
The Epidemiology of Malignant Melanoma during the First Two Years of the COVID-19 Pandemic: A Systematic Review
 ,
, 
Abstract
1. Introduction
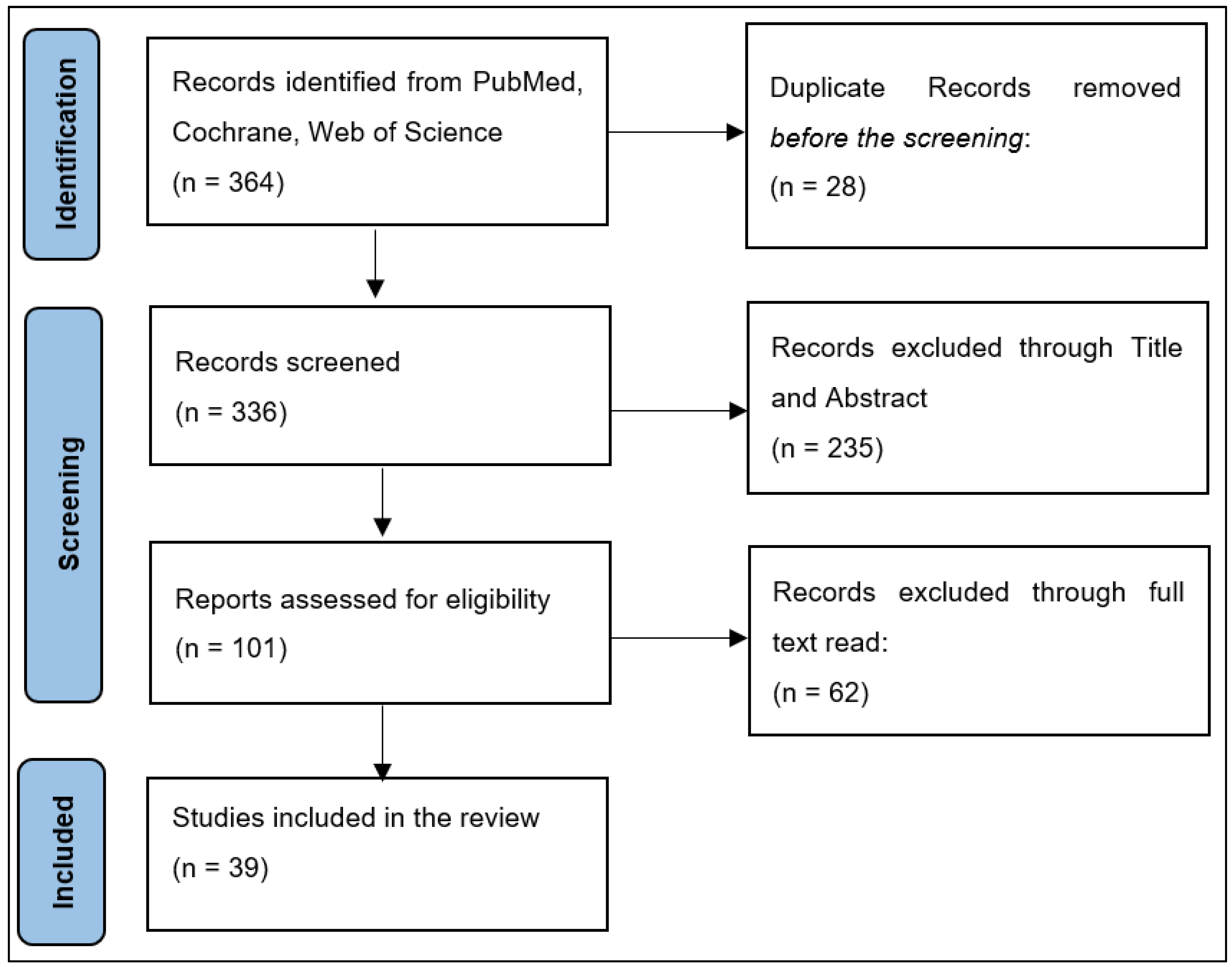
2. Materials and Methods
2.1. Study Design
Question 1: What percentage of malignant melanoma screenings and treatments were delayed during the COVID-19 pandemic?
Question 2: What is the degree of change in the malignant melanoma stage at diagnosis and Breslow depth index during the COVID-19 pandemic?
Question 3: Are there significant differences in short-term outcomes of patients with malignant melanoma during the COVID-19 pandemic?
2.2. Selection Criteria
2.3. Quality Assessment
2.4. Data Extraction
3. Results
3.1. Study Characteristics
3.2. COVID-19 Pandemic Effects on Malignant Melanoma
4. Discussion
4.1. Decreased Patient Presentation
4.2. Increased Staging and Grading
4.3. Management of Malignant Melanoma during the COVID-19 Pandemic
4.4. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Miyah, Y.; Benjelloun, M.; Lairini, S.; Lahrichi, A. COVID-19 Impact on Public Health, Environment, Human Psychology, Global Socioeconomy, and Education. Sci. World J. 2022, 2022, 5578284. [Google Scholar] [CrossRef] [PubMed]
- Bell, L.; van Gemert, C.; Merilles, O.E., Jr.; Cash, H.L.; Stoové, M.; Hellard, M. The impact of COVID-19 on public health systems in the Pacific Island Countries and Territories. Lancet Reg. Health West Pac. 2022, 25, 100498. [Google Scholar] [CrossRef]
- Sharma, A.; Tiwari, S.; Deb, M.K.; Marty, J.L. Severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2): A global pandemic and treatment strategies. Int. J. Antimicrob. Agents 2020, 56, 106054. [Google Scholar] [CrossRef] [PubMed]
- Iftekhar, E.N.; Priesemann, V.; Balling, R.; Bauer, S.; Beutels, P.; Valdez, A.C.; Cuschieri, S.; Czypionka, T.; Dumpis, U.; Glaab, E.; et al. A look into the future of the COVID-19 pandemic in Europe: An expert consultation. Lancet Reg. Health Eur. 2021, 8, 100185. [Google Scholar] [CrossRef] [PubMed]
- Glass, D.H. European and US lockdowns and second waves during the COVID-19 pandemic. Math. Biosci. 2020, 330, 108472. [Google Scholar] [CrossRef]
- Pujolar, G.; Oliver-Anglès, A.; Vargas, I.; Vázquez, M.-L. Changes in Access to Health Services during the COVID-19 Pandemic: A Scoping Review. Int. J. Environ. Res. Public Health 2022, 19, 1749. [Google Scholar] [CrossRef]
- Núñez, A.; Sreeganga, S.; Ramaprasad, A. Access to Healthcare during COVID-19. Int. J. Environ. Res. Public Health 2021, 18, 2980. [Google Scholar] [CrossRef]
- Silvia, C.; Denis, C.; Mario, C.; Luigi, V.; Federico, T.; Marcello, C. Impact of COVID-19 Pandemic on Non-Melanoma Skin Cancer’s Tumor Burden and Care: A Multi-Center Stdy based in Northern Italy. J. Plast. Reconstr. Aesthetic Surg. 2022, 75, 3616–3621. [Google Scholar] [CrossRef]
- Seretis, K.; Boptsi, E.; Boptsi, A.; Lykoudis, E.G. The impact of treatment delay on skin cancer in COVID-19 era: A case-control study. World J. Surg. Oncol. 2021, 19, 350. [Google Scholar] [CrossRef]
- Tejera-Vaquerizo, A.; Nagore, E. Estimated effect of COVID-19 lockdown on melanoma thickness and prognosis: A rate of growth model. J. Eur. Acad. Dermatol. Venereol. 2020, 34, e351–e353. [Google Scholar] [CrossRef]
- Makaranka, S.; Scutt, F.; Rahman, K. The Impact of the COVID-19 Pandemic on Diagnosis of Skin Cancer Cases in North Cancer Alliance and Scotland. Cureus 2022, 14, e25019. [Google Scholar] [CrossRef] [PubMed]
- Aabed, H.; Bloanca, V.; Crainiceanu, Z.; Bratosin, F.; Citu, C.; Diaconu, M.M.; Ciorica, O.; Bratu, T. The Impact of SARS-CoV-2 Pandemic on Patients with Malignant Melanoma at a Romanian Academic Center: A Four-Year Retrospective Analysis. Int. J. Environ. Res. Public Health 2022, 19, 8499. [Google Scholar] [CrossRef] [PubMed]
- Schiavo, J.H. PROSPERO: An International Register of Systematic Review Protocols. Med. Ref. Serv. Q. 2019, 38, 171–180. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ Br. Med. J. 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Tran, L.; Tam, D.N.H.; Elshafay, A.; Dang, T.; Hirayama, K.; Huy, N.T. Quality assessment tools used in systematic reviews of in vitro studies: A systematic review. BMC Med. Res. Methodol. 2021, 21, 101. [Google Scholar] [CrossRef]
- Filoni, A.; Del Fiore, P.; Cappellesso, R.; Dall’Olmo, L.; Salimian, N.; Spina, R.; Tropea, S.; Rastrelli, M.; Russano, F.; D’Amico, M.; et al. Management of melanoma patients during COVID-19 pandemic in an Italian skin unit. Dermatol. Ther. 2021, 34, e14908. [Google Scholar] [CrossRef]
- Cariti, C.; Merli, M.; Avallone, G.; Rubatto, M.; Marra, E.; Fava, P.; Caliendo, V.; Picciotto, F.; Gualdi, G.; Stanganelli, I.; et al. Melanoma Management during the COVID-19 Pandemic Emergency: A Literature Review and Single-Center Experience. Cancers 2021, 13, 6071. [Google Scholar] [CrossRef]
- Wong, W.L.; Ross, P.; Peters, K.; Frenz, M.; Hai, T.; Ridgeon, A.; Toop, R.; Strouhal, P.; Bomanji, J. The COVID-19 pandemic: Impact on NHS England PET-CT services and lessons learnt. Nucl. Med. Commun. 2020, 42, 127–137. [Google Scholar] [CrossRef]
- Dika, E.; Barisani, A.; Baraldi, C.; Pepe, F.; Patrizi, A.; Vaccari, S. COVID-19 and melanoma surgery in a dermo-oncology centre in Italy. Clin. Exp. Dermatol. 2021, 46, 1134. [Google Scholar] [CrossRef]
- Tejera-Vaquerizo, A.; Paradela, S.; Toll, A.; Santos-Juanes, J.; Jaka, A.; López, A.; Cañueto, J.; Villegas-Romero, I.; Fernández-Pulido, C.; Perandones, H.; et al. Effects of COVID-19 Lockdown on Tumour Burden of Melanoma and Cutaneous Squamous Cell Carcinoma. Acta Derm. Venereol. 2021, 101, adv00525. [Google Scholar] [CrossRef]
- Martinez-Lopez, A.; Diaz-Calvillo, P.; Cuenca-Barrales, C.; Montero-Vilchez, T.; Sanchez-Diaz, M.; Buendia-Eisman, A.; Arias-Santiago, S. Impact of the COVID-19 Pandemic on the Diagnosis and Prognosis of Melanoma. J. Clin. Med. 2022, 11, 4181. [Google Scholar] [CrossRef] [PubMed]
- Gisondi, P.; Cazzaniga, S.; Di Leo, S.; Piaserico, S.; Bellinato, F.; Pizzolato, M.; Gatti, A.; Eccher, A.; Brunelli, M.; Saraggi, D.; et al. Impact of the COVID-19 pandemic on melanoma diagnosis. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e714–e715. [Google Scholar] [CrossRef] [PubMed]
- Guven, D.C.; Sahin, T.K.; Yildirim, H.C.; Cesmeci, E.; Incesu, F.G.G.; Tahillioglu, Y.; Ucgul, E.; Aksun, M.S.; Gurbuz, S.C.; Aktepe, O.H.; et al. Newly diagnosed cancer and the COVID-19 pandemic: Tumour stage migration and higher early mortality. BMJ Support. Palliat. Care 2021. online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Cocuz, I.-G.; Cocuz, M.-E.; Niculescu, R.; Șincu, M.; Tinca, A.; Sabău, A.-H.; Chiorean, D.; Morariu, S.; Cotoi, O. The Impact of and Adaptations Due to the COVID-19 Pandemic on the Histopathological Diagnosis of Skin Pathologies, Including Non-Melanocyte and Melanoma Skin Cancers—A Single-Center Study in Romania. Medicina 2021, 57, 533. [Google Scholar] [CrossRef] [PubMed]
- Pala, L.; Conforti, F.; Saponara, M.; De Pas, T.; Giugliano, F.; Salè, E.O.; Jemos, C.; Rubatto, M.; Agostini, A.; Quaglino, P.; et al. Data of Italian Cancer Centers from two regions with high incidence of SARS CoV-2 infection provide evidence for the successful management of patients with locally advanced and metastatic melanoma treated with immunotherapy in the era of COVID-19. Semin. Oncol. 2020, 47, 302–304. [Google Scholar] [CrossRef]
- Intergruppo Melanoma Italiano. The effect of COVID-19 emergency in the management of melanoma in Italy. Dermatol. Rep. 2021, 13, 8972. [Google Scholar] [CrossRef]
- Gualdi, G.; Porreca, A.; Amoruso, G.F.; Atzori, L.; Calzavara-Pinton, P.; De Tursi, M.; Di Buduo, A.; Di Marino, P.; Fabroncini, G.; Fantini, F.; et al. The Effect of the COVID-19 Lockdown on Melanoma Diagnosis in Italy. Clin. Dermatol. 2021, 39, 911–919. [Google Scholar] [CrossRef]
- Davis, C.H.; Ho, J.; Greco, S.H.; Koshenkov, V.P.; Vidri, R.J.; Farma, J.M.; Berger, A.C. COVID-19 is Affecting the Presentation and Treatment of Melanoma Patients in the Northeastern United States. Ann. Surg. Oncol. 2022, 29, 1629–1635. [Google Scholar] [CrossRef]
- Berry, W.; Tan, K.; Haydon, A.; Shackleton, M.; Mar, V.J. Reduced melanoma referrals during COVID-19 lockdown. Aust. J. Gen. Pract. 2021, 50, 50. [Google Scholar] [CrossRef]
- Asai, Y.; Nguyen, P.; Hanna, T.P. Impact of the COVID-19 pandemic on skin cancer diagnosis: A population-based study. PLoS ONE 2021, 16, e0248492. [Google Scholar] [CrossRef]
- Weston, G.K.; Jeong, H.S.; Mu, E.W.; Polsky, D.; Meehan, S.A. Impact of COVID-19 on melanoma diagnosis. Melanoma Res. 2021, 31, 280–281. [Google Scholar] [CrossRef] [PubMed]
- Kleemann, J.; Meissner, M.; Özistanbullu, D.; Balaban, Ü.; Old, O.; Kippenberger, S.; Kloka, J.; Kaufmann, R.; Zacharowski, K.; Friedrichson, B. Impact of the Covid-19 pandemic on melanoma and non-melanoma skin cancer inpatient treatment in Germany—A nationwide analysis. J. Eur. Acad. Dermatol. Venereol. 2022, 36, 1766–1773. [Google Scholar] [CrossRef] [PubMed]
- Chang, M.S.; A Leachman, S.; Berry, E.G.; Curiel-Lewandrowski, C.; Geller, A.C.; Grossman, D.; Kim, C.C.; A Stein, J.; Swetter, S.M.; I Hartman, R. Changes in melanoma care practices during the COVID-19 pandemic: A multi-institutional cross-sectional survey. Dermatol. Online J. 2021, 27, 18. [Google Scholar] [CrossRef]
- Ricci, F.; Di Lella, G.; Fania, L.; Sobrino, L.; Pallotta, S.; Panebianco, A.; Fortes, C.; Abeni, D. Primitive melanoma and covid-19: Are we still paying the price of the pandemic? J. Eur. Acad. Dermatol. Venereol. 2021, 36, e260–e261. [Google Scholar] [CrossRef]
- Micek, A.; Diehl, K.; Teuscher, M.; Schaarschmidt, M.; Sasama, B.; Ohletz, J.; Burbach, G.; Kiecker, F.; Hillen, U.; Harth, W.; et al. Melanoma care during one year pandemic in Berlin: Decreasing appointment cancellations despite increasing COVID-19 concern. JDDG J. Dtsch. Dermatol. Ges. 2022, 20, 962–978. [Google Scholar] [CrossRef] [PubMed]
- Shannon, A.B.; Sharon, C.E.; Straker, R.J.; Miura, J.T.; Ming, M.E.; Chu, E.Y.; Karakousis, G.C. The impact of the COVID-19 pandemic on the presentation status of newly diagnosed melanoma: A single institution experience. J. Am. Acad. Dermatol. 2020, 84, 1096–1098. [Google Scholar] [CrossRef] [PubMed]
- Hoellwerth, M.; Kaiser, A.; Emberger, M.; Brandlmaier, M.; Laimer, M.; Egger, A.; Bauer, J.W.; Koelblinger, P. COVID-19-Induced Reduction in Primary Melanoma Diagnoses: Experience from a Dermatopathology Referral Center. J. Clin. Med. 2021, 10, 4059. [Google Scholar] [CrossRef]
- Van Not, O.J.; van Breeschoten, J.; van den Eertwegh, A.J.M.; Hilarius, D.L.; De Meza, M.M.; Haanen, J.B.; Blank, C.U.; Aarts, M.J.B.; van den Berkmortel, F.W.; de Groot, J.W.B.; et al. The unfavorable effects of COVID-19 on Dutch advanced melanoma care. Int. J. Cancer 2022, 150, 816–824. [Google Scholar] [CrossRef]
- Lamm, R.; Lyons, W.; So, W.; Willis, A.I. Advanced-Stage Melanoma at Presentation Following the Peak of the Pandemic: A COVID-19 Cancer Canary in a Coal Mine. World J. Surg. 2022, 46, 1820–1825. [Google Scholar] [CrossRef]
- Welzel, J.; Augustin, M.; Gutzmer, R. Impact of the COVID-19 pandemic on the care of patients with malignant melanoma. JDDG J. Dtsch. Dermatol. Ges. 2022, 20, 1028–1030. [Google Scholar] [CrossRef]
- Gedeah, C.; Damsin, T.; Absil, G.; Somja, J.; Collins, P.; Rorive, A.; Marchal, N.; Seidel, L.; Nikkels, A.F. The impact of COVID-19 on the new diagnoses of melanoma. Eur. J. Dermatol. 2021, 31, 565–567. [Google Scholar] [CrossRef] [PubMed]
- McFeely, O.; Hollywood, A.; Stanciu, M.; O’Connell, M.; Paul, L. Comment on “The impact of the COVID-19 pandemic on the presentation status of newly diagnosed melanoma: A single institution experience”. J. Am. Acad. Dermatol. 2021, 85, e419–e420. [Google Scholar] [CrossRef] [PubMed]
- Kostner, L.; Cerminara, S.E.; Pamplona, G.S.P.; Maul, J.-T.; Dummer, R.; Ramelyte, E.; Mangana, J.; Wagner, N.B.; Cozzio, A.; Kreiter, S.; et al. Effects of COVID-19 Lockdown on Melanoma Diagnosis in Switzerland: Increased Tumor Thickness in Elderly Females and Shift towards Stage IV Melanoma during Lockdown. Cancers 2022, 14, 2360. [Google Scholar] [CrossRef] [PubMed]
- Molinier, R.; Roger, A.; Genet, B.; Blom, A.; Longvert, C.; Chaplain, L.; Fort, M.; Saiag, P.; Funck-Brentano, E. Impact of the French COVID-19 pandemic lockdown on newly diagnosed melanoma delay and severity. J. Eur. Acad. Dermatol. Venereol. 2021, 36, e164–e166. [Google Scholar] [CrossRef]
- Valenti, M.; Pavia, G.; Gargiulo, L.; Facheris, P.; Nucca, O.; Mancini, L.; Sacrini, F.; Borroni, R.G.; Narcisi, A.; Costanzo, A. Impact of delay in follow-up due to COVID-19 pandemic on skin cancer progression: A real-life experience from an Italian hub hospital. Int. J. Dermatol. 2021, 60, 860–863. [Google Scholar] [CrossRef] [PubMed]
- Trepanowski, N.; Chang, M.S.; Zhou, G.; Ahmad, M.; Berry, E.G.; Bui, K.; Butler, W.H.; Chu, E.Y.; Curiel-Lewandrowski, C.; Dellalana, L.E.; et al. Delays in melanoma presentation during the COVID-19 pandemic: A nationwide multi-institutional cohort study. J. Am. Acad. Dermatol. 2022, 87, 1217–1219. [Google Scholar] [CrossRef] [PubMed]
- Barcaui, C.B.; Machado, C.J.; Piñeiro-Maceira, J. Impact of the SARS-CoV-2 pandemic on the diagnosis of primary cutaneous melanoma at a University Hospital in Rio de Janeiro. An. Bras. Dermatol. 2022, 97, 801–803. [Google Scholar] [CrossRef]
- Balakirski, G.; Michalowitz, A.; Kreuter, A.; Hofmann, S. Long-term effects of the COVID-19 pandemic on malignant melanoma: Increased lymph node metastases in two German dermatology clinics. J. Eur. Acad. Dermatol. Venereol. 2022, 36, e762–e764. [Google Scholar] [CrossRef]
- Shaikh, S.S.; Yang, X.; Fortman, D.D.; Wang, H.; Davar, D.; Luke, J.J.; Zarour, H.; Kirkwood, J.M.; Najjar, Y.G. A retrospective analysis of the impact of the COVID-19 pandemic on staging at presentation of patients with invasive melanoma. J. Am. Acad. Dermatol. 2022, 87, 906–908. [Google Scholar] [CrossRef]
- Villani, A.; Fabbrocini, G.; Scalvenzi, M. The reduction in the detection of melanoma during the coronavirus disease 2019 (COVID-19) pandemic in a melanoma center of South Italy. J. Dermatol. Treat. 2020, 33, 1778. [Google Scholar] [CrossRef]
- Koch, E.; Villanueva, F.; Marchetti, M.A.; Abarzúa-Araya, Á.; Cárdenas, C.; Castro, J.C.; Dominguez, F.; Droppelmann, K.; Droppelmann, N.; Galindo, H.; et al. Reduction in the number of early melanomas diagnosed during the COVID-19 pandemic: A single-centre cohort study. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e735–e737. [Google Scholar] [CrossRef] [PubMed]
- Sangers, T.E.; Wakkee, M.; Kramer-Noels, E.C.; Nijsten, T.; Louwman, M.W.; Jaspars, E.H.; Hollestein, L.M. Limited impact of COVID-19-related diagnostic delay on cutaneous melanoma and squamous cell carcinoma tumour characteristics: A nationwide pathology registry analysis. Br. J. Dermatol. 2022, 187, 196–202. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Dowling, J.P.; Murray, W.K.; McArthur, G.A.; Thompson, J.F.; Wolfe, R.; Kelly, J.W. Rate of growth in melanomas: Characteristics and associations of rapidly growing melanomas. Arch. Dermatol. 2006, 142, 1551–1558. [Google Scholar] [CrossRef] [PubMed]
- Tejera-Vaquerizo, A.; Nagore, E.; Meléndez, J.J.; López-Navarro, N.; Martorell-Calatayud, A.; Herrera-Acosta, E.; Traves, V.; Guillén, C.; Herrera-Ceballos, E. Chronology of Metastasis in Cutaneous Melanoma: Growth Rate Model. J. Investig. Dermatol. 2012, 132, 1215–1221. [Google Scholar] [CrossRef] [PubMed]
- Kwatra, S.G.; Sweren, R.J.; Grossberg, A.L. Dermatology practices as vectors for COVID-19 transmission: A call for immediate cessation of non-emergent dermatology visits. J. Am. Acad. Dermatol. 2020, 82, e179–e180. [Google Scholar] [CrossRef]
- Nazzaro, G.; Marzano, A.V.; Berti, E. What is the role of a dermatologist in the battle against COVID-19? The experience from a hospital on the frontline in Milan. Int. J. Dermatol. 2020, 59, e238–e239. [Google Scholar] [CrossRef]
- Morrone, A.; Cristaudo, A.; Ardigò, M.; Frascione, P.; Giuliani, M. Rescheduling of clinical activities and teleconsulting for public dermatology. Two prompt answers to COVID-19 emergency. Int. J. Dermatol. 2020, 59, e237–e238. [Google Scholar] [CrossRef]
- Kumar, S.; Bishnoi, A.; Vinay, K. Changing paradigms of dermatology practice in developing nations in the shadow of COVID-19: Lessons learnt from the pandemic. Dermatol. Ther. 2020, 33, e13472. [Google Scholar] [CrossRef]
- Temiz, S.A.; Dursun, R.; Daye, M.; Ataseven, A. Evaluation of dermatology consultations in the era of COVID-19. Dermatol. Ther. 2020, 33, e1364. [Google Scholar] [CrossRef]
- Sheriff, T.; Murrell, O.G.C.; Murrell, D.F. Restructuring an academic dermatology practice during theCOVID-19 pandemic. Dermatol. Ther. 2020, 33, e13684. [Google Scholar] [CrossRef]
- Litchman, G.H.; Rigel, D.S. The immediate impact of COVID-19 on US dermatology practices. J. Am. Acad. Dermatol. 2020, 83, 685–686. [Google Scholar] [CrossRef] [PubMed]
- Neagoe, O.C.; Ionica, M.; Mazilu, O. Use of methylene blue in the prevention of recurrent intra-abdominal postoperative adhesions. J. Int. Med. Res. 2018, 46, 504–510. [Google Scholar] [CrossRef]
- Petrovici, I.; Ionica, M.; Neagoe, O.C. Economic Crisis: A Factor for the Delayed Diagnosis of Breast Cancer. Int. J. Environ. Res. Public Health 2021, 18, 3998. [Google Scholar] [CrossRef] [PubMed]
- Geskin, L.J.; Trager, M.H.; Aasi, S.Z.; Bickers, D.R.; Carvajal, R.D.; Nghiem, P.; Taback, B.; Zeitouni, N.C.; Samie, F.H. Perspectives on the recommendations for skin cancer management during the COVID-19 pandemic. J. Am. Acad. Dermatol. 2020, 83, 295–296. [Google Scholar] [CrossRef] [PubMed]
- Giacalone, S.; Bortoluzzi, P.; Nazzaro, G. Which are the “emergent” dermatologic practices during COVID-19 pandemic? Report from the lockdown in Milan, Italy. Int. J. Dermatol. 2020, 59, e269–e270. [Google Scholar] [CrossRef]
- Sarriugarte Aldecoa-Otalora, J.; Loidi Pascual, L.; Cordoba Iturriagagoitia, A.; Yanguas Bayona, J.I. How Has the COVID-19 Pandemic and Lockdown Affected Breslow Thickness in Cutaneous Melanoma? Actas Dermosifiliogr. 2021, 113, 107–109. [Google Scholar] [CrossRef]
- Nazzaro, G.; Passoni, E.; Pozzessere, F.; Maronese, C.A.; Marzano, A.V. Dermoscopy Use Leads to Earlier Cutaneous Melanoma Diagnosis in Terms of Invasiveness and Size? A Single-Center, Retrospective Experience. J. Clin. Med. 2022, 11, 4912. [Google Scholar] [CrossRef]
- Nolan, G.S.; Dunne, J.A.; Kiely, A.L.; Pritchard Jones, R.O.; Gardiner, M.; Jain, A. The effect of the COVID-19 pandemic on skin cancer surgery in the United Kingdom: A national, multi-centre, prospective cohort study and survey of plastic surgeons. BJS Br. J. Surg. 2020, 107, e598–e600. [Google Scholar] [CrossRef]
- Andrew, T.W.; Alrawi, M.; Lovat, P. Reduction in skin cancer diagnoses in the UK during the COVID-19 pandemic. Clin. Exp. Dermatol. 2020, 46, 145–146. [Google Scholar] [CrossRef]
- Citu, I.M.; Citu, C.; Margan, M.-M.; Craina, M.; Neamtu, R.; Gorun, O.M.; Burlea, B.; Bratosin, F.; Rosca, O.; Grigoras, M.L.; et al. Calcium, Magnesium, and Zinc Supplementation during Pregnancy: The Additive Value of Micronutrients on Maternal Immune Response after SARS-CoV-2 Infection. Nutrients 2022, 14, 1445. [Google Scholar] [CrossRef]
- Marson, J.W.; Maner, B.S.; Harding, T.P.; Meisenheimer, J.; Solomon, J.A.; Leavitt, M.; Levin, N.J.; Dellavalle, R.; Brooks, I.; Rigel, D.S. The magnitude of COVID-19’s effect on the timely management of melanoma and nonmelanoma skin cancers. J. Am. Acad. Dermatol. 2021, 84, 1100–1103. [Google Scholar] [CrossRef] [PubMed]
- Sud, A.; Jones, M.E.; Broggio, J.; Loveday, C.; Torr, B.; Garrett, A.; Nicol, D.L.; Jhanji, S.; Boyce, S.A.; Gronthoud, F.; et al. Collateral damage: The impact on outcomes from cancer surgery of the COVID-19 pandemic. Ann. Oncol. 2020, 31, 1065–1074. [Google Scholar] [CrossRef] [PubMed]
- Nicholson, P.; Ali, F.R.; Mallipeddi, R. Impact of COVID-19 on Mohs micrographic surgery: UK-wide survey and recommendations for practice. Clin. Exp. Dermatol. 2020, 45, 901–902. [Google Scholar] [CrossRef] [PubMed]
- Der Sarkissian, S.A.; Kim, L.; Veness, M.; Yiasemides, E.; Sebaratnam, D.F. Recommendations on dermatologic surgery during the COVID-19 pandemic. J. Am. Acad. Dermatol. 2020, 83, e29–e30. [Google Scholar] [CrossRef] [PubMed]
- National Comprehensive Cancer Network. Short-Term Recommendations for Cutaneous Melanoma Management during COVID-19 Pandemic. Available online: https://www.nccn.org/covid-19/pdf/Melanoma.pdf (accessed on 20 October 2022).
- Wollina, U. Challenges of COVID-19 pandemic for dermatology. Dermatol. Ther. 2020, 33, e13430. [Google Scholar] [CrossRef] [PubMed]
- Bhargava, S.; Negbenebor, N.; Sadoughifar, R.; Ahmad, S.; Kroumpouzos, G. Global impact on dermatology practice due to the COVID-19 pandemic. Clin. Dermatol. 2021, 39, 479–487. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| No. | First Author (Year) | Country | Study Type | No. of Patients | Comparison Date | Quality Assessment |
|---|---|---|---|---|---|---|
| 1 [16] | Filoni (2020) | Italy | Retrospective | NR | 23 February 2020–21 May 2020 | Poor |
| 2 [17] | Cariti (2021) | Italy | Review | 172 | May–June (2017 + 2018 + 2019 vs. 2020) | Moderate |
| 3 [18] | Wong (2020) | England | Retrospective | 2759 | January–June (2019 vs. 2020) | Good |
| 4 [19] | Dika (2021) | Italy | Retrospective | 562 | January–December (2019 vs. 2020) | Poor |
| 5 [20] | Tejera-Vaquerizo (2021) | Spain | Retrospective | 559 | March–June (2019 vs. 2020) | Good |
| 6 [21] | Martinez-Lopez (2022) | Spain | Retrospective | 130 | 15 March 2019–15 March 2020 | Moderate |
| 7 [22] | Gisondi (2021) | Italy | Editorial letter | 1190 | March–October (2019 vs. 2020) | Moderate |
| 8 [23] | Guven (2021) | Turkey | Retrospective | 43 | March–December (2019 vs. 2020) | Poor |
| 9 [24] | Cocuz (2021) | Romania | Retrospective | 50 | April 2019–February 2020 vs. April 2020–February 2021 | Poor |
| 10 [25] | Pala (2020) | Italy | Retrospective | 169 | 1 January 2020–30 April 2020 | Poor |
| 11 [26] | NR (2021) | Italy | Retrospective | 11,324 | February–April (2019 vs. 2020) | Poor |
| 12 [27] | Gualdi (2021) | Italy | Retrospective | 1124 | 1 May–31 July (2017 + 2018 + 2019 vs. 2020) | Moderate |
| 13 [28] | Davis (2022) | USA | Retrospective | 688 | August 2019–March 2020; May 2020-December 2020; January–February 2020 vs. May 2020–June 2020 | Good |
| 14 [29] | Berry (2021) | Australia | Retrospective | NR | 30 March–30 June 2020 vs. 1 February–27 March 2020; 2017+2018+2019 vs. 2020 | Poor |
| 15 [30] | Asai (2021) | Canada | Retrospective | 595 | 6 January–19 April (2019 vs. 2020) | Moderate |
| 16 [31] | Weston (2021) | USA | Retrospective | NR | June–August (2015 + 2016 + 2017 + 2018 +2019 vs. 2020) | Moderate |
| 17 [12] | Hazzaa (2022) | Romania | Retrospective | 301 | January 2018–January 2020 vs. January 2020–January 2022 | Good |
| 18 [32] | Kleeman (2022) | Germany | Retrospective | 61,732 | 18 March 2019–17 March 2020 | Moderate |
| 19 [33] | Chang (2021) | USA | Retrospective | 237 | March–May (2019 vs. 2020) | Moderate |
| 20 [34] | Ricci (2022) | Italy | Review | 531 | 1 January–9 March 2020 vs. 2021 10 March–3 May 2020 vs. 2021 4 May–6 June 2020 vs. 2021 | Moderate |
| 21 [35] | Micek (2022) | Germany | Retrospective | 366 | 1 January 2019–1 March 2021 | Good |
| 22 [11] | Makaranka (2022) | Scotland | Retrospective | 4502 | 2019 vs. 2020 | Moderate |
| 23 [36] | Shannon (2021) | USA | Retrospective | 325 | 15 June–15 August (2019 vs. 2020) | Moderate |
| 24 [37] | Hoellwerth (2021) | Austria | Retrospective | 1365 | February–July (2018 + 2019) vs. 2020 | Moderate |
| 25 [38] | Van Not (2022) | Netherlands | Retrospective | 1318 | (2018 + 2019) vs. 2020 | Good |
| 26 [39] | Lamm (2022) | USA | Retrospective | 111 | May 2019–September 2021 | Moderate |
| 27 [40] | Welzel (2022) | Germany | Editorial letter | 940 | 2019 vs. 2020 vs. 2021 | Moderate |
| 28 [41] | Gedeah (2021) | Spain | Retrospective | 592 | (2018 + 2019) vs. 2020 | Poor |
| 29 [42] | McFeely (2021) | Ireland | Retrospective | 162 | 2019 vs. 2020 | Moderate |
| 30 [43] | Kostner (2022) | Switzerland | Retrospective | 1240 | 1 February 2019–30 April 2021 | Moderate |
| 31 [44] | Mollinier (2022) | France | Editorial letter | 373 | March–October (2019 vs. 2020) | Poor |
| 32 [45] | Valenti (2021) | Italy | Retrospective | 461 | 18 May–18 November (2019 vs. 2010) | Moderate |
| 33 [46] | Trepanowski (2022) | USA | Editorial letter | 3896 | 1 March 2019–29 February 2020 vs. 1 March 2020–28 February 2021 | Poor |
| 34 [47] | Barcaui (2022) | Brazil | Retrospective | 91 | January–March (2018/2019 vs. 2020/2021) | Poor |
| 35 [9] | Seretis (2021) | Greece | Retrospective | 47 | 20 May–20 September (2019 vs. 2021) | Moderate |
| 36 [48] | Balakirski (2022) | Germany | Retrospective | 986 | 2019 vs. 2020 vs. 2021 | Moderate |
| 37 [49] | Shaikh (2022) | USA | Editorial letter | 492 | 11 March 2020–12 January 2021 vs. 1 March 2019–10 March 2020 | Moderate |
| 38 [50] | Villani (2020) | Italy | Editorial letter | 131 | (2018 + 2019) vs. 2020 | Poor |
| 39 [51] | Koch (2021) | Chile | Editorial letter | 296 | January 2019–March 2020 | Poor |
| No. | Male % | Age * | Stage | Breslow Index (mm) |
|---|---|---|---|---|
| 1 [16] | NR | NR | NR | NR |
| 2 [17] | 58.5% vs. 50.0% | 61 vs. 55 | NR | 0.80 vs. 1.56 |
| 3 [18] | NR | NR | NR | NR |
| 4 [19] | NR | NR | NR | NR |
| 5 [20] | 44.3% vs. 57.5% | 64 vs. 63 | >SI (25.6% vs. 34.3%) | >1 mm (34.1% vs. 44.4%) |
| 6 [21] | 55.8% vs. 43.4% | 77 vs. 53 | SII+SIII (22.1% vs. 55.5%) | 1.08 vs. 2.65 |
| 7 [22] | 55.4% vs. 56.5% | 61 vs. 62 | NR | >1 mm (21.0% vs. 23.0%) |
| 8 [23] | 50.5% vs. 54.4% | 60 vs. 61 | >SII (66.6% vs. 80.0%) | NR |
| 9 [24] | NR | NR | NR | NR |
| 10 [25] | 60.0% | 62 | SIII (38.0%), SIV (62.0%) | NR |
| 11 [26] | NR | NR | NR | NR |
| 12 [27] | 50.8% vs. 50.9% | 60 vs. 59 | NR | 0.40 vs. 0.83 |
| 13 [28] | 62.9% vs. 58.1% | 65.7 vs. 67.0 | SII+SIII (7.1% vs. 27.5%) | NR |
| 14 [29] | NR | NR | NR | 2.06 vs. 2.70 |
| 15 [30] | 48.5% vs. 48.9% | 63 vs. 63 | NR | NR |
| 16 [31] | NR | NR | >TII (2.6% vs. 9.0%) Invasive (13.8% vs. 30.0%) | 0.78 vs. 2.04 |
| 17 [12] | 53.4% vs. 50.7% | 58.1 vs. 58.8 | >SII (58.3% vs. 79.7%) | 1.10 vs. 1.80 |
| 18 [32] | 55.6% vs. 54.5% | NR | NR | NR |
| 19 [33] | NR | NR | NR | NR |
| 20 [34] | NR | NR | NR | 0.88 vs. 1.40 |
| 21 [35] | 57.0% vs. 63.2% | 68.6 vs. 72.6 | >SII (28.9% vs. 32.3%) | NR |
| 22 [11] | NR | NR | NR | NR |
| 23 [36] | 55.8% vs. 57.5% | 68 vs. 68 | >SII (14.5% vs. 15.0%) | 0.87 vs. 1.40 |
| 24 [37] | 52.4% vs. 53.9% | 60.5 vs. 63 | NR | 0.62 vs. 0.70 |
| 25 [38] | 58.9% vs. 57.7% | 67 vs. 68 | >SIIIc (9.9% vs. 10.5%) | NR |
| 26 [39] | 62.7% vs. 52.5% | 61.3 vs. 63.0 | SI (60.8% vs. 54.1%) >SII (5.8% vs. 11.5%) | 49.0% vs. 68.8% > 1 mm |
| 27 [40] | NR | NR | SIV (19% vs. 12% vs. 21%) | 1.70 vs. 1.70 |
| 28 [41] | NR | NR | NR | 0.92 vs. 0.87 |
| 29 [42] | 44.0% vs. 46.4% | 68.5 vs. 75.5 | >SII (56.3% vs. 72.6%) | 1.15 vs. 1.90 |
| 30 [43] | NR | NR | NR | 2.60 vs. 2.90 |
| 31 [44] | NR | NR | >SII (10.0% vs. 22.0%) | 1.60 vs. 2.20 |
| 32 [45] | 51.7% vs. 56.9% | 64.3 vs. 65.4 | >SII (1.5% vs. 2.9%) | NR |
| 33 [46] | NR | NR | SII (14.8% vs. 18.3%) | 1.49 vs. 1.77 |
| 34 [47] | NR | 65.0 vs. 72.0 | SII+SII (31.3% vs. 75.0%) | 0.40 vs. 0.80 |
| 35 [9] | 56.0% vs. 44.0% | 66.2 vs. 63.4 | >SII (18.2% vs. 4.0%) | 6.88 vs. 1.31 |
| 36 [48] | NR | 65 vs. 64 | >SII (7.8% vs. 5.4%) | 0.90 vs. 0.90 |
| 37 [49] | 52.8% vs. 55.7% | 65 vs. 65 | >SII (36.1% vs. 49.2%) | 1.40 vs. 2.00 |
| 38 [50] | NR | 56.2 vs. 57.1 | Invasive (49.4% vs. 56.0%) | 4.70 vs. 4.90 |
| 39 [51] | 41.9% vs. 51.4% | 52.7 vs. 53.3 | >SII (24.8% vs. 42.3%) | 1.00 vs. 1.50 |
| No. | Patients before/after COVID-19 | Patient Ratio * | Screening/ Treatment Delay | DFS |
|---|---|---|---|---|
| 1 [16] | NR | −3.0% | DFU (−30.2%) SFU (−37.0%) SLNB (−29.0%) SE (+31.7%) | NR |
| 2 [17] | 47 average vs. 32 (2020) | −32.0% | DFU (−20.0%) | NR |
| 3 [18] | 1294 vs. 1465 | +13.0% | DFU (−31.0%) | NR |
| 4 [19] | 278 vs. 284 | +2.22% | NR | NR |
| 5 [20] | 352 vs. 207 | −58.8% | Excision (−41.0%) | NR |
| 6 [21] | 77 vs. 53 | −18.5% | NR | 94% vs. 89% |
| 7 [22] | 634 vs. 556 | −12.3% | NR | NR |
| 8 [23] | 27 vs. 16 | −40.7% | NR | −7% |
| 9 [24] | 40 (18.2%) vs. 10 (23.2%) | +5.0% melanoma −75.0% cases | NR | NR |
| 10 [25] | NR | NR | TD (−29.0%) | NR |
| 11 [26] | −31.3% | −24.4% | Biopsy (−36.5%) WLE (−22.9%) SLNB (+6.4%) | NR |
| 12 [27] | 295 average vs. 237 (2020) | −20.0% | NR | NR |
| 13 [28] | 375 vs. 313 | −17.0% | Excision (−11.7%) | NR |
| 14 [29] | NR | −48.0% | DFU (−23.0%) | NR |
| 15 [30] | NR | NR | Excision (−27.0%) | NR |
| 16 [31] | 106 (average) vs. 102 | −5.8% | NR | NR |
| 17 [12] | 163 vs. 138 | −15.3% | TD (−10.8%) | 76.7% vs. 65.9% |
| 18 [32] | 31,910 vs. 29822 | −7.0% | Procedures (−17.0%) | NR |
| 19 [33] | NR | NR | DFU (−23.2%) Excision (−28.1%) | NR |
| 20 [34] | 294 vs. 237 | −19.4% | NR | NR |
| 21 [35] | NR | NR | SLNB (−1.7%) DFU (−10.4%) | 87.6% vs. 57.1% |
| 22 [11] | 2468 vs. 2034 | −17.6% | NR | NR |
| 23 [36] | 172 vs. 153 | −11.0% | NR | NR |
| 24 [37] | 466 vs. 432 | −7.3% | NR | NR |
| 25 [38] | 794 vs. 524 | −34.0% | NR | NR |
| 26 [39] | 51 vs. 61 | +19.6% | TD (10 days) | NR |
| 27 [40] | 327 vs. 306 (average) | −6.4% | NR | NR |
| 28 [41] | 193 (average) vs. 196 | +1.6% | NR | NR |
| 29 [42] | 78 vs. 84 | +7.7% | NR | NR |
| 30 [43] | NR | NR | NR | NR |
| 31 [44] | 192 vs. 181 | −15.4% | NR | 94.0% vs. 94.0% |
| 32 [45] | 224 vs. 237 | +5.8% | SFU (+2.3 months) | NR |
| 33 [46] | 2062 vs. 1834 | −11.1% | NR | NR |
| 34 [47] | 20 vs. 16 | −20.0% | NR | NR |
| 35 [9] | 22 vs. 25 | +12.0% | NR | NR |
| 36 [48] | 320 vs. 319 vs. 347 | NR | SLNB (+9.5%) | NR |
| 37 [49] | 246 vs. 246 | NR | TD (34.5 days) | NR |
| 38 [50] | 53 (average) vs. 25 | −52.8% | NR | NR |
| 39 [51] | 191 vs. 105 | −45.0% | NR | NR |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Toma, A.-O.; Prodan, M.; Reddyreddy, A.R.; Seclaman, E.; Crainiceanu, Z.; Bloanca, V.; Bratosin, F.; Dumitru, C.; Pilut, C.N.; Alambaram, S.; et al. The Epidemiology of Malignant Melanoma during the First Two Years of the COVID-19 Pandemic: A Systematic Review. Int. J. Environ. Res. Public Health 2023, 20, 305. https://doi.org/10.3390/ijerph20010305
Toma A-O, Prodan M, Reddyreddy AR, Seclaman E, Crainiceanu Z, Bloanca V, Bratosin F, Dumitru C, Pilut CN, Alambaram S, et al. The Epidemiology of Malignant Melanoma during the First Two Years of the COVID-19 Pandemic: A Systematic Review. International Journal of Environmental Research and Public Health. 2023; 20(1):305. https://doi.org/10.3390/ijerph20010305
Chicago/Turabian StyleToma, Ana-Olivia, Mihaela Prodan, Akash Reddy Reddyreddy, Edward Seclaman, Zorin Crainiceanu, Vlad Bloanca, Felix Bratosin, Catalin Dumitru, Ciprian Nicolae Pilut, Satish Alambaram, and et al. 2023. "The Epidemiology of Malignant Melanoma during the First Two Years of the COVID-19 Pandemic: A Systematic Review" International Journal of Environmental Research and Public Health 20, no. 1: 305. https://doi.org/10.3390/ijerph20010305
APA StyleToma, A.-O., Prodan, M., Reddyreddy, A. R., Seclaman, E., Crainiceanu, Z., Bloanca, V., Bratosin, F., Dumitru, C., Pilut, C. N., Alambaram, S., Vasamsetti, N. G., Decean, L., & Pricop, M. (2023). The Epidemiology of Malignant Melanoma during the First Two Years of the COVID-19 Pandemic: A Systematic Review. International Journal of Environmental Research and Public Health, 20(1), 305. https://doi.org/10.3390/ijerph20010305