
Oxygen Uptake Measurements and Rate of Perceived Exertion during a Marathon

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. The Marathon Race
2.3. Experimental Measurements
2.4. The Rate of Perception of Exertion
2.5. Statistical Analysis
2.5.1. Global Tendency of Pace and Its Asymmetry
2.5.2. Tested “Ascending” and “Descending” Series
2.5.3. Multivariate Data Analysis
2.5.4. Principal Component Analysis
3. Results
3.1. Trend and Asymmetry Characteristics of Speed and Cardiorespiratory Variables in the Marathon Race
- -
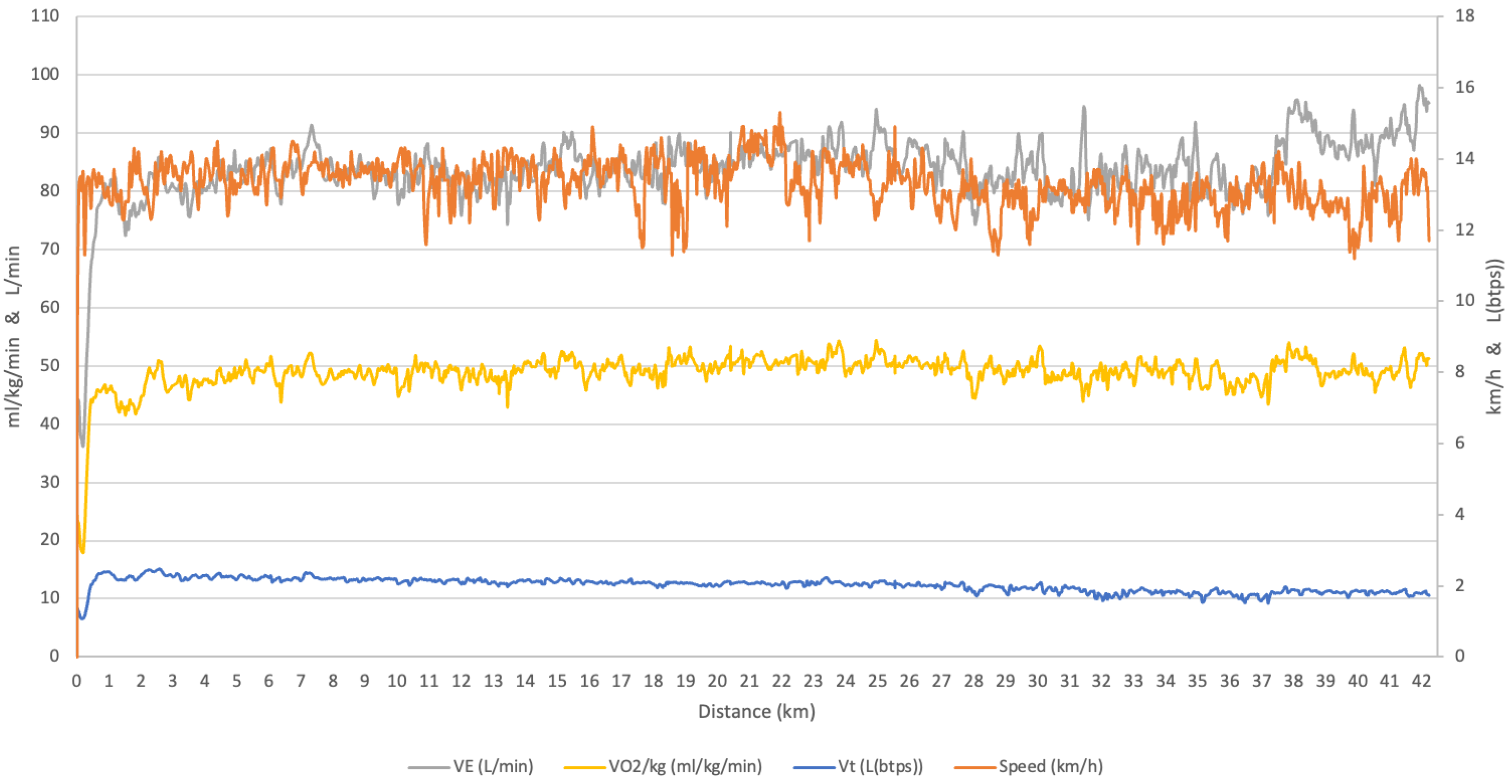
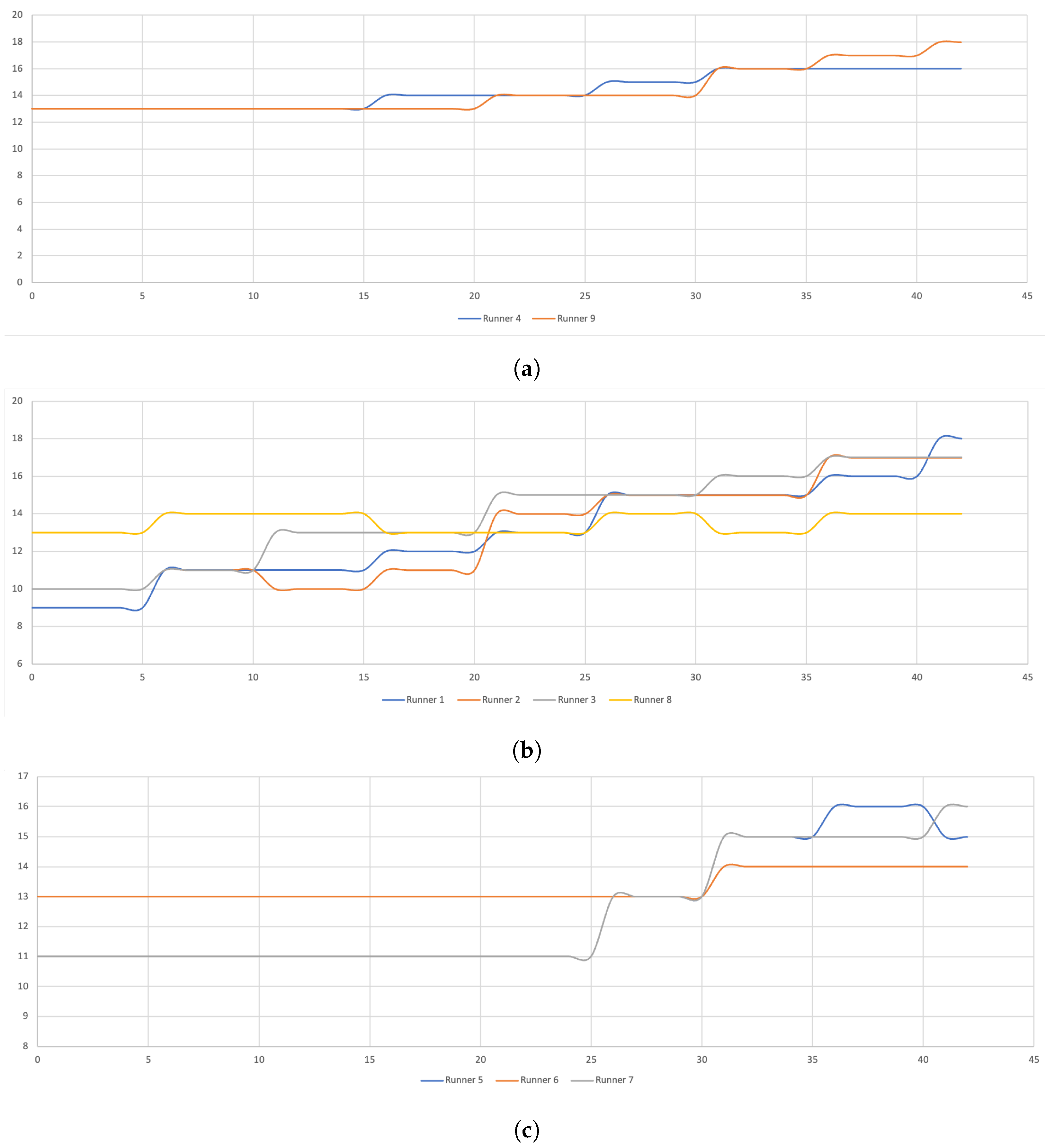
- Speed:All but one (runner 2), marathon runners ran a large positive split race as indicated by a negative Kendall’s (Table 2). The speed highly decreased throughout the race considering this global tendency. Furthermore, they had a positive skewness and a negative asymmetry (Table 2). A negative coefficient indicates a distribution shifted to the right of the median and thus a distribution tail spread to the left. More specifically, the speed factors: cadence and amplitude, also followed the same significantly negative trend (Table 2). All these runners (but the runner 2) ran more of the average distance above average speed (56 ± 3%).
- -
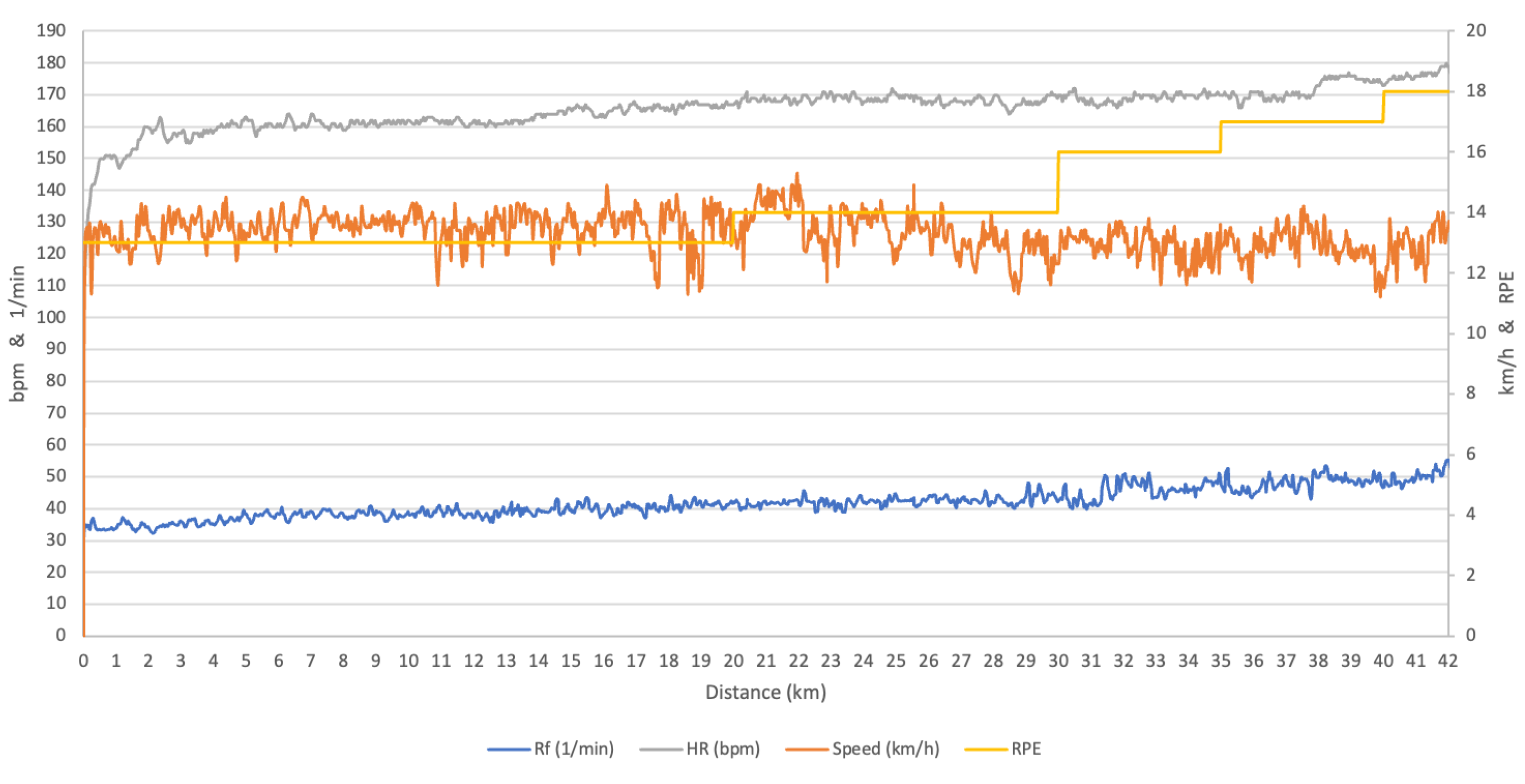
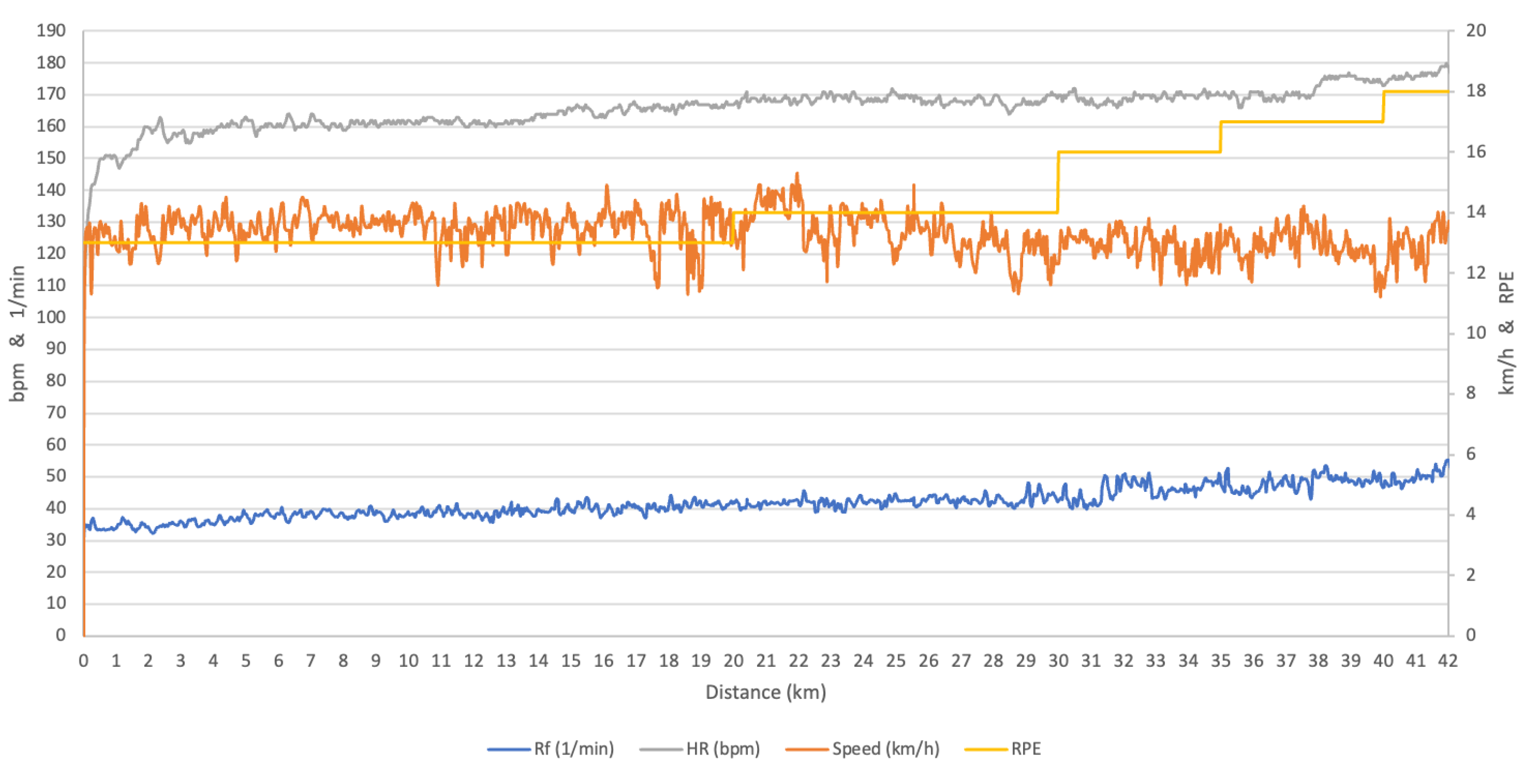
- Cardiorespiratory time series tendencies:There were different tendencies between the cardiorespiratory parameters as well as in the runners. In all runners (except runner 6), the respiratory rate showed a highly significant positive trend, while the tidal volume decreased. The minute ventilation increased (3/9) or decreased (6/9) depending on the balance between the respiratory rate increase and tidal volume decrease.Similarly, O2 decreased in two thirds of the marathoners (6/9) but CO2 and RER decreased in almost all (8/9) of the runners. The physiological variables indexed by the speed gave a clearer picture than the physiological variables alone, due to the decrease in speed. For example, Rf/speed decreased in every runners (9/9), including one who had a decrease in Rf (R4). However, expressing the variables as a function of the speed did not change the patterns observed for the other variables (HR, O2, CO2, Vt and VE) (Table 3). When we expressed the variables as a function of the RPE, we saw that all the variables showed a negative trend in all the runners (Table 4). Now, after having identified this global tendency, we attempt to identify some point distance where the variables change more abruptly.
3.2. Tested “Ascending” and “Descending” Series
3.3. Comparison of Each 5-km Splits (t-Student Test for Paired Data)
- -
- Cardiorespiratory responses: heart rate increased at the fifth km and then, stabilised until the 15th km where it increased again and then stabilise again until the end the marathon. O2 remained stable in contrast with CO2, which decreased at the tenth and the 30th km resulting in a decreases in the respiratory exchange ratio (RER).
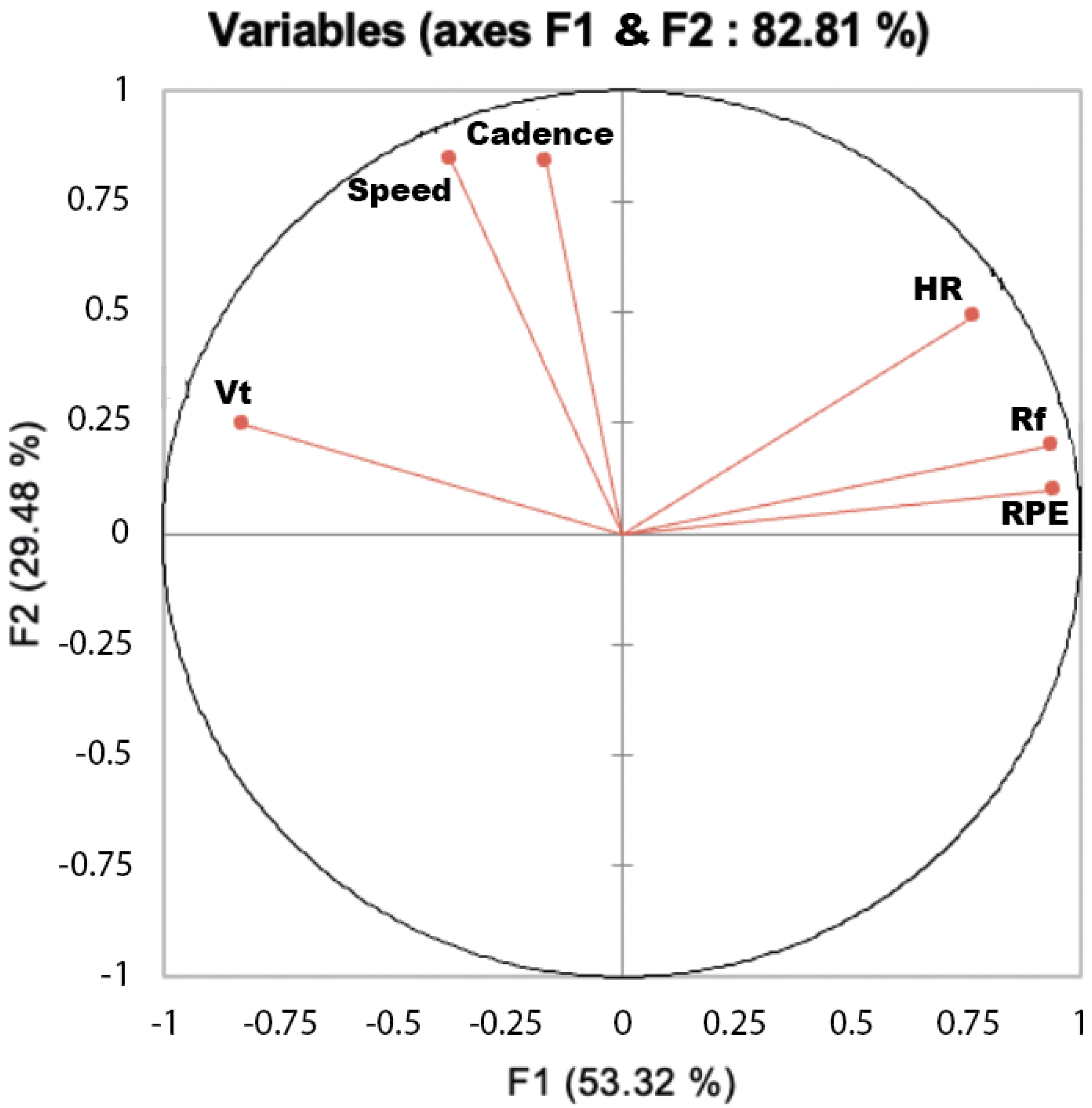
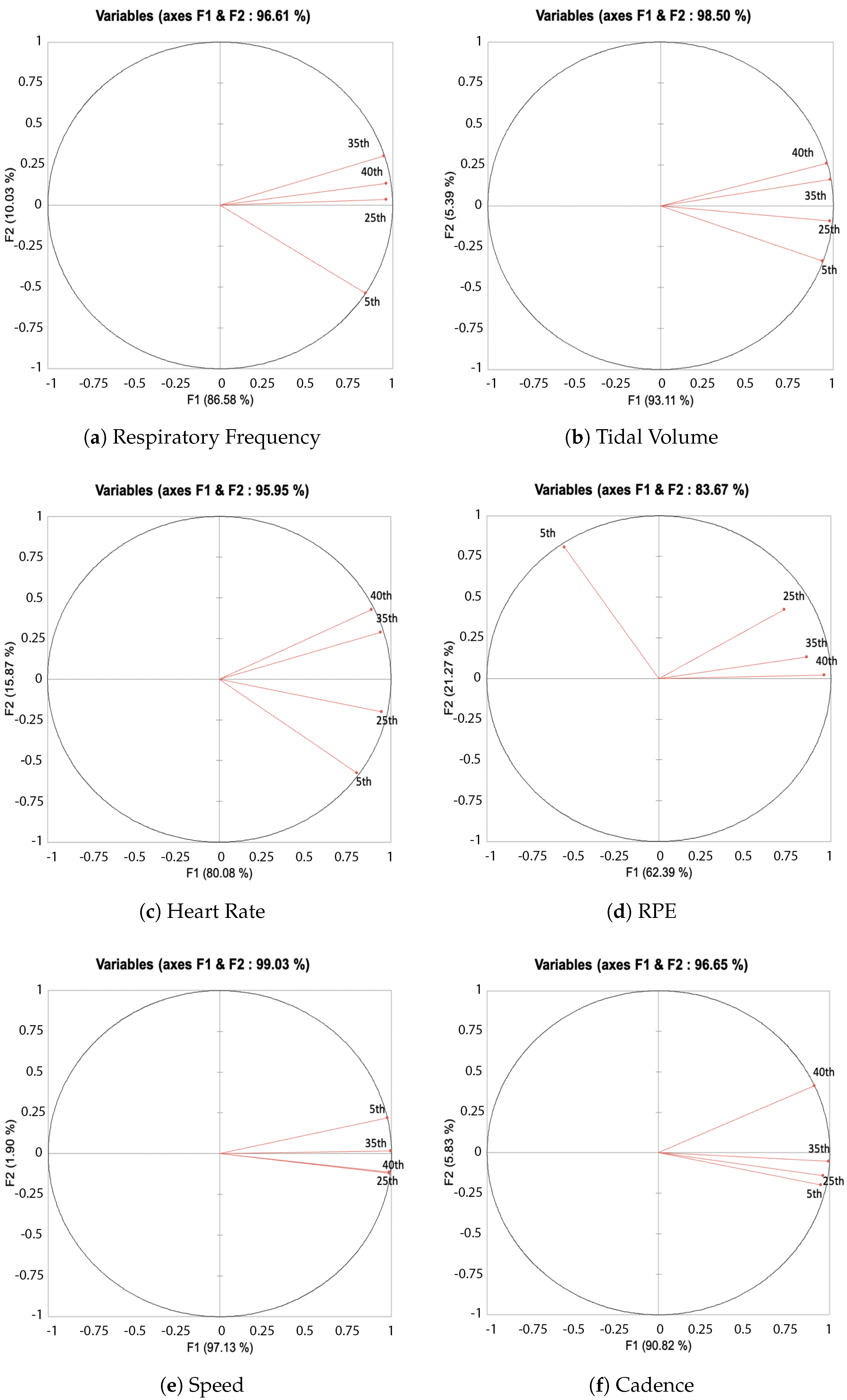
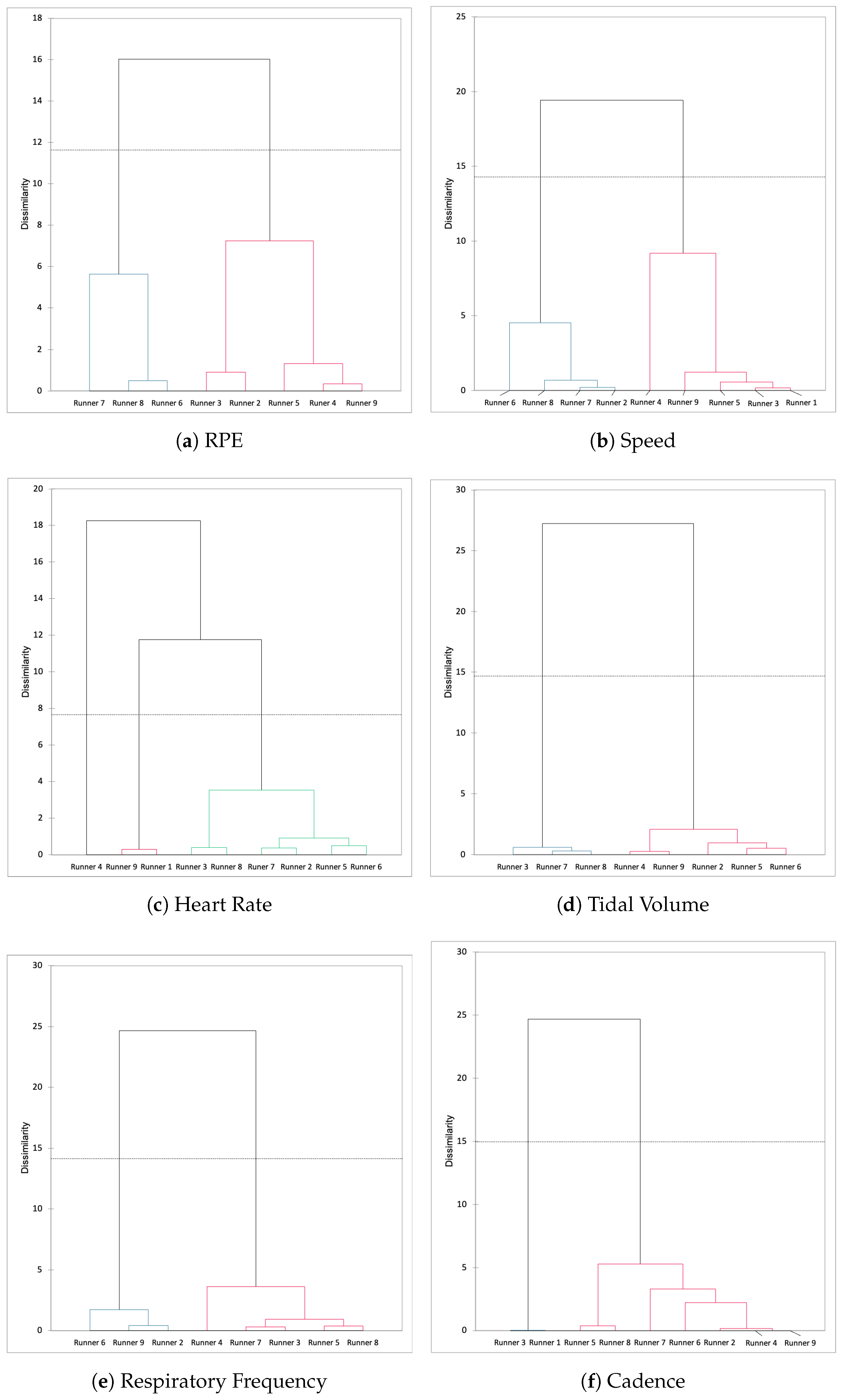
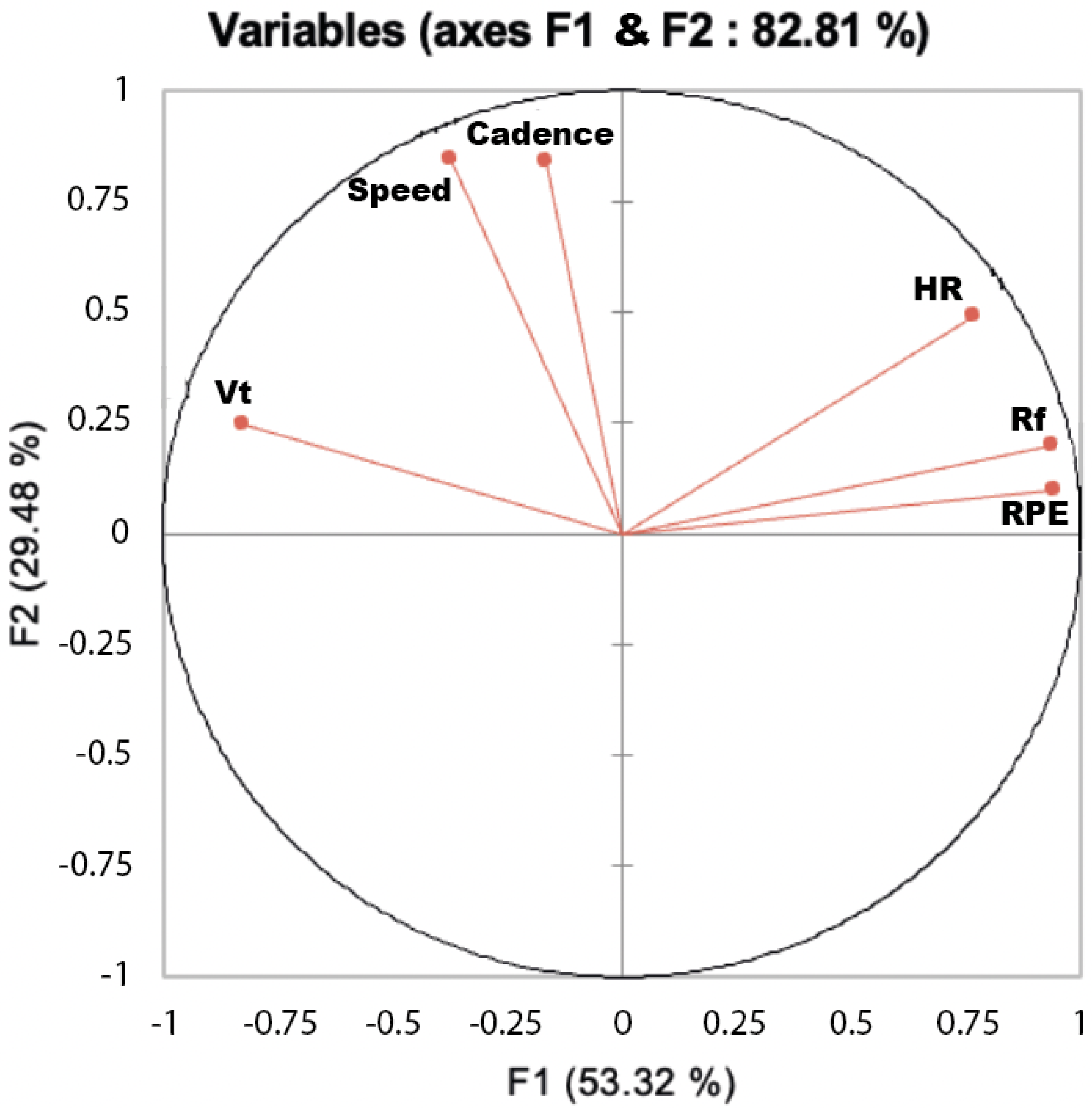
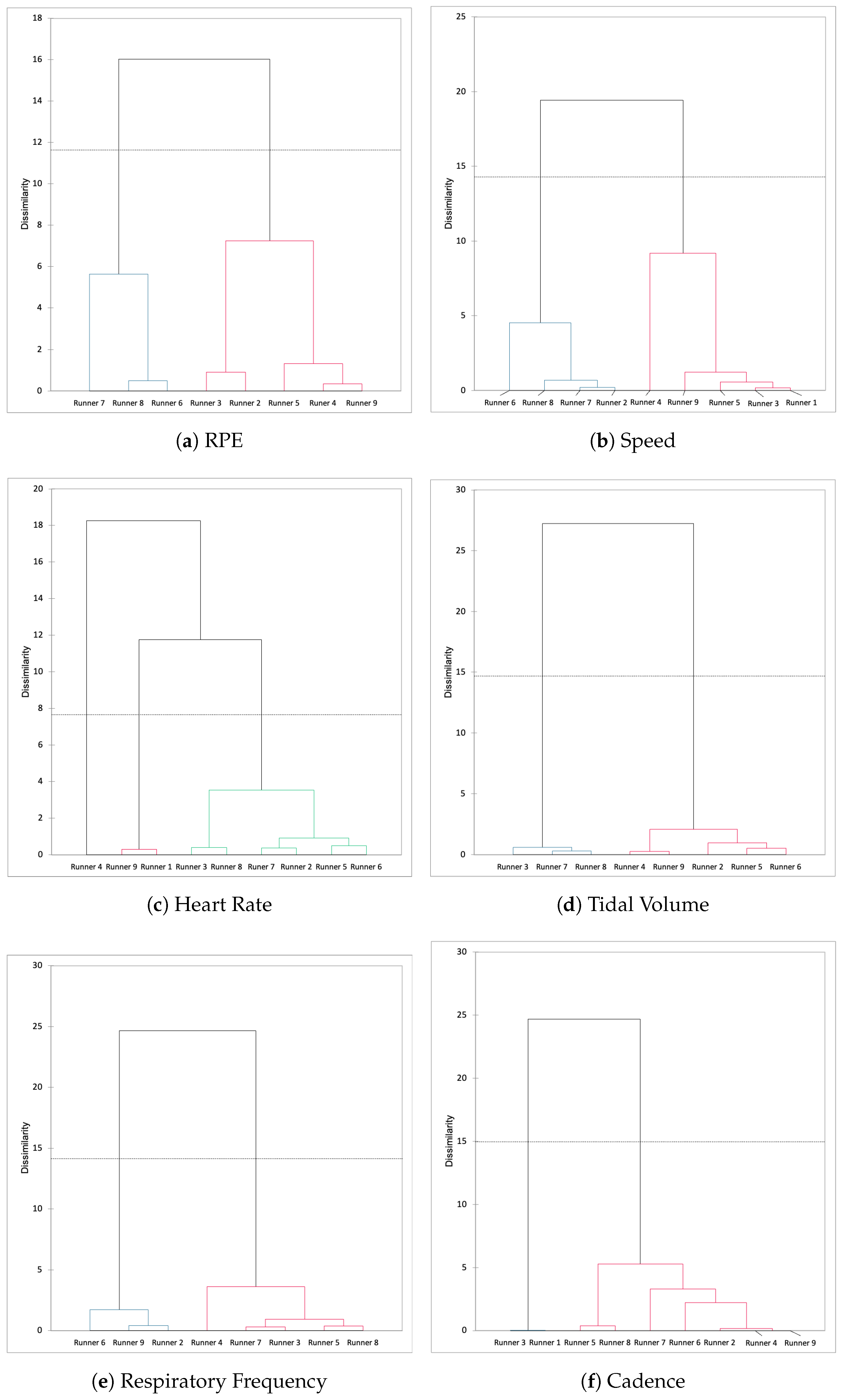
3.4. Multivariate Analysis for Cardiorespiratory and Speed Variables
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
References
- Run Repeat. Available online: https://runrepeat.com/state-of-running (accessed on 9 March 2022).
- Latta, S. Hitting the wall: If you understand the scientific reasons behind “the wall”, you should be able to avoid it. Marathon Beyond 2003, 7, 61–72. [Google Scholar]
- Berndsen, J.; Lawlor, A.; Smyth, B. Exploring the Wall in Marathon Running. J. Sport. Anal. 2020, 6, 173–186. [Google Scholar] [CrossRef]
- Smyth, B. How Recreational Marathon Runners Hit the Wall: A Large-Scale Data Analysis of Late-Race Pacing Collapse in the Marathon. PLoS ONE 2021, 16, e0251513. [Google Scholar] [CrossRef] [PubMed]
- Smyth, B. Fast Starters and Slow Finishers: A Large-Scale Data Analysis of Pacing at the Beginning and End of the Marathon for Recreational Runners. J. Sport. Anal. 2018, 4, 229–242. [Google Scholar] [CrossRef] [Green Version]
- Billat, V.L.; Palacin, F.; Correa, M.; Pycke, J.R. Pacing Strategy Affects the Sub-Elite Marathoner’s Cardiac Drift and Performance. Front. Psychol. 2020, 10, 3026. [Google Scholar] [CrossRef] [Green Version]
- Billat, V.L.; Petot, H.; Landrain, M.; Meilland, R.; Koralsztein, J.P.; Mille-Hamard, L. Cardiac Output and Performance during a Marathon Race in Middle-Aged Recreational Runners. Sci. World J. 2012, 2012, 810859. [Google Scholar] [CrossRef] [Green Version]
- Maron, M.; Horvath, S.M.; Wilkerson, J.E.; Gliner, J.A. Oxygen Uptake Measurements During Competitive Marathon Running. J. Appl. Physiol. 1976, 40, 836–838. [Google Scholar] [CrossRef]
- Maron, M.B.; Horvath, S.M. The Marathon: A History and Review of the Literature. Med. Sci. Sport. 1978, 10, 137–150. [Google Scholar]
- Costill, D.L. Physiology of marathon running. JAMA 1972, 221, 1024–1029. [Google Scholar] [CrossRef]
- Sjödin, B.; Svedenhag, J. Applied Physiology of Marathon Running. Sport. Med. 1985, 2, 83–99. [Google Scholar] [CrossRef]
- Coyle, E.F. Physiological Regulation of Marathon Performance. Sport. Med. 2007, 37, 306–311. [Google Scholar] [CrossRef] [PubMed]
- Joyner, M.J.; Hunter, S.K.; Lucia, A.; Jones, A.M. Physiology and Fast Marathons. J. Appl. Physiol. 2020, 128, 1065–1068. [Google Scholar] [CrossRef] [PubMed]
- Jones, A.M.; Kirby, B.S.; Clark, I.; Rice, H.M.; Fulkerson, E.; Wylie, L.J.; Wilkerson, D.P.; Vanhatalo, A.; Wilkins, B.W. Physiological Demands of Running at 2-h Marathon Race Pace. J. Appl. Physiol. 2021, 130, 369–379. [Google Scholar] [CrossRef] [PubMed]
- Utter, A.C.; Kang, J.; Robertson, R.J.; Nieman, D.C.; Chaloupka, E.C.; Suminski, R.R.; Piccinni, C.R. Effect of Carbohydrate Ingestion on Ratings of Perceived Exertion During a Marathon. Med. Sci. Sport. Exerc. 2002, 34, 179–184. [Google Scholar] [CrossRef] [PubMed]
- Borg, G. Borg’s Perceived Exertion and Pain Scales; Human Kinetics: Champaing, IL, USA, 1998; p. 104. [Google Scholar]
- Mauger, A.R. Factors Affecting the Regulation of Pacing: Current Perspective. J. Sport. Med. 2014, 5, 209–214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pycke, J.R.; Billat, V. Marathon Performance Depends on Pacing Oscillations between Non Symmetric Extreme Values. Int. J. Environ. Res. Public Health 2022, 19, 2463. [Google Scholar] [CrossRef]
- Kendall, M.G.; Stuart, A. The Advance Theory of Statistics; Griffin and Co.: London, UK, 1963. [Google Scholar]
- Billat, V.; Carbillet, T.; Correa, M.; Pycke, J.-R. Detecting the Marathon Asymmetry with a Statistical Signature. Phys. A Stat. Mech. Appl. 2019, 515, 240–247. [Google Scholar] [CrossRef]
- Billat, V.; Vitiello, D.; Palacin, F.; Correa, M.; Pycke, J.R. Race Analysis of the World’s Best Female and Male Marathon Runners. Int. J. Environ. Res. Public Health 2020, 17, 1177. [Google Scholar] [CrossRef] [Green Version]
- Schroeder, M.A. Diagnosing and dealing with multicollinearity. West. J. Nurs. Res. 1990, 12, 175–184. [Google Scholar] [CrossRef]
- Muñoz-Pérez, I.; Mecías-Calvo, M.; Crespo-Álvarez, J.; Sámano-Celorio, M.L.; Agudo-Toyos, P.; Lago-Fuentes, C. Different Race Pacing Strategies Among Runners Covering the 2017 Berlin Marathon under 3 h and 30 min. PLoS ONE 2020, 28, e0236658. [Google Scholar]
- Breen, D.; Norris, M.; Healy, R.; Anderson, R. Marathon Pace Control in Masters Athletes. Int. J. Sport. Physiol. Perform. 2018, 13, 332–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nikolaidis, P.T.; Knechtle, B. Pacing Strategies in the ’Athens Classic Marathon’: Physiological and Psychological Aspects. Front. Physiol. 2018, 9, 1539. [Google Scholar] [CrossRef] [PubMed]
- Myrkos, A.; Smilios, I.; Kokkinou, E.M.; Rousopoulos, E.; Douda, H. Physiological and Race Pace Characteristics of Medium and Low-Level Athens Marathon Runners. Sport 2020, 9, 116. [Google Scholar] [CrossRef] [PubMed]
- Morgan, W.P. Psychological Components of Effort Sense. Med. Sci. Sport. Exerc. 1994, 26, 1071–1077. [Google Scholar] [CrossRef]
- Foster, C.; Hendrickson, K.J.; Peyer, K.; Reiner, B.; Dekoning, J.J.; Lucia, A.; Battista, R.A.; Hettinga, F.J.; Porcari, J.P.; Wright, G. Pattern of developing the performance template. Br. J. Sport. Med. 2009, 43, 765–769. [Google Scholar] [CrossRef] [Green Version]
- Noakes, T.D. Rating of Perceived Exertion as a Predictor of the Duration of Exercise that Remains Until Exhaustion. Br. J. Sport. Med. 2008, 42, 623–624. [Google Scholar]
- Lambert, E.V.; St Clair Gibson, A.; Noakes, T.D. Complex Systems Model of Fatigue: Integrative Homoeostatic Control of Peripheral Physiological Systems During Exercise in Humans. Br. J. Sport. Med. 2005, 39, 52–62. [Google Scholar] [CrossRef] [Green Version]
- Ranum, M.; Foster, C.; Cami, C.; Wright, G.; Guidotti, F.; De Koning, J.J.; Dodge, C.; Porcari, J.P. Effect of Running Velocity Variation on the Aerobic Cost of Running. Int. J. Environ. Res. Public Health 2021, 18, 2025. [Google Scholar] [CrossRef]
- Crandall, C.G.; González-Alonso, J. Cardiovascular Function in the Heat-Stressed Human. Acta Physiol. 2010, 199, 407–423. [Google Scholar] [CrossRef] [Green Version]
- Fritzsche, R.G.; Switzer, T.W.; Hodgkinson, B.J.; Coyle, E.F. Stroke Volume Decline During Prolonged Exercise Is Influenced by the Increase in Heart Rate. J. Appl. Physiol. 1999, 86, 799–805. [Google Scholar] [CrossRef] [Green Version]
- Billat, V.L.; Dupre, M.; Karp, J.R.; Koralsztein, J.P. Mountaineering Experience Decreases the Net Oxygen Cost of Climbing Mont Blanc (4808 m). Eur. J. Appl. Physiol. 2010, 108, 1209–1216. [Google Scholar] [CrossRef] [PubMed]
- Meyer, F.; Falbriard, M.; Mariani, B.; Aminian, K.; Millet, G.P. Continuous Analysis of Marathon Running Using Inertial Sensors: Hitting Two Walls? Int. J. Sport. Med. 2021, 42, 1182–1190. [Google Scholar] [CrossRef] [PubMed]
- Doherty, C.; Keogh, A.; Davenport, J.; Lawlor, A.; Smyth, B.; Caulfield, B. An Evaluation of the Training Determinants of Marathon Performance: A Meta-Analysis with Meta-Regression. J. Sci. Med. Sport. 2020, 23, 182–188. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n° Runners | Age (Years) | Fastest Marathon Times (Years) | Sénart Marathon (2019) |
|---|---|---|---|
| 1 | 47 | 03 h 1248 (2016) | 03 h 3134 |
| 2 | 44 | 03 h 3457 (2019) | 03 h 3457 * |
| 3 | 22 | 03 h 2240 (2019) | 03 h 2240 * |
| 4 | 34 | 02 h 5000 (2019) | 02 h 5000 * |
| 5 | 47 | 02 h 5922 (2016) | 03 h 3207 |
| 6 | 58 | 03 h 2732 (2013) | 04 h 3034 |
| 7 | 29 | 02 h 5703 (2015) | 03 h 1424 |
| 8 | 36 | 03 h 2758 (2017) | 03 h 5144 |
| 9 | 43 | 02 h 4400 (2015) | 03 h 1353 |
| n° Runner | Rf | Vt | E | Cad | HR | Speed | O2 | CO2 | |
|---|---|---|---|---|---|---|---|---|---|
| Runner 1 | Trend | ↗ | ↘ | ↘ | ↘ | ↗ | ↘ | ↘ | ↘ |
| Kendall Tau | 0.42 | −0.70 | −0.46 | −0.24 | 0.43 | −0.54 | −0.25 | −0.59 | |
| p-value | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | |
| Sk Pearson | −0.43 | 0.84 | −0.29 | −0.30 | −0.08 | 0.05 | −0.50 | 0.29 | |
| % km | 41 | 56 | 78 | 45 | 49 | 36 | 47 | 61 | |
| Runner 2 | Trend | ↗ | ↘ | ↘ | ↘ | ↘ | ↗ | ↘ | ↘ |
| Kendall Tau | 0.63 | −0.67 | −0.39 | −0.28 | −0.003 | 0.07 | −0.19 | −0.30 | |
| p-value | 0.001 | 0.001 | 0.001 | 0.001 | 0.883 | 0.001 | 0.001 | 0.001 | |
| Sk Pearson | 0.36 | −0.12 | −0.18 | −0.08 | 0.05 | 0.50 | 0.29 | 0.05 | |
| % km | 56 | 49 | 48 | 49 | 51 | 40 | 50 | 22 | |
| Runner 3 | Trend | ↗ | ↘ | ↗ | ↘ | ↗ | ↘ | ↗ | ↘ |
| Kendall Tau | 0.71 | −0.62 | 0.42 | −0.35 | 0.66 | −0.34 | 0.20 | −0.04 | |
| p-value | 0.03 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.03 | |
| Sk Pearson | 0.28 | −0.37 | −0.21 | −0.17 | −0.30 | −0.89 | −0.48 | 0.04 | |
| % km | 52 | 47 | 46 | 45 | 43 | 38 | 41 | 73 | |
| Runner 4 | Trend | ↗ | ↘ | ↗ | ↘ | ↘ | ↘ | ↗ | ↗ |
| Kendall Tau | 0.40 | −0.40 | 0.15 | −0.48 | −0.12 | −0.45 | 0.01 | 0.02 | |
| p-value | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.41 | 0.32 | |
| Sk Pearson | 1.09 | −0.36 | −0.01 | −0.23 | −0.12 | −0.70 | −0.24 | 0.34 | |
| % km | 68 | 45 | 49 | 47 | 48 | 22 | 44 | 53 | |
| Runner 5 | Trend | ↗ | ↘ | ↘ | ↘ | ↘ | ↘ | ↘ | ↘ |
| Kendall Tau | 0.15 | −0.36 | −0.14 | −0.19 | −0.21 | −0.57 | −0.076 | −0.35 | |
| p-value | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | |
| Sk Pearson | −0.93 | 0.41 | −0.32 | −0.22 | 0.08 | 0.01 | −0.44 | −0.11 | |
| % km | 29 | 56 | 45 | 45 | 51 | 61 | 42 | 35 | |
| Runner 6 | Trend | ↘ | ↘ | ↘ | ↘ | ↗ | ↘ | ↘ | ↘ |
| Kendall Tau | −0.07 | −0.41 | −0.35 | −0.57 | 0.20 | −0.59 | −0.35 | −0.49 | |
| p-value | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | |
| Sk Pearson | −0.43 | 0.02 | −0.18 | −0.40 | −0.10 | −0.79 | −0.46 | −0.36 | |
| % km | 42 | 50 | 47 | 44 | 48 | 33 | 44 | 32 | |
| Runner 7 | Trend | ↗ | ↘ | ↘ | ↘ | ↘ | ↘ | ↘ | ↘ |
| Kendall Tau | 0.59 | −0.73 | −0.36 | −0.46 | −0.26 | −0.47 | −0.46 | −0.59 | |
| p-value | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | |
| Sk Pearson | −0.28 | 0.27 | −0.60 | −0.54 | −0.51 | −0.46 | −0.85 | −.65 | |
| % km | 45 | 53 | 41 | 42 | 43 | 42 | 39 | 43 | |
| Runner 8 | Trend | ↗ | ↘ | ↘ | ↘ | ↗ | ↘ | ↘ | ↘ |
| Kendall Tau | 0.54 | −0.46 | −0.19 | −0.57 | 0.40 | −0.58 | −0.26 | −0.40 | |
| p-value | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | |
| Sk Pearson | −0.34 | 0.57 | 0.11 | −1.20 | −1.33 | −0.41 | −0.36 | −0.64 | |
| % km | 46 | 55 | 51 | 34 | 33 | 32 | 39 | 47 | |
| Runner 9 | Trend | ↗ | ↘ | ↗ | ↘ | ↗ | ↘ | ↗ | ↘ |
| Kendall Tau | 0.79 | −0.71 | 0.30 | −0.51 | 0.77 | −0.21 | 0.13 | −0.39 | |
| p-value | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | |
| Sk Pearson | 0.30 | −0.62 | −0.11 | −0.36 | −0.33 | −0.80 | −0.08 | 0.55 | |
| % km | 55 | 42 | 48 | 42 | 44 | 40 | 44 | 53 |
| n° Runner | ||||||||
|---|---|---|---|---|---|---|---|---|
| Runner 1 | Trend | ↗ | ↘ | ↘ | ↗ | ↗ | ↗ | ↘ |
| Kendall Tau | 0.62 | −0.46 | −0.002 | 0.49 | 0.64 | 0.32 | −0.22 | |
| p-value | 0.001 | 0.001 | 0.941 | 0.001 | 0.001 | 0.001 | 0.001 | |
| Runner 2 | Trend | ↗ | ↘ | ↘ | ↘ | ↗ | ↗ | ↗ |
| Kendall Tau | 0.35 | −0.58 | −0.32 | −0.08 | 0.02 | −0.23 | −0.41 | |
| p-value | 0.001 | 0.001 | 0.001 | 0.001 | 0.34 | 0.001 | 0.001 | |
| Runner 3 | Trend | ↗ | ↘ | ↗ | ↗ | ↗ | ↗ | ↗ |
| Kendall Tau | 0.74 | −0.50 | 0.53 | 0.26 | 0.64 | 0.44 | 0.19 | |
| p-value | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | |
| Runner 4 | Trend | ↗ | ↘ | ↗ | ↗ | ↗ | ↗ | ↘ |
| Kendall Tau | 0.34 | −0.30 | 0.07 | 0.26 | 0.38 | 0.02 | −0.02 | |
| p-value | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.302 | |
| Runner 5 | Trend | ↗ | ↗ | ↗ | ↗ | ↗ | ↗ | ↗ |
| Kendall Tau | 0.55 | 0.07 | 0.26 | 0.54 | 0.53 | 0.37 | 0.08 | |
| p-value | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | |
| Runner 6 | Trend | ↗ | ↗ | ↗ | ↗ | ↗ | ↗ | ↘ |
| Kendall Tau | 0.50 | 0.30 | 0.21 | 0.52 | 0.60 | 0.30 | −0.04 | |
| p-value | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | |
| Runner 7 | Trend | ↗ | ↘ | ↗ | ↗ | ↗ | ↘ | ↘ |
| Kendall Tau | 0.74 | −0.48 | 0.06 | 0.45 | 0.57 | −0.02 | −0.38 | |
| p-value | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.314 | 0.001 | |
| Runner 8 | Trend | ↗ | ↘ | ↗ | ↗ | ↗ | ↗ | ↘ |
| Kendall Tau | 0.67 | −0.23 | 0.09 | 0.52 | 0.62 | 0.12 | −0.15 | |
| p-value | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | |
| Runner 9 | Trend | ↗ | ↘ | ↗ | ↗ | ↗ | ↗ | ↘ |
| Kendall Tau | 0.73 | −0.52 | 0.38 | 0.07 | 0.54 | 0.28 | −0.13 | |
| p-value | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 |
| n° Runner | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Runner 1 | Trend | ↘ | ↘ | ↘ | ↘ | ↘ | ↘ | ↘ | ↘ |
| Kendall Tau | −0.62 | −0.84 | −0.78 | −0.79 | −0.80 | −0.79 | −0.78 | −0.51 | |
| p-value | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | |
| Runner 2 | Trend | ↘ | ↘ | ↘ | ↘ | ↘ | ↘ | ↘ | ↘ |
| Kendall Tau | −0.48 | −0.78 | −0.70 | −0.74 | −0.70 | −0.73 | −0.71 | −0.74 | |
| p-value | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | |
| Runner 3 | Trend | ↘ | ↘ | ↘ | ↘ | ↘ | ↘ | ↘ | ↘ |
| Kendall Tau | −0.24 | −0.83 | −0.66 | −0.83 | −0.74 | −0.78 | −0.72 | −0.73 | |
| p-value | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | |
| Runner 4 | Trend | ↘ | ↘ | ↘ | ↘ | ↘ | ↘ | ↘ | ↘ |
| Kendall Tau | −0.28 | −0.72 | −0.55 | −0.82 | −0.63 | −0.73 | −0.50 | −0.54 | |
| p-value | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | |
| Runner 5 | Trend | ↘ | ↗ | ↘ | ↘ | ↘ | ↘ | ↘ | ↘ |
| Kendall Tau | −0.24 | 0.56 | −0.38 | −0.54 | −0.53 | −0.65 | −0.43 | −0.53 | |
| p-value | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | |
| Runner 6 | Trend | ↘ | ↘ | ↘ | ↘ | ↘ | ↘ | ↘ | ↘ |
| Kendall Tau | −0.29 | −0.59 | −0.50 | −0.65 | 0.08 | −0.64 | −0.51 | −0.61 | |
| p-value | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | |
| Runner 7 | Trend | ↘ | ↘ | ↘ | ↘ | ↘ | ↘ | ↘ | ↘ |
| Kendall Tau | −0.06 | −0.81 | −0.59 | −0.62 | −0.51 | −0.56 | −0.66 | −0.70 | |
| p-value | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | |
| Runner 8 | Trend | ↘ | ↘ | ↘ | ↘ | ↘ | ↘ | ↘ | ↘ |
| Kendall Tau | −0.38 | −0.68 | −0.54 | −0.86 | −0.78 | −0.81 | −0.65 | −0.71 | |
| p-value | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | |
| Runner 9 | Trend | ↘ | ↘ | ↘ | ↘ | ↘ | ↘ | ↘ | ↘ |
| Kendall Tau | −0.02 | −0.81 | −0.51 | −0.82 | −0.53 | −0.66 | −0.53 | −0.70 | |
| p-value | 0.301 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 |
| 5 km | 10 km | 15 km | 20 km | 25 km | 30 km | 35 km | 40 km | 42 km | ||
|---|---|---|---|---|---|---|---|---|---|---|
| RPE | Mean | 11.6 | 12.33 | 12.56 | 13.33 | 14.13 | 15 | 15.28 | 15.78 | 16.11 |
| SD | 1.65 | 1.2 | 1.3 | 1.01 | 1.11 | 1.11 | 1.0 | 1.2 | 1.53 | |
| Test-t | 2.30 * | 2.30 * | 2.30 | 2.30 | 2.30 ** | 2.30 ** | 2.30 * | 2.30 ** | 2.30 | |
| Cad | Mean | 87.6 | 88.0 | 87.7 | 87.5 | 87.5 | 86.9 | 86.9 | 85.7 | 84.6 |
| SD | 3.2 | 2.5 | 2.9 | 3.0 | 3.0 | 3.0 | 3.3 | 4.8 | 1.9 | |
| Test-t | 2.30 | 2.30 | 2.30 ** | 2.30 | 2.30 | 2.30 * | 2.30 | 2.30 | 2.30 | |
| CO2 | Mean | 39.9 | 41.9 | 40.1 | 39.8 | 39.44 | 38.7 | 36.9 | 34.5 | 32.3 |
| SD | 4.7 | 3.5 | 3.6 | 4.0 | 4.3 | 4.4 | 5.6 | 6.9 | 5.7 | |
| Test-t | 2.30 | 2.30 | 2.30 *** | 2.30 | 2.30 | 2.30 | 2.30 * | 2.30 | 2.30 | |
| O2 | Mean | 40.1 | 43.9 | 43.1 | 43.1 | 42.6 | 42.7 | 41.8 | 39.8 | 37.8 |
| SD | 4.0 | 4.1 | 4.4 | 4.5 | 4.6 | 4.7 | 5.7 | 6.8 | 5.9 | |
| Test-t | 2.30 | 2.30 *** | 2.30 ** | 2.30 | 2.30 | 2.30 | 2.30 | 2.30 | 2.30 | |
| Speed | Mean | 12.7 | 13.3 | 13 | 12.9 | 12.7 | 12.3 | 11.9 | 11.18 | 11.43 |
| SD | 1.0 | 1.1 | 1.2 | 1.2 | 1.2 | 1.3 | 1.4 | 1.6 | 1.8 | |
| Test-t | 2.30 ** | 2.30 *** | 2.30 ** | 2.30 | 2.30 | 2.30 | 2.30 ** | 2.30 ** | 2.30 | |
| HR | Mean | 150 | 159 | 159 | 160 | 162 | 161 | 160 | 158 | 160 |
| SD | 8.7 | 6.18 | 5.35 | 6.84 | 6.16 | 6.23 | 8.05 | 8.4 | 6.9 | |
| Test-t | 2.30 *** | 2.30 ** | 2.30 | 2.30 | 2.30 | 2.30 | 2.30 | 2.30 | 2.30* | |
| RER | Mean | 0.96 | 0.95 | 0.93 | 0.92 | 0.92 | 0.89 | 0.87 | 0.86 | 0.86 |
| SD | 0.01 | 0.04 | 0.04 | 0.03 | 0.03 | 0.02 | 0.03 | 0.03 | 0.02 | |
| Test-t | 2.11 *** | 2.30 *** | 2.31 *** | 2.31 *** | 2.30 *** | 2.30 *** | 2.31 *** | 2.30 *** | 2.30 *** |
| Rf | Speed | Vt | RPE | HR | Cadence | F1/F2(%) | ||
|---|---|---|---|---|---|---|---|---|
| Runner 1 | F1 | 0.715 | −0.696 | −0.817 | 0.926 | 0.507 | −0.242 | 79.6 |
| F2 | 0.566 | 0.617 | 0.328 | 0.085 | 0.768 | 0.729 | ||
| VIF | 3.58 | 3.82 | 4.96 | 3.43 | 1.63 | 5.37 | ||
| Runner 2 | F1 | −0.823 | 0.742 | 0.924 | −0.89 | 0.468 | 0.015 | 75.1 |
| F2 | 0.391 | 0.448 | −0.08 | 0.237 | 0.567 | 0.82 | ||
| VIF | 3.08 | 2.12 | 3.89 | 3.81 | 1.33 | 1.23 | ||
| Runner 3 | F1 | 0.937 | −0.372 | 0.826 | 0.943 | 0.764 | −0.160 | 82.8 |
| F2 | 0.200 | 0.842 | 0.246 | 0.09 | 0.491 | 0.84 | ||
| VIF | 7.14 | 2.60 | 4.11 | 6.03 | 6.44 | 1.75 | ||
| Runner 4 | F1 | −0.55 | 0.83 | 0.686 | −0.73 | 0.04 | 0.66 | 68.9 |
| F2 | 0.947 | −0.78 | −0.820 | 0.895 | 0.754 | −0.388 | ||
| VIF | 2.23 | 2.96 | 1.68 | 1.93 | 1.76 | 2.43 | ||
| Runner 5 | F1 | −0.44 | 0.861 | 0.65 | −0.801 | 0.449 | 0.44 | 60.2 |
| F2 | 0.76 | 0.21 | −0.42 | −0.235 | 0.587 | −0.03 | ||
| VIF | 1.39 | 0.611 | 0.29 | 0.558 | 0.171 | 0.086 | ||
| Runner 6 | F1 | 0.05 | 0.89 | 0.29 | −0.72 | 0.706 | 0.906 | 65.7 |
| F2 | −0.71 | 0.06 | 0.64 | −0.27 | −0.44 | −0.09 | ||
| VIF | 1.05 | 3.37 | 1.13 | 1.56 | 1.76 | 3.69 | ||
| Runner 7 | F1 | 0.61 | −0.839 | −0.86 | 0.93 | −0.35 | −0.82 | 83.3 |
| F2 | 0.74 | 0.32 | −0.26 | 0.08 | 0.84 | 0.23 | ||
| VIF | 4.45 | 2.97 | 4.16 | 4.59 | 2.35 | 2.52 | ||
| Runner 8 | F1 | 0.801 | −0.805 | −0.706 | 0.900 | 0.538 | −0.731 | 76.0 |
| F2 | 0.439 | 0.359 | 0.04 | −0.048 | 0.736 | 0.526 | ||
| VIF | 2.90 | 2.81 | 2.05 | 3.28 | 2.06 | 2.39 | ||
| Runner 9 | F1 | −0.875 | 0.832 | 0.826 | 0.895 | −0.714 | 0.461 | 78.6 |
| F2 | 0.19 | 0.35 | 0.045 | 0.184 | 0.410 | 0.865 | ||
| VIF | 8.90 | 2.72 | 4.59 | 4.59 | 4.55 | 1.63 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Billat, V.; Poinsard, L.; Palacin, F.; Pycke, J.R.; Maron, M. Oxygen Uptake Measurements and Rate of Perceived Exertion during a Marathon. Int. J. Environ. Res. Public Health 2022, 19, 5760. https://doi.org/10.3390/ijerph19095760
Billat V, Poinsard L, Palacin F, Pycke JR, Maron M. Oxygen Uptake Measurements and Rate of Perceived Exertion during a Marathon. International Journal of Environmental Research and Public Health. 2022; 19(9):5760. https://doi.org/10.3390/ijerph19095760
Chicago/Turabian StyleBillat, Véronique, Luc Poinsard, Florent Palacin, Jean Renaud Pycke, and Michael Maron. 2022. "Oxygen Uptake Measurements and Rate of Perceived Exertion during a Marathon" International Journal of Environmental Research and Public Health 19, no. 9: 5760. https://doi.org/10.3390/ijerph19095760
APA StyleBillat, V., Poinsard, L., Palacin, F., Pycke, J. R., & Maron, M. (2022). Oxygen Uptake Measurements and Rate of Perceived Exertion during a Marathon. International Journal of Environmental Research and Public Health, 19(9), 5760. https://doi.org/10.3390/ijerph19095760