
Patient Safety and the COVID-19 Pandemic in Germany: A Repeated Population-Based Cross-Sectional Survey

 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Questionnaire and Implementation
2.4. Data Analysis
3. Results
3.1. Participants
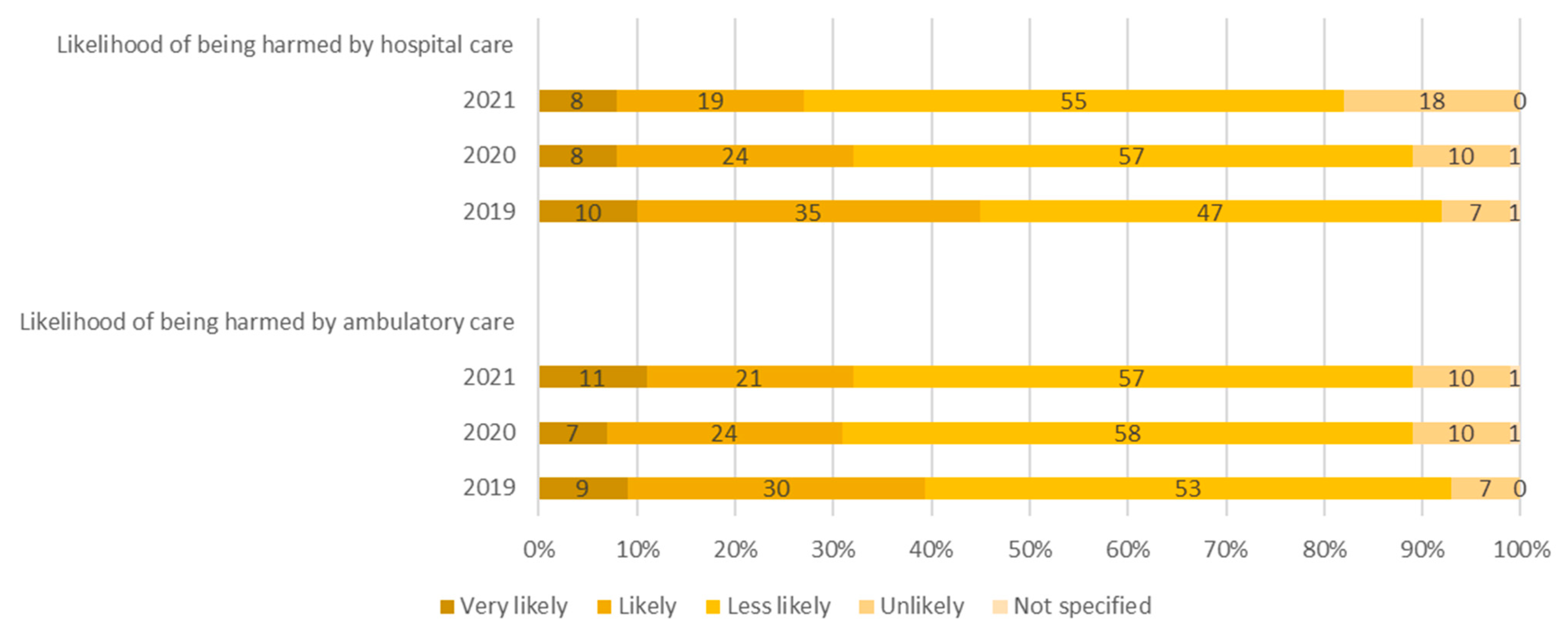
3.2. Patient Safety Perceptions from 2019 to 2021
3.3. Experiences with Patient Safety from 2019 to 2021
3.4. Healthcare during COVID-19 Pandemic (Results from 2020)
3.5. Knowledge about Long COVID (Results from 2021)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Implications of the COVID-19 Pandemic for Patient Safety: A Rapid Review; World Health Organization: Geneva, Switzerland, 2022; Available online: https://www.who.int/publications/i/item/9789240055094 (accessed on 2 November 2022).
- World Health Organization. Conceptual Framework for the International Classification for Patient Safety. Available online: https://apps.who.int/iris/bitstream/handle/10665/70882/WHO_IER_PSP_2010.2_eng.pdf;jsessionid=1E35A42092E063E55BF56FC5823CE842?sequence=1 (accessed on 9 December 2020).
- World Health Organization. 10 Facts on Patient Safety: World Health Organization. Available online: www.who.int/features/factfiles/patient_safety/en/ (accessed on 26 March 2022).
- Rangachari, P.; Woods, J.L. Preserving Organizational Resilience, Patient Safety, and Staff Retention during COVID-19 Requires a Holistic Consideration of the Psychological Safety of Healthcare Workers. Int. J. Environ. Res. Public Health 2020, 17, 4267. [Google Scholar] [CrossRef] [PubMed]
- Armitage, R.; Nellums, L.B. Whistleblowing and patient safety during COVID-19. EClinicalMedicine 2020, 24, 100425. [Google Scholar] [CrossRef]
- Hölscher, U.M.; Gausmann, P.; Haindl, H.; Heidecke, C.-D.; Hübner, N.-O.; Lauer, W.; Lauterberg, J.; Skorning, M.; Thürmann, P.A. Übersichtsartikel: Patientensicherheit als nationales Gesundheitsziel: Status und notwendige Handlungsfelder für die Gesundheitsversorgung in Deutschland. Z. Evid. Fortbild. Qual. Gesundhwes. 2014, 108, 6–14. [Google Scholar] [CrossRef] [PubMed]
- Fiol-deRoque, M.A.; Serrano-Ripol, M.J.; Gens-Barberà, M.; Sánchez, E.; Mayer, M.A.; Martín-Luján, F.; Valderas, J.M.; Ricci-Cabello, I. Impacto de la pandemia de COVID-19 en la seguridad del paciente percibida por los pacientes en Atención Primaria. Aten. Primaria 2021, 53 (Suppl. S1). [Google Scholar] [CrossRef] [PubMed]
- Lotan, I.; Romanow, G.; Levy, M. Patient-reported safety and tolerability of the COVID-19 vaccines in persons with rare neuroimmunological diseases. Mult. Scler. Relat. Disord. 2021, 55, 103189. [Google Scholar] [CrossRef] [PubMed]
- Anhang Price, R.; Elliott, M.N.; Zaslavsky, A.M.; Hays, R.D.; Lehrman, W.G.; Rybowski, L.; Edgman-Levitan, S.; Cleary, P.D. Examining the role of patient experience surveys in measuring health care quality. Med. Care Res. Rev. 2014, 71, 522–554. [Google Scholar] [CrossRef]
- Doyle, C.; Lennox, L.; Bell, D. A systematic review of evidence on the links between patient experience and clinical safety and effectiveness. BMJ Open 2013, 3, e001570. [Google Scholar] [CrossRef]
- Davis, R.E.; Sevdalis, N.; Jacklin, R.; Vincent, C.A. An examination of opportunities for the active patient in improving patient safety. J. Patient Saf. 2012, 8, 36–43. [Google Scholar] [CrossRef]
- Ward, J.K.; Armitage, G. Can patients report patient safety incidents in a hospital setting? A systematic review. BMJ Qual. Saf. 2012, 21, 685–699. [Google Scholar] [CrossRef]
- Rea, D.; Griffiths, S. Patient safety in primary care: Incident reporting and significant event reviews in British general practice. Health Soc. Care Community 2016, 24, 411–419. [Google Scholar] [CrossRef]
- Kraska, R.A.; Weigand, M.; Geraedts, M. Associations between hospital characteristics and patient satisfaction in Germany. Health Expect. 2017, 20, 593–600. [Google Scholar] [CrossRef] [PubMed]
- Müller, H.; Müller, B.; Schwappach, D. TK-Monitor Patientensicherheit: Erlebte Patientensicherheit aus Sicht der Bevölkerung. Eine bevölkerungsrepräsentative Befragung zum Stand der Sicherheit in der medizinischen Versorgung, Hamburg. 2020. Available online: https://www.tk.de/resource/blob/2091462/d2497d0f412892ec1232a2b143e77227/tk-monitor-patientensicherheit---report-data.pdf (accessed on 14 April 2021).
- Müller, A.; Sawicki, O.A.; Müller, H.; Schwappach, D.; Wendt, P.; Ploeger, C.; Brückle, M.-S.; Müller, B.S. Subjektive Informiertheit von Patient* innen zum Thema Patientensicherheit: Ergebnisse einer Bevölkerungsbefragung in Deutschland. Z. Evidenz Fortbild. Qual. Gesundh. 2021, 165, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Arbeitsgemeinschaft ADM-Stichproben—ADM e.V. ADM-Forschungsprojekt, Dual-Frame-Ansätze 2011/2012. 2022. Available online: https://www.adm-ev.de/wp-content/uploads/2021/02/Forschungsbericht-Dual-Frame-Ansaetze.pdf (accessed on 3 November 2022).
- Statista. Festnetztelefon—Ausstattungsgrad privater Haushalte Deutschland 2021|Statista. Available online: https://de.statista.com/statistik/daten/studie/2597/umfrage/ausstattungsgrad-privater-haushalte-mit-einem-stationaeren-telefon-seit-1998/ (accessed on 3 November 2022).
- Forsa. Gesellschaft für Sozialforschung und Statistische Analysen mbH. Available online: https://www.forsa.de/1/ (accessed on 5 May 2022).
- ICC/ESOMAR. Internationaler Kodex zur Markt-, Meinungs- und Sozialforschung sowie zur Datenanalytik. Available online: https://www.esomar.org/what-we-do/code-guidelines (accessed on 10 January 2021).
- Universität Erfurt. COSMO—COVID-19 Snapshot Monitoring. Available online: https://projekte.uni-erfurt.de/cosmo2020/web/ (accessed on 12 December 2021).
- Lippke, S. TeamBaby—Sichere, digital unterstützte Kommunikation in der Frauenheilkunde und Geburtshilfe—G-BA Innovationsfonds. Available online: https://innovationsfonds.g-ba.de/projekte/versorgungsforschung/teambaby-sichere-digital-unterstuetzte-kommunikation-in-der-frauenheilkunde-und-geburtshilfe.220 (accessed on 12 December 2021).
- Schwappach, D.L.B. Risk factors for patient-reported medical errors in eleven countries. Health Expect. 2014, 17, 321–331. [Google Scholar] [CrossRef] [PubMed]
- Schwappach, D.L. Frequency of and predictors for patient-reported medical and medication errors in Switzerland. Swiss Med. Wkly. 2011, 141, w13262. [Google Scholar] [CrossRef]
- Schwappach, D.L.B.; Frank, O.; Buschmann, U.; Babst, R. Effects of an educational patient safety campaign on patients’ safety behaviours and adverse events. J. Eval. Clin. Pract. 2013, 19, 285–291. [Google Scholar] [CrossRef]
- Commonwealth Fund. 2016 Commonwealth Fund International Health Policy Survey of Adults. Available online: https://www.commonwealthfund.org/publications/surveys/2016/nov/2016-commonwealth-fund-international-health-policy-survey-adults (accessed on 30 November 2020).
- European Commission. PublicOpinion—European Commission. Available online: https://ec.europa.eu/commfrontoffice/publicopinion/index.cfm/Survey/getSurveyDetail/instruments/SPECIAL/yearFrom/2010/yearTo/2011/search/Patient%20Safety/surveyKy/796 (accessed on 30 November 2020).
- Eurobarometer Spezial 241. Medizinische Fehler. 2006. Available online: https://ec.europa.eu/health/ph_information/documents/eb_64_de.pdf (accessed on 30 November 2020).
- Müller, B.S.; Uhl, M.C.; Sophia, N.T.; Schoch, G.G.; Gerlach, F.M.; Muth, C. Patienten MIT Multimedikation: Ambulante Herausforderungen und Lösungswege: Eine qualitative studie. Z. Allg. Med. 2018, 94, 396–400. [Google Scholar]
- McHugh, M.L. The chi-square test of independence. Biochem. Med. 2013, 23, 143–149. [Google Scholar] [CrossRef]
- R Core Team. R: The R Project for Statistical Computing. Available online: https://www.r-project.org/ (accessed on 5 May 2022).
- Geraedts, M.; Krause, S.; Schneider, M.; Ortwein, A.; Leinert, J.; de Cruppé, W. Patient safety in ambulatory care from the patient’s perspective: A retrospective, representative telephone survey. BMJ Open 2020, 10, e034617. [Google Scholar] [CrossRef]
- OECD. Health at a Glance 2019. Available online: https://www.oecd.org/berlin/publikationen/health-at-a-glance-2019.htm (accessed on 2 November 2022).
- Leape, L.L.; Woods, D.D.; Hatlie, M.J.; Kizer, K.W.; Schroeder, S.A.; Lundberg, G.D. Promoting patient safety by preventing medical error. J. Am. Med. Assoc. 1998, 281, 1444–1447. [Google Scholar] [CrossRef]
- Hibbard, J.H.; Peters, E.; Slovic, P.; Tusler, M. Can patients be part of the solution? Views on their role in preventing medical errors. Med. Care Res. Rev. 2005, 62, 601–616. [Google Scholar] [CrossRef]
- Nabhan, M.; Elraiyah, T.; Brown, D.R.; Dilling, J.; LeBlanc, A.; Montori, V.M.; Morgenthaler, T.; Naessens, J.; Prokop, L.; Roger, V.; et al. What is preventable harm in healthcare? A systematic review of definitions. BMC Health Serv. Res. 2012, 12, 128. [Google Scholar] [CrossRef] [PubMed]
- Uimonen, M.; Kuitunen, I.; Paloneva, J.; Launonen, A.P.; Ponkilainen, V.; Mattila, V.M. The impact of the COVID-19 pandemic on waiting times for elective surgery patients: A multicenter study. PLoS ONE 2021, 16, e0253875. [Google Scholar] [CrossRef] [PubMed]
- Moynihan, R.; Sanders, S.; Michaleff, Z.A.; Scott, A.M.; Clark, J.; To, E.J.; Jones, M.; Kitchener, E.; Fox, M.; Johansson, M.; et al. Impact of COVID-19 pandemic on utilisation of healthcare services: A systematic review. BMJ Open 2021, 11, e045343. [Google Scholar] [CrossRef] [PubMed]
- Du, Q.; Zhang, D.; Hu, W.; Li, X.; Xia, Q.; Wen, T.; Jia, H. Nosocomial infection of COVID-19: A new challenge for healthcare professionals (Review). Int. J. Mol. Med. 2021, 47, 31. [Google Scholar] [CrossRef] [PubMed]
- Noble, D.J.; Pronovost, P.J. Underreporting of patient safety incidents reduces health care’s ability to quantify and accurately measure harm reduction. J. Patient Saf. 2010, 6, 247–250. [Google Scholar] [CrossRef] [PubMed]
- Güldner, S.; Mang, H.; Popp, S.; Heuser, D.; Krause, M.; Christ, M. Gedanken zur Fehler- und Sicherheitskultur in deutschen Notaufnahmen. Notfall Rettungsmed. 2011, 14, 351–360. [Google Scholar] [CrossRef]
- Robert Koch Institute. Coronavirus Disease 2019 (COVID-19) Daily Situation Report of the Robert Koch Institute: 2020-08-31-en, Berlin. Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Situationsberichte/2020-08-31-en.pdf?__blob=publicationFile (accessed on 11 February 2022).
- Gasparri, M.L.; Gentilini, O.D.; Lueftner, D.; Kuehn, T.; Kaidar-Person, O.; Poortmans, P. Changes in breast cancer management during the Corona Virus Disease 19 pandemic: An international survey of the European Breast Cancer Research Association of Surgical Trialists (EUBREAST). Breast 2020, 52, 110–115. [Google Scholar] [CrossRef]
- Lazzerini, M.; Barbi, E.; Apicella, A.; Marchetti, F.; Cardinale, F.; Trobia, G. Delayed access or provision of care in Italy resulting from fear of COVID-19. Lancet Child Adolesc. Health 2020, 4, e10–e11. [Google Scholar] [CrossRef]
- Chan, H.F.; Brumpton, M.; Macintyre, A.; Arapoc, J.; Savage, D.A.; Skali, A.; Stadelmann, D.; Torgler, B. How confidence in health care systems affects mobility and compliance during the COVID-19 pandemic. PLoS ONE 2020, 15, e0240644. [Google Scholar] [CrossRef]
- Rawaf, S.; Allen, L.N.; Stigler, F.L.; Kringos, D.; Yamamoto, H.Q.; van Weel, C.; on behalf of the Global Forum on Universal Health Coverage; Primary Health Care. Lessons on the COVID-19 pandemic, for and by primary care professionals worldwide. Eur. J. Gen. Pract. 2020, 26, 129–133. [Google Scholar] [CrossRef]
- Saadatjoo, S.; Miri, M.; Hassanipour, S.; Ameri, H.; Arab-Zozani, M. Knowledge, attitudes, and practices of the general population about Coronavirus disease 2019 (COVID-19): A systematic review and meta-analysis with policy recommendations. Public Health 2021, 194, 185–195. [Google Scholar] [CrossRef] [PubMed]
- Gottlieb, M.; Dyer, S. Information and Disinformation: Social Media in the COVID-19 Crisis. Acad. Emerg. Med. 2020, 27, 640–641. [Google Scholar] [CrossRef] [PubMed]
- Schulz, P.J.; Pessina, A.; Hartung, U.; Petrocchi, S. Effects of Objective and Subjective Health Literacy on Patients’ Accurate Judgment of Health Information and Decision-Making Ability: Survey Study. J. Med. Internet Res. 2021, 23, e20457. [Google Scholar] [CrossRef] [PubMed]
- Stacey, A.F.; Gill, T.K.; Price, K.; Taylor, A.W. Differences in risk factors and chronic conditions between informal (family) carers and non-carers using a population-based cross-sectional survey in South Australia. BMJ Open 2018, 8, e020173. [Google Scholar] [CrossRef] [PubMed]
- Cobben, F.; Bethlehem, J. Adjusting Undercoverage and Nonresponse Bias in Telephone Surveys; Statistics Netherlands: Voorburg/Heerlen, The Netherlands, 2005. [Google Scholar]


{kind=link}
| Demographic | Characteristics | 2019 n (%) | 2020 n (%) | 2021 n (%) |
|---|---|---|---|---|
| Gender | Male | 489 (49) | 490 (49) | 489 (49) |
| Female | 511 (51) | 510 (51) | 511 (51) | |
| Age group | 18–39 years | 319 (32) | 317 (32) | 316 (32) |
| 40–59 years | 348 (35) | 321 (32) | 324 (32) | |
| ≥60 years | 333 (33) | 362 (36) | 360 (36) | |
| Employment status | Employed | 524 (52) | 551 (55) | 537 (54) |
| Unemployed | 476 (48) | 449 (45) | 463 (46) | |
| Chronic condition | Yes | 366 (37) | 311 (31) | 287 (29) |
| No | 634 (63) | 689 (69) | 713 (71) | |
| Self-rated health status | Very good/good | 572 (57) | 679 (68) | 677 (68) |
| Satisfactory | 295 (30) | 255 (26) | 254 (25) | |
| Less good/bad | 133 (13) | 66 (7) | 69 (7) | |
| Number of prescription medications | No | 458 (46) | 508 (51) | 533 (53) |
| One drug | 177 (18) | 211 (21) | 175 (18) | |
| Two drugs | 133 (13) | 117 (12) | 111 (11) | |
| Three or more drugs | 231 (23) | 164 (16) | 181 (18) | |
| Education level | Primary school | 338 (34) | 83 (8) | 65 (7) |
| Secondary school | 280 (28) | 258 (26) | 255 (23) | |
| Tertiary/University | 355 (36) | 637 (64) | 663 (66) | |
| Insurance status | Statutory health insurance | 875 (88) | 786 (79) | 807 (81) |
| Private health insurance | 125 (13) | 214 (21) | 193 (19) |
| Likelihood of Adverse Events | Likelihood of Prevention of Adverse Events | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| 2019 | 2020 | 2021 | p Value | 2019 | 2020 | 2021 | p Value | ||
| Hospital-acquired infection | <0.0001 | <0.0001 | |||||||
| Yes, definitely (%) | 16 | 12 | 15 | 21 | 13 | 13 | |||
| Yes, probably (%) | 47 | 44 | 47 | 43 | 47 | 54 | |||
| Probably not (%) | 31 | 35 | 33 | 29 | 33 | 27 | |||
| Certainly not (%) | 6 | 8 | 4 | 7 | 6 | 6 | |||
| Not specified (%) | 1 | 1 | 2 | 0 | 0 | 0 | |||
| Wrong diagnosis | 0.001 | 0.8912 | |||||||
| Yes, definitely (%) | 14 | 14 | 13 | 17 | 15 | 16 | |||
| Yes, probably (%) | 45 | 36 | 40 | 42 | 44 | 45 | |||
| Probably not (%) | 36 | 42 | 42 | 34 | 34 | 33 | |||
| Certainly not (%) | 5 | 6 | 5 | 6 | 6 | 6 | |||
| Not specified (%) | 0 | 1 | 0 | 1 | 1 | 1 | |||
| Error during operation | <0.0001 | 0.0823 | |||||||
| Yes, definitely (%) | 6 | 7 | 8 | 16 | 14 | 15 | |||
| Yes, probably (%) | 36 | 24 | 27 | 39 | 45 | 43 | |||
| Probably not (%) | 51 | 55 | 55 | 36 | 31 | 33 | |||
| Certainly not (%) | 7 | 13 | 9 | 7 | 8 | 8 | |||
| Not specified (%) | 0 | 1 | 1 | 1 | 1 | 1 | |||
| Medication error | <0.0001 | 0.0018 | |||||||
| Yes, definitely (%) | 8 | 8 | 12 | 20 | 19 | 19 | |||
| Yes, probably (%) | 40 | 30 | 32 | 42 | 37 | 45 | |||
| Probably not (%) | 43 | 48 | 45 | 32 | 36 | 29 | |||
| Certainly not (%) | 9 | 13 | 11 | 5 | 8 | 6 | |||
| Not specified (%) | 0 | 0 | 0 | 1 | 1 | 1 | |||
| Medical device adverse event | <0.0001 | 0.1298 | |||||||
| Yes, definitely (%) | 5 | 3 | 3 | 18 | 20 | 18 | |||
| Yes, probably (%) | 26 | 20 | 21 | 41 | 40 | 47 | |||
| Probably not (%) | 58 | 62 | 62 | 31 | 30 | 28 | |||
| Certainly not (%) | 12 | 14 | 12 | 7 | 8 | 6 | |||
| Not specified (%) | 0 | 1 | 2 | 2 | 2 | 2 | |||
| 2019 | 2020 | 2021 | p Value | |
|---|---|---|---|---|
| Self-efficacy in error prevention | <0.0001 | |||
| Yes, definitely (%) | 26 | 34 | 34 | |
| Yes, probably (%) | 43 | 41 | 40 | |
| Probably not (%) | 23 | 20 | 18 | |
| Not at all (%) | 6 | 5 | 8 | |
| Not specified (%) | 2 | 0 | 0 | |
| Patient safety knowledge | <0.0001 | |||
| Good (%) | 9 | 11 | 18 | |
| Moderate (%) | 46 | 57 | 51 | |
| Poor (%) | 34 | 24 | 23 | |
| None at all (%) | 11 | 8 | 8 | |
| Not specified (%) | 0 | 0 | 1 |
| 2019 | 2020 | 2021 | p Value | ||
|---|---|---|---|---|---|
| Suspected errors | 0.2238 | ||||
| All respondents | 1000 | 1000 | 1000 | ||
| Yes, once (%) | 17 | 18 | 18 | ||
| Yes, several times (%) | 7 | 6 | 9 | ||
| No (%) | 75 | 76 | 73 | ||
| Not specified (%) | 0 | 0 | 0 | ||
| Reported errors | 0.1648 | ||||
| Respondents reporting an error | 242 | 237 | 266 | ||
| Yes (%) | 34 | 30 | 40 | ||
| No (%) | 64 | 67 | 57 | ||
| Not specified (%) | 2 | 2 | 3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amberger, O.; Müller, A.; Lemke, D.; Müller, H.; Schwappach, D.; Wendt, P.; Wensing, M.; Brueckle, M.-S.; Müller, B.S. Patient Safety and the COVID-19 Pandemic in Germany: A Repeated Population-Based Cross-Sectional Survey. Int. J. Environ. Res. Public Health 2023, 20, 112. https://doi.org/10.3390/ijerph20010112
Amberger O, Müller A, Lemke D, Müller H, Schwappach D, Wendt P, Wensing M, Brueckle M-S, Müller BS. Patient Safety and the COVID-19 Pandemic in Germany: A Repeated Population-Based Cross-Sectional Survey. International Journal of Environmental Research and Public Health. 2023; 20(1):112. https://doi.org/10.3390/ijerph20010112
Chicago/Turabian StyleAmberger, Olga, Angelina Müller, Dorothea Lemke, Hardy Müller, David Schwappach, Peter Wendt, Michel Wensing, Maria-Sophie Brueckle, and Beate S. Müller. 2023. "Patient Safety and the COVID-19 Pandemic in Germany: A Repeated Population-Based Cross-Sectional Survey" International Journal of Environmental Research and Public Health 20, no. 1: 112. https://doi.org/10.3390/ijerph20010112
APA StyleAmberger, O., Müller, A., Lemke, D., Müller, H., Schwappach, D., Wendt, P., Wensing, M., Brueckle, M.-S., & Müller, B. S. (2023). Patient Safety and the COVID-19 Pandemic in Germany: A Repeated Population-Based Cross-Sectional Survey. International Journal of Environmental Research and Public Health, 20(1), 112. https://doi.org/10.3390/ijerph20010112