
Government Reactions, Citizens’ Responses, and COVID-19 around the World


Abstract
:1. Introduction
2. Materials and Methods
3. Empirical Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Countries with No Past Experience |
|---|
| Afghanistan, Albania, Algeria, Argentina, Armenia, Australia, Austria, Bangladesh, Belgium, Benin, Bolivia, Bosnia and Herzegovina, Botswana, Brazil, Bulgaria, Burkina Faso, Burundi, Cameroon, Canada, Chad, Chile, Colombia, Costa Rica, Croatia, Cyprus, Czech Republic, Denmark, Dominican Republic, El Salvador, Estonia, Finland, France, Georgia, Germany, Ghana, Greece, Guatemala, Guinea, Honduras, Hungary, Iceland, India, Ireland, Israel, Italy, Kenya, Kyrgyzstan, Latvia, Lebanon, Liberia, Lithuania, Luxembourg, Madagascar, Malawi, Malta, Mauritius, Mexico, Moldova, Montenegro, Mozambique, Myanmar, Netherlands, New Zealand, Nicaragua, Niger, Norway, Panama, Paraguay, Peru, Poland, Portugal, Romania, Russia, Senegal, Serbia, Sierra Leone, Slovakia, Slovenia, South Africa, Spain, Sri Lanka, Sweden, Switzerland, Tanzania, Tunisia, Turkey, Uganda, Ukraine, United Kingdom, United States, Uruguay, Uzbekistan, Zambia |
| Countries with Pandemic Past Experience (Sachs, 2021) |
| Indonesia, Japan, Malaysia, Singapore, Thailand |
References
- Serikbayeva, B.; Abdulla, K.; Oskenbayev, Y. State Capacity in Responding to COVID-19. Int. J. Public Adm. 2020, 44, 920–930. [Google Scholar] [CrossRef]
- Siegrist, M.; Zingg, A. The Role of Public Trust During Pandemics: Implications for Crisis Communication. Eur. Psychol. 2014, 19, 23–32. [Google Scholar] [CrossRef]
- Schmelz, K.; Bowles, S. Overcoming COVID-19 vaccination resistance when alternative policies affect the dynamics of conformism, social norms, and crowding out. Proc. Natl. Acad. Sci. USA 2021, 118, e2104912118. [Google Scholar] [CrossRef]
- Siegrist, M.; Luchsinger, L.; Bearth, A. The Impact of Trust and Risk Perception on the Acceptance of Measures to Reduce COVID-19 Cases. Risk Anal. 2021, 41, 787–800. [Google Scholar] [CrossRef]
- Algan, Y.; Cohen, D.; Davoine, E.; Stantcheva, S. Trust in Scientists in Times of Pandemic: Panel Evidence from 12 Countries. Proc. Natl. Acad. Sci. USA 2021, 118, e210857611. [Google Scholar] [CrossRef] [PubMed]
- Bargain, O.; Aminjonov, U. Trust and compliance to public health policies in the time of COVID-19. J. Public Econ. 2020, 192, 104316. [Google Scholar] [CrossRef] [PubMed]
- Barrios, J.; Benmelech, E.; Hochberg, Y.; Sapienza, P.; Zingales, L. Civic Capital and Social Distancing during the COVID-19 Pandemic; Working Paper; Chicago University: Chicago, IL, USA, 2020. [Google Scholar]
- Bartscher, A.K.; Seitz, S.; Siegloch, S.; Slotwinski, M.; Wehrhöfer, N. Social capital and the spread of COVID-19: Insights from European countries. J. Health Econ. 2021, 80, 102531. [Google Scholar] [CrossRef]
- Durante, R.L.; Guiso, L.; Gulino, G. Asocial capital: Civic culture and social distancing during the COVID-19 crisis. J. Public Econ. 2021, 194, 104342. [Google Scholar] [CrossRef]
- OECD. Health at a Glance; OECD: Paris, France, 2020. [Google Scholar]
- Oksanen, A.; Kaakinen, M.; Latikka, R.; Savolainen, I.; Savela, N.; Koivula, A. Regulation and Trust: 3-Month Follow-up Study on COVID-19 Mortality in 25 European Countries. JMIR Public Health Surveill. 2020, 6, e19218. [Google Scholar] [CrossRef]
- Ma, M.; Wang, S.; Wu, F. COVID-19 Prevalence and Well-being: Lessons from East Asia. In World Happiness Report; Helliwell, J., Layard, R., Sachs, J.D., De Neve, J.-E., Aknin, L., Wang, S., Paculor, S., Eds.; 2021; Available online: https://worldhappiness.report/ed/2021/ (accessed on 5 February 2022).
- Sachs, J.D. Comparing COVID-19 Control in the Asia-Pacific and North Atlantic Regions. Asian Econ. Pap. 2021, 20, 30–54. [Google Scholar] [CrossRef]
- Ostrom, E. Governing the Commons. The Evolution of Institutions for Collective Action; Cambridge University Press: Cambridge, UK, 1991. [Google Scholar]
- Putnam, R. Making Democracy Work. Civic Traditions in Modern Italy; Princeton University Press: Princeton, NJ, USA, 1994. [Google Scholar]
- Putnam, R. Bowling Alone: The Collapse and Revival of American Community; Simon and Schuster: New York, NY, USA, 2000. [Google Scholar]
- Rothstein, B. Social Traps and the Problem of Trust; Cambridge University Press: Cambridge, UK, 2005. [Google Scholar]
- Svendsen, G.T.; Svendsen, G.L.H. Handbook of Social Capital. The Troika of Sociology, Political Science and Economics; Edward Elgar Publishing Ltd.: Cheltenham, UK, 2009. [Google Scholar]
- Cassan, G.; Van Steenvoort, M. Political regime and COVID 19 death rate: Efficient, biasing or simply different autocracies? An econometric analysis. SSM—Popul. Health 2021, 16, 100912. [Google Scholar] [CrossRef] [PubMed]
- Annaka, S. Political regime, data transparency, and COVID-19 death cases. SSM—Popul. Health 2021, 15, 100832. [Google Scholar] [CrossRef]
- Cepaluni, G.; Dorsch, M.; Branyiczki, R. Political Regimes and Deaths in the Early Stages of the COVID-19 Pandemic. Journal of Public Finance and Public Choice, Preprint Version. 2021. Available online: https://www.ingentaconnect.com/content/bup/jpfpc/pre-prints/content-jpfpcd2100013# (accessed on 5 February 2022).
- Cheibub, J.A.; Hong, J.Y.; Przeworski, A. Rights and Deaths: Government Reactions to the Pandemic. 2020. Available online: https://ssrn.com/abstract=3645410 (accessed on 5 February 2022).
- Karabulut, G.; Zimmermann, K.F.; Bilgin, M.H.; Doker, A.C. Democracy and COVID-19 outcomes. Econ. Lett. 2021, 203, 109840. [Google Scholar] [CrossRef] [PubMed]
- Yao, L.; Li, M.; Wan, J.Y.; Howard, S.C.; Bailey, J.E.; Graff, J.C. Democracy and case fatality rate of COVID-19 at early stage of pandemic: A multicountry study. Environ. Sci. Pollut. Res. 2021, 29, 8694–8704. [Google Scholar] [CrossRef] [PubMed]
- EIU. Democracy Index 2020. In Sickness and in Health; The Economist Intelligence Unit Limited: London, UK, 2020. [Google Scholar]
- Dohle, S.; Wingen, T.; Schreiber, M. Acceptance and Adoption of Protective Measures during the COVID-19 Pandemic: The Role of Trust in Politics and Trust in Science. Soc. Psychol. Bull. 2020, 15, 1–23. [Google Scholar] [CrossRef]
- Helliwell, J.; Wang, S. Trust and Wellbeing. Int. J. Wellbeing 2011, 1, 42–78. [Google Scholar]
- Wellcome Trust. How Does the World Feel about Science and Health? Wellcome Global Monitor; Gallup: Washington, DC, USA, 2019. [Google Scholar]
- Lenton, T.; Boulton, C.; Scheffer, M. Resilence pf Countries to COVID-19 correlated with Trust. Sci. Rep. 2022, 12, 75. [Google Scholar] [CrossRef]
- Gerring, J.; Bond, P.; Barndt, W.T.; Moreno, C. Democracy and Economic Growth. World Politics. A Historical Perspective. J. Political Econ. 2005, 57, 323–364. [Google Scholar]
- Mazzucchelli, R.; Agudo-Dieguez, A.; Dieguez-Costa, E.; Crespi-Villarías, N. Democracia y Mortalidad por COVID-19 en Europa. Rev. Esp. Salud Pública 2020, 94, 78. Available online: https://pesquisa.bvsalud.org/portal/resource/pt/ibc-192512 (accessed on 5 February 2022).
- Franco, A.; Alvarez-Dardet, C.; Ruiz, M. Effect of Democracy on Health: Ecological Study. Politics Health 2004, 329, 18–25. [Google Scholar] [CrossRef] [Green Version]
- Bandres, E.; Gonzalez, R. La reducción del gasto sanitario en España durante la crisis. Cuad. De Inf. Econ. 2015, 248, 37–48. [Google Scholar]

| Variable | Std. Dev. | Min | Pctl. 25 | Pctl. 75 | Max | Source |
|---|---|---|---|---|---|---|
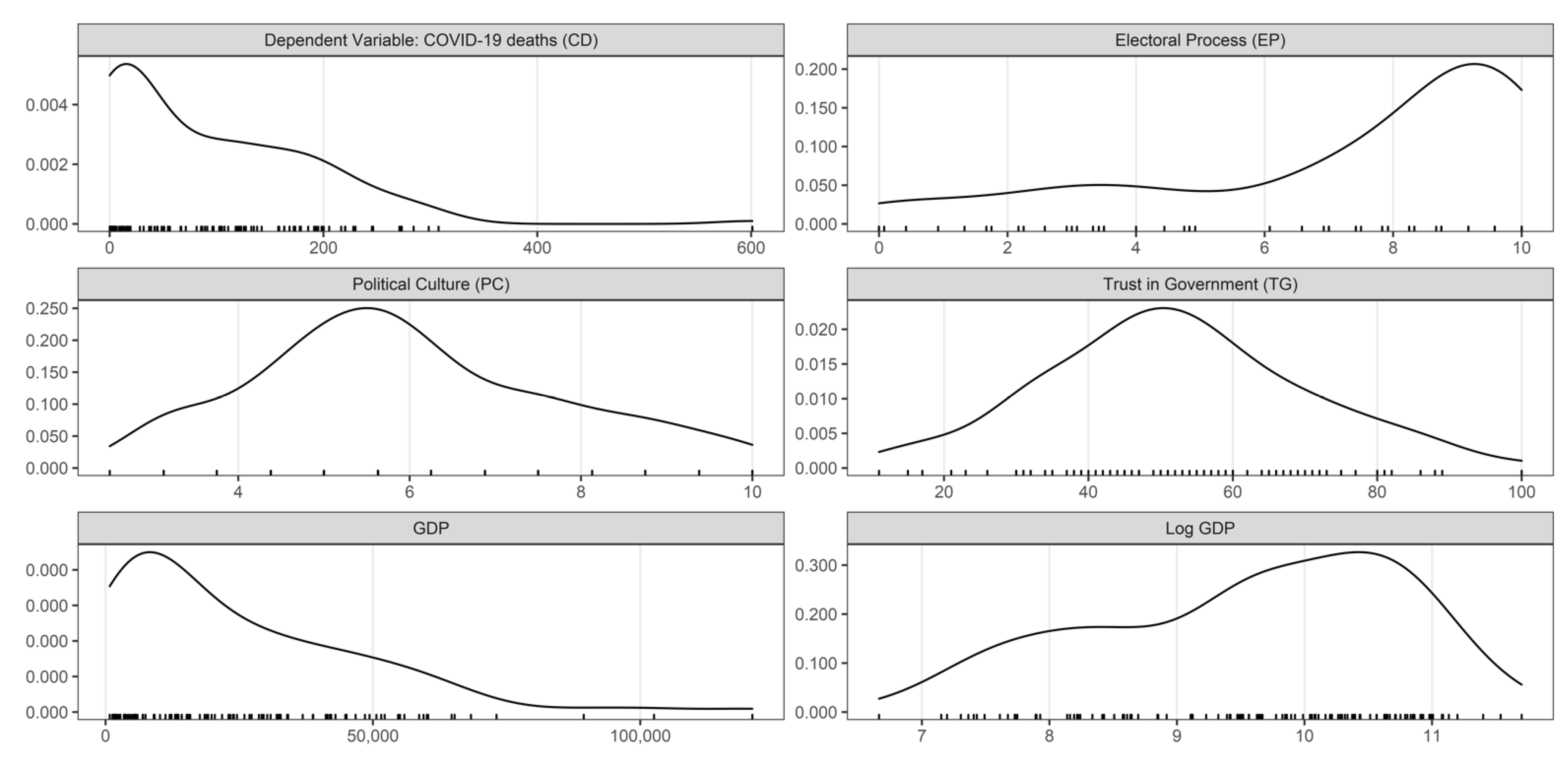
| Trust in Government | 17.22 | 11 | 40.75 | 64.25 | 89 | Wellcome Global Monitor |
| Electoral Process | 2.27 | 0.42 | 7 | 9.58 | 10 | The Economist Intelligence Unit |
| Political Culture | 1.84 | 3.13 | 5 | 7.5 | 10 | The Economist Intelligence Unit |
| GDP per capita | 23.90 | 1.28 | 11.8 | 42.39 | 12.09 | World Bank |
| log. GDP per capita | 1.11 | 7.15 | 9.38 | 10.66 | 11.70 |
| Predictors | CD Estimates |
|---|---|
| Intercept | −78.293 |
| (72.186) | |
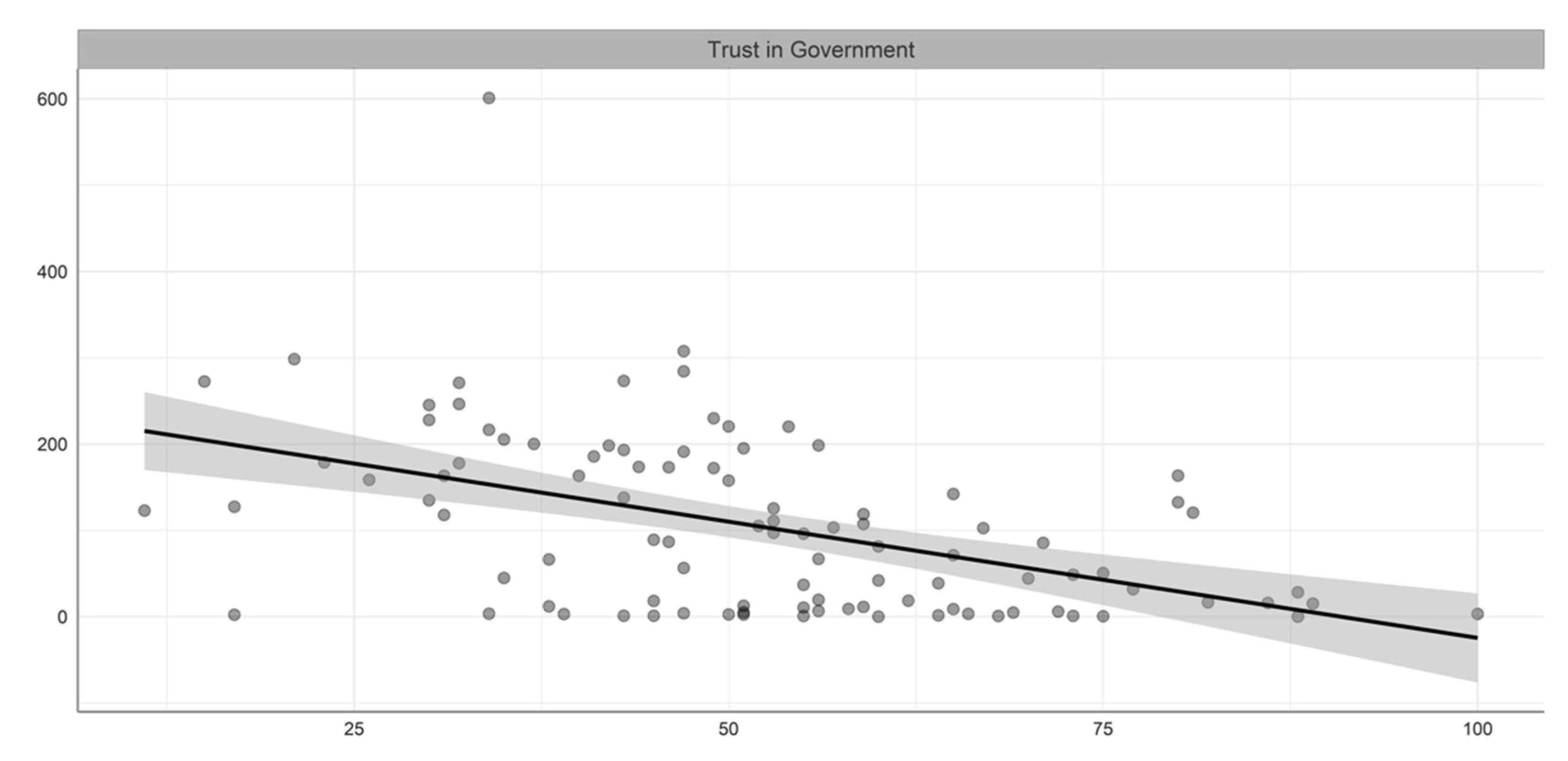
| Trust in Government | −1.589 * |
| (0.494) | |
| Electoral Process and Pluralism | 12.388 * |
| (3.940) | |
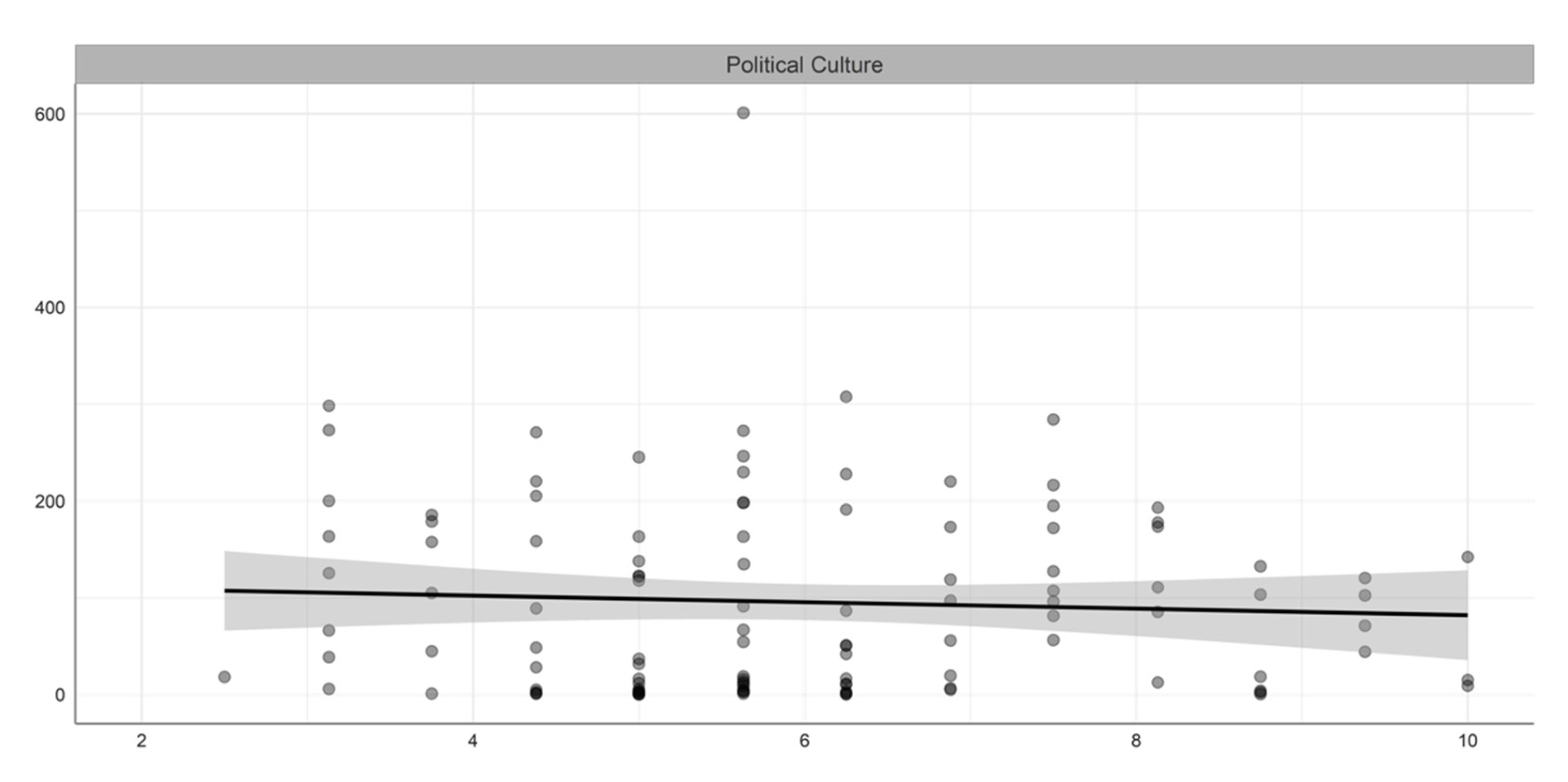
| Political Culture | −21.865 * |
| (5.441) | |
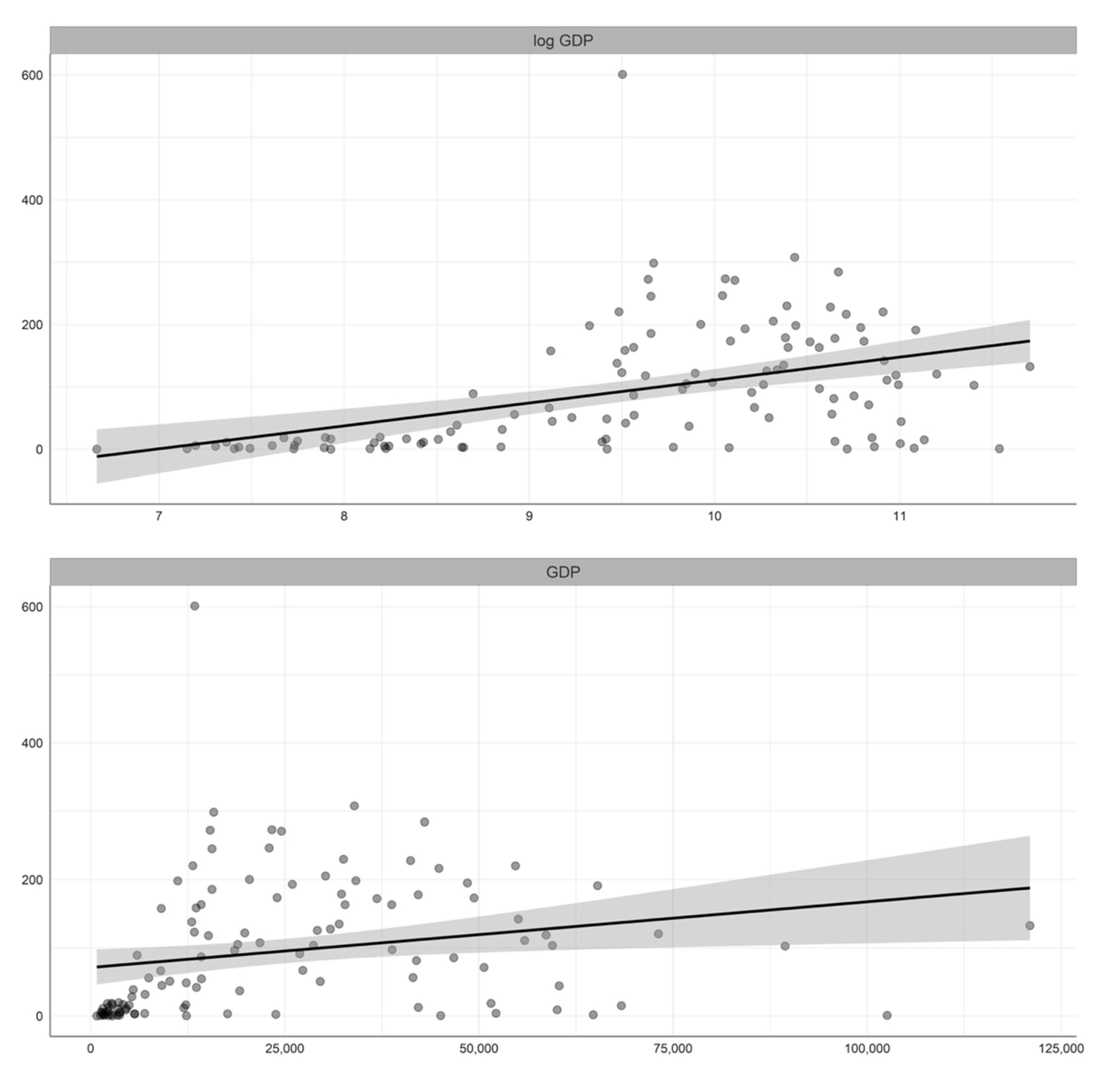
| Gross domestic product (log GDP) | 32.122 * |
| (8.901) | |
| Experience | −61.111 + |
| (35.167) | |
| Observations | 98 |
| R2 | 0.511 |
| Adjusted R2 | 0.485 |
| Residual Std. Error | 73.546 (df = 92) |
| F Statistic | 19.251 (df = 5; 92) |
| Predictors | Estimates | Standardized |
|---|---|---|
| Trust in Government | −1.59 | −0.27 |
| Electoral Process and Pluralism | 12.38 | 0.34 |
| Political Culture | −21.87 | −0.39 |
| Gross domestic product (log GDP) | 32.12 | 0.38 |
| Experience | −61.11 | −0.13 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reiersen, J.; Romero-Hernández, M.; Adán-González, R. Government Reactions, Citizens’ Responses, and COVID-19 around the World. Int. J. Environ. Res. Public Health 2022, 19, 5667. https://doi.org/10.3390/ijerph19095667
Reiersen J, Romero-Hernández M, Adán-González R. Government Reactions, Citizens’ Responses, and COVID-19 around the World. International Journal of Environmental Research and Public Health. 2022; 19(9):5667. https://doi.org/10.3390/ijerph19095667
Chicago/Turabian StyleReiersen, Jon, Manuel Romero-Hernández, and Romén Adán-González. 2022. "Government Reactions, Citizens’ Responses, and COVID-19 around the World" International Journal of Environmental Research and Public Health 19, no. 9: 5667. https://doi.org/10.3390/ijerph19095667
APA StyleReiersen, J., Romero-Hernández, M., & Adán-González, R. (2022). Government Reactions, Citizens’ Responses, and COVID-19 around the World. International Journal of Environmental Research and Public Health, 19(9), 5667. https://doi.org/10.3390/ijerph19095667