 | 4 | 3.1 | |
| Marital status | 0.04 | ||||||
| Married/Cohabiting | 213 | 91.4 | 101 | 91.8 | 112 | 91.1 | |
| Divorced/Separated/Broken up | 20 | 8.6 | 9 | 8.2 | 11 | 8.9 | |
| Educational attainment | 2.02 | ||||||
| Primary or below | 44 | 17.0 | 26 | 19.7 | 18 | 14.2 | |
| Secondary | 176 | 68.0 | 89 | 67.4 | 87 | 68.5 | |
| Tertiary or above | 39 | 15.0 | 17 | 12.9 | 22 | 17.3 | |
| Monthly income | 1.19 | ||||||
| Less than HKD 7000 | 70 | 50 | 34 | 48.6 | 36 | 51.4 | |
| HKD 7000 to HKD 14,999 | 57 | 40.7 | 31 | 44.3 | 26 | 37.1 | |
| HKD 15,000 or above | 13 | 9.3 | 5 | 7.1 | 8 | 11.4 | |
| Receiving CSSA | 46 | 17.7 | 18 | 13.5 | 28 | 22.0 | 3.23 |
| Unemployed | 155 | 59.6 | 71 | 53.4 | 84 | 66.1 | 4.46 * |
| Has chronic health conditions | 68 | 26.2 | 49 | 36.8 | 19 | 15.0 | 16.11 *** |
| Diagnosed with mental illness | 50 | 19.2 | 29 | 21.8 | 21 | 16.5 | 1.16 |
| Characteristics | Total (N = 289) | IPV Only (N = 103) | IPV & CAN (N = 186) | χ2/t | |||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| Age range, in years | 3.52 | ||||||
| 0–5 | 114 | 39.4 | 48 | 46.6 | 66 | 35.5 | |
| 6–11 | 111 | 38.4 | 34 | 33.0 | 77 | 41.4 | |
| 12–17 | 64 | 22.1 | 21 | 20.4 | 43 | 23.1 | |
| Age: mean, SD | 7.39 | 4.62 | 6.62 | 4.54 | 7.82 | 4.62 | −2.11 * |
| Gender | 0.88 | ||||||
| Male | 151 | 52.2 | 50 | 48.5 | 101 | 54.3 | |
| Female | 138 | 47.8 | 53 | 51.5 | 85 | 45.7 | |
| Residence | 1.7 | ||||||
| Born in HK | 205 | 70.9 | 76 | 73.8 | 129 | 69.4 | |
| <7 years in HK (new immigrants) | 65 | 22.5 | 19 | 18.5 | 46 | 24.7 | |
| 7 years and longer | 12 | 4.2 | 5 | 4.9 | 7 | 3.8 | |
| Non-local | 7 | 2.4 | 3 | 2.9 | 4 | 2.2 | |
| Has chronic health conditions | 11 | 3.8 | 2 | 1.9 | 9 | 4.8 | 1.52 |
| Diagnosed with mental illness | 11 | 3.8 | 3 | 2.9 | 8 | 4.3 | 0.35 |
| Victimization/Outcome | Total (N = 260) | IPV Only (N = 133) | IPV & CAN (N = 127) | χ2/t | |||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| Abuser (harmed or threatened to harm participant) | 0.54 | ||||||
| Partner | 210 | 95.5 | 101 | 94.4 | 109 | 96.5 | |
| Ex-partner | 10 | 4.5 | 6 | 5.6 | 4 | 3.5 | |
| Years of being victimized | 4.95 | ||||||
| <5 years | 123 | 52.8 | 66 | 55 | 57 | 50.4 | |
| 5–10 years | 52 | 22.3 | 20 | 16.7 | 32 | 28.3 | |
| >10 years | 58 | 24.9 | 34 | 28.3 | 24 | 21.2 | |
| No. of abusive incidents in the past year | 3.41 | ||||||
| 1–5 times | 126 | 68.9 | 69 | 74.2 | 57 | 63.3 | |
| 6–10 times | 22 | 12.0 | 11 | 11.8 | 11 | 12.2 | |
| >10 times | 35 | 19.1 | 13 | 14.0 | 22 | 24.4 | |
| No. of abusive incidents in the past year: Mean, SD | 11.9 | 35.4 | 6.9 | 20.8 | 17.4 | 45.9 | −2.13 * |
| Compared with previous years, the past-year’s victimization was | 3.5 | ||||||
| More frequent | 123 | 53.9 | 63 | 53.8 | 60 | 54.1 | |
| Comparable | 71 | 31.1 | 41 | 35.0 | 30 | 27.0 | |
| Less frequent | 34 | 14.9 | 13 | 11.1 | 21 | 18.9 | |
| Currently has injuries or other physical issues | 97 | 40.6 | 57 | 45.6 | 40 | 35.1 | 2.73 |
| Level of injury | 0.58 | ||||||
| Minor (e.g., scratches, bruises, redness) | 110 | 81.5 | 62 | 83.8 | 48 | 78.7 | |
| Severe and/or permanent (e.g., fractures, severe bruises, coma, blindness, hearing loss, etc.) | 25 | 18.5 | 12 | 16.2 | 13 | 21.3 | |
| Has been threatened by the abuser in the past year | 198 | 76.4 | 97 | 73.5 | 101 | 79.5 | 1.31 |
| Has been forced to have sex with the abuser in the past year | 64 | 24.9 | 24 | 18.3 | 40 | 31.7 | 6.19 * |
| Is afraid of the abuser | 197 | 76.7 | 98 | 74.8 | 99 | 78.6 | 0.51 |
| Is still in contact with the abuser | 74 | 28.9 | 37 | 28.0 | 37 | 29.8 | 0.10 |
| Thinks the abuser will track her and her children down | 142 | 57.7 | 64 | 41.6 | 78 | 63.9 | 3.83 # |
| Is still currently harassed by the abuser | 52 | 20.5 | 25 | 18.9 | 27 | 22.1 | 0.4 |
| Current health problems | |||||||
| Insomnia | 98 | 37.7 | 53 | 39.8 | 45 | 35.4 | 0.61 |
| Headache | 52 | 20.0 | 28 | 21.1 | 24 | 18.9 | 0.20 |
| Muscle pain | 23 | 8.8 | 10 | 7.5 | 13 | 10.2 | 0.60 |
| Loss of appetite | 34 | 13.1 | 19 | 14.3 | 15 | 11.8 | 0.37 |
| Tiredness | 42 | 16.2 | 17 | 12.8 | 25 | 19.7 | 2.33 |
| Substance dependence | 10 | 3.8 | 7 | 5.3 | 3 | 2.4 | 1.50 |
| Panic/Fear/Nervousness | 71 | 27.3 | 36 | 27.1 | 35 | 27.6 | 0.01 |
| Upset | 81 | 31.2 | 51 | 38.3 | 30 | 23.6 | 7.09 |
| Anxious | 29 | 11.2 | 16 | 12.0 | 13 | 10.2 | 0.22 |
| Other | 35 | 13.5 | 21 | 15.8 | 14 | 11.0 | 1.31 |
| Any symptom above | 169 | 65.0 | 90 | 67.7 | 79 | 62.2 | 0.85 |
| Has suicidal ideation | 142 | 54.6 | 77 | 57.9 | 65 | 51.2 | 1.18 |
| Forms of Abuse/Neglect | IPV & CAN (N ^ = 186) | Perpetrator–Women | Perpetrator–Partner | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | % | n | Past 6 Months (%) | Past 12 Months (%) | n | Before 12 Months (%) | n | Past 6 Months (%) | n | Past 12 Months (%) | n | Before 12 Months (%) | ||
| Psychological aggression | 168 | 90.3 | 20 | 11.9 | 1 | 0.6 | 6 | 3.6 | 140 | 83.3 | 8 | 4.8 | 2 | 1.2 |
| Physical assault | 117 | 62.9 | 20 | 17.1 | 4 | 3.4 | 5 | 4.3 | 73 | 62.4 | 8 | 6.8 | 13 | 11.1 |
| Sexual abuse | 2 | 1.1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 50.0 | 1 | 50.0 | |
| Neglect | 19 | 10.2 | 3 | 15.8 | 1 | 5.3 | 0 | 0 | 14 | 73.7 | 2 | 10.5 | 1 | 5.3 |
| Variables | IPV Only (N = 133) | IPV & CAN (N = 127) | Crude OR | ||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Characteristics of battered women | |||||
| Age: mean, SD | 43.8 | 13.8 | 37.2 | 6.9 | 0.94 *** (0.92, 0.97) |
| Educational attainment (ref: tertiary or above) | 115 | 86.5 | 105 | 82.7 | 0.71 (0.36, 1.40) |
| Unemployed | 71 | 53.4 | 84 | 66.1 | 1.72 * (1.04, 2.85) |
| Divorced/Separated (ref: married/cohabiting) | 9 | 8.2 | 11 | 8.9 | 1.10 (0.44, 2.77) |
| Characteristics of battered women/family members | |||||
| Disabled | 8 | 6.0 | 10 | 7.9 | 1.32 (0.51, 3.47) |
| Mentally ill | 35 | 26.3 | 37 | 29.1 | 1.17 (0.67, 2.03) |
| Chronic disease | 57 | 42.9 | 35 | 27.6 | 0.50 ** (0.30, 0.84) |
| New immigrants | 49 | 36.8 | 65 | 51.2 | 1.78 * (1.08, 2.92) |
| Low-income or receiving social security | 62 | 46.6 | 63 | 49.6 | 1.08 (0.66, 1.78) |
| In debt | 38 | 28.6 | 38 | 29.9 | 1.14 (0.66, 1.99) |
| Addicted to gambling | 30 | 22.6 | 24 | 18.9 | 0.79 (0.43, 1.46) |
| Unemployed | 91 | 68.4 | 86 | 67.7 | 1.03 (0.60, 1.76) |
| Spousal age difference (>10 years) | 29 | 21.8 | 40 | 31.5 | 1.52 (0.87, 2.67) |
| Frequent daily conflict with partner | 104 | 78.2 | 119 | 93.7 | 4.58 ** (1.66, 12.63) |
| Conflict with in-laws | 14 | 10.5 | 25 | 19.7 | 1.93 (0.95, 3.92) |
| Characteristics of abusers | |||||
| Experienced childhood abuse or neglect | 23 | 17.3 | 24 | 18.9 | 1.19 (0.61, 2.30) |
| Witnessed violence between parents | 18 | 13.5 | 27 | 21.3 | 1.66 (0.84, 3.30) |
| History of criminal offence | 20 | 15.0 | 25 | 19.7 | 1.52 (0.78, 2.94) |
| History of sexual abuse | 4 | 3.0 | 1 | 0.8 | 0.26 (0.03, 2.34) |
| History of perpetrating CAN/IPV | 49 | 36.8 | 60 | 47.2 | 1.52 (0.90, 2.57) |
| Low self-esteem | 51 | 38.3 | 51 | 40.2 | 1.24 (0.73, 2.09) |
| Approves of violence | 71 | 53.4 | 85 | 66.9 | 2.39 ** (1.28, 4.46) |
| Poor anger management | 116 | 87.2 | 118 | 92.9 | 1.45 (0.53, 3.95) |
| High level of stress | 74 | 55.6 | 96 | 75.6 | 2.59 ** (1.43, 4.70) |
| Keen on face-saving | 116 | 87.2 | 106 | 83.5 | 0.59 (0.26, 1.32) |
| Disregards social norms | 48 | 36.1 | 48 | 37.8 | 0.97 (0.57, 1.64) |
| Jealousy issues | 67 | 50.4 | 64 | 50.4 | 0.90 (0.54, 1.51) |
| Shifts responsibility | 109 | 82.0 | 116 | 91.3 | 2.13 (0.92, 4.94) |
| Manipulates partner | 80 | 60.2 | 89 | 70.1 | 1.27 (0.74, 2.17) |
| Has suicidal ideation | 27 | 20.3 | 25 | 19.7 | 0.98 (0.53, 1.81) |
| Alcohol addiction | 32 | 24.1 | 33 | 26.0 | 1.06 (0.61, 1.87) |
| Drug abuse | 15 | 11.3 | 22 | 17.3 | 1.63 (0.80, 3.31) |
| Depression | 32 | 24.1 | 29 | 22.8 | 0.91 (0.50, 1.64) |
| Antisocial personality disorder | 12 | 9.0 | 9 | 7.1 | 0.76 (0.31, 1.88) |
| Borderline personality disorder | 11 | 8.3 | 7 | 5.5 | 0.62 (0.23, 1.66) |
| Risks | Total (N = 260) | IPV Only (N = 133) | IPV & CAN (N = 127) | χ2 | |||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| Severe violence | 0.93 | ||||||
| Low | 22 | 8.5 | 12 | 9.1 | 10 | 7.9 | |
| Medium | 26 | 10.0 | 11 | 8.3 | 15 | 11.8 | |
| High | 211 | 81.5 | 109 | 82.6 | 102 | 80.3 | |
| Recidivism | 3.42 | ||||||
| Low | 12 | 4.6 | 6 | 4.5 | 6 | 4.7 | |
| Medium | 53 | 20.5 | 33 | 25.0 | 20 | 15.7 | |
| High | 194 | 74.9 | 93 | 70.5 | 101 | 79.5 | |
| General risk | 1.7 | ||||||
| Low | 6 | 2.3 | 2 | 1.5 | 4 | 3.1 | |
| Medium | 32 | 12.4 | 19 | 14.4 | 13 | 10.2 | |
| High | 221 | 85.3 | 111 | 84.1 | 110 | 86.6 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chan, K.L.; Chen, M.; Lo, C.K.M.; Chen, X.Y.; Tang, D.; Ip, P. Who Is at High Risk for Child Abuse and Neglect: Risk Assessment among Battered Women Using Shelter Services. Int. J. Environ. Res. Public Health 2023, 20, 833. https://doi.org/10.3390/ijerph20010833
Chan KL, Chen M, Lo CKM, Chen XY, Tang D, Ip P. Who Is at High Risk for Child Abuse and Neglect: Risk Assessment among Battered Women Using Shelter Services. International Journal of Environmental Research and Public Health. 2023; 20(1):833. https://doi.org/10.3390/ijerph20010833
Chicago/Turabian StyleChan, Ko Ling, Mengtong Chen, Camilla K. M. Lo, Xiao Yan Chen, Debbie Tang, and Patrick Ip. 2023. "Who Is at High Risk for Child Abuse and Neglect: Risk Assessment among Battered Women Using Shelter Services" International Journal of Environmental Research and Public Health 20, no. 1: 833. https://doi.org/10.3390/ijerph20010833
APA StyleChan, K. L., Chen, M., Lo, C. K. M., Chen, X. Y., Tang, D., & Ip, P. (2023). Who Is at High Risk for Child Abuse and Neglect: Risk Assessment among Battered Women Using Shelter Services. International Journal of Environmental Research and Public Health, 20(1), 833. https://doi.org/10.3390/ijerph20010833